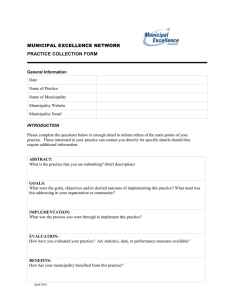
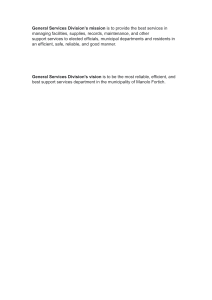
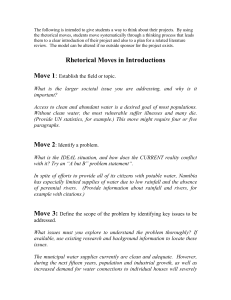
Health System Management Field Program Campus Presentation Prepared by Group A3 MBBS 40th Batch Group Members S.No. Name Roll Numbers 1 Amrit Pandey 1922 2 Gunjan Agrawal 1942 3 Nabin Ayer (Group Leader) 1954 4 Pradeep Oli 1957 5 Sachet Subedi 1967 6 Samir Sedhai 1970 7 Susmita Khatiwada 1982 8 Uday Pandey 1986 Field Sites and Activities S.No. Sites Duration Tasks Performed 1. Gulmi Hospital and Resunga Municipality, Resunga, Gulmi Day 1 to 21 • Hospital profile • Municipality profile 2. Syangja Hospital and Putalibazar Municipality, Putalibazar, Syangja Day 22 to 42 • Five year action plan 3. United Mission Hospital Tansen, Tansen Palpa Day 43 to 63 • Critical Analysis • Epidemiological Study Objectives General Objectives: • To acquire vital knowledge and insight into the management of the country's health system, and to cultivate the essential skills and concepts needed for efficiently managing municipal health systems. Specific Objectives : • To collect relevant information from different sources, analyze and interpret • To describe the health service delivery mechanism at regional, district and community level • To prepare hospital profile and municipality health profile • To analyze prevalence and epidemiological trend of health problems • To critically analyze the health system management and produce alternative solutions • To prepare five year plan to address a particular problem • To disseminate the information and effectively advocate Methodology Study Areas: • Gulmi - Gulmi Hospital and Resunga Municipality • Syangja - Syangja Hospital and Putalibazar Municipality • Palpa - United Mission Hospital Tansen Methodology (continued): Study Design: • Descriptive observational studies for hospital and municipal profiles • Descriptive cross-sectional study for critical analysis • Descriptive retrospective study for epidemiological study of the selected disease Methodology (continued): Study Population: • Patients presenting for OPD services Study Data: • Secondary for quantitative data • Interview from concerned authorities for qualitative data Study Duration: • 9 weeks Tools and Techniques Hospital Profile Technique Tools Source of Information Key informant interview Interview guidelines Medical Superintendent, Administrator, Consultants, Medical Officers, Nurses, Radiographer, Emergency in charge, Department in charges, laboratory personnel and other hospital staffs of Gulmi Hospital Observation Observation checklists Gulmi Hospital premises Record review Record review format Hospital Patient Records of Gulmi Hospital Literature review Literature review format Minimum Service Standards, MoHP Municipal and Municipal Health Profile Technique Tools Source of Information Key informant interview Interview guidelines Administrative In-charge, Health section chief of Resunga Municipality Health Office Chief Observation Observation checklists Resunga Municipality Office Record review Record review format Municipality Records, Records at Health Office Literature review Literature review format Resunga Municipality Annual Report 2079/80 Critical Analysis Technique Tools Source of Information Key informant interview Interview guidelines HR Manager,Medical Supervisor, Emergency In-charge, Emergency Patients of UMHT Observation Observation checklists Emergency Ward of UMHT Record review Record review format Emergency records of UMHT Literature review Literature review format Hospital Management Strengthening Program (HMSP) Epidemiological Study Technique Tools Source of Information Key informant interview Interview guidelines Doctors of internal medicine department Record review Record review format Hospital In-patient Records, Annual Reports of 3 fiscal year (2077/78, 2078/79, 079/80), Literature review Literature review format Class notes, Standard textbooks, HMIS Reports of the past three fiscal years, DoHS Annual Report 5 year plan on Safe Motherhood S.N. Activities Technique Tools Remarks 1. Selection topic Secondary data review Key informant Interview Data review format Interview guidelines Annual Report DOHS (2079/80) District Health Report, Syangja Records from Putalibazar Municipality 2. Situation Analysis Secondary Data review Interview with Stakeholders Data review formats Interview guidelines District Health report, Syangja Records from Syangja municipality Key informants: Health Coordinator Medical Superintendent, Syangja Hospital 3. Stakeholder Analysis Interview with Stakeholders Interview guidelines Stakeholders: Health Coordinator, Putalibazar Muncipality, Health Office, Birthing center Staffs Peripheral Institutions chief 5 year plan of Safe Motherhood S.N. Activities Tools Sources Problem Analysis Technique Key Informant