Compassion Fatigue:
Healing the Heart-Renewing the Soul
by
Donna M. White RN, PhD, CS, CADAC
Fellow-Board Certified Expert in Traumatic Stress
Lemuel Shattuck Hospital, Boston, MA
Public Health Nursing Webinar
August 3, 2010
Copyright, D.White 2010
Acknowledgements
• New England Alliance for Public Health
Workforce Development
• Boston University School of Public Health
• Massachusetts Association of Public Health
Nurses (MAPHN)
Copyright, D.White 2010
Overview
The purpose of this workshop is to present the
profile of a Health Care Professional suffering
from Compassion Fatigue. The interactive
seminar will identify common stressors that
impact performance of professionals working in
Health Care. The learner will be given
methodologies to identify patterns of Compassion
Fatigue and strategies to promote Wellness,
Recovery and a renewed sense of identity as a
caring professional.
Copyright, D.White 2010
Learning Objectives
Upon completion of this session you will be able to:
• Identify three symptoms of Secondary Traumatic
Stress Disorder (STSD)
• Describe how Secondary Traumatic Stress
Disorder (STSD) and the sequelae Compassion
Fatigue, is a risk to Health Care Professionals
(HCP)
• List two Occupational Supports for Health Care
Professionals experiencing STSD.
Copyright, D.White 2010
Lemuel Shattuck Hospital
Copyright, D.White 2010
A dedication…
St. Francis of Assisi—Patron Saint of
Compassion
He relinquished a life of wealth &
chose a humble life to care for the
sick, the disenfranchised, the poor,
prisoners, and believed no one
should ever die alone at the end of
their earthly life.
Copyright, D.White 2010
Ever wonder…
•
•
•
•
•
Why you chose your profession?
Ever think about the rewards of it?
Why you continue even when exhausted?
Do you regret anything? Name it…
How often do you think about what you do
and the impact it has on who you are?
• How can you learn to “live softly”?
Copyright, D.White 2010
Health Care Professional
Prone to Compassion Fatigue
•
•
•
•
•
•
•
•
•
Heroic treaters
Intensely caring and concerned for others
High achievers
Strong academics - top ½ of their class
Dysfunctional home/early life
Highly competent
Excellent employee
Driven to succeed
Finds failure difficult
Copyright, D.White 2010
Cerney, 1995
Positions available
• Long hours with required overtime
• Must be available off-shifts,weekends, and
holidays
• Must be tolerant of aberrant behavior
• Must be willing to handle daily crises
• Emotionally draining and physically difficult work
• Sadness and tragedy seen often
• High degree of paperwork and responsibility
• Low salary that will increase after 20+ years
Copyright, D.White 2010
Occupational Signs of Stress
Biological:
• Bodily functions
• Physical symptoms
• Adverse physiological changes
Copyright, D.White 2010
Occupational Signs of Stress
Psychological:
• Decreased tolerance of others
• Low frustration ability
• Loss of humor and joy
Copyright, D.White 2010
Occupational Signs of Stress
Social:
• Withdrawal
• Isolation
• Loneliness
• Unable to complete tasks
• Poor utilization of social networks
• Negative patterns in supervision
Copyright, D.White 2010
So what is
happening?
Copyright, D.White 2010
Burnout…a patient cousin
Well intended aspirations evolve into
behaviors that can lay the groundwork for
burnout and possibly compassion stress and
other negative patterns in the workplace
Such as…
Copyright, D.White 2010
Negative factors
•
•
•
•
•
•
•
Decreased energy—”keeping up the speed”
Feelings of inadequacy, possibly failure
Reduced recognition for good work
High propensity towards feelings of guilt
Feelings of helplessness/powerlessness
Pressure to succeed-overachieve
Vulnerability to criticism
Copyright, D.White 2010
Negative factors…cont’d.
