")
Strategies and Lessons from California’s MCAH
Five-Year Needs Assessment and
Implementation Plan
Maternal, Child & Adolescent Health Program
Center for Family Health
California Department of Public Health
Rocky Mountain Public Health Education Consortium, Albuquerque, NM;
Sept. 19, 2008
California’s Story – Presentation Outline
– Overview
• California’s Environment & Demographics
• MCAH Program
– Title V 2005 Needs Assessment
•
•
•
•
•
Framework
Guideline Development
Quantitative Indicators & Qualitative Analysis
Stakeholder Input & Capacity Assessment
Establishing Priorities
– Title V Implementation Plan
• Development Process
• Monitoring Progress
– Lessons Learned
• Recommendations
• Challenges
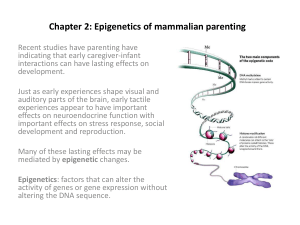
California Demographic Characteristics: 2006
•
State Projected Total Population
– Hispanic
– Non-Hispanic
• White
• Asian
• Pacific Islander
• African American
• American Indian
• Multi-Race
37.4 million
13.2 million (35%)
24.2 million (65%)
16.4 million (44%)
4.3 million (12%)
0.1 million (0.4%)
2.3 million (6%)
0.2 million (0.6%)
0.8 million (2.1%)
•
California Resident Women Births
– 13.3% of 2005 US Births
562,157
•
Births to Resident Hispanic Women
52% of total births
•
Paid by Medi-Cal
– Prenatal Care
– Delivery
46% of total births
47% of total births
•
Unintended Births to California Women
43%
Data Sources: State of California, Department of Public Health, 2006 Birth Records; Hamilton BE, Martin JA, Ventura SJ. Births: Preliminary data for 2005. Health E-Stats. Released
November 21, 2006; State of California, Department of Finance, Race/Ethnic Population with Age and Sex Detail, 2000–2050. Sacramento, CA, July 2007.; Maternal and Infant
Health Assessment (MIHA) Survey, 2005.
Modoc
Hu
mb
o
ldt
NDoer
tle
Siskiyou
California
Counties by
Urban &
Rural
Designation
Shasta
Lassen
Tehama
Plumas
doc
Rural
Glenn Butte
Sierra
a
a ad
ub ev c er
Colusa Y N
a
Pl
Lake
So
no
El Dorado
m Yolo Sacraor
a
a dra s Alpine
Napa
e
Am
mento
v
la
Ca
Solano
San
Contra
s Tuolumne
Marin
lau
osa
Mono
CostaJoaquin
nis
rip
a
a
t
M
AlamedSa
San Francisco
a
er
San Mateo
ad
Santa S
M
an
Clara Merced
Be
Santa Cruz
ni
Fresno
to
Mo
nt
er
ey
Tulare
Kings
Su
Men
Urban
ino
Trinity
r
tte
Rural counties are defined
by the state Rural
Health Policy Council
as having a population
of less than 250
persons per square
mile and do not
contain an
incorporated area with
a population greater
than 50,000.
San
Luis
Obispo
Santa
Barbara
Inyo
Kern
San Bernardino
Los
Ventura Angeles
Orange
Riverside
San Diego
Imperial
Live Births by County of Residence, 2006
California = 562,157 Resident Births
Source: 2006 Birth Statistical Master File
Prepared by: Maternal, Child and Adolescent Health Program, Center for Family Health, California Department of Public Health
LOCAL HEALTH DEPARTMENT MCAH PROGRAM
GENERAL PROGRAM ACTIVITIES
• All 61 Local Health Jurisdictions (LHJs) have MCAH programs
which serve women of reproductive age, infants, children,
adolescents and their families, especially low-income families
and individuals
• Assess and monitor the health status, needs and services
available to women and children, especially low-income
populations
• Provide community health programs that address a broad
range of topics
• Local MCAH agencies provide the CDPH MCAH Program
annual documentation of progress made on SOW objectives
and strategies
• Four Objectives included in the SOW
• Objective Four relates to development of an action plan at the
local level
Organization of the MCAH Division
Center for Family Health
Deputy Director
Catherine Camacho
Maternal, Child and Adolescent Health Division
Acting Division Chief
Shabbir Ahmad, DVM, MS, PhD
Assistant Division Chief
Les Newman
Program Standards
Chief
Policy Development
Chief
Anita Mitchell, M.D.
Karen Ramstrom, DO,
MSPH
Program Allocations,
Integrity, & Support
Chief
Fred Chow
Epidemiology,
Assessment, and
Program Development
Acting Chief
Mike Curtis, PhD
Human Stem Cell
Research & Cord
Blood Program
Chief
Shabbir Ahmad
Financial Management
& Contract Operations
Chief
Jo Miglas
California Birth Defect
Monitoring Program
Chief
Marcia Ehinger, M.D.