interview 4. Interview Guidelines Key Informants: Health coordinator Sr. Health Officer, Health Office, Syangja 5. Objective Analysis Key Informant Interview Interview guidelines Key Informants: Health coordinator , Sr. Health Officer, Health office, Syangja 6. Logical Matrix Analysis Group Discussion Logical Framework Matrix 7. Budget Estimation Key informant Interview Interview Guidelines Members of Health division, Putalibazaar Municipality. Sr. Health Officer, Health Office, Syangja Key Informants: Health coordinator, Syangja Municipality, Finance Officer, Putalibazar Municipality ,Syangja Health Service Delivery : Structure Municipal and Municipal Health Profile Resunga Municipality Resunga Municipality • Area = 83.74 sq. km. • Province = Lumbini • District = Gulmi • Wards = 14 Resunga Municipality Organizational Structure Municipal Assembly Municipality Office Mayor Deputy Mayor Judiciary Committee Chief Administrative Officer Resunga Municipality Organizational Structure Administration Section Economic Administrative Section Revenue Section Account Section Chief Administrative Officer IT Section Education Section Public Health Section Technical Section Vetenirary Section Resunga Municipality Health System • There are currently 3 staffs in the health unit of the municipality which includes Health Unit Chief (Sr. ANM), 2 Sr. AHWs. Resunga Municipality Health System Resunga Municipality Health System Management • There are 4 health posts, 10 basic health service centres, 2 Urban health centres, total 16 institutes in 14 wards that fall under the health section of the municipality. Resunga Municipality Health System Budget • Top down: mostly • Bottom up: few, from local level • Source: mostly handled by Account section • Utilization: According to guideline, no difficulty in utilization Resunga Municipality Health System Logistics • Mostly bought from top down budget. • For other items (eg, Stationery): coordination with Store section. • Demand and Supply: enough • Information on logistics for health unit handled by health unit itself. Resunga Municipality Health System Planning • No 5 year plan. • Yearly planning is done. • Top down planning done according to budget and respective guidelines. • Bottom up planning done as per necessity. • For this fiscal year, planning for: Nutrition and Adolescent friendly Municipality. • Adolescent friendly: orientation, easy health access regarding family planning/mental health for adolescents organized by health section of municipality but there is no specific focal person. Resunga Municipality Health System Coordination • Coordination with health institutions in wards, with planning, account, education units. Resunga Municipality Health System Recording and Reporting • Hard copy, soft copy both • No specific guideline • No specific committee • No problem while utilizing information Resunga Municipality Health System Monitoring • Monthly meeting with units' head. • Analysis of data. • Discuss planning and program for institutes. Resunga Municipality Health System Evaluation • Done in monthly meeting. • Also done as needed every 3 months or 6 months. Resunga Municipality Health System Data Total Service Users New Service Users Service Receivers Vaccination Status CB-IMNCI Nutrition Program ANC Visits Hospital Deliveries Breastfeeding Contraceptives TB Treatment Hospital Profile IPO Model • Input • Infrastructure • Human resource • Logistics • Finance • Process • Planning • Organization • Direction • Recording and reporting • Coordination and Communication • Supervision and Monitoring • Output • Health Programs and Services 45 Organizational Structure 46 47 Logistics • The procurement committee decides upon the purchase. • Goods valued up to 10,00,000 can be procured with a single quotation. • For goods valued between >10,00,000 and <20,00,000, sealed quotation is required. • Minimum three suppliers are required. • Tender calls are made for goods exceeding 20 lakhs. 48 Management of expired logistics • A First Expired First Out (FEFO) principle is followed for inventory management. 49 Finance 50 Budgeting • Budget for the operating expenses is provided by the MoHP with federal government, provincial government and the internal revenue of the hospital. 51 Audit • The hospital runs its audit once a year internally and externally. • Internal audit is done as per the feasibility by कोष तथा लेखा नियन्त्रक कायाा लय • External audit is done by महालेखा परीक्षक कायाा लय 52 Hospital Development Committee • There are 5 members in the Hospital Development Committee including Chairperson of the committee, Mayor of Resunga Municipality, Chief District Officer, Senior Medical Superintendent and a member of the committee. 