presentation ( format)
advertisement
")
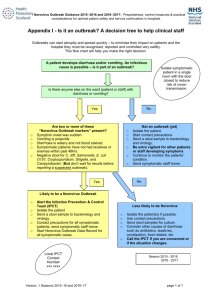
Update on Epidemiology and Management of Norovirus Aron J. Hall, DVM, MSPH Viral Gastroenteritis Team Centers for Disease Control and Prevention ajhall@cdc.gov Presented at American College Health Association Annual Meeting Philadelphia, PA June 3, 2010 “I have NO actual or potential conflict of interest in relation to this educational activity or presentation” History • 1929: “Winter vomiting disease” first described • 1940s-1960s: 75% of gastroenteritis episodes of unknown etiology • 1968: Outbreak of acute gastroenteritis (AGE) at elementary school in Norwalk, Ohio • 1972: Viral particle seen by electron microscopy • 1973-1992: Electron microscopy and serology used to confirm outbreaks • 1992-1994: Reverse transcription-polymerase chain reaction (RT-PCR) developed Disease Burden • #1 cause of acute gastroenteritis in U.S. – 23 million cases annually – 1 in 13 Americans become ill each year • Affects all ages, though greatest burden in children and elderly – 63,000 children hospitalized annually in U.S. – 80 deaths annually among elderly in U.K. • Occurs year round, though seasonal peak activity during winter • Found worldwide Mead 1999 EID Patel 2008 EID Harris 2008 EID Norovirus Detection in Outpatients, British Infectious Intestinal Disease Study Amar 2007 Eur J Clin Micro Clinical Disease • Incubation period: 12-48 hours • Acute-onset vomiting and/or diarrhea – Watery, non-bloody stools – Abdominal cramps, nausea, low-grade fever • Most recover after 12-72 hours – Up to 10% seek medical attention; some require hospitalization and fluid therapy – More severe illness and death possible in elderly and those with other illnesses Laboratory Diagnostics • No cell culture or animal model available • Polymerase chain reaction (PCR) – Gold standard: Quantitative real-time assay – Conventional RT-PCR used for genetic sequencing • Enzyme Immunoassays (EIA) – Recent use of virus-like particles (VLP) – Inadequate sensitivity (<50%) for clinical use • Electron Microscopy (EM) – Resource intensive – Poor sensitivity Viral Shedding • Primarily in stool, but also vomitus • Occurs for at least 2-3 weeks • Peaks 4 days after exposure – Greater in those with symptoms – May occur after resolution of symptoms • Infectivity of shed virus unknown • Infectious dose: 10-100 viral particles Viral Shedding After Experimental Infection Asymptomatic Vomiting and Diarrhea Atmar 2008 EID Immunity • Short-term homologous immunity • No persistent cross-protective immunity • 30% infections asymptomatic • Genetic susceptibility – Histo-blood group antigens – Secretor status (FUT2 gene) Treatment • No specific antiviral agents or vaccines currently available • Supportive care for dehydration, primarily oral or IV fluid therapy • Antibiotics, antiemetics, antimotility agents generally not recommended Transmission • Person to person – Direct fecal-oral – Ingestion of aerosolized vomitus – Indirect via fomites or contaminated environment • Food – Contamination by infected food handlers – Point of service or source (raspberries, oysters) • Recreational and Drinking Water – Well contamination from septic tank – Chlorination system breakdown Norovirus Transmission Cycle Intestinal Pathology Symptomatic (70%) Asymptomatic (30%) A B Infected Present (40%) Absent (60%) Protected Susceptible to Infection Viral Shedding Stool Vomit Previously Acquired Immunity Transmission Vehicles Nonsecretor (20%) Innately Resistant Secretor (80%) Susceptible to infection Exposed Population Person-toPerson Environment & Fomites Water Food Foodborne Burden • Causes 67% of all foodborne illness in U.S. from known agents • Annual foodborne norovirus estimates (rank among known agents) – 9,200,000 cases of disease (#1) – 20,000 hospitalizations (#1) – 120 deaths (#4) Mead 1999 EID Confirmed and Suspected Etiology of 1270 Foodborne Outbreaks Reported to CDC, 2006 Other/Multiple 2% Unknown 29% Norovirus 40% Chemical 5% Parasites 1% Bacteria 23% CDC 2009 MMWR Etiology of Foodborne Outbreaks Reported to CDC CDC 2009 MMWR Single Food Commodities Involved in Norovirus Outbreaks, 1998-2007 Outbreaks Illnesses Commodity No. (%) No. (%) Leafy vegetables 124 (31.6) 3771 (33.7) Fruits-nuts 58 (14.8) 2511 (22.4) Mollusks 54 (13.8) 749 (6.7) Poultry 40 (10.2) 645 (5.8) Pork 26 (6.6) 564 (5.0) Beef 23 (5.9) 369 (3.3) Dairy 16 (4.1) 862 (7.7) Grains-beans 13 (3.3) 157 (1.4) Vine-stalk 11 (2.8) 447 (4.0) 392 (100) 11185 (100) Total Preliminary CDC Data Norovirus Classification • Genogroups Broad – >60% amino acid similarity – 3 affect humans (GI, GII, GIV) • Genotypes – >80% amino acid similarity – 8 GI genotypes, 17 GII genotypes • Strains (variants, clusters) – >95% amino acid similarity – 11 GII.4 strains identified Specific Norovirus Classification Tree Patel 2009 J Clin Virol Norovirus GII.4 Pandemics Winter Season 1995-96 2002-03 2004-05 2006-07 2006-07 2009-10 Strain Name(s) Bristol (US95/96) Farmington Hills (2002) Hunter (2004) Laurens (Yerseke, 2006a) Minerva (Den Haag, 2006b) New Orleans GII.4 Strain Prevalence in Outbreaks Tested at CDC Siebenga 2009 JID Setting of Norovirus Outbreaks Reported to CDC, 1994-2006 250 GII-4 other GII GI 200 150 100 50 0 Long-term Care Restaurants, Cruise Ships & Facilities Parties & Events Vacations Schools & Communities Zheng 2010 JCM Seasonality of Norovirus Outbreaks Reported to CDC, 1994-2006 Zheng 2010 JCM Dynamics of Strain Evolution and Population Immunity 500 Variant 1 450 Estimated population