File - Optometry Peer Tutoring
advertisement

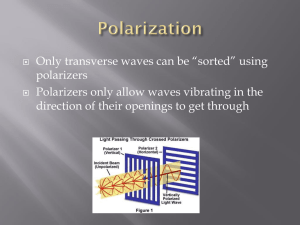
Retinoscopy OP1201 – Basic Clinical Techniques Part 2 - Astigmatism Dr Kirsten Hamilton-Maxwell Today’s goals By the end of today’s lecture, you should be able to Describe the major types of regular astigmatism Explain key issues in retinoscopy Describe how to perform retinoscopy in a patient with astigmatism Be aware of procedural adaptations for difficult cases By the end of the related practical, you should be able to Assess distance refractive error in both meridians using retinoscopy, within 10min for both eyes Astigmatism Astigmatism means “not spherical” You will find yourself describing it to patients as “your eye is shaped like a rugby ball instead of a football” The difference in curvature (usually of the cornea or crystalline lens) results in the eye having two different powers along two different meridians In regular astigmatism, the two meridians are exactly 90deg apart Describing astigmatism Two powers and an axis Power 1 = most positive (or least negative) meridian Power 2 = least positive (or most negative) meridian Axis = the orientation of the flattest side of the rugby ball. More specifically, orientation of the least positive (most negative) meridian. Lying on its side = Axis 180 and sitting on its point = Axis 90 Hint: Look at a trial frame Note: orientation of line foci will change with cyl. axis, separation will change with cyl. power. + cyl. +2.00 DC, axis vertical (900) + cyl. +1.00 DC, axis horizontal (1800) +1.00/+1.00 X 90 (+2.00/-1.00 X 180) sphero-cylinder + = Note: vertical power gives horizontal line focus, horizontal power gives vertical line focus Circle of least confusion Astigmatic cone Simple myopic astigmatism Simple hypermetropic astigmatism Compound myopic astigmatism Compound hypermetropic astigmatism Mixed astigmatism What does it look like? Distribution of astigmatism Power Axis 1/3 of all prescriptions are With the rule: axis within 15 spherical 1/3 contain an astigmatic correction of 0.25 to 0.50DC 1/6 contain an astigmatic correction of 0.75 to 1.00DC remaining 1/6 contain an astigmatic correction of over 1.00DC 1% contain an astigmatic correction of > 4.00DC either side of horizontal (38%) Against the rule: Axis within 15 either side of vertical (30%) respectively All other axes considered as oblique (32%) Prevalence of oblique astigmatism is unaffected by power, but with the rule becomes more prevalent (and therefore against the rule less prevalent) as astigmatic power increases. More on astigmatism As a rule, astigmatism is equal and symmetrical across the two eyes. Degree of astigmatism is unrelated to spherical errors between + and -8.00DS. Beyond these values, higher spherical refractive error is associated with higher astigmatic errors. Can consider +/-8.00DS range as ‘normal’ eyes with ‘normal’ refractive errors. Errors beyond +/-8.00DS can be considered ‘abnormal’. Higher errors of both spherical and astigmatic type are increasingly associated with ocular pathology. “Homework” See what you can find out about how astigmatism changes with age. In particular: Many babies are born with astigmatism. How much would be considered “normal” and how does it change in the first 2 years of life? Why does “against the rule” astigmatism become more common in older patients? Please revise your Dispensing notes on sphero-cyl format Spectacle prescriptions by optometrists are always written in sphero minus cyl format Ret for astigmatism What does the reflex look like Finding the axis Finding the power Recording your results Astigmatism As we have just discussed, the eye can be a different power along different meridians (in different directions) Astigmatism The primary meridians are always 90deg apart, but can be in any orientation The axis Retinoscopy can measure the powers of both meridians and determine the axis Correction of astigmatism To correct astigmatism, we need a lens that has a different power in different meridians Cylindrical lens, abbreviation DC When doing ret, we will scan and then correct each of the meridians separately The (eventual) idea is… Find and then correct the most positive (least negative) meridian first with a sphere At exactly 90deg to that (always 90deg), add a minuscyl until corrected In 3D This example is against the rule astigmatism Retina behind astigmatic cone: compound myopic astigmatism. Against in all directions. -sph., –cyl.x90 (-sph., +cyl.x180) Retina at rear (horizontal) line focus: simple myopic astigmatism. Neutral vertically, against horizontally. -cyl.x90 only (or –sph. then +cyl.x180) Retina in between line foci: mixed astigmatism. With vertically, against horizontally. + sph., –cyl.x90 (or –sph., +cyl.x180) Retina at circle of least confusion: best vision Retina at front (vertical) line focus: simple hypermetropic astigmatism. With vertically, neutral horizontally. + sph., –cyl.x90 (or +cyl.x180 only) Always use –cyl, i.e. not the option in brackets: move posterior focal line onto retina with sphere, collapse anterior backwards with –ve cyl. Retina in front of astigmatic cone: compound hypermetropic astigmatism. With movement in all directions. + sph., –cyl.x90 (+ sph., +cyl.x180) Identifying astigmatism Oblique movement Set up Measure your patient’s pupillary distance (PD) Dial your patient’s PD into the trial frame and fit it to your patient’s face Place a working distance (WD) lens in the back cell for the trial frame (if using) Illuminate a non-accommodative target Usually the duochrome Turn room lights off Procedure Turn retinoscope to brightest setting, with collar at the bottom Scan along 90 