How to Write a Case Note using the SOAP Method (PowerPoint)
advertisement
")
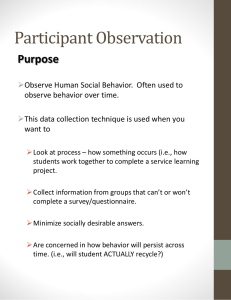
Presented by UIC-CON State the importance of documenting risk. Describe how identification of risk impacts the delivery of quality care and improves outcomes. Identify the differences between the old and new risk inventory. Explain the expanded content areas covered in the risk inventory. Construct a risk inventory on a participant. To maintain participant’s safety and quality of life. To create awareness of participants’ risks among the care team. To develop a mitigation plan addressing preventable incidents. To identify additional supports and/or services required. To prioritize risk based on severity of harm. To evaluate a mitigation plan based on changing risk. Pre-transition o Complete baseline (MFP requirement) o Revise as needed, based on change(s) to the participant’s condition Post-transition o Review at least monthly o Revise as needed, based on change(s) to the participant’s condition Complete assessment. If your agency does not have a formal assessment, a demonstration on how to convert the risk inventory into an assessment will be presented. Complete MFP Risk Inventory based on findings from your assessment. May need to expand assessment based on new areas on the risk inventory. 80 questions, 10 domains Physical Health Behavioral and Emotional Health Substance Abuse Self-Harm or Harm to Others Cognition Medication, Laboratory, and Utilization Functional: ADLs & IADLs Environment Interpersonal and Social Supports Engagement, Self-Management, Recovery Representation of major body systems: circulatory, respiratory, digestive, intestinal, urinary, etc. Includes additional questions on pain, wounds, sleep, falls, burns, etc. Assess participant’s knowledge of disease management. Assess for presence of acute physical symptoms (a good indicator of disease management). Assess for presence of acute behavioral or emotional health symptoms (a good indicator of disease management). Symptoms identified include disorganized thought processes, false sensory perceptions, social withdrawal, mood changes, anxiety, etc. This domain focuses on presence of symptoms rather than self-management of disease. Assess for current signs of substance abuse and risk for relapse. Assess for history of substance abuse. Assess for history or current engagement in criminal activity (i.e., arson, gang activity, property destruction). Assess for history or current engagement in risky behaviors (i.e., unhealthy sexual practices). Assess for history of suicidal and/or homicidal behavior. Assess for history or current vulnerability for abuse, neglect, or exploitation. Assesses for presence or risk of diminished cognitive functioning resulting in impaired judgment, impaired problem solving ability, or lack of orientation. Assess participant’s knowledge, ability, and adherence to medication management. Assess for lack of primary care services. Assess for frequent utilization of emergency services. Assess participant’s ability to perform Activities of Daily Living (ADLs) and Instrumental Activities of Daily Living (IADLs). Assess need and proper use of assistive and adaptive devices. Assess participant’s home and neighborhood for accessibility and safety (e.g., accessibility of home, availability of community resources). Assess engagement and quality of interpersonal relationships (e.g., presence of social support system, healthy interactions). Assess engagement in plan of care (e.g., motivation, trust, interest, understanding, historical success). Identify barriers that negatively affect plan of care. Each question is equivalent to a risk. Check ‘Yes’ if risk was identified Check ‘No’ if risk was not identified For each risk identified, you will be asked to “Describe why this is a risk for the participant” – This is where you enter data from your assessment. Then, you will be asked (for each risk identified) to “Describe how this risk will be mitigated before and after transition” – This is your mitigation plan. In the mitigation plan, you are asked to develop individualized strategies to mitigate a known risk using an action verb (i.e., evaluate, educate, coach, arrange, coordinate, etc.). Risk Inventory is a tool used to organize assessment findings into specific content domains. Conducting a comprehensive assessment is significant to risk identification. Developing tailored strategies specific to the participant is consequential to risk mitigation. Presented by UIC-CON At the end of this session, the learner will be able to: Define the importance of documenting case notes. Describe the SOAP method for documenting case notes. Illustrate when, where, and how to document a case note. Construct a case note in the MFP CRM Web Application. 20 Keeps provider(s) abreast on current treatment plan and ongoing developments Provides the care team with a mechanism to communicate with one another Supports an action by demonstrating providers’ engagement with participant Provides a representation of the participant and his/her progress before and after transition 21 After a home visit with an MFP participant and/or caregiver After a phone call with an MFP participant and/or caregiver After an office visit with an MFP participant Documentation of case notes is ongoing, pre- and post-transition. 