Maternal, Child and Adolescent Health Programs
(www.cdph.ca.gov/programs/MCAH/Pages/default.aspx)
1. Local Maternal and Child Health (MCH) Program - www.cdph.ca.gov/programs/LocalMCAH/Pages/Default.aspx
2. Birth Defects Monitoring Program – www.cbdmp.org or www.cdph.ca.gov/programs/CBDMP/Pages/default.aspx
3. Black Infant Health (BIH) - www.cdph.ca.gov/programs/BIH/Pages/default.aspx
4. Fetal Infant Mortality Review Program (FIMR) - www.cdph.ca.gov/programs/FIMR/Pages/default.aspx
5. Sudden Infant Death Syndrome (SIDS) - www.cdph.ca.gov/programs/SIDS/Pages/default.aspx
6. Comprehensive Perinatal Services Program (CPSP) - www.cdph.ca.gov/programs/CPSP/Pages/default.aspx
7. Regional Perinatal Programs of California (RPPC) - www.cdph.ca.gov/programs/RPPC/Pages/default.aspx
8. California Diabetes and Pregnancy Program (CDAPP) - www.cdph.ca.gov/programs/CDAPP/Pages/default.aspx
9. Breastfeeding Program (BFP) - www.cdph.ca.gov/programs/BreastFeeding/Pages/default.aspx
10. California Perinatal Quality Care Collaborative (CPQCC) - http://www.cpqcc.org
11. California Perinatal Transport System (CPeTs) - http://www.perinatal.org
12. California Perinatal Profiles - http://perinatalprofiles.berkeley.edu
13. Improved Perinatal Outcome Data Report (IPODR) – http://ipodr.org/ccpr.html or
www.cdph.ca.gov/data/indicators/Pages/InfantPerinatalOutcomesDataReport.aspx
Maternal, Child and Adolescent Health Programs
(www.cdph.ca.gov/programs/MCAH/Pages/default.aspx)
14. Local Maternal and Child Health (MCH) Program – www.cdph.ca.gov/programs/LocalMCAH/Pages/Default.aspx
15. Adolescent Family Life Program - www.cdph.ca.gov/programs/AFLP/Pages/default.aspx
16. Pregnancy Associated Maternal Mortality Review (PAMR) www.cdph.ca.gov/data/statistics/Pages/CaliforniaPregnancy-RelatedandPregnancyAssociatedMortalityReview.aspx
17. California Maternal Quality Care Collaborative (CMQCC) - www.cpqcc.org/
18. Advanced Practice Nurse Program 19. Human Stem Cell Research and Cord Blood Program - www.cdph.ca.gov/programs/HSCR/Pages/default.aspx
20. Nutrition and Physical Activity – www.cdph.ca.gov/programs/NutiritionandPhysicalActivity/Pages/default.aspx
21. Family Health Outcome Project (FHOP) www.cdph.ca.gov/data/indicators/Pages/FamilyHealthOutcomesProject(FHOP).aspx
22. Maternal Infant Health Assessment (MIHA) www.cdph.ca.gov/data/surveys/Pages/MaternalandInfantHealthAssessment(MIHA)survey.aspx
Maternal, Child and Adolescent Health Programs
(www.cdph.ca.gov/programs/MCAH/Pages/default.aspx)
23. Childhood Injury Prevention Program (CIPP) – www.cdph.ca.gov/programs/CIPP/Pages/default.aspx
24. Oral Health Program - www.cdph.ca.gov/programs/MCAHOralHealth/Pages/default.aspx
25. California Early Childhood Comprehensive System (CA-ECCS) www.cdph.ca.gov/programs/ECCS/Pages/default.aspx
26. Preconception Health and Health Care (PC) – www.cdph.ca.gov/programs/Preconception/Pages/default.aspx
27. Birth and Beyond California –
www.cdph.ca.gov/HealthInfo/healthyliving/childfamily/Pages/BirthandBeyondCaliforniaDescription.aspx
28. Adolescent Health Promotion
29. Perinatal Substance Use Prevention (PSU) www.cdph.ca.gov/programs/perinatalsubstanceuse/Pages/default.aspx
MCAH Work Philosophy
(http://ww2.cdph.ca.gov/programs/MCAH/Pages/default.aspx)
Data and/or Evidence
Information
Evaluation
Plan
Action
Maternal, Child and Adolescent Health Program
Center for Family Health, California Department of Public Health
Title V Needs Assessment &
Implementation Plan
Timeline
Compartmentalize Needs Assessment
State
Oversight of
the Process
61 Local
Jurisdictions
UCSF
Needs
Assessment
Quantitative
Qualitative
Analysis
Local & State
Stakeholders
Program
Administrators
Major MCAH Needs Assessment Components
•
Select Health Status Indicators by surveying local jurisdictions
•
Have local jurisdictions conduct a needs assessment
•
State Title V Agency summarize local level needs and priorities
– Provide summary to local jurisdictions and stakeholders
•
Analyze both local jurisdiction qualitative information and statewide
quantitative epidemiologic data
•
Assess State Title V Agency capacity
•
Involve external stakeholders, state administrators, and State Title V
agency staff in the prioritization of needs
•
Obtain public input on needs assessment report
•
Develop SPM to measure progress towards achievement of objectives
•
Provide feedback to local jurisdictions
•
Develop and monitor state level MCAH implementation plan
Conceptual Framework
• Decentralize statewide needs assessment process by
having each local jurisdiction conduct a needs assessment
•
61 local health jurisdictions
• Key Goals
1. Build local jurisdiction needs assessment capacity
2. Obtain extensive stakeholder input at the local level
3. Identify “needs” that may have been missed by only
analyzing statewide surveillance data systems
4. Focus local MCAH efforts by having each jurisdiction identify
2-7 priority areas they will focus on during the next five years
Needs Assessment Activity Timeline, 2003
MCAH
Comprehensive
list of potential
MCAH
indicators
Ranking of
MCAH
indicators by
local MCAH
jurisdictions
Aug
Nov
Guidelines for
local MCAH needs
assessment
(27 indicators)
FHOP provided local level MCAH data
FHOP provided training in needs assessment methods
MCAH Directors prepared local needs
assessment reports
Key:
MCAH Branch
Local MCAH
jurisdications
Dec
Apr
Sep
Oct
May
Jun
Jul
Jan
Feb
Mar
2003
Needs Assessment Activity Timeline, 2004
MCAH
MCAH Directors
FHOP reviewed
submitted local
local needs
FHOP provided local level MCAH data
needs
assessments for
assessment
completeness
report
FHOP provided training in needs
assessment methods
MCAH Directors prepared local needs
assessment reports
Key:
MCAH Branch
Local MCAH
jurisdications
Nov
Oct
Aug
Sep
Feb
Mar
Apr
May
Jun
Jul
Jan
2004
Dec
Summarized
local needs
assessments
Needs Assessment Activity Timeline, 2005
2005
MCAH
Jan Feb Mar
Apr
May
Jun
Statewide MCAH
Summarized local
Selection of seven
Stakeholder's
needs assessments
Title V priority needs
Meeting
Review of state-level indicators
Public comment
MCAH statewide capacity
assessment
Key:
MCAH Branch
Local MCAH
jurisdications
Jul
Submit Title
V Five Year
Needs
Assessment
Development of Needs Assessment
Guidelines to Local Health Jurisdictions
2005 Needs Assessment Guideline Development
• 2000 Statewide Needs Assessment criticized due to vague
guidelines resulting in local needs assessments that varied greatly
in structure and were difficult to summarize.
