CHAIRPERSON- Dr Prabhat K Chand
CO- CHAIRPERSON- Dr Manoj Kumar Sharma
PRESENTOR- Dr Virupakshappa Irappa Bagewadi
PSYCHODIAGNOSTICS:
‘CRUTCHES FOR CLINICIANS’
O UTLINE
INTRODUCTION
TESTS COMMONLY USED
EVIDENCE FOR SUPPORT
INDIAN PERSPECTIVE
CLINICIAN’S PERSPECTIVE
LIMITATIONS
CONCLUSION
I NTRODUCTION
I NTRODUCTION
Like other branches of medicine, PSYCHIATRIC practice,
needs diagnostic tests to supplement anamnesis and
clinical examination.
In clinical psychiatry, even more than elsewhere in
medicine, differential diagnosis is safer, if several tests are
available than if only one test is at our disposal.
Attempts at developing and clinically exploring psycho
diagnostic procedures can be a potent tool in exploring
organization and disorder of the personality.
[David Rapaport,1950]
I NTRODUCTION
Medical diagnosis
Psycho diagnosis
Framework of
physiology
Framework of
psychology.
[David Rapaport,1950]
P SYCHOMETRY
Psychometry has now evolved as study on theory &
technique of psychological measurements.
Includes measurement of knowledge, skills , abilities,
aptitudes, attitudes, intelligence, memory, creativity,
adjustment & personality.
Field uses – questionnaires, schedules, rating scales,
inventories & tests
[Venkatesan S. 2010]
P SYCHOMETRIC A PPROACHES
Relies on Normative approaches to psychological assessments.
Comparisons with a norm group enabled statistically based
diagnostic decisions .
In criterion referenced testing the scores relate directly to
individual competencies .
Behavioral assessments look into contemporary behaviors in
individuals and are directly linked to planning / implementing
for there remediation .
In recent times idiometric approaches to assessments is gaining
momentum based on search for underline common
denominators for overt behavioral deficits .
[Venkatesan S. 2010]
P SYCHOMETRY F OR C LINICIAN :
CLINIMETRICS
Introduced by Alvan R. Feinstein in 1982.
The purpose is to provide an intellectual home for a number
of distinct clinical phenomenon .
It includes
Types ,severity and sequence of symptoms;
Rate of progression of illness ,
Severity of comorbidity ;
Problems of functional capacity ;reasons for medical decisions
and many other aspects of daily life ,such as well being and
distress
Example : Apgar’s score
[Venkatesan S. 2010]
P SYCHOMETRY TO C LINIMETRY
TRADITIONAL
PSYCHOMETRY
CLINIMETRICS
Less sensitive to symptom
Sensitive
change
Less clinically coherent
–assess sx
based on their prevalence
Clinically coherent
Homogeneity of
Assess
More subjective
More
Cross sectional
Consider
components were given
importance
to symptom change
sx based on importance
of those sx to define severity
(weighting of sx)
objective
longitudinal course of
illness
[Venkatesan S. 2010]
P SYCHOLOGICAL T ESTS
P SYCHOLOGICAL T EST
C LINICAL RELEVANCE
It elicits, in a scientifically standardized manner,
responses which reveal psychological
characteristics in the patient being tested with a
high degree of statistical reliability and validity.
It includes obtaining samples of behaviour,
relevant to cognitive or affective functioning, and
for scoring and evaluation.
[Essentials of behavioral science]
W HY A RE A SSESSMENTS
D ONE ?
Screening & diagnosing
Treatment Planning
Functional Impairment/Severity
Subjective Distress
Social Support and Attachment Style
Reactant/Resistance Tendencies
Coping Style
Monitoring of Treatment Progress
Prognostic Indicators
D OMAINS O F T ESTS
Tests of Cognitive
Functions
Norm referenced tests of
memory, intelligence,
perceptual-motor functions,
Neuropsychological tests,
etc.