22 Use the notes feature to document contacts. Click the “+” sign to add a new note (upper right hand corner). 23 Select Contact Date Select Contact Type: Face-to-face visit Phone call Email Fax Other Select Location: Participant’s home TC’s office Hospital/Institutional care setting Service Provider’s Office (i.e., psychiatrist) Community Provider (i.e., day program) Other 24 Select Persons Contacted (Select All): Participant Family/Guardian/Significant Other/Power-of-Attorney for Health Care Physician Hospital Staff (e.g., nurse, social worker, discharge planner) Facility Staff Community Provider/Worker/Case Manager Other Community Based Persons (e.g., friend, lawyer) Other Enter a SOAP Note for contact: Subjective findings Objective findings Assessment findings Plan Other Notes 25 Definition An organized method of documentation used by providers to describe events involving the participant. Purpose The SOAP note format is used to facilitate effective communication among the care team by providing assessment findings, identifying problem(s), and developing action plan(s). 26 Describe how the participant feels. Example: Jack reports he is “feeling well and has no concerns.” Document what the participant says about his/her current living situation. Example: Susan reports she is “happy, healthy and enjoying her new apartment.” Record participant’s exact words to describe his/her health. Example: John reports he has a “dull headache” and it has lasted over a week. Document any mention of changes to his/her medications, diet, activity level, etc. Example: When Sarah went to visit her family doctor this week, he told her she had “high blood pressure and added a new medication.” 27 Document objective data including blood pressure and/or blood glucose readings, and findings from physical assessment (i.e., noticeable scraps or cuts, tearfulness, etc.). Example: TC checked Henry’s blood pressure log and found his last three readings were all within normal limits, 122/78, 120/76, and 122/80. 28 Document your interpretation of the subjective and objective findings. Example: Courtney met with a dietician last week to discuss how to follow a diabetic diet. Courtney stated an understanding and compliance with following a diabetic diet. However, her personal assistant reported that Courtney was eating a ½ gallon of ice cream weekly and drinking a 2L of pop daily. 29 Document plan on addressing assessment finding (address each abnormal finding). Example: Create food diary with Courtney and follow-up weekly. Take Courtney grocery shopping weekly and teach her how to read food labels and choose healthy foods. Report any issues or barriers to implementing this action plan. Example: The nearest grocery store with a variety of fresh fruits and vegetables is 45 minutes away. Document follow-up to action items. Example: TC re-visited Courtney a month later and found her blood glucose readings were consistently over 200 mg/dl. TC will arrange for Courtney to meet with her dietician and primary care provider to discuss strategies to improve diabetic management. 30 Ruth is a 47-year old female who has resided at We Care nursing facility for the past two years. Her admitting diagnosis was major depressive disorder, alcohol abuse and paraplegia. At the time of her admission, Ruth was involved in a motor vehicle accident while driving under the influence of alcohol. She was not taking any medications and consumed a 24-pack of beer weekly for 15 years. Ruth’s medical history includes hypertension, chronic liver disease, chronic renal disease, secondary hyperparathyroidism, hepatic encephalopathy, and paraplegia. She is taking eight different medications for her physical and mental health. She uses a motorized wheelchair for mobility. Ruth has stabilized at We Care and is excited about moving into her own apartment. 31 Physical Health Domain 32 Substance Abuse Domain 33 Interpersonal and Social Supports Domain 34 Functional Domain 35 Contact On: 8/24/14 Contact Type: Face-to-face contact Location: Participant Home Persons Contacted: Participant SOAP Note Subjective findings: Ruth stated, “I hate living here and want to move.” Objective findings: Ruth was tearful and in distress. Assessment findings: This is her first week living in her new apartment. Ruth has a history of depression and is prescribed Zoloft 50 mg in the evening. Her support system is sparse. She is connected with a community psychiatrist and counselor. Plan: Discuss what she likes and dislikes about her apartment. Develop strategies on how improve her current living situation. Inquire about medication compliance and substance abuse. Administer depression screening tool and compare findings to baseline results. Provide Ruth with a crisis hotline number. Offer to sit with Ruth while she calls her counselor, if needed. Offer to take Ruth on a community outing, if she desires. Follow-up with Ruth the next day via phone. 36 37 Questions? Please contact your UIC Pod Leader with any questions. UIC College of Nursing DRS Carla Tozer Brian O’Sullivan 312-996-7494 217-586-6039 ctozer2@uic.edu bosulliv@uic.edu DOA Valerie Gruss Ryan Reid 312-996-2193 217-586-6039 vgruss@uic.edu rdreid1@uic.edu 217-586-6039 DMH Dennis Crowley Mike Berkes Justin Wesley djcrowle@uic.edu mberkes2@illinois.edu jwesley1@uic.edu 217-586-6039 DDD Carrie Berger Justin Wesley Jason Immertreu cberger3@uic.edu jwesley1@uic.edu jimmer2@uic.edu 312-996-7643 38