• 2005 local needs assessment guidelines written very specifically
and comprehensively in response to 2000 needs assessment
experience.
• Stakeholders involved in development of 2005 guidelines
–
–
–
–
State MCAH Epidemiology, Program and Policy Staff
Family Health Outcomes Project (FHOP)
MCAH Local Jurisdictions
MCAH Contractors (Adolescent Health, Injury, etc.)
• Consideration of Department of Health Services Strategic Plan
(2003)
• HP 2010 objectives
Local MCAH Needs Assessment
Guideline Components
1. Convene a planning group
2. Stakeholder input: consumers, local MCAH programs; providers;
health, social service and educational providers
3. Community Assessment
– Community health profile and resources assessment
– Review required and other health status indicators
– Assess local MCAH program capacity
4. Identify MCAH population needs
5. Identify 2-7 local MCAH priority areas
– Take into account local capacity to address identified needs
6. Conduct a preliminary problem analysis for one priority
Support Provided for Local MCAH
Needs Assessments
• Provide specific needs assessment guidelines with page limits
in order to ensure:
– Consistency of reporting format across jurisdictions
– Comprehensive local needs assessment process
– Prevention of extensive narrative reporting
• Provide training on conducting needs assessments and
ongoing technical support to local jurisdictions
– Support local level capacity
• Provide trend data to local jurisdictions for 27 health status
indicators stratified by race/ethnicity:
– Minimize local data collection/analysis burden
– Ensure standardized reporting
Training and Technical Assistance Provided to
Local Health Jurisdictions
•
FHOP provided training throughout the year to local health jurisdiction
staff:
–
–
–
–
Conducting a formal problem analysis
Conducting a community assessment
Developing objectives, performance measures and action plans
Etc.
•
FHOP developed a training book: “Developing an Effective MCH
Planning Process: A Guide for Local MCH Programs”
•
FHOP provided ongoing technical assistance to local health
jurisdictions on how to complete different components of the needs
assessment
–
–
–
–
–
How to do capacity assessment
Data analysis and interpretation assistance
Involving stakeholders
Developing and implementing surveys
Etc.
Quantitative Indicator Data Selection
• As part of their community health assessment, each
local health jurisdiction was required to review data for
27 different health status indicators.
• Selection of health status indicators local health
jurisdictions were required to review was based upon a
survey of jurisdictions.
– Jurisdictions were asked to rank the indicators they thought were
most important to assessing overall MCAH population health.
– Over 110 indicators were reviewed, the highest ranked indicators
were selected.
Examples of Quantitative Indicators
•
Birth
– # of births / fertility rates / teen birth rates
– Low, very low, and preterm births
•
Death
– Perinatal, neonatal, post-neonatal, and infant mortality
– Death rates (ages 1-14 years and 15-19 years)
•
Prenatal/Postnatal Care
– 1st trimester prenatal care initiation / Adequacy of Prenatal Care
– In-hospital exclusive breastfeeding
•
Injuries
– Hospitalization for non-fatal injuries (1-14 years, 15-24)
– Non-Fatal injuries due to motor vehicle accidents (1-14 years, 15-24)
•
Health
– Percent of children without health insurance / Percent without dental
insurance
– Percent of children who are overweight
– Asthma hospitalization rates
– Chlamydia rates for 15-19 year old females
– Hospitalization rates for mental health (5-14 year olds, 15-19 year olds)
Quantitative Indicator Data and Additional
Optional Data
• For each local health jurisdiction, FHOP computed tables
and graphs for 27 health status indicators.
– Data computed for the past 10 years and stratified by
race/ethnicity
– Compare local rate with a standard (HP 2010 and/or State rate)
• Jurisdictions were encouraged to review additional data
beyond the 27 indicators, including consideration of
other quantitative and qualitative data sources.
• Examples of additional topics include
– physical activity, immunizations, vaccine preventable diseases,
mental health problems, perinatal substance abuse, gestational
diabetes, oral health, and youth development.