53 Planning • The overall planning of the hospital is done by the committee formed for the same purpose. • Budget for the planning comes from the MoHP with federal government, provincial government and the internal revenue of the hospital. • Planning is done on the 1st month of the fiscal year. • Additionally, meeting of the Hospital Development Committee, staffs takes place monthly as well as when needed to add up new changes to the planning process. 54 Recording and Reporting • The recording is done using HMIS tools and reporting is done every month. • EWARS tools is also used for reporting communicable diseases. • Daily patient records are done manually. 55 Coordination and Communication • The hospital coordinates and communicates with the local bodies specially in the health related programs where speciality and manpower of the hospital is required. 56 Supervision and Monitoring • Daily supervision and monitoring of hospital services are done by the respective incharges. • Internal analysis is performed by Medical Superintendent and Administrative head. • Self analysis is also done by using checklist of Minimum Service Standards. • Officials from MoHP also visit the hospital occasionally for supervision and monitoring. 57 No. of Emergency patients by fiscal year 58 OPD Services of Past 3 Fiscal Years 59 Inpatient Visit in Past 3 Fiscal Years 60 Types of Delivery in Last 3 Fiscal Year Types of delivery FY 077/78 FY 078/79 FY 079/80 Normal 527 534 494 CS 168 226 157 Vaccum/Forceps 17 8 3 Total 712 768 654 61 Family Planning New Acceptors 62 Surgical Intervention 63 Services 2077/78 2078/79 2079/80 X-ray 8801 15031 18373 Ultrasonogram (USG) Electrocardiogram (ECG) Lab services 5899 7268 7931 2807 4800 6868 21285 28412 31080 64 Other Services: • Medicolegal Services • Dialysis Service Critical Analysis in Emergency Services of United Mission Hospital Tansen Strengths: • There were upgraded modern Beds in ER. • Separate Procedure Room available. • Well-lit and Well-ventilated room. • Hospital provides 24-hr emergency services • Laboratory and imaging services available 24-hr round the clock. • Emergency Surgical services available round the clock. • Regular trainings are provided to ER staffs. • Hospital has prepared its own Mass Casualty management protocol. • Activities of ER are reviewed in every 3-months • Availability of oxygen, defibrillator and cardiac monitors. Weakness: • No separate Observation room in Emergency department. • There were no separate entry and exit doors. • Unavailability of CT in Emergency ward which is crucial in cases of neurovascular emergencies. • Human resource management in ER during peak hours is same as that of normal period. • No provision of automated digitalized records of patients admitted in ER. • Doctors are only on call during the night-shifts which may delay in making lifesaving decisions during the time. Opportunities: • Additional human resources can be mobilized during peak hours in Emergency ward. • A CT machine can be made available with 24-hr services. • Digitalization of medical records could be done which will make the patient’s medical record more easily accessible and retrievable. • The hospital can coordinate with organizations like local Red Cross societies which will be helpful in managing cases during mass casualties. Threats: • Patient crowding and overflow can occur in the emergency ward if no measures are taken to expand the ward. • Manpower and infrastructure issues may arise while installing new equipments. • Financial problems can arise if efforts are made to introduce additional manpower. • Hindrance in service delivery may arise due to hesitance of new consultants to work in the hospital. Five Year Plan on Safe Motherhood Situation Analysis Indicators National Gandaki Syangja Putalibazar 2078/79 2079/80 2078/79 2079/80 2078/79 2079/80 2078/79 2079/80 Percentage of pregnant women who had four ANC check ups as per protocol (4th, 6th, 8th and 9th month) 79.2 93.5 135 134.5 64.5 105.7 89.9 234 Pregnant women who attended first ANC visit (any time) 80 81 126.3 103.7 183.8 132.9 % of institutional deliveries 79 83.4 64.4 67.9 33.1 30.5 85.8 71 % of births attended by a skilled birth attendant (SBA) 75 80 63.5 66 Percentage of women who had 3 PNC check-ups as per protocol (1st within 24 hours, 2nd within 72 hours and 3rd within 7 days of delivery) 40.8 44.2 35.5 42.3 % of pregnant women who received Td2 and Td2+ 72 72 58.7 60 Maternal mortality ratio per 100,000 live birth 151 Neonatal Mortality rate per 1000 live births 33 % of pregnancies terminated by induced procedure at health facility 14.2 161 7.5 25 25.9 41 48 42.8 62 79 73 71 0 0 0 0 0 0.1 0 0 19.9 24.1 28 25.5 Indicators 2077/78 Putalibazar Municipality 2078/79 2079/80 Percentage of pregnant women who had four ANC check ups as per protocol (4th, 6th, 8th and 9th month) 40 89.9 234 Pregnant women who attended first ANC visit (any time) 108.3 183.8 132.9 