Tests of Personality
Projective tests and self
report inventories
Tests for Diagnostic
Clarification
Tests of concept formation
(thought deviance and
psychosis), projective tests,
inventories and rating scales
Other Tests
Developmental tests,
Aptitude tests, Psychoeducational tests and
Behavioral procedures
E XAMPLES O F C OMMONLY U SED
T ESTS I N A C LINICAL S ETTING
Cognitive Functions
• Memory-PGIMS,WMS
• Intelligence-BKT ,WAPIS, Bhatia, SPM,
VSMS
Personality & Inter
personality
• Projective –Rorschach IBT, draw a man
test, SCT, TAT
• Objective-16PF,MMPI
Diagnostic
Neuropsychological
assessment
• RIBT ,MPQ, OST,TAT
• Halstead –Reitan
• Luria
• Indian Batteries – PGI BBD,NIMHANS
C OGNITIVE F UNCTION
https://encrypted-tbn2.google.com/images
PGI M EMORY S CALE
Developed by Dwarka Prasad and N.N. Wig (1977)
10 subtests
Percentile norms
for 20 -45 years
Gives profiles for intervention
Indian norms available
In at least 5 subsets
Organics
Below 20th percentile
Psychotics Below 40th percentile
Controls
Between 40- 60
percentile
W ECHSLER ’ S M EMORY S CALE
(WMS)
Developed in 1940 at Belleuve hospital,New York
Norms available for 25-50 yrs
7 subtests
Gives a memory quotient (MQ) which is highly
correlated with IQ
B INET -K AMAT T EST
Includes both verbal and performance tests
3 -22 yrs, age level
Pattern analysis
Language
Reasoning
Conceptual thinking Memory
Social Intelligence
Visuo-motor…….etc.
Verbally loaded , difficult to assess if verbal function is
impaired
WAPIS-W ECHSLER A DULT
P ERFORMANCE I NTELLIGENCE
S CALE
WAPIS Indian adaptation of WAIS
[Ramalingaswamy, 1975]
Age: 15-45
Edu : min 5th std
B HATIA BATTERY OF PERFORMANCE
TESTS OF INTELLIGENCE
C.M. Bhatia-1942 -5 sub-tests
⌾
⌾
Kohs Block Design- discrimination of patterns
Alexander’s Pass along test- discrimination of movement of
concrete material
⌾
Pattern drawing test- analysis in terms of lines
⌾
Immediate memory- verbal memory
⌾
Picture construction- discrimination of picture parts
Norms- 11 to 16 yrs, literate and illiterate
PQ (performance quotient)
IQ (intelligence quotient)
Can not be used to assess MR
R AVEN ’ S P ROGRESSIVE
M ATRICES T EST
Has three versions
Advanced, Standard , Coloured.
Standard Progressive Matrices
(SPM), 60 problems divided into
five sets of A,B,C,D and E. Each 12
items in the order of progressive
difficulty.
It does not give IQ
It can be used in everyone
irrespective of culture, nationality,
age, education, physical condition
VSMS-V INELAND S OCIAL
M ATURITY S CALE
DR. Edgar A. Doll- 1935
Assesses 8 areas of development
Self-help general , Eating , Dressing , Direction
Occupation, Communication ,Locomotion ,Socialization .
0-25 yrs age level items
Done with the informants
Projective
Objective
[downloaded from https://encrypted-tbn2.google.com/images]
P ERSONALITY & I NTER
P ERSONALITY
Projective Techniques
Purpose is to gain insight into the individual personality
as a system
Rely to some degree on ambiguous stimuli and opaque
directions as catalysts for creating data.
The projective hypothesis
Ambiguous stimulus will reveal important aspects of
his or her personality
[Frank, 1939]
R ORSCHACH I NKBLOT T EST
Hermann Rorschach- 1910.
The test consists of ten ambiguous, symmetrical
inkblots, card appears as if a blot of ink was poured onto
a piece of paper and folded over—hence, the
symmetrical appearance.
These 6½ × 9½–inch inkblot cards are the standard
stimuli
Are referred by Roman numerals I to X.
