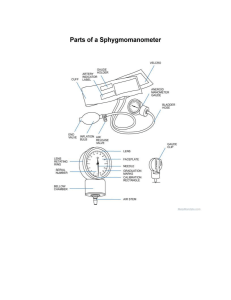
YILDIZ TECHNICAL UNIVERSITY DEPARTMENT OF B IOMEDICAL E NGINEERING EXPERIMENT 7 Blood Pressure Author: MARWA ABOUARRA 24.May.2023 Grading Objective Theory Data and Calculations Discussion Questions References Total Points 5 10 25 30 25 5 100 Total 1. OBJECTIVE The objective of the Blood Pressure experiment is to: 1) We're going to use a fancy auscultatory method to indirectly figure out the systolic and diastolic blood pressures in your arteries. We'll be matching those pressure points with the appearance and disappearance of some vascular sound. It's like a symphony in your veins! 2) We'll be measuring, recording, and comparing your arterial blood pressure in each arm. And we're going to make sure the conditions are identical. 3) Time to put your body to work! We're going to check your arterial blood pressure again, but this time in different experimental conditions—rest and exercise. To see how your blood vessels handle the action! 4) We'll crunch some numbers and compare your pulse pressure and mean arterial pressure under those different conditions we mentioned earlier. It's all about understanding how your blood flow behaves when you're chilling or breaking a sweat. 5) And last but not least, we're going to measure the time between the R-wave of your ECG and those funky Korotkoff sounds to calculate the pulse pressure wave velocity. 2. THEORY Circulating blood plays a vital role in the body by providing transportation and communication among cells while maintaining a stable internal environment for optimal cellular activity. This circulation occurs as the heart pumps blood through a closed circuit of blood vessels. The flow of blood through the heart and blood vessels is unidirectional, with blood entering the heart from the pulmonary and systemic veins and exiting the heart through the pulmonary and systemic arteries. To ensure the unidirectional flow of blood through the heart's chambers, four valves inside the heart come into action during each cardiac cycle. The right atrioventricular valve (tricuspid) and the left atrioventricular valve (bicuspid or mitral) prevent blood from flowing back into the atria from the ventricles. Similarly, the pulmonary semilunar valve and the aortic semilunar valve prevent the backward flow of blood from the arteries into the ventricles. The ventricles serve as the primary pumping chambers of the heart. During ventricular diastole, when the ventricles relax, the atrioventricular valves open and the semilunar valves close, allowing the ventricles to fill with blood. In contrast, during ventricular systole, when the ventricles contract, the atrioventricular valves close and the semilunar valves open, enabling the ventricles to eject blood into the arteries. This continuous cycle of relaxation, filling, and ejection maintains the blood flow. The heart performs the crucial function of pumping blood throughout the body. As part of its rhythmic cycle, the ventricles relax and fill with blood, followed by contraction to eject the blood. This cycle repeats, ensuring a continuous flow of blood. However, due to the nature of the cardiac cycle, the ejection of blood into the arteries is not constant. As a result, both blood pressure and blood flow in the arteries exhibit a pulsatile pattern. During ventricular systole (contraction), blood pressure and flow increase, while during ventricular diastole (relaxation), they decrease. In Figure1, you can observe a graphical representation of changes in systemic arterial blood pressure, which was directly measured using a small catheter inserted into an artery and connected to a pressure measuring and recording device [1]. Figure 1. graphical representation of changes in systemic arterial blood pressure [1] Systolic pressure refers to the peak arterial pressure that occurs during ventricular systole, which is the contraction phase of the heart. In a resting adult, the typical range for systolic pressure is between 100 𝑎𝑛𝑑 139 𝑚𝑚𝐻𝑔. On the other hand, diastolic pressure represents the lowest arterial pressure experienced during ventricular diastole, the relaxation phase of the heart. For a resting adult, the normal range of diastolic pressure falls between 60 𝑎𝑛𝑑 89 𝑚𝑚𝐻𝑔. Pulse pressure refers to the mathematical difference between systolic pressure and diastolic pressure. It is influenced by various factors, including the stroke volume of the heart, heart rate, and peripheral resistance. When stroke volume increases, such as during exercise, systolic pressure tends to rise more than diastolic pressure, resulting