64 85.8 71 0 0 42.8 28 62 79 0 0 0 0 0 0 28 25.5 73 71 % of institutional deliveries % of births attended by a skilled birth attendant (SBA) Percentage of women who had 3 PNC check-ups as per protocol (1st within 24 hours, 2nd within 72 hours and 3rd within 7 days of delivery) Maternal mortality ratio per 100,000 live birth Neonatal Mortality rate per 1000 live births % of pregnancies terminated by induced procedure at health facility % of pregnant women who received Td2 and Td2+ 28 69 Stakeholder Analysis Stakeholders Problem Interest Potential Linkages Municipality Office There was no such problem for the safe motherhood program. They are interested to further decrease home deliveries to zero. They are interested to make all existing deliveries to be attended by SBA. Nutrition program to the Postpartum mother is conducted supporting Safe motherhood. There is separate allocation of budget for transportation and ANC checkup to pregnant mother after institutional delivery. Outreach clinic were also focused on the Safe Motherhood program. Resources provided by the federal and provincial government. Health institutions and academic institutions for the implementation of program INGOs Local medias Stakeholder Analysis Stakeholders Problem Interest Potential Linkages MCH clinic Incharge Immunization is provided on only one day a week. They wish having immunization services at least two or three days a week. They wished increase in human resources as only 2 people are available now. There is availability of all required lab tests Availability of ANC checkup, immunization and family planning. Resources and facilities from the federal and provincial government. District health office for vaccines and other essential supplies. Municipality and other health institutions. Stakeholder Analysis Stakeholders Problem Interest Potential Linkages Birthing Center Staffs Portable USG machines are not available in some birthing center. The few available ones too, are nonfunctional. There is no facility for anomaly scan in the district. They wished to have portable USG machine in every birthing center. Skilled birth attendant are available in all birthing centers. All birthing center are well equipped with logistic as per there need. Beds are sufficient according to patient flow. Resources and logistics provided by local government. Problem Analysis Objective Analysis Safe Mother and child Increased Number of Institutional Deliveries Increased safe termination of pregnancies by induced procedure at health facility Promote Human Resources Development and capacity building Increase equity, assets and utilization of safe motherhood services Making Availability and adequate Physical assets and Health commodities Increase awareness about the health risks of unsafe termination of pregnancy Increased number of deliveries attended by Skilled Birth Attendant develop strategies that generate demand for SBAs and also reduce financial, geographic and cultural barriers to such services. Regular Monitoring of safe motherhood knowledge through community survey Objective and Strategies • The objectives and strategies are aligned with the National Safe Motherhood and Newborn Health Road Map 2030 endorsed by the Government of Nepal and the Global Strategy for Women's, Children's, and Adolescents' Health (2016-2030) endorsed by the World Health Organization (WHO). Vision • Putalibazar Municipality striving towards zero maternal deaths, disease, and suffering related to pregnancy and childbirth, through a comprehensive Safe Motherhood Program. Goal • To significantly improve maternal health outcomes in Putalibazar Municipality by addressing factors contributing to pregnancy-related complications and promoting early identification and access to essential healthcare services. Objective and Strategies • Objective 1: Strengthen the integration of comprehensive maternal health services, including • Preconceptional counseling and screening for high-risk factors. • Antenatal care with early identification and management of potential health complications. • Skilled birth attendance to ensure safe delivery and immediate newborn care. • Objective 2: Strengthen community engagement to promote healthy behaviors and advocate for improved access to healthcare services, contributing to a healthier environment for mothers and newborns. • Promote healthy habits within the community through existing outreach programs, emphasizing: Balanced diet and importance of good nutrition during pregnancy and for overall health. Benefits of regular health checkups for early detection of potential health issues. • Advocate for: Increased access to essential healthcare services within the community, focusing on facilities frequented by pregnant women and mothers. • Collaboration with relevant health authorities to explore