Jim Schwartz, Chief
Arlington County Fire Department
Located directly across from Washington D.C.
Highly urbanized community of 26 square
miles; population if 212,900
• Columbine High School Shooting –April 20, 1999
• Eric Harris & Dylan Klebold
• Both had self-inflicted fatal wounds
• Occurred within 45 minutes from start of incident
• No significant law enforcement entry for 1 hour
• No medical operations inside for 4 hours
• 12 students & 1 teacher killed
• 24 wounded
• Coach Dave Sanders
• Bled for > 2hrs before dying
IAFC, IACP, FBI and DHS Host meeting to
discuss medical response to active shooter
IAFF, Metro Chiefs and USFA also in
attendance
Discussion also covered use of ICS during
incidents
Conclusion -“integrated and coordinated
planning, policies, training and team building
prior to any incident will ensure effective and
successful response”
Initial EMS/Fire medical responders should work
with Law Enforcement assets to rapidly deploy
into areas that have been cleared but not
secured to initiate treatment and effect rescue
of injured victims
▪
▪
▪
▪
NOT tactical medics but first arriving EMS assets
Security and/or escort provided by LE teams
Requires appropriate equipment and PPE
Should utilize TECC medical principles
One answer to the issue
of rapidly providing
stabilizing medical care in
areas that are clear but
not secure
NIMS compliant name
Task Force: Any
combination of single
resources, but typically two
to five, assembled to meet
a specific tactical need
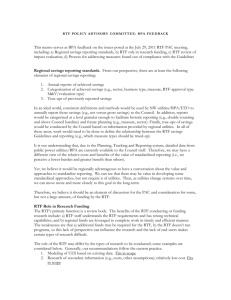
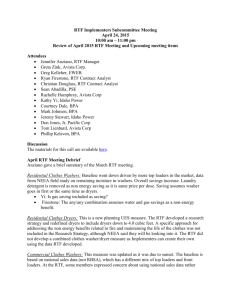
First arriving EMS providers (NOT tactical medics)
team up with 3 patrol officers to move quickly into
“warm” zone areas along cleared corridors to
initiate treatment and evacuation of victims
3 patrol officers for front and
rear security
Readily available resource
Do NOT assist medics in care
Responsible for security and
movement only
2 street medics in ballistic
gear with supplies to treat
up to 14 patients
Readily available resource
Able to initiate TECC care and
rapidly evacuate
Comprehensive document summarizing
commonalities, trends, and events
Total qualifying cases from 1966-2012: 230
Some common characteristics found but also
a large degree of variation across broad
categories
Age, Sex, Planning, Location, Relationship to
victim, weapons used
Duration of event
Average <10 minute duration
▪ Most as short as 3-4 minutes
Average 12-15 min response by Police
93% of incidents in academic institutions were over
prior to the first responding asset, police or
fire/EMS, arriving on scene
After review of combat and post-incident data:
The immediate threat is rapidly mitigated in almost all
incidents well prior to Fire/EMS response
The sooner the first responders start medical
treatment, the greater the chance that victims will
survive
The risk from active shooter incidents is very low in
areas that are clear but not secure
Mumbai Attack November 26-28, 2008
• 10 terrorists –6 killed / 4 arrested
• 171 killed
• Multiple attack sites
•
•
•
•
TajMahalPalace andTower –50 killed
OberoiHotel –30 killed
NaramanHouse –8 killed
Other incidents
• Overcoming the ‘us vs. them’ mentality
• Who ‘s in charge of the scene
• Cost sharing concerns
• Emphasize the force multiplying benefit
during ASEs
• Emphasize improved operational relationships
• During both ASEs and normal day to day operations
• Public image of collaboration between police &
fire
• Teach TECC –Tactical Emergency Casualty Care
Evidenced-based best practices medical
guidelines for care at or near the point of
wounding in high risk operations
NOT Law Enforcement tactical medic specific
For use by any first responder who is providing
medical care whenever and wherever there is
increased risk to provider and patient
Goals:
Provide principles for point of wounding
management of trauma for response to ALL
atypical and high risk civilian emergencies
To balance appropriate medical care with
the threat, the required tactics, and the
civilian scope of practice, equipment, and
population
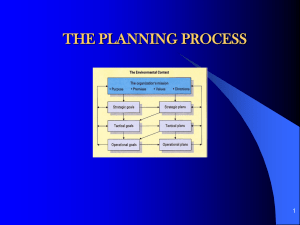
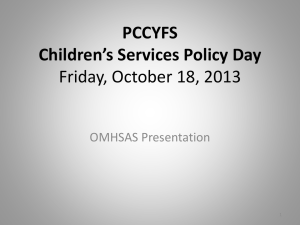
Initial responding patrol officers form 2-3 contact
teams that all enter building along same corridor
and move quickly to engage shooter
Contact teams essentially are clearing the
primary corridor as they move to sound of
shooting
Identify and notifty command of threats (IEDs, etc)
Do not open locked doors unless sound from behind would
indicate threat
Do not aide or assist injured
As victims encountered, notify Command of location
Need for RTF identified by 2nd contact team
Initial RTF team formed and quickly moves
into area down the corridor cleared by the
contact teams
Will not move into un-cleared areas or get in front
of contact teams
RTF
Goal of initial RTF team is to stabilize as many victims
as possible using TECC principles
Will penetrate into building as far as possible until they run
out of accessible victims or out of supplies
“Stabilize, position, and move on”
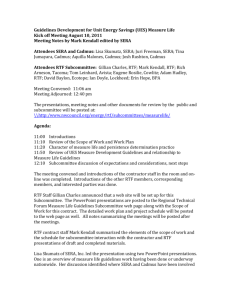
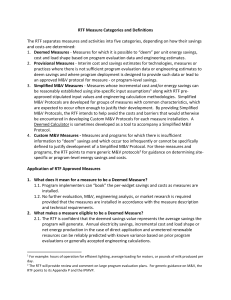
Once RTF operational, Fire and Police Unified
Command will establish:
RTF re-supply near point of entry
External casualty collection point for transfer of
patients
Warm Corridor for evacuation away from area
Dedicate non-RTF assets to assist in transfer of
patients from RTF assets for external evacuation
C
C
P
Resupply boxes
Questions?