Scoring
Location , Determinants ,Content , Popular, Form level
R ORSCHACH I NKBLOT T EST
Scoring Systems
Beck (1937) , Klopfer (1937),Pitrowski ,
Hertz ,Rapapport, Exner (1969)
Pathognomic Signs
Colour shock, Shading shock,
Perseveration.
Contamination, Confabulation,
Number responses
Behavioral responses like rejection ,
perplexity, automatic phrasing etc.
U SES O F R ORSCHACH
Main use differential diagnosis
and detecting early
schizophrenics
Other uses –
Detecting organicity : Pitrowsky’s
signs
Measuring hostility : Elizur’s
hostility scores
Screening psychopathology
Studying personality patterns
Evaluating treatment outcomes
Prognosis indication
U PS A ND D OWN O F
R ORSCHACH
At one time it was most
commonly used test for various
conditions including child
dispute, divorce etc
Validity of the result has been
questioned
Critically reviewed by
psychologists
Number of psychology school
have stopped using the test
T HEMATIC A PPERCEPTION T EST
Developed by Morgan and Murray 1935
A narrative projective device
21 Black & White cards of individuals
in classic human situation
Indian Adaptation by Uma Choudary10 cards & a blank card
Murray’s scoring (need aggression,
affiliation, affection)
Bellack’s Scoring
S ENTENCE C OMPLETION T EST
Semi projective technique by Sacks and Levy-1950
60 item test that assesses adjustment through 4
subscales
family, sex, interpersonal relationships and self concept
My father seldom…….(family)
When I see a man and woman together…..(sex area)
O BJECT
Kurt Goldstein , Martin Scheerer
-1941
Consists of 30 objects like
ribbon, bottle , needle, cloth etc
2 phases- active and passive
phase,
Responses -Common,
Impoverished, Peculiar
Measures thought deviance
SORTING TEST
M INNESOTA M ULTIPHASIC
P ERSONALITY I NVENTORY
Hathaway& Mckinley -1942
566 items, T /F, Cannot Say
10 Clinical scales
Hypochondriasis, Depression, Hysteria, Psychopathic
deviation, Paranoia..etc
4 Validity Scales (?, L, F, K)
Additional Scales – Ego Strength, Alcohol Scale
16 P ERSONALITY FACTOR T EST
Cattell-trait theory of
personality
Measures 16 functionally
independent dimensions
Age 16 & above
Form standardized and
used in India
N EUROPSYCHOLOGICAL
A SSESSMENT
Halstesd –Reitan Battery(1940)
Luria’s neuropsychological investigation
Frontal lobe lesion
10subtests
Criticized being not theoretical
More comprehensive
Based on theoretical principles
11 major cortical functions
Luria-Nebraska Neuropsychological Battery
Standardized luria’s test by Golden
N EUROPSYCHOLOGICAL
A SSESSMENT
INDIAN TEST BATTTERIES
PGI Battery of Brain Dysfunction(PGI BBD)- 5 subtests
PGI memory scale
WAIS Verbal scale
Bhatia’s short revised scale
Bender –Gestalt scale
Nehor & Benson scale
Gives a profile of 19 variables
NIMHANS Neuropsychological Battery
19 tests
W ISCONSIN C ARD S ORTING
T EST
David A. Grant and Esta A. Berg 1948
Used to test “set-shifting”
“Frontal" lobe functions
Executive function
Abstract thinking
R ATING S CALES
Help in diagnosis, functioning, symptom severity
and side effects
Domain
Scales
Functional status/
impairment
GAF, IDEAS
MOSSF 36
Side effect
AIMS,SAS
Psychiatric diagnosis
SCID,MINI,CIDI
Psychotic disorder
PANSS, BPRS
Mood disorders
HDRS,YMRS
Anxiety disorders
BAI
E VIDENCE F OR S UPPORT
D ESCRIPTION O F C LINICAL
S YMPTOMATOLOGY & DD
Test
Domain
Evidence
Neuropsychological test
Differentiating Dementia R-0.68
Brief
Screening brain
neuropsychological tests dysfunction
WAIS
Predicting a range of
criterion measures
R-0.57
MMPI
Descriptor of
personality
R--0.42
MMPI & MCMI -2
Depression
Good positive & negative
predictive power.