GENERAL APPROACH TO THE ANALYSIS OF
QUALITATIVE DATA
• Narrative results from a needs assessment must be
summarized in a manner that can facilitate the
discussion of problems or priorities.
• Decisions should be made on:
• whether to code information based on predetermined
categories or based on themes developed from the dataset
• whether to code the literal reading of a transcript or make
inferences about what the author meant
Qualitative Data Coding
• The evaluation required multiple readings of each report
to reduce the likelihood of overlooking important
information.
• Coding was done for five areas across health
jurisdictions:
- type and number of participants involved in the planning process
- the types and the levels of community input,
- the sources of information used for identifying problems,
- the categories and subcategories of problems identified, and
- the categories and subcategories of named priorities.
Coding of Local Needs and Priorities
• “Problems” and “priorities” identified by local needs
assessments were coded separately
• Problems and priorities were coded two ways to
understand the nature of the problems
– General thematic areas (Substance Abuse, Mental Health, etc.)
– Specific sub-topics (perinatal substance abuse, adolescent
drug use, etc.)
• Local jurisdictions identified 122 specific problems, of
which 81 were identified by local jurisdictions as a
priority area
• “Access to Care” – 23 different specific topics
• “Breastfeeding” – 3 different specific topics
Example: Subtopics Within the Access to Care
Category
•
•
•
•
•
•
•
•
•
•
•
•
Lack of health insurance
Lack of transportation
Lack of bilingual professional staff
Lack of specialty providers
Access to health or dental care
Lack of nurses, physicians, dietitians, & dentists
Lack of providers in general
Cost of health care or health insurance
Complexity & bureaucracy of system
Lack of information or awareness of services
Language & cultural communication barriers
Lack of providers who accept Medicaid
Example Summary Spreadsheet: Access to Care
Sub-Topics Frequencies by Jurisdiction
Local Health Jurisdiction Stakeholder Participation
• Over 1,600 stakeholders participated in local needs
assessment meetings
–
–
–
–
–
–
–
City or county representatives
Social service agency representatives
Health care provider representatives
Elementary school administrators
University or college academicians
Local residents in the community
Other organization representatives
Supplemental Data Sources Used by
Local Jurisdictions to Identify Needs
• Secondary Research Data and Reports (500+ citations)
– Academic journals, state/federal agencies, interest groups
– Reports by other local health and social service groups
• Local Program and Jurisdiction Data (100+ citations)
– MCH program data, foster care placements, FIMR, etc.
• Local Surveys
– Over 5,000 individuals surveyed, such as school administrators,
clients, providers, and family members
State Level Stakeholder Input in
Setting Statewide MCAH Priorities
Capacity Assessment
Statewide External Stakeholder Meeting
• Over 50 representatives from state, local and private
agencies were invited, 37 organizations attended.
– State Agencies, Local Health Jurisdictions, Provider Groups,
Consumer Groups, MCAH Programs, Academic Institutions
• Stakeholders were asked to review prior to the meeting
– Summarized results of local MCAH jurisdiction priorities
– Statewide epidemiological data
Stakeholders Invited to Statewide Needs
Assessment Meeting
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Adolescent Family Life Program
American Academy of Pediatrics
American College of Obstetricians and Gynecologists
Birth Defects Monitoring Program
Black Infant Health Program
California Adolescent Health Collaborative
California Conference of Local Health Officers
California Dental Association
California Family Health Council
California Healthcare Foundation
California Hospital Association
California Nursing Association
California Perinatal Quality Care Initiative
California Public Health Association
California Department of Alcohol and Drug Programs
California Dept. Developmental Services
California Department of Education
California Department of Mental Health
California Department of Rehabilitation
California Department of Social Services, Children and
Family Services Division
Center for Healthier Children, Families and
Communities, UCLA
Center for Injury Prevention Policy and Practice; SDSU
Charlotte Maxwell Newhart & Associates
Child Death Review Team
Children Now
Dept. of Family & Community Medicine, UCSF
Domestic Violence Programs Epidemiology and Prevention
for Injury Control Branch
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Epidemiology and Prevention for Injury Control Branch
Fetal & Infant Mortality Review Program
First Five Commission
Genetic Diseases Branch, CDPH
Immunization Branch, CDPH
Indian Health Program, DHCS
Institute for Health Policy Studies, UCSF
Kaiser Family Foundation
March of Dimes, California
MCAH Action Executive Committee
Medi-Cal Dental Services, DHCS
Medi-Cal SCHIP, DHCS
Office of AIDS, CDPH
Office of Family Planning, CDPH
Office of Multicultural Health, CDPH
Office of Women’s Health Advisory Group
Office of Oral Health, CDPH
Pacific Business Group on Health
Planned Parenthood
Primary & Rural Health Care System, CDPH
Regional Perinatal Programs of California Directors
Sexually Transmitted Disease Control Branch, CDPH
School of Public Health, UC Berkeley
State Council on Developmental Disabilities
Sudden Infant Death Syndrome Program
The ARC of California
Women, Infants and Children Supplemental Nutrition
Branch, CDPH
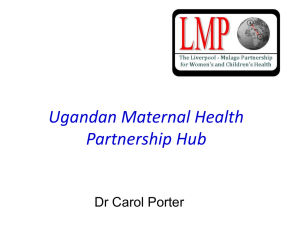
Criteria Developed by Stakeholder Group to
Rank Priorities