immunity to circulating variant 400 Variant 2 350 300 250 200 Cases 150 100 50 0 2001 2002 2003 Challenges • • • • • Asymptomatic infections Persistent in the environment Resistant to common disinfectants Very low infectious dose Recurrent infections College Campus Outbreaks: Recent Examples Outbreak 1: California, 2008 • Large university (enrollment 32,000) • Oct 3: Initial report of >30 students at emergency dept or student health center (SHC) with AGE • L.A. County Dept of Public Health (LACDPH) – Conducted site visits for interviews with ill students and environmental inspection – Monitored daily GI reports from hospitals, SHC, and residence hall advisors • Campus administration sent mass email to all students to complete web-based survey – case ascertainment – risk factor analysis Outbreak 1: Investigation Findings • 5,227 (16%) students completed web-based survey • 478 (1.5%) total cases identified via survey or reported directly LACDPH – 185 (39%) sought medical care at SHC – 35 (7.3%) visited ED – 10 (2.1%) hospitalized for dehydration • 10 stool specimens tested – 6 positive for norovirus GII by qRT-PCR – All identical GII.6 Seacroft strain • No single event, residence hall, eating venue, or ill food handler were implicated Student AGE Cases by Onset Date, California, 2008 Outbreak 2: Michigan, 2008 • Small college (enrollment 3,000) • Nov 6: 60 AGE cases at campus medical clinic • State and County health depts sent health alert – local schools – healthcare providers – medical facilities • Nov 7: total increased to 130 cases, suggesting point source exposure – One primary dining facility on campus – Parents’ day activities began following day Outbreak 2: Actions Taken • County health dept closed campus – Curtail transmission and facilitate disinfection – Only take-out and delivery available on campus • Email & text messages sent to students – Stay in residence unless required medical attention – Completed electronic questionnaire if ill – Disinfect dorm room with dilute bleach, wash soiled linens and clothing, and wash hands frequently • Ill faculty and staff advised to stay home until 72 hours after symptoms resolved • Parents and media sent outbreak updates via email and announcements on college website Outbreak 2: Investigation Findings • 418 (13%) of 3,238 students ill – 205 via electronic reporting – 213 via direct reporting to medical clinic • 33 (5.2%) of 630 faculty/staff ill • 5 stool specimens tested – All positive for norovirus GI by qRT-PCR – All identical GI.4 strain • 3 ill food service workers with vomiting and diarrhea at work on Nov 4 Student/Faculty/Staff AGE Cases by Onset Date, Michigan, 2008 Ill food workers Outbreak 3: Wisconsin, 2008 • Large university (enrollment 42,000) • Nov 6: 2 students from residence Hall A (population 1,150) with AGE – Students reported additional residents in Hall A with similar symptoms – AGE reported during following week from other residence halls and a sorority house Outbreak 3: Actions Taken • Campus health services led investigation – Daily reports of ill residents from Hall A staff – Email sent to all residence hall residents (3,480) and fraternity/sorority members (2,700) – If AGE during preceding 2 weeks, asked to complete online questionnaire • Students educated on hand washing • Dormitories, public restrooms, communal areas cleaned with approved disinfectants Outbreak 3: Investigation Findings • 156 total student cases reported – 138 identified online, 18 through campus health – 36 (23%) sought healthcare, none hospitalized – Symptoms included: • diarrhea (92%) • chills (80%), • vomiting (88%) • body aches (81%), • cramps (88%) • subjective fever (65%) – 93 cases among Hall A residents (8% attack rate) • 5 stool specimens tested – 2 positive for norovirus GII by qRT-PCR – Sequencing not performed Student AGE Cases by Residence and Onset Date, Wisconsin, 2008 Index cases reported Email sent Outbreak Examples Summary • 1,000 reported cases of illness, including at least 10 hospitalizations – Median outbreak duration: 19 days (range: 16-20) – Minimum attack rates ranged from 1.5% to 12.9% • College campuses at high risk for norovirus outbreaks – Extensive opportunities for transmission – Numerous shared exposures and living areas • Access to healthcare encourages illness reporting and facilitates outbreak recognition Prevention and Control Recommendations • Promote appropriate hand hygiene – Wash with soap and water ≥ 20 seconds – Alcohol-based hand sanitizers as adjunct • Prompt and thorough environmental disinfection – Bleach solution for contaminated surfaces (1000-5000 ppm) – Other EPA-approved disinfectants? • Exclude ill students/staff from food preparation for ≥48-72 hrs after symptom resolution • Encourage ill students to seek medical care and limit social activities • Consider facility closure and/or event cancellation • Disseminate recommendations promptly during outbreak, including via electronic media Acknowledgments • University of Southern California • University of WisconsinMadison – Craig Roberts • Hope College – Tom Renner • Ottawa County Health Dept – Paul Heidel – Debra VandeBunte • Los Angeles County Dept of Public Health – Curtis Croker – Roshan Reporter – Shikari Nakagawa-Ota • Michigan Dept of Community Health – Brenda Brennan • Wisconsin Div of Public Health – John Archer Thank You… Questions? Disclaimer: The findings and conclusions in this presentation are those of the author and do not necessarily represent the views of the Centers for Disease Control and Prevention.