•
•
•
•
Inner-directed rage
Under-assertiveness
Feeling victimized
Inflexibility*—in professions that do not reward
flexibility
• Personality influences—perfectionism, rigidity
and an enormous capacity for an extreme
workload*
Red Cape Syndrome— “super-martyr”
Copyright, D.White 2010
Negative factors
• A strong work ethic, self-direction and idealism in
the workplace can spiral negatively without
supervision*
• Subsurface anger in HCPs equates to a sense of
powerlessness
• Horizontal violence-misdirected anger and subtle
sabotage towards others in their lives
• Highly critical and fault finding
Dropplemann & Thomas, 1996
Copyright, D.White 2010
Burnout…
“A state of physical, emotional and
mental exhaustion caused by long-term
involvement in emotionally demanding
situations”.
-Pines & Arnson, 1988
Copyright, D.White 2010
Stages of Burnout…
•
•
•
•
•
The Honeymoon -- Thank you so much!
The Awakening -- expectations are different
The Brownout -- self-confidence wanes
Full Scale Burnout -- open criticism
The Phoenix Phenomena -- you can get well
Maslach, 1985, et al
Copyright, D.White 2010
Burnout
The essence of the problem is not the
recognition of the feelings.
It is the clash between expectations and
reality.
Can emerge gradually…
Copyright, D.White 2010
A Conspiracy of Silence
• The work of Healthcare in this century is
physically exhausting and emotionally
daunting…caring for the seriously ill, the
dying, the wounded and the diseased.
• Effects on the provider are myriad
• Viewed as “just doing my job”
• Professional disciplines minimize their
contribution…
Finke, 2003
Copyright, D.White 2010
Figley’s Model of Compassion
Stress and Fatigue
Emotional
Contagion
Empathic
Ability
Disengagement
Empathic
Response
Empathic
Concern
Sense of
Achievement
Copyright, D.White 2010
Compassion
Stress
Blurring of roles
• Compassion stress has its roots in burnout.
• A sense of achievement can be known as a
“helper’s high”. The reward of the task
completion is greater for the professional
than the fulfillment of the need in the
person being cared for.
• Empathic responses can fuel continued
spiraling to fulfill the needs of others…
leading to exhaustion.
Copyright, D.White 2010
Cognitive Impact of
Secondary Traumatic Stress
• Diminished
concentration
• Confusion
• Spaciness
• Loss of meaning
• Decreased self-esteem
• Preoccupation with
trauma
• Trauma imagery
•
•
•
•
•
Apathy
Rigidity
Disorientation
Whirling thoughts
Thoughts of self-harm
or harm towards others
• Self-doubt
• Perfectionism
• Minimization
Copyright, D.White 2010
Emotional Impact of
Secondary Traumatic Stress
•
•
•
•
•
•
•
•
Powerlessness
Anxiety
Guilt
Anger-rage
Survivor guilt
Shutdown
Numbness
Fear
•
•
•
•
•
Helplessness
Sadness
Depression
Hypersensitivity
Emotional roller
coaster
• Overwhelmed
• Depleted
Copyright, D.White 2010
Spiritual Impact of
Secondary Traumatic Stress
• Questioning the
meaning of life
• Lack of selfsatisfaction
• Pervasive
hopelessness
•
•
•
•
Loss of purpose
Ennui
Anger at God
Questioning of prior
religious beliefs
Copyright, D.White 2010
Interpersonal Impact of
Secondary Traumatic Stress
• Withdrawn
• Decreased interest
in intimacy or sex
• Mistrust
• Impact on parenting
(protectiveness,
concern about
aggression)
• Projection of anger
or blame
• Intolerance
• Loneliness
• Isolation from
friends
Copyright, D.White 2010
Physical Impact of
Secondary Traumatic Stress
•
•
•
•
Shock
Sweating
Rapid heartbeat
Breathing
difficulties
• Aches and pains
• Dizziness
• Impaired immune
system
• Somatic reactions
Copyright, D.White 2010
Behavioral Impact of
Secondary Traumatic Stress
•
•
•
•
•
•
•
•
•
Clingy
Impatient
Irritable
Withdrawn
Moody
Regression
Sleep disturbances
Appetite changes
Nightmares
• Hypervigilance
• Elevated startle
response
• Use of negative coping
(smoking, alcohol or
other substance misuse)
• Accident proneness
• Losing things
• Self-harm behaviors
Copyright, D.White 2010
Crimean War…
“Their moans would pierce the heart”
-Irish Nurse
1864
Copyright, D.White 2010
PTSD Experiences
What Constitutes a Sufficiently Traumatic Experience:
The person has experiences an event outside the range
of usual human experience that would be markedly
distressing to almost anyone: a serious threat to his or
her life or physical integrity; serious threat or harm to
their children, spouse or other close relatives, or
friends; sudden destruction of his home or community:
or seeing another person seriously injured or killed in
an accident or by physical violence.
