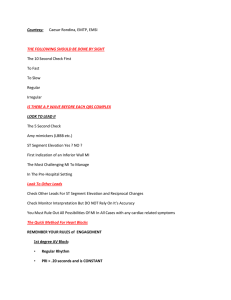
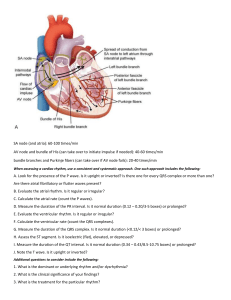
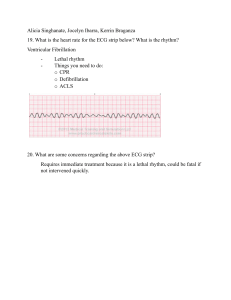
Analyzing a Rhythm Component Characteristic Rate • • • • The bpm is commonly the ventricular rate. Normal: 60–100 bpm Slow (bradycardia): <60 bpm Fast (tachycardia): >100 bpm Regularity • • • • Measure R-R intervals and P-P intervals. Regular: Intervals consistent Regularly irregular: Repeating irregular pattern Irregular: No pattern P Waves • • • • Same in size, shape, position Precedes each QRS Upright (positive), uniform, rounded Absent: Rhythm is junctional or ventricular. PR Interval • Constant: Intervals are the same. • Variable: Intervals differ • Normal: 0.12–0.20 sec and constant QRS Interval • Normal: 0.04–0.12 sec • Wide: >0.12 sec QT Interval • Beginning of R wave to end of T wave • Varies with HR. • Normal: 0.36 - 0.44 seconds Method 3: Six-Second ECG Rhythm Strip The best method for measuring irregular rates with varying R-R intervals is to count the number of R waves in a 6-sec strip and multiply by 10. This gives the average number of bpm. Using 6-sec ECG rhythm strip to calculate heart rate. Formula: 7 × 10 = 70 bpm If a rhythm is extremely irregular, it is best to count the number of RR intervals per 60 sec (1 min). Jones, MS ed, MHA, EMT-P, Shirley A. ECG Notes Interpretation and Management Guide. Philadelphia: FA Davis Company, 2005. Normal ECG Criteria Rate Atrial and ventricular rates are the same. Adults - 60 to 100 cycles/min Rhythm Regular P Wave Precedes the QRS Shape Uniformly rounded and upright without peaking or notches Size Amplitude 2.0 - 3.0 mm Duration of 0.06 - 0.12 seconds Deflection Upright in leads I, II, aVF, V2 through V6; Inverted in aVR; may be flat, inverted Biphasic in leads III, V1, and V2 PR Interval Adults – Consistent 0.12 - 0.20 second QRS Follows the P wave QRS interval is 0.06 - 0.10 second Q Wave Duration is <0.03 second Depth is 1-2 mm in leads I, aVL, V5, and V6 Deep QR or QS in aVR and possibly in lead III QT Interval <0.42 second (men) <0.43 second (women) ST Segment Follows isoelectric line Slight curve at proximal portion of the T wave Not depressed more than 1 mm T Wave Asymmetric and slightly rounded, without sharp points or large notches Deflection Should be in the same direction as QRS; Upright in leads I, II, aVF, V4 through V6; Inverted in aVR; Varied in all other leads Sinus Bradycardia Rate P wave QRS Conduction Rhythm 40-59 bpm Sinus Normal (.06-.10) P-R normal or slightly prolonged at slower rates Regular or slightly irregular This rhythm is often seen as a normal variation in athletes, during sleep, or in response to a vagal maneuver. Common causes: Inferior wall MI Hyperkalemia Increase intracranial pressure Hypothermia Myocardial ischemia Cardiac medication; Beta blockers, calcium channel blockers, antiarrhythmics Asymptomatic patient needs no treatment Interventions include: Stopping medications that suppress the SA node; digoxin, beta blockers, calcium channel blockers Identify the precipitating cause Medication; atropine, epinephrine, and dopamine Temporary or permanent pacing Posey, RN, MSN, Andrea D. "Interactive Online Continuing Education for Nurse Professionals.Feb. 2009 http://www.rnceus.com. Springhouse. ECG Interpretation Made Incredibly Easy! Philadelphia: Lippincott Williams & Wilkins, 2007. Sinus Tachycardia Rate P wave QRS Conduction Rhythm 101-160/min Sinus Normal Normal Regular or slightly irregular The clinical significance of this arrhythmia depends on the underlying cause. It may be normal. Common causes: Increased circulating catecholamine’s CHF