• Stakeholders reviewed a list of possible criteria upon
which to rank priorities and selected the following:
–
–
–
–
–
Problem has serious health consequences
Large number of individuals affected
Problem results in significant economic/social costs
Problem is cross-cutting across multiple issues
Problem has disparities across sub-groups
• Each of the above criteria received a weight established
collectively by the stakeholders
O
ut
co
m
ce
ss
to
Ca
re
we
igh
t
rth
s
1,172
en
at
Ch
al
la
Ca
m
yd
re
ia
In
fe
ct
ion
s
O
ra
lH
ea
Br
lth
ea
stfe
ed
in
g
Pr
1,196
Bi
1,200
Te
en
1,219
Vi
ol
en
ce
a
1,333
th
m
1,348
es
t ic
1,375
As
1,400
Do
m
1,451
es
/M
or
ta
lit y
M
en
ta
lH
Su
ea
bs
lth
ta
nc
e
Un
Ab
in
us
te
nt
e
ion
al
In
ju
rie
s
Bi
rt h
ve
r
1,600
Ac
O
MCAH Needs Assessment Stakeholder
Meeting Ranking Results
1,331
1,169
1,000
1,156
1,097
1,009
931
800
600
400
200
0
State Title V Agency Capacity Assessment
• State Title V Agency conducted internal capacity
assessment
• CAST-V Tool used for assessment
• Managers and senior staff participated in the process
• Results listed by “strengths” and “weaknesses/areas for
improvement” for each of the 10 Essential Public Health
Services
California MCAH Priority Setting
Local MCAH
jurisdiction input
MCAH
Priorities
Quantitative
analysis of
statewide epidemiologic data
Stakeholder
input
State MCAH Program, Policy &
Epidemiology Staff Input
Administrative/Fiscal/Political Considerations
Capacity
Duties fulfilled by other departments
and agencies
Case Study 1: Perinatal Substance Abuse
• Data on perinatal substance use was very limited and no data was
provided to local jurisdictions. Perinatal substance abuse,
however, was one of the most common problems and priorities
identified. Many jurisdictions relied on qualitative data sources.
• Data Sources used by Local Jurisdictions
– Provider surveys
– Foster care placement information
– Key informant interviews / Stakeholder input
Case Study 2: Pregnancy-Related Mortality
• Pregnancy-related mortality was one of the most rare
events at local level.
• Pregnancy-related mortality surfaced as one of the
priority for state MCAH program based largely upon
quantitative analysis of statewide trends.
• Data Sources used by State
– Death records
– Linked birth - death – hospital patient discharge dataset
2006-2010 MCAH Priorities
•
Enhance preconception care and work toward eliminating disparities in infant
and maternal morbidity and mortality.
•
Promote healthy lifestyle practices among MCAH populations and reduce the
rate of overweight children and adolescents.
•
Promote responsible sexual behavior to decrease the rate of teenage
pregnancy and sexually transmitted infections.
•
Improve mental health and decrease substance abuse among children,
adolescents, and pregnant or parenting women.
•
Improve access to medical and dental services, including the reduction of
disparities.
•
Decrease unintentional and intentional injuries and violence, including family
and intimate partner violence.
•
Increase breastfeeding initiation and duration
Development of California’s MCAH
Title V Implementation Plan
(July 2005 – October 2007)
Maternal, Child & Adolescent Health Division
Center for Family Health
California Department of Public Health
California Title V Implementation Plan
Acknowledgements:
• CDPH, MCAH Division Leadership
–
–
•
CDPH, MCAH Division IP Steering Committee:
–
–
–
–
–
–
–
–
–
•
Susann J. Steinberg, MD (retired)
Shabbir Ahmad, DVM, MS, PhD
Kate Marie, MPA (Chair)
Angela Furnari, RN, PHN, MPA
Janet Hill, MS, RD
Lori Llewelyn, MPP
Anita Mitchell, MD
Kathleen Nettesheim-Engle, MPH, RN
Karen Ramstrom, DO, MSPH
Leona Shields, PHN, MN, NP
Eileen Yamada, MD
University of California San Francisco, Family Health Outcomes Project
–
–
–
–
Judith Belfiori, MA, MPH
Brianna Gass, MPA
Geraldine Oliva, MD, MPH
Jennifer Rienks, PhD
Developing an Action Plan
External
Environment
Should
Do
Organizational
Values, Culture,
Leadership
Wants
To Do
Internal
Environment
Can
Do
Strategy of the Organization
Focused Strategic Thinking; AC Rucks; University of Alabama Birmingham
Developing a Plan:
Oral Health Example
• External Environment (Should Do):
– Data:
• By third grade, over 70% of children have a history of tooth decay
• By age 2, only 1 in 10 children had any kind of preventive dental visit
• Fewer than 1 in 5 pregnant women have received any dental services
– Oral Health Stakeholders and Partners:
• Proposed additional IP objectives and strategies
– Greater use of case management with regard to maternal and
children's’ oral health
– Establish a Dental Health Advisory Committee to the MCAH Division,
encourage local MCAH programs to do the same
• Organization Values, Culture & Leadership (Want to Do):
– Improve access to dental services for MCH population
– Reduce disparities
• Internal Environment (Can Do)
– Fiscal constraints limit assistance available at state and local level
– Build strong collaborations with other state and advocacy groups to address
oral health issues specific to MCH population
Development of the
Title V Implementation Plan
Ten priority goals identified for 2006-2010
– Seven Priority Goals – Maternal Child Adolescent Health
Division
– Three Priority Goals – Children’s Medical Services
Implementation Plan
• Focus on State MCAH Program role with regard to the identified
priorities and supporting needs at the local level
• Builds on existing and emerging efforts
• General direction to be taken by the State MCAH Division during
the Title V 2006 – 2010 grant cycle
2006-2010 MCAH Program Priorities
(biphasic process)
Priorities Addressed in State Fiscal Year 2006-2007
•
•
•
•
Enhance preconception care and work toward eliminating disparities in
infant and maternal morbidity and mortality.
