MIDWIFERY II PRESENTATION
MUGABE JOSHUA
Hyperemesis gravidarum(HG)
Definition
Signs and symptoms
Investigations
Management
Complications
Definition
Excessive nausea and vomiting in the first half of pregnancy
not responding to simple measures and destabilizing
pregnancy or/and the mother’s life.
It is most common in the first three months of pregnancy,
molar or multiple pregnancy.
Signs and symptoms
Severe nausea and feeling faint and dizzy when
standing(postural hypotension)
Persistent vomiting which can lead to dehydration
Dehydration, fatigue, light-headedness. Morning sickness,
anxiety, hyper salivation, ketosis, weight loss(>5% of prepregnancy weight).
Diagnosis
Period of amenorrhoea
History of nausea and excessive vomiting not responding to
simple measures
The woman has difficulty in performing normal daily duties
Weak, dehydrated, tachycardia
Differential Diagnosis
Malaria
Urinary Tract Infection (Pyelonephritis and Cystitis)
Gastrointestinal disorder
Hepatitis
Pancreatitis
Central nervous system disease
Investigations
Blood for:
Haemogram
Urea and electrolytes
Malarial parasites
Urinalysis
Ultrasound scan to confirm pregnancy and rule out molar or
multiple pregnancy
Management
Immediate Treatment
• Take history, review past records and examine the mother
• If the mother is dehydrated, start IV fluids (normal saline
alternating with 5% dextrose OR Ringer’s Lactate).
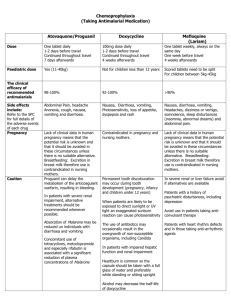
Treat with antiemetics:
• Metoclopramide (Plasil) IM (10 mg 8-hourly)
• OR Phenogan (promethazine hydrochloride) IM (12.5 mg 8-hourly
for 24 hours).
• OR Prochlorperazine (Buccastem, Stemetil) IM (12 mg once 12hourly)
Cont.
Note: If vomiting subsides, give antiemetics orally.
In addition to any of the above antiemetics, give Vitamin B
complex, 2ml in 500mls of Normal Saline or Ringer’s Lactate, single
dose
If condition doesn’t improve within 24 hours, consult or refer to
higher level facility.
• Use of ginger can help reduce hyperemesis.
• If patient improves, encourage oral and frequent fluid intake at least
three litres in 24 hours.
Counsel on the following
• Possible aggravating factors like if the pregnancy is not
wanted/planned, family problems and complications that may arise if
the condition continues
• Avoid nauseating drugs e.g. Metronidazole, Ferrous Sulphate,
(Iron), sweetened drinks, fatty foods
• Encourage the mother to eat dry foods like roasted cassava,
popcorns, hard corns which should be taken in the morning before
any meal
• Brush the teeth at night at least one hour after a meal Note: Avoid
brushing the teeth in the morning or immediately after meals
• Mother should come out of bed very slowly in the morning
Follow-up
• Review after 1 week. Then resume subsequent visits as per
antenatal schedule.
• Identify appropriate social support for the mother during the
course of treatment.
Note: Excessive vomiting can result to reduced levels of
vitamin B complex. Use of vitamin B complex prevents
Wernicke’s encephalopathies
COMPLICATIONS
Dehydration
Electrolyte imbalance
Weight loss
Preterm labor
Maternal morbidity such as micronutrient deficiency, GI bleeding
Low birth weight(LBW)
Preterm birth(PTB)
Small-for-gestational age(SGA)
Perinatal death
References
Essential Maternal and Newborn Clinical Care Guidelines for
Uganda
Uganda Clinical Guidelines 2020
https://bmcpregnancychildbirth.biomedcentral.co
https://www.ncbi.nlm.nih.gov
22 January, 2023
 0
0
![Questionnaire used in the study Demographics GENDER: M [ ] F](http://s3.studylib.net/store/data/006712173_1-21c851410b04058d524e1b79e54e32b0-300x300.png)