(APA, 1994)
Copyright, D.White 2010
Secondary Traumatic Stress
• STS is the natural consequent behaviors and
emotions resulting from knowing about a
traumatizing event experienced by another
human being. It is the stress resulting from
helping or wanting to help a traumatized or
suffering person.
(Figley, 1993a)
Copyright, D.White 2010
Vicarious Traumatization…
•Vicarious traumatization refers to a
transformation in the person’s inner
experience resulting from empathic
engagement with trauma material.
• Graphic accounts of abuse & pain
• Effects are cumulative & permanent
McCann & Pearlman, 1998
Copyright, D.White 2010
Vicarious Traumatization…
• Effects may be intrusive and painful
• Emotional residue may remain after direct
exposure
• Contamination of personal life
• Disruption of schema or beliefs about the
self and the world.
• Also called Transformational World View
Copyright, D.White 2010
Posttraumatic Embitterment
Disorder
• A distinct state of mood
• Differs from depression, hopelessness, and
anger… but can share common emotional features
or exist in parallel with them
• In contrast to anger…has additional quality of
self-blame and a feeling of injustice
• A feeling of being let down and is nagging and
self-increasing
• Person may feel vengeful but helpless.
Linden, Rotter, et al (2007)
Copyright, D.White 2010
I am not what happened to me.
I am what I choose to become.
Carl Jung
Copyright, D.White 2010
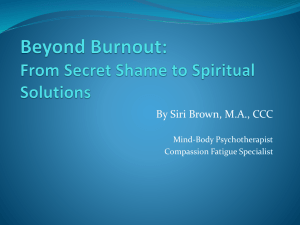
Figley’s Model of Compassion
Stress and Fatigue
Degree of Life
Disruption
Prolonged Exposure
Secondary
Traumatic Stress
Compassion
Fatigue
Traumatic
Recollections
Copyright, D.White 2010
Emotional and Spiritual Effects
Through exposure to graphic accounts
of abuse experiences, and the realities
of people’s intentional cruelty to one
another, a caring person is vulnerable to
the emotional and spiritual effects of
vicarious traumatization.