Promote healthy lifestyle practices among MCAH populations and reduce
the rate of overweight children and adolescents.
Improve mental health and decrease substance abuse among children,
adolescents, and pregnant or parenting women.
Increase breastfeeding initiation and duration (make breastfeeding the
norm).
Priorities Addressed in State Fiscal Year 2007-2008
•
•
•
Promote responsible sexual behavior to decrease the rate of teenage
pregnancy and sexually transmitted infections.
Improve access to medical and dental services, including the reduction of
disparities.
Decrease unintentional and intentional injuries and violence, including
family and intimate partner violence.
Developing an Action Plan
Understanding
the Situation
Planning
the Strategy
Planning the
Implementation
Planning
the Control
External
Environmental
Issues
Internal
Environmental
Issues
Vision,
Mission,
Values
Strategy Formulation
Goal Development -- Strategic Direction
Implementation of the Plan
Develop Specific Actions – Specify Time Priority
Control of the Plan
Setting Measures – Budgeting – Recycling the Plan
Focused Strategic Thinking; AC Rucks; University of Alabama Birmingham
Development of Implementation Plan
Process
Internal Planning
Meetings
MCAH Management and
Program Supervisors’
Input
On-site meetings with
local MCAH
representatives
Input from MCAH County
Health Directors
Statewide MCAH
Stakeholder meeting
Review and input from
recognized MCAH
experts
Public input via webbased posting
MCAH Implementation
Plan
Implementation Plan -Understanding the Situation
• Input from MCAH Program Managers
– Need to know where you’ve been in order to plan where
you’re going
• Local Health Jurisdiction’s Input
– Identified evidence based or successful program models
that address TV priority area(s)
– Discussed barriers to implementation; how barriers were
addressed; and any problems or unresolved issues with
these programs
Implementation Plan Planning the Strategy
• MCAH Action Committee Input
– Review & input from local MCH Directors
• Statewide Stakeholder Meeting
– Representatives from 48 government, research, and
community-based organizations
State of California-Health and Human Services Agency
Department of Health Services
January 31, 2007
TO:
TITLE V STAKEHOLDERS
SUBJECT: TITLE V MATERNAL, CHILD AND ADOLESCENT HEALTH
FIVE-YEAR IMPLEMENTATION PLAN (PHASE II)
STAKEHOLDERS’ MEETING
I invite you to participate in a meeting sponsored by the California Department of Health
Services (CDHS); Maternal, Child and Adolescent Health/Office of Family Planning
(MCAH/OFP) Branch to review and discuss implementation objectives and strategies
for priorities identified through the 2005-2006 Title V Needs Assessment. Your input will
contribute to the five-year implementation plan that will be submitted this July as part of
California’s 2007-08 Title V Maternal and Child Health Block Grant application. The
meeting will be held on Tuesday, March 20, 2007, from 10:00 a.m. to 4:00 p.m., in
Sacramento, and will be facilitated by the Family Health Outcomes Project of the
University of California, San Francisco.
Title V Implementation Plan –
Participating Stakeholders
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Adolescent Health Collaborative
California Conference of Local Health Officers
California Department of Alcohol and Drug
Programs
California Dept. Developmental Services
California Department of Education
California Department of Mental Health
California Department of Rehabilitation
California Family Health Council
California Hospital Association
California Perinatal Quality Care Collaborative
California Public Health Association South
Center for Injury Prevention Policy and Practice;
SDSU
Center for Positive Prevention Alternatives
Child & Health Permanency, Department of Social
Services
Children's Medical Services Branch, DHCS
Chronic Disease and Injury Control, CDPH
Dept. of Family & Community Medicine, UCSF
Family Health Outcomes Project, UCSF
FASD Advocacy Group, The Arc of California
Fetal & Infant Mortality Review Program
Genetic Diseases Branch, CDPH
Health Initiatives for Youth
Immunization Branch, CDPH
Indian Health Program, DHCS
Institute for Health Policy Studies, UCSF
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
LA Best Babies Network
March of Dimes, California
Maternal, Child and Adolescent Health Program
Office of Family Planning Branch, CDPH
MCAH Action Executive Committee
MCH-Contra Costa County
Medi-Cal Dental Services, DHCS
Medi-Cal Eligibility, DHCS
Medi-Cal Policy, DHCS
Obstetrics, Gynecology & Reproductive Sciences:
UCSF
Office of AIDS, CDPH
Office of Oral Health, CDPH
Office of Perinatal Substance Abuse, California
Department of Alcohol and Drug Programs
Primary & Rural Health Care System, CDPH
Refugee Health Section; CDPH
Regional Perinatal Programs of California
Sexually Transmitted Disease Control Branch,
CDPH
State & Local Injury Control Section, CDPH
State Council on Developmental Disabilities
Sudden Infant Death Syndrome Program
Sutter Medical Center
WEAVE, Inc
Wellstart International
Women, Infants and Children Supplemental
Nutrition Branch, CDPH
Stakeholder Meeting
Criteria for Evaluating Strategies
The strategy/intervention …
•
•
•
•
•
•
is evidence-based and/or promising
can be implemented in different size counties with
modification or assistance (broadly applied);
is cost effective (based on research);
addresses Federal and State priorities for reducing
health disparities;
is supported by “political will”;
provides collaboration opportunities across State
and/or local agencies and programs
Priority Goal 3: Promote responsible sexual
behavior in order to decrease the rate of teenage
pregnancy and sexually transmitted infections.