in an increase in pulse pressure. In the systemic circuit, blood is pumped out of the left ventricle into systemic arteries, then it flows through arterioles, capillaries, venules, and veins before returning to the heart for circulation through the pulmonary circuit. The flow of blood in a closed circuit like the systemic circuit is determined by the pressure energy propelling the flow and the resistance offered by the blood vessel walls and the internal viscosity of the blood [1]. The relationship between flow (F), pressure (P) causing the flow, and resistance (R) to the flow can be expressed as follows: 𝑃(mmHg ) 𝐹(liters/min) = 𝑅 Mean arterial pressure (MAP) represents the pressure that lies between systolic and diastolic pressures. It is a continuous pressure that is derived from the pulsatile pressure of the cardiac cycle. This pressure determines the average blood flow rate throughout the circulatory system. The ventricle spends more time in diastole than in systole during one heartbeat, which leads to an approximation of the geometric mean rather than a simple mathematical average of systolic and diastolic pressures. There are two equations commonly used to calculate Mean Arterial Pressure (MAP): 𝑝𝑢𝑙𝑠𝑒 𝑝𝑟𝑒𝑠𝑠𝑢𝑟𝑒 𝑀𝐴𝑃1 = + 𝑑𝑖𝑎𝑠𝑡𝑜𝑙𝑖𝑐 𝑝𝑟𝑒𝑠𝑠𝑢𝑟𝑒 3 𝑠𝑦𝑠𝑡𝑜𝑙𝑖𝑐 𝑝𝑟𝑒𝑠𝑠𝑢𝑟𝑒 + 2𝑑𝑖𝑎𝑠𝑡𝑜𝑙𝑖𝑐 𝑝𝑟𝑒𝑠𝑠𝑢𝑟𝑒 𝑀𝐴𝑃2 = 3 Systemic arterial blood pressure is often assessed using indirect techniques since direct methods, which involve invasive procedures, are not practical or convenient for routine measurements. It's crucial to acknowledge the drawbacks of indirect measurement, as it can only provide an estimation of the actual blood pressure. Additionally, the accuracy of indirect methods may be influenced by factors such as the listener's ability to perceive sound changes accurately. Moreover, the quality and calibration of the equipment used can also impact the reliability of indirect measurements [1]. The typical indirect approach for assessing systemic arterial blood pressure involves utilizing a stethoscope or microphone alongside a sphygmomanometer. This technique is known as the auscultatory method, which essentially entails using diagnostic monitoring via a stethoscope to listen to the internal organ sounds [1]. The sounds heard during the measurement of blood pressure are called Korotkoff Sounds. Arterial pressure is measured by wrapping an inflatable rubber cuff, connected to a pressure gauge, around the arm. The cuff is then inflated to compress the underlying artery, and the healthcare provider listens to the sounds using a stethoscope or microphone placed over the vessel beneath the cuff, look at Figur2 [1]. Figure 2.measuring Arterial pressure [1]. Sound is produced by the turbulent flow of blood through a compressed vessel. When the pressure applied by the cuff exceeds the arterial pressure during systole, the artery collapses, and blood flow ceases, resulting in the absence of sound. By slowly reducing the cuff pressure, blood flow resumes as the cuff pressure falls just below systolic arterial pressure. At this moment, a distinct tapping sound, known as the first sound of Korotkoff, can be heard using a stethoscope or microphone placed over the artery. The cuff pressure at which this sound is first heard is typically taken as an approximation of systolic pressure. As the cuff pressure is further decreased, the sounds become louder (sometimes resembling a swishing noise), and then abruptly become muffled, representing the second sound of Korotkoff, indicating diastolic pressure. Eventually, the sounds disappear altogether as the pressure cuff no longer compresses the vessel, allowing normal, non-turbulent blood flow to resume. Since it is easier to identify the point at which the sound disappears compared to when it becomes muffled, and since there is only a small pressure differential between the two, the absence of sound is commonly used as an indicator of diastolic pressure [1]. Figure 3. Summary [1]. 3. METHOD Figure 4, Alternate electrode lead attachment [1]. 4. DATA and CALCULATIONS 1. Systolic Measurements Table 1. Systolic Data Systolic Pressure mmHg Condition Trial Audibly Detected Pressure (Event marker) mmHg Average Pressure (Calculate) Microphone Detected Pressure (In data, unmarked) Average Pressure (Calculate) mmHg mmHg mmHg A B Δ Average Pressure B minus Average Pressure A mmHg Left arm, seated Right arm, seated Right arm, lying down Right arm, after exercise* 1 119.5 mmHg 2 116.07 mmHg Δ 3.43 mmHg 1 141.48 mmHg 2 128.91 mmHg Δ 12.57 mmHg 1 123.35 mmHg 2 126.68 mmHg Δ 3.33 mmHg 0.93 mmHg 1 171.5 mmHg 176.5 mmHg 117.785 mmHg 125.85 mmHg 118.61 mmHg 122.23 mmHg 4.445 mmHg 138.805 mmHg 3.61 mmHg 131.205 mmHg 6.19 mmHg 2.24 mmHg 135.195 mmHg 144.48 mmHg 133.13 mmHg 10.35 mmHg 125.015 mmHg 131.67 mmHg 130.74 mmHg 5 mmHg *For ‘Right arm, after exercise’ recording, calculate the Delta difference between the ‘Audibly Detected Pressure’ and the ‘Microphone Detected Pressure’ values, and record the result in the right column. 