Copyright, D.White 2010
PTSD and STSD
PTSD
Stressor
• Outside of usual human experiences
Serious threat to self
Sudden destruction of one’s environment
• Re-experience of Trauma event
• Avoidance/numbing of reminders
• Persistent arousal
Copyright, D.White 2010
PTSD and STSD
STSD
Stressor
• Outside of usual human experiences
Serious threat to Traumatized Person
Sudden destruction of TP’s environment
• Re-experiencing Trauma Event of TP
• Avoidance/numbing of reminders
• Persistent arousal
Copyright, D.White 2010
Compassion Fatigue Defined
• Identical to Secondary Traumatic Stress
Disorder (STSD)
• Is the equivalent of PTSD
• Potential for chemical use
Figley, 1995
Copyright, D.White 2010
Clinical Practice Issues
• Loss of therapeutic realism
• Negative or non-existent supervision
• Personal health changes
• Self-neglect
• Transference/Countertransference
• Compassion Stress and Compassion
Fatigue
Copyright, D.White 2010
Clinical Practice Issues, continued
• Diminished interaction with colleagues and
team discipline
• Black/White-all or nothing thinking
• Emotionalism
• Judgmental behavior
• Use of chemicals for stress reduction (use,
abuse, dependence)
• Impaired Practice
Copyright, D.White 2010
Culture of the Workplace
Key marker for identifying issues for employee performance
and health maintenance
• Professional: established roles, clear policies and
protocols, supervision sessions, reasonable expectations
• Negative and Punitive…. “the bureaucratic response”
• Harried and rushed…...“a ticking clock”
• Fragmented and productivity driven… “just get it done”
• Team oriented vs. discipline specific…“that’s not my job”
• Poor reflection of specific cultures
• Chronic role strain
Copyright, D.White 2010
“You have brains in your head…You
have feet in your shoes. You can steer
yourself in any direction you choose!”
-Dr. Seuss
Copyright, D.White 2010
Key points for clinical practice
•
•
•
•
•
•
Supervision*
Boundary adherence
Self-awareness
Processing of events and emotions
Horizontal violence
De-obligate yourself
Copyright, D.White 2010
More stuff to know…
• The way you feel or behave is never caused by
others or the way they treat you.
• The way you behave is influenced by how you feel.
• The way you feel is created and controlled and
maintained by interpretations in your mind.
• Anything that was learned can be unlearned.*
• You can change the way you think!
• Getting reasonably upset instead of overly upset
can give you choice and control.
Managing Emotions Under Pressure, 2006
Copyright, D.White 2010
Methodologies for
Biopsychosocial Role Strain
•Personal Philosophy
•Support Groups
•Workplace Support (lunch time meetings, gyms,
spiritual areas, supervision luncheons, away days)
•Exercise programs
•Educational pursuits
•RTW (Return-to-Work) Contracts (when applicable,
established boundaries and parameters)
Copyright, D.White 2010
Healthy Strategies for Survival
• Assertiveness Training - Learning how to present
•
•
•
•
•
personal views without aggression
Health Promotion - Learning & self - health care
Adaptation - Goal surrender
Learning to “Roll with the Punches”
Cooperation - Affiliation “Social Glue” bonding
Develop emotional resilience
Copyright, D.White 2010
Healthy Strategies for Survival,
continued
• Recognition of competing—originates
in primal drives…food, power, sex
• Supervision - New techniques/new
perspective
• Continuous critical thinking
• Methodologies for role strain
Copyright, D.White 2010
More Healthy Strategies
•
•
•
•
•
•
•
•
Therapy—individual or group
Employee Assistance Program (EAP) consultation
Quiet/sacred areas “Take 5 Room”
Study groups
Yoga/exercise/good nutrition*
Stress e-mail forums
Stress reduction programs
Compassionate writing
Copyright, D.White 2010
Healthy Strategies…
•
•
•
•
•
•
•
•
Mental diversions—songs, movies, stories
Schedule vacations routinely
Alternative Therapies
Dining…not gulping food*
Pursue and interest—hobbies
Encourage recreation
Private time on a daily basis
Contact with family & friends
Copyright, D.White 2010
Ten Worry Stopping Techniques
• Set aside a special time for worrying. Concentrate only on
worrying during selected times.
• Ask yourself: “What is the absolute worst thing that may
happen?”
• Ask yourself: “Will that absolute worst thing really
happen?” How many times?
• Use “self-talk” and thought-stopping to short circuit
“worries.” STOP!
• Learn and use Scientific Conflict Resolution Techniques
for family and personal decisions. Resolve internal
conflict; reduce worrying.
Copyright, D.White 2010
Ten Worry Stopping
Techniques, continued
• Instead of imagining and re-imagining the negative, picture
what you ideally want to have happen. Imagine it and then
develop an action plan to begin to move toward that ideal.