Good negative predictive
power
Schizophrenia
D ESCRIPTION OF C LINICAL
S YMPTOMATOLOGY & DD
Test
Domain
Evidence
Rorschach
Description of
symptomatology
R-0.37
Ego deficits
Impairment in social
and occupational
functioning
Rorschach
Schizophrenia Index
Diagnosing psychotic
disorders
Excellent Positive
predictive power
Rorschach & TAT
Problematic
interpersonal
relationships
Strong association with
clinical ratings
Interviews or informal
observation
Low accuracy
D ESCRIPTION AND P REDICTION
OF F UNCTIONAL B EHAVIOUR
Psychological assessments will predict functional behaviours
which have an effect on diagnosis, treatment and prognosis.
[Moras, 1997]
Tests of Cognitive Ability
Highly predictive of proficiency on the job and success in job
training
Strong utility as descriptors and predictors of academic
achievement
[Gottfredson, 1997]
Self-Report Personality Measures
Multi method assessment batteries better than single method
approaches to assessment.
[Robertson & Kinder, 1993]
M ENTAL H EALTH O UTCOMES
In children Baseline self reports of negative emotionality predict
behavior problems & subsequent clinical outcomes.
[Mattison et al1990]
In adults, baseline testing has determined that self-reported
neuroticism is a better predictor of long-term clinical outcome in
depression
[Hirschfeld et al1986]
In general, elevated baseline neuroticism scores predispose people
to negative outcomes in individual and marital therapy
[Luborsky et al1993]
Baseline assessment of hopelessness is the best predictor of
subsequent suicide
[Stewart, & Steer,1990]
A SSISTING I N T REATMENT
Patients with externalizing symptoms do better in
treatment that is more structured or directed by the
therapist
Patients with internalizing symptoms do better in
treatments where they set the pace and determine the
structure
[Engle & Mohr, 1993]
A SSESSMENT A S A T REATMENT
Patients receiving a 2-hour MMPI-2 assessment with
feedback reported symptomatic improvement compared
who did not.
[Finn and Tonsager 1992]
Personality testing can assist the formation of a "therapeutic
community" among men in inpatient treatment for severe
substance dependence.
[Moffett et al. 1996]
Personality testing also help to analyze and resolve
interpersonal difficulties that arise between difficult patients
and their therapists or treatment teams
[Berg 1988]
I NDIAN P ERSPECTIVE
S CENE I N I NDIA
Clinimetrics is of a recent origin in the country.
It is still in the process of establishing
Economical, cultural, educational, language & gender
differences contribute to the scenario of poor understanding
or acceptance of psychometry .
Despite these limitations and challenges ,the field of
clinimetrics has witnessed a periodic although unsteady or
patchy growth in mental health practice in the country.
[Venkatesan S. 2010]
D ISTRIBUTION O F R ESEARCH
A RTICLES I N I NDIA [ 1958-2009]
Year
Total Personality
Cognitive/organic
Diagnostic General
Total
<1970
339
6
1
1
2
10
1971-80
521
14
2
10
3
30
1981-90
705
2
2
16
2
22
1991-00
546
1
2
5
21
29
2001>
471
1
5
3
5
14
Total
2582 24
13
35
33
105
[Venkatesan S. 2010]
S CALES & I NVENTORIES U SED
I N I NDIA [1958-2009]
PERSONALITY
COGNITIVE
DIAGNOSTIC
RIBT
Luria nebraska NPA
Middlesex hospital Q Family interaction
patterns scale
Draw a person
Wisconsin card s
PGI health Q
SES Scale
Eysenck PI
BGT
Beck depression I
Parental handling
Maudsley PQ
PGI Memory
General health Q
Sex knowledge and
attitude scale
MMPI
Cattell’s infant IS
Hamilton depression Brief addiction
scale
rating scale
Bortner rating
scale for type A
peronality
Suicidal intent Q
16 PF Q
SANS
BPRS....