Objective 3.2 – Increase the sexual health knowledge and counseling skill level of providers and
professionals providing family planning and reproductive health services to teens.
3.2.1 Create a comprehensive outline of
knowledge, abilities and skills
necessary to be an effective and highly
qualified educator, counselor, or case
manager in the area of adolescent
sexual health.
3.2.2 Disseminate core competencies
applicable to a wide range of
professionals for providing sexual
health education and counseling
services to adolescents and young
adults consistent with best practices for
effective interventions and appropriate
to age and ethnicity.
3.2.3 Develop a comprehensive and
appropriate training based on the core
competencies. Explore the need for the
development of a certification program
for defined categories of counselors
Evidencebased
Broadly
Applied
Cost
Addresses Political
Effective Disparities
Will
Collaborative
Opportunities
Stakeholder Identified
Cross Cutting Objectives
• MCAH key program components integrated
throughout all programs
– Preconception Health
– Breastfeeding
– Nutrition & Healthy Lifestyles
– Oral Health
• Eliminate health disparities
• Promote cultural and linguistic competence in MCAH
programs and staff
Implementation Plan –
Planning the Strategy
• Review and input by recognized leaders/experts in
MCAH
– Is the information accurate?
– Are there additional activities that are feasible given
limited resources?
– Are there any glaring omissions?
• Web-based posting for public input
– Notice sent to MCAH stakeholders, directors and
program coordinators
Implementation Plan – Overview Maternal
Health
Implementation Plan – Case Study
Maternal Health
• Maternal Quality Indicator Workgroup (2001)
– Assess current levels of maternal morbidity in California and
– Develop valid indicators in order to measure trends in maternal outcomes where
local and statewide projects have been initiated to improve maternal health.
• CA-Pregnancy-Associated Mortality Review (2004)
– Identify and review deaths of women during pregnancy and childbirth
– Deaths of African American women are over-sampled in order to gain insight into
maternal health disparities.
• CA Maternal Quality Care Collaborative (2006)
– Improving maternal health through data driven quality improvement
– Determine possible opportunities for prevention
• Hemorrhage Task Force
• Maternal Quality Improvement Panel
– Provide recommendations to reduce future morbidity and mortality
• Local Assistance for Maternal Health (2008)
– Improve prevention of, recognition of, and response to maternal morbidities and
obstetrical emergencies
– Improve accuracy and usefulness of administrative data
– Reduce fragmentation of maternity care
– Inform and educate the public and families about maternal issues related to reducing
morbidity and mortality
Post Implementation Plan Programmatic Changes
• Preconception Care Council of California (Priority
Goal 1)
– Forum for statewide planning and decision-making on issues
and programs related to preconception health and health care.
– Convener of the Second National Preconception Care Summit,
October 2007
• Perinatal Substance Abuse Prevention Efforts
(Priority Goal 4)
– California Fetal Alcohol Spectrum Disorders Task Force
– State Interagency Team Workgroup on Alcohol and Other Drugs
– Perinatal Substance Use Screening Data Report by Dr. Ira
Chasnoff
• Projected publication release: Summer 2008
• Breastfeeding Promotion (Priority Goal 10)
– Encourage Baby Friendly Hospitals
Title V Implementation Plan:
Monitoring Progress
Are we there yet?
Implementation Plan –
Planning the Control
• National and State Title V performance and outcome measures
monitor progress on state priorities
– Intermediary measures of change needed
• Documentation of progress made on objectives and strategies
following the Phase I Stakeholder Meeting
– Inform stakeholders about progress in preparation for
Phase II Stakeholder Meeting
– First step for developing means to monitor progress
• Ongoing monitoring of Title V implementation plan
– Developing a process
– Build into how we do day-to-day business
State Performance Measures
To measure progress toward achievement of objectives
SPM #3. Percent of women (18-44 years) who reported 14 or more “not good” mental
health days in the past 30 days.
SPM #4. Percent of women who reported drinking any alcohol in the 1st or 3rd trimester
of pregnancy.
SPM #5. Rate of deaths per 100,000 adolescents (15-19 years) caused by motor vehicle
accidents.
SPM #6. Incidence of neural tube defects (NTDs) per 10,000 live births plus fetal
deaths among counties participating in the California Birth Defects Monitoring System.
SPM #8. Percent of births resulting from an unintended pregnancy.
SPM #9. Percent of 9th grade students who are not within the Healthy Fitness Zone for
Body Composition.
SPM #10. Percent of women reporting intimate partner physical, sexual, or
psychological abuse in the past 12 months.
SOM #1. The pregnancy-related mortality rate per 100,000 live births.
MCAH Priority Areas and Corresponding
Performance Measures
Priority
National
Performance
Measure
State
Performance
Measure
Enhance preconception care and work toward
eliminating disparities in infant and maternal
morbidity and mortality.
01, 15, 17, 18
06 (and SOM 01)
Promote healthy lifestyle practices among MCAH
populations and reduce the rate of overweight
children and adolescents.
14
09
Promote responsible sexual behavior to decrease
the rate of teenage pregnancy and sexually
transmitted infections.