• Learn to disagree agreeably. To protect …use I- messages
and active listening techniques, “I believe….discussion”
• Take a risk & ask questions…you can’t know everything!
• Read. Books and articles are available to teach yourself.
• Talk to those you trust… for their guidance
Accept reality…know the limits of your control…
The crisis will pass…with or without you being stressed
Copyright, D.White 2010
Stress Hardiness
• The concept of “stress hardiness” or resistance to
stress was developed by Dr. Suzanne Kobasa at
City University in New York.
• Dr. Kobasa has studied many groups of people
who have very stressful occupations. Those who
seem to cope with their job stress, having a
hardiness to it, have three specific characteristics.
• How do these apply to you?
Copyright, D.White 2010
3 Characteristics
of Stress Hardiness
• Commitment
• Control
• Challenge
Kobasa, 1979, 1985
Copyright, D.White 2010
Fourth “C”
• The fourth “C” stands for “closeness.”
• Everyone who wants to be stress hardy must
have someone (one person or one hundred)
with whom to share the stress, a confidante
who is willing to “be there” when times are
tough.
-Betty Morgan RN, PhD, CS
Copyright, D.White 2010
Positive Effects?…
“…a heightened sensitivity & enhanced empathy for
the suffering of victims, resulting in a deeper
sense of connection with others…a deep sense of
hopefulness about the capacity of human beings to
endure, overcome and even transform their
traumatic experience: and a more realistic view of
the world, through the integration of the dark sides
of humanity with healing images”.
McCann & Pearlman, 1990
Copyright, D.White 2010
Small Stuff
•
•
•
•
•
•
•
•
Choose your attitude every day
Listen with your ears…and eyes
Strive for integrity…not fame
Listen to your own advice
Think of the “Plane analogy”
Cherish tranquility
Rest without guilt
Learn to relax when you are “too busy”
Copyright, D.White 2010
and finally…..
“I want to know what sustains you from the inside
when all else falls away.
I want to know if you can be alone with yourself.
…and if you like the company you keep in the
empty moments”
-Oriah Mountain Dreamer
Indian Elder
Copyright, D.White 2010
References
• Cavaiola, A. & Colford, J. (2006) A Practical
Guide to Crisis Intervention, Boston: Lahaska
Press.
• Echterling, L.G., Presbury, H.H., & McGee, J.E.
(2005). Crisis intervention: Promoting resilience
and resolution in troubled times. Upper Saddle
River, NJ: Pearson
• Ferrell B., and Coyle, Nessa. (2007). The Nature
of Suffering and the Goals of Nursing. Oxford
University Press.
Copyright, D.White 2010
References
• Figley, C.R. Compassion Fatigue. New
York, Brunner/Mazel, 1995.
• Garfield, Charles. (1996). Sometimes My
Heart Goes Numb.
• Halpern, J. From Detached Concern to
Empathy: Humanising Medical Practice.
Oxford, Oxford University Press, 2001.
Copyright, D.White 2010
References
• James,R.K. (2008). Crisis intervention
strategies (6th ed.). Belmont, CA:
Brooks/Cole.
• Reynolds, W.J. The Measurement and
Development of Empathy. Aldershot:
Ashgate Publishing, 2000.
Copyright, D.White 2010
Thank you to all…
• To all of you here today for your interest and commitment to
your colleagues
• To all those present for their willingness to promote this
topic…discussion promotes wellness in ourselves and
ultimately, those we serve.
• Especially to the organizers
of today for their hard work
& tireless efforts to make
today happen for all of us.
Copyright, D.White 2010
QUESTIONS and ANSWERS
Donna M. White, PhD, RN, CS, CADAC
Contact via email:
donna.white@state.ma.us
Nursing Continuing Education credits are available for
30 days following the live presentation. In order to
receive your evaluation form and nursing contact hour
certificate please email your: name, state, email
address to: Patti White, MAPHN at
pattiwhite105@gmail.com
Copyright, D.White 2010