SOCIAL
Burden assessment
schedule...
A DVANCES I N A SSESSMENT
C OMPUTERS I N D IAGNOSIS
Computer soft wares are also utilized in a variety of ways.
To aid mental health professional in arriving at a psycho
diagnostic classification
To define psychiatric symptomatology terms, employ crossreferential diagnostic numbers to diagnostic categories,
and even refer the user to a specific page number
Ashton-Tate's dBase lll+ software was utilized and it was
found to be user friendly
[Stout & Scheramic, 1989]
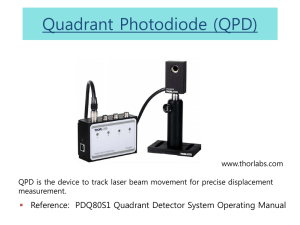
Q UICK P SYCHO D IAGNOSTICS
PANEL [QPD PANEL ]
Designed for primary care physicians.
It integrates easily into busy medical
clinics and provides valid diagnostic
information in a user-friendly format.
Fully automated.
Self-administered in 6.2 minutes using
portable, hand-held computer tablets.
The test screens for nine common
psychiatric disorders.
Physicians immediately receive a
computer-generated “lab report”
[Shedler Quick PsychoDiagnostics
Panel]
E VIDENCE F OR QPD
Criterion validity tested with Structured Clinical Interview
for DSM-IV
In 203 patients , not on treatment ,59 core questions, with
more than 200 questions
Diagnosis Sensitivity
Specificity
Kappa QPD
(PRE)
SCID
(PRE)
Major D
0.81
0.96
0.79
30
34.2
Gad
0.79
0.90
0.67
26.4
23.9
Panic
0.71
0.97
0.72
12.4
13.4
OCD
0.69
0.97
0.64
8.3
7.6
[Shedler et al 2000]
C ONVERGENT VALIDITY FOR
QPD
Sample ranging from 113 to 215
The QPD Panel depression scale correlated highly with
Beck Depression Inventory (BDI, r=.80)
Hamilton Depression Inventory (r=.87)
Center for Epidemiological Studies Depression (CESD) Scale(r=.79)
Zung Self-Rating Depression Scale (r=.78)
[Shedler et al 2000]
C ONVERGENT VALIDITY F OR
QPD
The QPD Panel anxiety scale correlated highly with
Spielberger State-Trait Anxiety Inventory (r=.67)
Anxiety subscale of the Symptom Checklist-90 (SCL-90)
(r=.76).
The QPD Panel somatization scale correlated highly
with
somatization subscale of the Symptom Checklist 28
(SCL-28), r=.59.
All correlations are statistically significant (Ps <.001)
[Shedler et al 2000]
U TILITY OF QPD
Sensitivity to Change
Patient Satisfaction
Physician Acceptance
Items
% Strongly agree
QPD R EPORT -S CREENING
[Shedler Quick PsychoDiagnostics
Panel]
QPD R EPORT -M ONITORING
[Shedler Quick PsychoDiagnostics
Panel]
R ECOMMENDATION TO C LINICIANS
E VALUATING A P SYCHOLOGICAL
T EST
Theoretical Orientation
Practical Considerations
Standardisation
Reliability
Validity
R ECOMMENDATIONS TO
C LINICIANS
Should use comprehensive, structured or at least semi
structured approaches to interviewing.
Should not only consider the data that supports their
hypotheses, but also carefully consider or even least evidence
that does not support their hypotheses.
This will likely reduce the possibility of hindsight and
confirmatory bias.
Diagnoses should be criteria based to minimise gender &
ethnicity bias
Should avoid relying on memory and refer to careful notes as
much as possible.
[Garb1998]
R ECOMMENDATIONS TO
C LINICIANS
In making predictions, clinicians should attend to base
rates as much as possible.