the possibility of incorporating targeted awareness campaigns on the importance of Safe Motherhood and Chid Health Care. • Objective 3: Guarantee a reliable and efficient supply chain for essential maternal healthcare resources. • Secure a consistent supply of essential medicines, equipment, and supplies required for comprehensive maternal healthcare services. • Implement effective logistics management systems to ensure: Proper storage and handling of medicines, equipment, and supplies according to recommended guidelines. • Timely distribution of resources to healthcare facilities serving pregnant women and mothers. • Inventory management to maintain adequate stock levels and prevent stockouts. • Objective 4: Strengthen referral mechanisms and healthcare worker capacity to ensure early detection and management of potential health complications during pregnancy and the postpartum period. • Establish a comprehensive referral network connecting the Safe Motherhood program with various healthcare specialists and facilities. This network should include Obstetricians and gynecologists for specialized care during pregnancy and childbirth. Pediatricians for essential newborn care. Other relevant specialists based on identified needs within the community (e.g., nutritionists, mental health professionals). • Enhance the knowledge and skills of healthcare workers involved in the Safe Motherhood program: Training on early identification of potential health complications throughout pregnancy and the postpartum period. • Effective communication skills to guide women on the importance of regular checkups and seeking timely medical attention when needed. • Objective 5: Advocate for improved access to comprehensive healthcare services to address the health needs of mothers and newborns throughout pregnancy and the postpartum period. • Collaborate with relevant healthcare authorities to: Advocate for the integration of essential maternal health services within existing healthcare facilities frequented by pregnant women and mothers. • Explore the possibility of establishing outreach programs in areas with limited access to healthcare, focusing on prenatal and postnatal care. • Promote health awareness and education among pregnant women and mothers through: Educational workshops and seminars on various health topics relevant to pregnancy, childbirth, and newborn care. • Dissemination of informative materials (e.g., brochures, posters) on healthy practices, nutrition, and early detection of potential health complications. • Objective 6: Expand the reach and impact of the Safe Motherhood Program across all 14 wards through strategic implementation and resource allocation. • Increased community engagement activities. • Deployment of additional healthcare personnel. • Establishment of satellite clinics or outreach programs in remote areas. • Objective 7: Mitigate the disruption of essential maternal healthcare services during natural disasters and public health emergencies. • Collaborate with relevant authorities: Health department: Establish communication channels to: Stay informed about the evolving situation and public health priorities. Coordinate the program's response efforts with broader emergency response measures. • Disaster management agencies: Advocate for the inclusion of the program's needs within local disaster preparedness plans, ensuring: Access to safe birthing facilities and essential supplies in emergency shelters. • Continuity of critical services like prenatal care and immunization for newborns. • Objective 8: Strengthen data collection and analysis capabilities to improve program monitoring and evaluation, leading to better maternal health outcomes. • Data collection: Include relevant indicators related to maternal health outcomes like prenatal care access, birthing complications, and newborn health. • Data analysis: Analyze collected data to identify trends, correlations, and areas where program interventions are most effective. • Utilize the findings to refine program strategies and resource allocation for achieving optimal maternal health outcomes. Targets By the end of 2085/86: ➢ Institutional Delivery: (current 71%) 2080/81: 80% 2081/82: 85% 2082/83: 90% 2083/84: 95% 2084/85: 99% ➢ Eight ANC visit as per protocol: (current 91%) 2080/81: 92% 2081/82: 94% 2082/83: 95% 2083/84: 98% 2084/85: 99% ➢ ➢ Delivery Conducted by SBA: 42.8% 2080/81:50% 2081/82:60 % 2082/83:70 % 2083/84:80% 2084/85:90% Four PNC checkup as per protocol: (National Target 90% by 2030, current 96.7%) 2080/81: 97% 2081/82: 98% 2082/83: 98% 2083/84: 99% 2084/85: 100% (complete PNC visit municipality) Logical Framework Matrix OBJECTIVES/VERIFIABLE INDICATORS NARRATIVE SUMMARY MEANS OF VERIFICATION ASSUMPTION GOAL Enhance the health and well-being of mothers, newborns, and their families in