Pacemaker Malfunctions
Even less amusing!
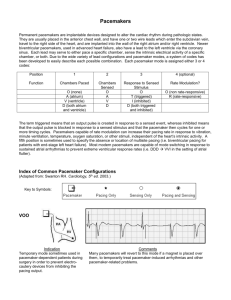
Pacemaker Codes
(NASPE/BPEG)
Position
Category
I
II
III
Chamber(s)
paced
Chamber(s)
sensed
Response to
sensing
O=None
A=Atrium
V=Ventricle
D=Dual (A+V)
O=None
A=Atrium
V=Ventricle
D=Dual(A+V)
O=None
T=triggered
I=Inhibited
D=Dual (T+I)
Triggered
Means different things
If
an intrinsic event is sensed, the
pacemaker will trigger pacing to that
chamber OR to another chamber
– P wave will trigger an AV interval
– R wave will trigger pacing to the ventricle
Triggered?
Atrial paced spike
triggers AV interval
Triggered ventricular
pacing spike is in refractory
period of ventricular cycle
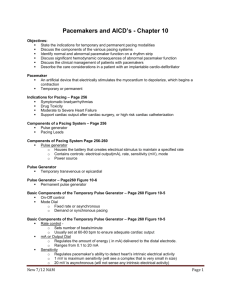
AOO Pacing
Chamber Paced
Chamber Sensed
A
O
O
Action or Response to a
Sensed Event
Asynchronous mode
Not sensing so can’t react
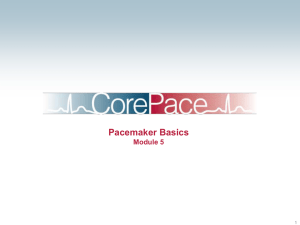
VVI Pacing
Chamber Paced
Chamber Sensed
V
V
I
Action or Response to a
Sensed Event
Even more!
Fourth letterProgrammable
Functions
R = rate modulation
C = Communicating
M = Multiprogrammable
S = simple
programmable
O = None
Fifth letter –
antitachycardic
functions
O = none
P = paced
S = shock
Rate Modulation
Atrium or Ventricle is pacing or tracking
above the set upper limit (permanent
pacemaker)
Used
to help compensate for increased
demands
– Sensor can be:
Change in temperature
Change in movement or body position
Change in pH
Change in minute ventilation
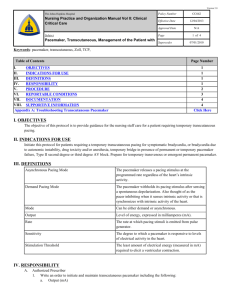
DDDR Pacing
Chamber Paced
Chamber Sensed
Response to a Sensed Event
Rate modulated
D
D
D
R
Pacing Malfunctions
Often a two person job
One
person supports the patient
One person troubleshoots the pacemaker
Failure to pace
(not tryin’ to tickle)
No pacing spikes or not
enough coupled with the
intrinsic rhythm to
ensure good CO
Pacing energy not being
transmitted from
generator to patient
Failure to pace ( not trying to tickle)
How do you fix this?
Pacing spikes not visible (often an equipment
problem)
Pacer on?
Rate set correctly?
Battery fresh ?
Connections tight?
Get another cable
Get another generator
Often an equipment problem-no energy thrown
Failure to capture (target is not
ticklish/not ticklin’ hard enough)
Pacing Arm is throwing out energy-target
is not responding
Loss of Capture (target is not ticklish)
Nothing happens in response to
arm throwing out impulse
How do you fix this?
Myocardium is not responding to stimulation
Battery fresh?
Connections tight?
– Make sure lead is in contact with myocardium
mA high enough?
Assess electrolytes, oxygenation, acid base
balance
Ischemic tissue? Fibrin sleeve?
Reposition patient or patient’s arm on side of
pacemaker if subclavian entry
Undersensing (ticklin’ too much)
Intrinsic rhythm not seen so pacing arm
throws out energy
Undersensing (ticklin’ at the wrong time)
Pacer eyeball is set too high!
Can’t see target moving so the arm
throws out a stimulus
The danger of “not seeing”...
Pacer arm throws out
stimulus during vulnerable
portion of cardiac cycle
How do you fix this
Pacermaker not seeing correctly
Battery
fresh
Connections tight
– Leads in contact with myocardium
– Lead fracture
Do
a sensitivity threshold to get eyes at
proper level
Oversensing
( not ticklin’ enough)
Pacemaker misinterprets noncardiac
events as intrinsic activity
Oversensing (not ticklin’ enough)
Pacer eyeball thinks it sees
cardiac activity so the arm does
not throw out an stimulus
How do you fix this
Pacermaker not seeing correctly
Battery
fresh
Connections tight
– Leads in contact with myocardium
– Lead fracture
Do
a sensitivity threshold to get eyes at
proper level
Let’s practice
Other Complications
Infection
Pulmonary
embolus
Venous Thrombus
Myocardial
perforation
Endocarditis
Nursing Care
Assess heart rate
and rhythm
Protect patient from
injury
Troubleshoot
malfunctions
Evaluate pacemaker
function
Keep patient
informed
Sample documentation
Temporary pacemaker (0800)
Epicardial wires ( 2 ventricular)
Pacing threshold 3; mA set at 6
Sensitivity threshold 4 mV; mV set at 2 mV
Rate set at 60; patient’s intrinsic rate 30
Patient pacing about 50% of time. 100% capture
when paced.
Temporary pacemaker (1400)
Pacemaker off. Pacing wires grounded and taped
to chest wall. Site care with betadine.
Flippin’ a switch
What’s the deal with
the magnet?
No Magnet
With Magnet
Rapid Atrial Pacing
Rapid Atrial Pacing
Used only in the atrium
Pace at rates from 80-800
Need
to get higher than patient’s ATRIAL
rate
Physician must be present when in use
Nurse
may only connect
Always have defibrillator available
What are the possibilities?
Single chamber pacemaker
Dual chamber pacemaker
Free standing RAP machine
Think
Frankenstein
Rapid Atrial Pacing (single chamber)
Flip open top of
pacemaker
Set rate according to
physician instruction or
let MD set rate
Press enable to begin
Rate will be higher than
patient’s atrial rate
Press hold to deliver
until instructed to stop
Will be done in bursts
Pacing light will flash
Rapid Atrial Pacing (dual chamber)
Found on bottom half of
pacer
Must hit menu screen
and scroll to menu 3
Set rate by turning
round knob
Press select to deliver
and HOLD until
instructed to release
DDD
320
RAP
80
440
800
Press SELECT
to
Deliver
Rapid Atrial
Pacing
Select
3
Menu
Permanent pacemakers
Differences
You cannot access pacing generator
You cannot see leads
Helps interpretation of strip if you know
how pacemaker is set up
Should
have card
Old records
Request info from cardiologist
You are in trouble!
What can you try if you have a malfunction
with a permanent pacemaker that is
compromising your patient?
Biventricular pacemakers?
Pacing leads in the RV
and into the coronary
sinus
Allow both ventricles to
pace synchronously
Improves heart function
for patients with CHF
EKG will not look
different from single
ventricular pacing
The END
 0
0