AMIRAH BT JAMALUDIN
NURHIDAYATUL HUSNA BT JOHARI
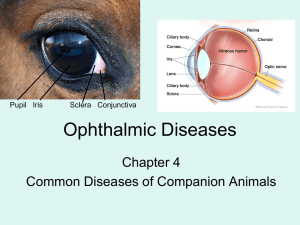
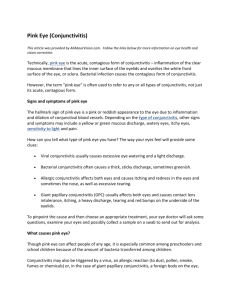
Allergic conjunctivitis is an inflammation of
the conjunctiva (the membrane covering the
white part of the eye) due to allergy.
If something irritates this conjunctiva, eyes
may become red and swollen. The eyes also
may itch, hurt or watery.
It is also known as “pink eye”.
Allergic simple conjunctivitis
Spring catarrh
Phlyctenular kerato-conjunctivitis
Giant papillary conjunctivitis
•
•
•
•
•
•
•
•
Definition : Occurring as the result of exposure to a
wide variety of allergens
Simple allergic conjunctivitis often results from
exposure to eye medications or contact lens solutions
(or their preservatives).
Symptoms:
Itching and tearing in response to antigen exposure.
Signs :
Unilateral or bilateral
Mild to moderate conjunctiva hyperaemia
Chemosis
Management:
General measures include:
Avoid allergen where possible
Avoid wearing contact lenses until symptoms and
signs resolve
Avoid rubbing the eyes
Cool compresses and preservative-free lubricants may
also help
If severe,
- Oral or topical anti-histamine
- Mast cell stabilizer
Definition: Kerato-conjunctivitis produced as an allergy
to an endogenous agent.
Aetiology: It is a manifestation of allergy to an
endogenous toxin as
Tuberculo-protein
Intestinal parasites
Septic foci as in tonsils and adenoids
Symptoms :
Discomfort and lacrimation
If cornea involved,photophobia and blepharospasm
occur
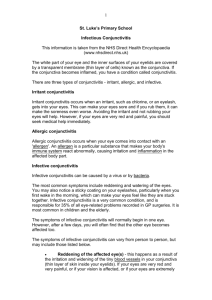
Signs :
◦ Phlyctens
Rounded nodules
Size 1-3 mm
Grayish in color
Eleveated above the surface
Surrounded by a small area of injection
Complications:
(1)Cornea
A-Corneal phlycten
B-Phlyctenular ulcers
C-Phlyctenular pannus
•
(2)Eczema of lids
(3)Muco-purulent conjunctivitis: due to secondary infection
with staph. Aureus
(4)Recurrence: are common if the cause is not removed.
•
Treatments :
Local cortisone drops and ointment
Atropine if cornea is involved
Fascicular ulcer needs cautery with carbolic + Periotomy &
cautery of vessel
Definition : It is a bilateral seasonal conjunctivitis
recurring in the warm seasons.
Aetiology : It is an allergy of the conjunctiva to an
unknown exogenous factor.
The contributing factors are :
U.V rays
Heat
Dust
Incidence :
Age : Children
Sex : boys more
Season : summer (not spring)
Symptoms :
Itching
Photophobia
Lacrimation
Ropy discharge (thread): formed of
mucus,eosinophils and epithelial debris so that it is
scanty,white and elastic
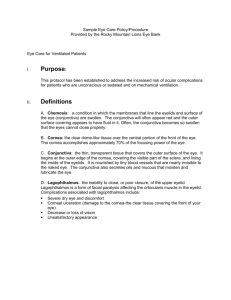
Palpebral type (70%)
• Large flat-topped papillae
• Bluish white color
• Cobble stone arrangement
• Fornix always free
• Milky white film (ropy discharge)
Bulbar type (10%)
• Gelatinous masses (due to thickened epithelium and hyaline degeneration )
• Tranta spots (white spots)
Mixed type (20%)
• Keratitis superficialis vernalis of Tobgy
• Superficial ulcers
• Epithelial plaque formation that should be scraped
• Weakness of the cornea with higher incidence of Keratoconus and Keratectesia
Treatment:
General:
-Antiallergy drugs (antistine,Benadryl,calcium etc)
Local:
-Dark glasses for photophobia
-Cold compression for sensation of heat
-Frequent washing with cold lotion as 4 % boric acid
-Local antihistaminic as antistine of preisoline drops
-Local vasoconstrictor as adrenaline or privine for
hyperaemia
-Local cortisone drops (Dexamethasone 0.1 %) pulse
therapy during an attack every 2 hours for 5 days only to
guard against its complication (may induce glaucoma)
-Local disodium chromoglycate eye drops to stabilize the
mast cells “one month before summer”
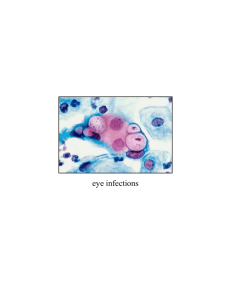
Definition : It is an allergic conjunctivitis
characterized by the formation of giant papillae.
It occurs most probably due to mechanical
irritation of the palpebral conjunctiva in case of :
-Contact lenses (more with extended wear CL
and with lens deposits)
-Artificial eyes
-Prominent suture following surgery
Symptoms :
-Red Eye
-Mucoid discharge
-Itching
Signs :
Conjunctival hyperaemia
Giant papillae on superior tarsal conjunctiva
Superficial punctuate keratitis
Peripheral corneal subepithelial infilterates
Treatment :
Stops using contact lenses for 2 weeks
Topical mast cell stabilizer (disodium
chromoglycate) 4 times daily
Topical steroids for few days only
Use new daily wear lenses after complete cure
Thank you
Syukran
Terima kasih…