Should seek feedback when possible regarding the
accuracy and usefulness of their judgments.
Should learn as much as possible regarding the
theoretical and empirical material relevant to the person
or group they are assessing
Familiarity with the literature on clinical judgment
should be used to continually update practitioners on
past and emerging trends
[Garb1998]
C LINICAL VS A CTUARIAL
P REDICTION
The clinical approach used clinicians’ judgment,
Actuarial approach used empirically derived formulas, such as
single/multiple cut offs and regression equations, to come to
decisions regarding a client
Statistical decisions consistently outperformed clinical judgments
When the focus changes from institutional to individual decision
making, the relevance of statistical rules becomes less practical
Controlled studies generally favour a statistical approach over a
clinical one but, at the same time, that truth is seldom useful to the
practitioner involved in the changing and unique world of practice
[Hand book of psychological assessments 4th edition Gary Groth ]
C LINICAL VS A CTUARIAL
P REDICTION
Ideally, clinicians need to be aware of and to use, whenever
available, actuarial approaches such as multiple cut offs and
regression equations.
Future computer-assisted analysis of assessment results can
increasingly provide actuarial predictions especially from
multiple sources
Clinicians must recognize possible increases and decreases in
test interpretation and clinical judgment resulting from the
incremental validity of their instruments
Because more information does not necessarily increase the
accuracy of clinically based predictions
[Hand book of psychological assessments 4th edition Gary Groth ]
L IMITATIONS
L IMITATIONS
Although many studies have recommended these
assessments, the validity & reliability are low.
The test norms needs to be periodically revised .
Most of assessments are developed in western countries
which has to adapted for INDAN setting.
Non availability of well trained & experienced professional
limits the use of test.
Cost & time spent on testing may not be feasible for Indian
setting
C ONCLUSIONS
Tests can be used for screening, diagnosing, treatment
planning, monitoring & as prognostic indicators
Considerable empirical support exists for the validity of
psychological assessments
Psychological assessments may be viewed as analogues
to lab reports of other medical conditions.
While it is unlikely that actuarial prediction rules will
replace clinical judgment
Formal prediction rules can and should be used more
extensively as a resource to improve the accuracy of
clinical decision making
T HANK YOU
C ASE V IGNETTE
Mr P, 38 year old, married male, MBA, HSES, Mumbai (Settled in US for
past 16 yrs)
Pre morbidly sensitive & quick to temper with low frustration
tolerance,
Personal h/o ongoing marital discord,
Family h/o difficulties in relationship b/w pt & parents,
Past h/o thalassemia minor,
C/O difficulty in establishing emotional connections with people,
frequent change in jobs since the past 10 yrs, with h/o intermittent
bouts of irritability & withdrawn behavior since the past 8 months in
the back ground of severe marital discord. While in US the pt has
consulted 3 psychiatrists, at the insistence of his wife, who had
variously diagnosed him as adjustment disorder, paranoid
schizophrenia & PPD. The pt had come to NIMHANS
W HAT WOULD YOU LIKE TO DO ?
How would you like to proceed this case?
Would you refer this case for psychometry?
What areas would you assess?
What are the tests you would chose?
C OMMONLY USED
NEUROPSYCHOLOGICAL TESTS
Domain
Function
Test
Speed
Motor speed
Finger tapping
Mental speed
Digital Symbol
Substitution
Focussed
Colour trails
Sustained attention
Digit vigilance
Divided attention
Triads test
Verbal fluency
Controlled oral word
Category fluency
Animal names
Design fluency
Design fluency test
Working memory
N Back (verbal& visual)
Attention
Executive functions
C OMMONLY USED
NEUROPSYCHOLOGICAL TESTS
Domain
Function
Test
Executive functions
Planning
Tower of london
Set shifting
Wisconsin card sorting
Response inhibition
Stroop
Comprehension
Verblal
Token
Learning & memory
Verbal
Auditory verbal learning
Passages test
Visuo-spatial
construction
Learning &memory
Complex figure
Visual
Complex figure
Design learning test