2. Diastolic Measurements Table 2. Diastolic Data Diastolic Pressure mmHg Condition Trial Audibly Detected Pressure (Event marker) Average Pressure (Calculate) Microphone Detected Pressure Average Pressure (Calculate) (In data, unmarked) A B 1 73.66 mmHg 2 90.42 mmHg 90.71 mmHg Δ -16.76 mmHg -13.17 mmHg 1 72.53 mmHg 2 89.42 mmHg 89.42 mmHg Δ -16.89 mmHg -11.44 mmHg 1 76.80 mmHg 2 79.10 mmHg 82.16 mmHg Δ -2.3 mmHg -3.91 mmHg Left arm, seated Right arm, seated Right arm, lying down 77.54 mmHg 82.04 mmHg 77.98 mmHg 80.97 mmHg minus Average Pressure A 84.125 mmHg 2.085 mmHg 83.7 mmHg 2.73 mmHg 80.205 mmHg 2.255 mmHg 78.25 mmHg 77.95 mmHg Δ Average Pressure B Right arm, after 1 74.55 mmHg 78.83 mmHg 4.28 mmHg exercise* *For ‘Right arm, after exercise’ recording, calculate the Delta difference between the ‘Audibly Detected Pressure’ and the ‘Microphone Detected Pressure’ values, and record the result in the right column. 3. BPM Measurements Table 3. BPM Condition Left arm, seated Calculate the Mean Cycle* Trial 1 2 3 of Cycles 1 – 3 of Trial 1 – 2 means 1 87.96 bpm 83.56 bpm 87.71 bpm 86.40 bpm 84.26 bpm 2 83.33 bpm 82.64 bpm 80.42 bpm 82.13 bpm 1 81.74 bpm 81.96 bpm 82.64 bpm 82.11 bpm 2 81.36 bpm 79.36 bpm 79.78 bpm 80.16 bpm 1 76.14 bpm 75 bpm 74.62 bpm 75.25 bpm 2 76.53 bpm 75.75 bpm 76.72 bpm 76.33 bpm 84.50 bpm 82.87 bpm 82.87 bpm 83.41 bpm 81.13 bpm Right arm, seated Right arm, lying down Right arm, after exercise 1 75.78 bpm Table 4. Average Systolic Pressure/Average Diastolic Pressure SYSTOLE DIASTOLE BPM Calculations: Table 1 Sound Average Table 2 Sound Average Table 3 Pulse pressure Left arm, seated 4.445 mmHg 2.085 mmHg 84.26 bpm 2.36 mmHg Right arm, seated 3.61 mmHg 2.73 mmHg 81.13 bpm 0.88 mmHg Right arm, lying down 6.19 mmHg 2.255 mmHg 75.78 bpm 4 mmHg CONDITION Right arm, after exercise 5. 5 mmHg 4.28 mmHg 0.72 mmHg DISCUSSION Systolic pressure is the top-notch arterial pressure that struts its stuff during ventricular systole. Picture it as the heart flexing its muscles. When a relaxed adult is taking it easy, the systolic pressure usually hangs out between 100 and 139 mmHg, thus in Table1 the measurements align with our expectations. Now, diastolic pressure is a different story. It's the chilled-out arterial pressure when the ventricles are enjoying their downtime in diastole. It's like the heart taking a breather. In a resting adult, the diastolic pressure keeps it cool within the range of 60 to 89 mm Hg. So, remember, it's all about finding that balance between the heart's power play and its laid-back moments. thus, in Tabl21 the measurements also align with our expectations. As for the negative diastolic pressure when subtracting two diastolic pressure measurements could be due to errors in measurement or calculation, such as inaccuracies in recording or transcribing the values, or improper calibration of the measuring equipment. It could also indicate a physiological anomaly or a unique circumstance that deviates from the typical pattern of diastolic pressure. The reason behind the dissimilarities in measured values between the right arm and the left arm is all about those funky veins and their shapes. When accidents happen, they can mess up the vascular pathways, causing changes in blood flow. When we switch positions, like going from sitting to lying down, we don't have gravity pulling us anymore. So, the pressure drops, and blood pressure takes a dip when we're lying flat compared to sitting up. Now, after a good workout, we need more oxygen pumping through our bodies, right? So, our heart rate goes up, our systolic pressure gets all amped, and the blood is flowing faster. That means higher blood pressure. But need not worry, it's just a temporary thing. Our body knows how to find its chill and gradually brings the blood pressure down to keep things balanced. In order to calculate the pulse pressure, we just subtract the diastolic pressure from the systolic pressure. It tells us how much blood is getting pumped with each beat, like a little performance metric for your heart. The systolic value tends to jump more after exercise than the diastolic value. So, keep an eye on that. Now, at the start of the experiment, our ears might've heard a different beat than the stethoscope gadget, but as time went on, we got used to the sound and synced up like a well-oiled machine. 