Putalibazar municipality. Percentage of pregnant women receiving at least four antenatal care visits Maternal Mortality Ratio (MMR) Percentage of deliveries attended by skilled birth attendants Neonatal mortality rate • • Percentage of pregnant women receiving at least four antenatal care visits Skilled Birth Attendance (SBA) Rate Postnatal Care Coverage Neonatal Immunization Coverage Family Planning Acceptance Rate • HMIS data Vital registration data • system • Strong support and prioritization of maternal health initiatives from local government authorities in Putalibazar municipality. Strategies to ensure the program's long-term viability beyond initial funding or support. PURPOSE Enhance access to and utilization of essential maternal healthcare services, contributing to improved maternal and newborn health outcomes in Putalibazar municipality. • • HMIS data for Putalibazar municipality Facility delivery records Community-based surveys Political commitment Alignment with National Frameworks Stakeholder Engagement Willingness and acceptance of the program's interventions by the target population. Activities Timeline S.N. Activities FY2080/81 FY2081/82 A. Conducting awareness program, workshop, and health program in Community 1. Awareness program, workshop and health program in community 2. Orientation sessions to Aama Samuhas on Safe Motherhood 3. Special sessions on Safe motherhood services and SRHR to school children 4. Publication and broadcastingof information on Safe Motherhood on TV, radio and newspapers 5. World Safe Motherhood Day celebration on April 11 6. Establishment of information boards on Safe motherhood services in different areas ineach ward Experience sharing sessionsby those who have already received safe 7. motherhood services in Aama Samuha Meetings B. Resource Mobilization and Trainings FY 2082/83 FY 2083/84 FY 2084/85 8. 9. 10. 11. Expansion of birthing centers Provision of waiting homes for expecting mothers near the birthing centers Orientation to FCHV for safemotherhood services Maintenance and proper functioning of Ambulanceservices 12. Skilled Birth Attendant training for ANMs 13. Refresher training to all the healthcare worker from timeto time 14. Training on systematic andcomplete recording and reporting of HMIS forms C. Others 15. 16. 17. 18. Establishment of Emergencycommunity referral fund Development of IEC materials on safe motherhood and distribution to all health institutions Well-coordinated transportation and timely supply of essential logistics to healthcare facilities Motivation to ANMs and SBA conducting most delivery round the year through reward and recognition programs 19. Encouraging greater engagement of FCHVs through rewards and incentives 20. Promotion of Postpartum family planning devices 21. Nyano Jhola Program 22. Nutrition Programs for the Pregnant and Post-deliverywomen 23. ANC Visit Incentives 24. Conduction of needs-based research to strengthen SafeMotherhood program 25. Integrated SupportiveSupervision Budgeting S.No. Fiscal Year Budget (Rs.) 1. 2080/81 3930000 2. 2081/82 3745000 3. 2082/83 3865000 4. 2083/84 3145000 5. 2084/85 3215000 Total 17900000 Budget Allocation by Objective and Time (Budget in 1000) S.No. Objective 80/81 81/82 82/83 83/84 84/85 Total 1. To conduct awareness program, workshop, and health program in community 239 174 174 174 174 935 2. Trainings and Resource Mobilizations 2420 2300 2420 1600 1820 10560 1281 1281 1281 1281 1281 6405 3940 3755 3875 3055 3275 17900 3. Others Total Sources for the Budget • Many of the activities delineated in the plan come under national programs for which conditional grant is provided by the federal government. The remainder of the budget along with the budget for supervision and monitoring is expected to be invested by the municipality office itself. The federal government also provides Special Grant. S.No. Source Amount 1. Conditional Grants by federal government 8055000 2. Special Grant by Provincial Government 6265000 3. Municipality 3580000 Total 1,79,00,000 Monitoring and Evaluation Indicators Process Indicators Outcome Indicators • Number of health facilities providing safe motherhood services. • Number of health facilities providing Safe delivery services. • Number of health workers trained as skilled birth attendants. • Number of active FCHVs working in notifying health issues related to ‘sunaulo 1000 dine aama’. • Percentage of annual budget allocated for Safe motherhood program • Number of maternal and neonatal deaths recorded. • Percentage of ANC and PNC visits • Percentage of iron, folic acid and Vitamin A supplementation • Number of institutional deliveries • Percentage of birth attended by SBA. • Number of safe abortions performed • Number of used family planning devices Timing Indicators Timing of monitoring and evaluation