and 180deg to quickly check adequate fogging in both eyes There should be against movement in both eyes (accommodation control) WD lens provides some fog but it will not be enough in many hypermetropes Quick guesstimate of refractive error Reflex brightness? With or against movement? Astigmatism? Finding the axis Return the light to vertical and focus light to thinnest beam on the face using collar Is the beam in the pupil aligned with the beam on the face? Rotate until they are This will occur in two positions These are the primary meridians Scan along the primary meridians Does the reflex move along the same axis? If there is oblique movement, further rotation is required Finding the sphere power Return the collar to the bottom Find the most hypermetropic meridian Slowest “with” or fastest “against” This assumes you are using minus cyls (some textbooks talk about plus cyl refraction) Neutralise the most hypermetropic meridian first Use the bracketing technique from last week As you have found the most hypermetropic meridian, you’ll be adding plus (or reducing minus) Check for reversal Refine in smaller steps until neutrality Finding the cyl power Rotate the beam 90deg to the other primary meridian You should see against movement Fast = low astigmatism Slow = high astigmatism Confirm no oblique movement Neutralise this meridian using minus spheres This is an intermediate step! You can, and should, use cyls Replace the sphere with a minus cyl of the same power, with the axis lined up with your beam All meridians should now be neutralised The final steps Repeat all steps for the LE Return to the RE to recheck that you do not need to add more positive power Remove WD lens from both eyes Check vision monocularly and record Should be within ±0.50D in both meridians and within 15deg of the axis Complete both eyes within 10min Recording results You will now have used two different sphere powers at two primary meridians (not including the WD lens) For example: +2.00DS axis 20deg and an additional -1.50DS axis 110deg The highest positive power becomes the sphere power (+2.00DS) The amount of astigmatism is recorded as cylinder, and is the difference between the power of the two primary meridians (-1.50DC) The axis is the position of the beam in the most negative/least positive meridian (110deg) Result: +2.00DS/-1.50DCx110 Another example You have found RE -1.00DS axis 90 and an additional -2.00DS axis 180 Sphere power = -1.00DS Cyl power = -2.00DS Axis = 180deg -1.00DS/-2.00DCx180 This is called “with the rule astigmatism” Axis within 15deg of horizontal Most of your classmates will have this Another example You have found RE +1.00DS axis 180 and an additional -4.00DS axis 90 Sphere power = +1.00DS Cyl power = -4.00DS Axis = 90deg +1.00DS/-4.00DCx90 This is called “against the rule” astigmatism Axis within 15deg of vertical Some of your classmates will have this Overcoming problems Reflex is very dim in high prescriptions Use high powered lenses to see if reflex becomes brighter and movement more obvious Also look out for differences in brightness in different meridians because this means high astigmatism Small pupil makes retinoscopy and ophthalmoscopy more difficult Move closer, try dimmer lighting, or consider use of tropicamide to dilate pupil Asphericity of cornea/lens can result in change in power with increased distortion in the peripheral pupil Concentrate on centre of ret reflex Overcoming problems Lenticular or corneal opacities will make reflex dimmer Slide collar up (but watch how far) and/or move closer (change WD lens to compensate for change in working distance) Reflex may become distorted with lenticular or corneal opacities or distortions e.g. keratoconus and cataract, which may produce scissors movement Scissors movement Issues in retinoscopy Controlling accommodation Optical effects of being off axis Effect of pupil size Controlling accommodation Intraocular lens can change in shape and thus change the power of the eye Accommodation system is particularly strong/unstable in young people so needs to be controlled The WD lens is part of the solution Vision becomes worse if accommodates, so patients tend to avoid doing this Longest working distance possible Use non-accommodative target Green(? by convention) light on duochrome Being on axis Oblique astigmatism is induced if retinoscopy is performed more than 5deg from the visual axis -0.50DCx90 induced if 10deg from visual axis along the horizontal Check that you are almost blocking the fixation target with your head, both horizontally and vertically Completely blocking the target will induce accommodation Effect of pupil size Small pupils limit the visibility of the reflex Use dimmest beam possible (to decrease constriction due to light) Use shorter working distance Don’t forget to use a different working lens Short WD also helps if your patient has a dim reflex. Eg. Cataracts This will commonly be an issue for your older patients Large pupils suffer from peripheral aberration Look only at the centre This will commonly be an issue for your younger patients Sources of error Not being in the right position Incorrect working distance (getting too close is most common) Head blocking the patient’s view Off axis Observation errors Failure to obtain reversal Failure to locate principal meridian Paying too much attention to peripheral movement with a large pupil Sources of error Not fogging appropriately Forgetting to account for the WD lens, or not removing it when you are finished Patient not looking at an appropriate target Further reading Read Elliott sections 4.5-4.7 Real examples of ret can be found in Elliott Online