6. QUESTIONS 1) Note the difference in systolic pressure value between when: (a) the sound actually began, (b) was detected by the stethoscope transducer, and (c) was recorded, and the time when the observer first heard the sound and pressed the event marker keystroke. (Example: 141 𝑚𝑚𝐻𝑔– 135 𝑚𝑚𝐻𝑔 = 6 𝑚𝑚𝐻𝑔.) What factors could account for this difference? Would the observed difference be the same if measured by another observer? Explain your answer. Some individuals may find it challenging to perceive the Korotkoff sound, but this doesn't necessarily indicate any underlying issue. It's also possible for unwanted external noises to interfere, contributing to these difficulties. Such factors account for the variations observed. If the observed difference is a result of the individual's own circumstances, then there is no inherent discrepancy. However, if the observed difference stems from external noise, it is plausible to observe a variance. For instance, when another person conducts the measurement in a noise-free environment, the person being measured can expect a closer approximation to the accurate result. 2) Define the following terms: a) Does your systolic and/or diastolic arterial pressure change as your heart rate increases? When arteriole resistance remains constant, a higher heart rate can potentially lead to an elevation in the measured diastolic pressure. Additionally, diastolic pressure tends to follow systolic pressure, meaning that an increase in systolic pressure establishes a higher baseline for arterial pressure during the relaxation phase between contractions. b) How does this change affect your pulse pressure? The change in heart rate, specifically an increase, generally leads to a widening of pulse pressure. As the systolic pressure rises, it establishes a higher baseline for arterial pressure during the relaxation phase between contractions. Consequently, the difference between systolic and diastolic pressures, known as pulse pressure, tends to increase. c) How would you expect the systolic, diastolic and pulse pressures to change in a normal healthy individual as the heart rate increases? when the heart rate increases, it is expected that the systolic pressure will rise. This occurs because a higher heart rate leads to an increase in cardiac output, which in turn elevates the pressure exerted by the heart during contraction. On the other hand, the diastolic pressure may not change significantly or may even slightly decrease. The diastolic pressure is influenced by factors like peripheral resistance and arterial compliance, which may not be significantly impacted by a moderate increase in heart rate. As a result, the pulse pressure, which represents the difference between systolic and diastolic pressures, tends to widen as the systolic pressure increases while the diastolic pressure remains relatively stable. 3) Give three sources of error in the indirect method of determining systemic arterial blood pressure. error resulted from the observer, lack of standardization in measurement techniques, and equipment malfunction. 4) Define pulse pressure. Explain, in terms of changes in systolic and diastolic pressures, why pulse pressure increases during exercise. Mathematical difference between systolic pressure and diastolic pressure. When the volume of blood ejected per beat (called stroke volume) increases at the beginning of exercise, systolic pressure increases more than diastolic pressure, resulting in an increase in pulse pressure. 5) Give one reason why blood pressure in the left arm may be different than blood pressure in the right arm of a Subject at rest. A blood pressure difference of a few points between arms isn’t usually a cause for concern and is quite normal. A repeated difference of more than 10 mm Hg in blood pressure measurement between the arms can be a sign of a health problem such as: Blocked arteries in the arms, known as peripheral artery disease, Stroke, Diabetes. Kidney disease [2]. REFERENCEs [1] R. Pflanzer and W. Mcmullen, “Physiology Lessons for use with the Biopac Student Lab Lesson 16 BLOOD PRESSURE Indirect measurement Ventricular Systole & Diastole Korotkoff sounds Mean Arterial pressure.” Available: https://www.biopac.com/wpcontent/uploads/L16v373.pdf [2] “When blood pressure is higher in one arm,” Mayo Clinic, 2019. https://www.mayoclinic.org/diseases-conditions/high-blood-pressure/expert-answers/bloodpressure/faq-20058230