Process indicators Once every two months by the Health Section of the municipality Outcome indicators Once every six months Supervising Team • The supervision, monitoring and evaluation committee shall consist of the following members: Mayor of the municipality Health Coordinator of Putalibazar municipality Medical Superintendent of Syangja Hospital Health post in-charges Health related experts At the end of each supervision, the supervision team will discuss the report of the process, the success, weaknesses, opportunities and constrains of the process based on the indicators. Epidemiological Study of COPD Rationale • COPD is the major public health problem in Nepal and one of the major causes of morbidity and mortality in the world (third leading cause of death worldwide). (Source: WHO) • COPD was one of the leading causes for morbidity and mortality in United Mission Hospital. (2nd highest IPD diagnosis and 2nd leading cause of IPD Mortality in FY 079/ 080) (Source: Annual Report, United Mission Hospital, 079/080) • Mortality and morbidity due to COPD can largely be prevented and treated if managed promptly and adequately. Example: by behavioural modification like smoking cessation, decreasing exposure to household smoke. Time based distribution of COPD cases 900 785 800 Number of COPD Patients 700 592 600 500 400 382 300 200 100 0 2077/78 2078/79 Fiscal Year 2079/80 Percentage of COPD cases among total inpatient cases in last three fiscal years Fiscal Year 2079/80 6,3 2078/79 5 2077/78 3,4 0 1 2 3 4 5 Percentage of COPD cases among all inpatient cases 6 7 Age-wise distribution of COPD in last 3 fiscal years Agewise Distribution of COPD 400 350 300 250 200 150 100 50 0 <40 40-49 50-59 2077/78 60-69 2078/79 70-79 2079/80 80-89 >90 Sex-wise distribution of COPD in last 3 fiscal years Sexwise Distribution of COPD 600 500 400 300 200 100 0 2077/78 2078/79 F M 2079/80 Ethnicity-wise distribution of COPD in last 3 fiscal years Ethnicity wise Distribution of COPD 350 300 250 200 150 100 50 0 Janajati Brahmin/Chhetri 2077/78 2078/79 2079/80 Dalit Risk Factors (at present) • Cigarette-smoking or exposure to environmental tobacco smoke since childhood. • Exposure to fumes and smoke from carbon-based cooking and heating fuels like charcoal and gas. • Occupational hazards (exposure to chemicals and pollutants). • Pneumonia and childhood respiratory infections. • Age and genetic pre-disposition. • Lower socio-economic status. • Acute exacerbation of COPD attributed to the cold climate (in winter) and pollen (in summer). Recommendations: To Department of Community Medicine: • Incorporation of Minimum Service Standards (MSS) protocols in the orientation sessions • Practical sessions on Budget Formulation for Five Year Plan Recommendations: To Gulmi Hospital: • Increase manpower (specially in radiology) and infrastructure for delivering health services • Provision of quarters to the doctors Recommendations: To Resunga Municipality: • Increase human resource in the health section • Increase collaboration with NGOs/INGOs • Greater attention to proper maintenance of health records Recommendations: To Syangja Hospital: • Fulfillment of vacant post • Effective Management of inpatient medical records. • Management of proper Ambulance facilities. Recommendations: To Putalibazar Municipality: • Regular supervision and monitoring of peripheral health institutions • Proper recording and reporting system Recommendations: To United Mission Hospital Tansen: • Management of Human Resources in ER during the Peak time. • Improve OPD based recording and reporting. • Expansion of the emergency services. • Fulfillment of ENT physician and other vacant posts. Learning Reflections: • We learned about the basic political structure and function of health service in local, provincial and national level • We got exposed to various constraints faced within the current healthcare system of Nepal to deliver services of optimum quality. • We understood how private, governmental and non-governmental health institutions play a coordinated role in providing health services to the general public • We understood detailed structure and function of community, district and provincial hospitals in Nepal. Learning Reflections (continued): • We learned how a particular aspect of the health service system can be critically analyzed, and how potential solutions can be reached • We learned how to extract, analyze and report epidemiological data • We learned to identify, prioritize and analyze health issues in a municipality and create a plausible plan to mitigate the issue with available resources • We understood various opportunities as well as constraints occurring as a result of transition to federal system. • Personal Lessons: Time management, Teamwork, Communication Appreciation Letters: Photos: Thank you!!