08
08
Improve mental health and decrease substance
abuse among children, adolescents, and pregnant or
parenting women.
16
03, 04
Improve access to medical and dental services,
including the reduction of disparities.
01, 04, 07, 09, 12,
13, 17, 18
Decrease unintentional and intentional injuries and
violence, including family and intimate partner
violence.
10, 16
Increase breastfeeding initiation and duration.
11
05, 10
Health Status
Indicator
01, 02
05
03, 04
Monitoring Title V Implementation Plan Progress
• Local Health Jurisdiction Activities
– Capture how local activities support our state level objectives
and strategies
• MCAH Division Internal Monitoring
Monitoring Title V Implementation Plan Progress
– Local Health Jurisdictions
• Track local health jurisdictions activities in a uniform way
– Identify activities through LHJ annual reports
– Utilize MCH pyramid of services to capture information
• Utilize information to integrate evaluation and program
planning
– Identify best or promising practices
– Identify challenges/barriers faced
– Provide technical assistance back to LHJs
• Capture anecdotes about MCAH programs (infrastructure
challenges, accomplishments)
– Inform Legislators; guide policy discussions
Monitoring Title V Implementation Plan Progress
2008 INDEX- Local Annual Report
Instructions: Type "1" if the health topic is covered in their report and "0" if not covered in the report. DO NOT type "Yes" or "No" in
the box; typing "1" automatically converts to "Yes" and "0" converts to a "No" response in the grid.
COUNTY/ Health
Topic
Infant
Morbidity/
Mortality
Preconception
Care
D
H
C
E
S
P
B
S
I
B
D
H
C
E
S
P
B
S
Maternal
Morbidity/
Mortality
I
B
D
H
C
E
S
P
B
S
Obesity/
Nutrition/
Physical
Activity
Obesity
I
B
D
H
C
E
S
P
B
S
I
B
D
H
C
E
S
P
B
S
Childhood
Injury
Prevention
Smoking/
Substance Use
I
B
D
H
C
E
S
P
B
S
I
B
D
H
C
E
S
P
B
S
I
B
Alameda
Alpine
Amador
Berkeley
Mental Health
Breastfeeding
Teen Pregnancy
Access to
Medical Care
STD
Oral Health
Injury/ Violence
D
H
C
E
S
P
B
S
I
B
D
H
C
E
S
P
B
S
I
B
D
H
C
E
S
P
B
S
I
B
D
H
C
E
S
P
B
S
I
B
D
H
C
E
S
P
B
S
I
B
D
H
C
E
S
P
B
S
I
B
D
H
C
E
S
P
B
S
I
B
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
Alameda
Alpine
Amador
Berkeley
TOTAL
DHC=Direct Health Care Services; ES=Enabling Services; PBS=Population-Based Services; IB=Infrastructure Building Services
Monitoring Title V Implementation Plan Progress
Monitoring Title V Implementation Plan Progress –
MCAH Division Internal Monitoring
• Monitor Internal Progress on Title V Implementation Plan
Activities
– Develop tool to document Title V Priority area activities
– Draft format includes: priority goal, objective, strategies, team,
activities, resources, process measures and short and
intermediate outcomes
• Next Steps:
– Pilot test the tool
– Finalize the format and process for use
– Assess indicator data for each priority area
– Revisit objectives/strategies and identify revisions needed
Recommendations for 2010 Needs Assessment
Recommendations
•
Needs assessment efforts in large states need to be decentralized.
•
Clear, concise guidelines need to be provided to local jurisdictions
•
Emphasize the need for local jurisdictions to obtain stakeholder input.
•
Technical assistance, training, and data need to be provided to local jurisdictions.
•
Qualitative analysis of local needs assessment data should organize the needs/priorities
by both general subject areas as well as specific sub-topics. Both levels of information
are important.
•
Most priority areas are inter-related. Use the needs assessment process to bring
together other state departments. Areas of common interest will be identified among all
stakeholders and collaborative efforts will be strengthened.
Lessons Learned
•
Small jurisdictions may find the needs assessment hard to complete. We will be
assessing our guidelines to identify areas to delete while still ensuring the needs
assessment is comprehensive.
•
Enhance analysis of local level MCAH capacity and report findings back to jurisdictions.
2010 Five Year Needs Assessment
Capacity Assessment
• Discussion started in September 2007
– Modified CAST-V
– Assess Local Health Jurisdiction Capacity
• Guidelines released in May 2008
– For 2010 Five-year Needs Assessment
– Available online at:
http://www.cdph.ca.gov/programs/MCAH/Documents/
MO-TitleVGuidelinesForLocalNeedsAssessment11a.pdf
Title V
Five Year Needs Assessment
and Implementation Plan
are indeed
CONTINUOUS PROCESSES
(The cycle started in Jan 2003 and ended in Oct 2007)
Challenges…
• Staff Turnover
• Fiscal Constraints
• Department Reorganization (planning started in Jan 2006)
• Development of efficient process
– Takes into account existing process
– Feeds into Implementation Plan progress
• Keeping Stakeholders informed on the progress made
Must Haves…
• Support of Management/Leadership
• Right people at the table
– Engage staff in the process
• Structured but flexible process
– Open lines of communication
– Ongoing evaluation
– Subsequent revision/adjustment of activities
• Stakeholder’s buy-in on common priorities
– Local Health Jurisdictions
“And you better start swimming
or you’ll sink like a stone.
For the Times,
they are a-changin”
Bob Dylan
Thank you
")