Hypoxia Pulmonary embolism Increased temperature Stress Response to pain Asymptomatic patient needs no treatment Interventions include: Treatment of underlying cause Beta blockers Calcium channel blockers Posey, RN, MSN, Andrea D. "Interactive Online Continuing Education for Nurse Professionals.Feb. 2009 <http://www.rnceus.com>. Springhouse. ECG Interpretation Made Incredibly Easy! Philadelphia: Lippincott Williams & Wilkins, 2007. Premature Atrial Contractions Rate P wave QRS Conduction Rhythm Irregular atrial and ventricular rates Usually have a different morphology than sinus P waves because they originate from an ectopic pacemaker Normal Normal, however the ectopic beats may have a different P-R interval. Irregular - PAC’s occurring early in the cycle and they usually do not have a complete compensatory pause. PAC's occur normally in a non diseased heart. Common causes: Coronary or valvular heart disease Acute respiratory failure Pulmonary disease Electrolyte imbalances Fever Infectious diseases Anxiety Interventions include: Patient who are asymptomatic don’t need treatment Finding the underlying cause; fever, anxiety Digoxin, procainamide and quinidine Posey, RN, MSN, Andrea D. "Interactive Online Continuing Education for Nurse Professionals.Feb. 2009 <http://www.rnceus.com>. Springhouse. ECG Interpretation Made Incredibly Easy! Philadelphia: Lippincott Williams & Wilkins, 2007. Atrial Flutter Rate P wave QRS Conduction Rhythm Atrial 250-350/min; Ventricular conduction depends on the capability of the AV junction (usually rate of 150-175 bpm). Not present; usually a "saw tooth" pattern is present. Normal 2:1 or 4:1 Atrial to Ventricular Usually regular, but can be irregular if the AV block varies. Common causes: Mitral valve disease Hyperthyroidism Pericardial disease Acute MI After cardiac surgery The treatment depends on the level of hemodynamic compromise. The arrhythmia becomes more dangerous as the rate increases. Interventions include: Synchronized cardioversion is the treatment of choice. Otherwise, antiarrhythmics, digoxin and calcium channel blockers. Be alert for s/s of low cardiac output! Posey, RN, MSN, Andrea D. "Interactive Online Continuing Education for Nurse Professionals.Feb. 2009 <http://www.rnceus.com>. Springhouse. ECG Interpretation Made Incredibly Easy! Philadelphia: Lippincott Williams & Wilkins, 2007. Atrial Fibrillation Rate P wave QRS Conduction Rhythm Atrial rate: 400 bpm or greater; Ventricular: fast or slow Not present; wavy baseline is seen instead. Normal Variable AV conduction; if untreated the ventricular response is usually rapid. Irregularly irregular. (This is the hallmark of this dysrhythmia). Atrial fibrillation may occur suddenly, but it often becomes chronic. Common causes: Cardiac surgery Mitral regurgitation Mitral stenosis Hyperthyroidism Coronary artery disease Acute MI Pericarditis Interventions include: Digoxin, diltiazem, or other anti-dysrhythmic medications to control the AV conduction rate and assist with conversion back to normal sinus rhythm. Cardioversion may also be necessary to terminate this rhythm. Posey, RN, MSN, Andrea D. "Interactive Online Continuing Education for Nurse Professionals.Feb. 2009 <http://www.rnceus.com>. Springhouse. ECG Interpretation Made Incredibly Easy! Philadelphia: Lippincott Williams & Wilkins, 2007. Paroxysmal Supraventricular Tachycardia Atrial 160-250/min: Conducts to ventricles 1:1 unless a block is present. P wave Abnormal, possibly hidden in previous T wave Normal (unless associated with aberrant ventricular QRS conduction). P-R interval depends on the status of AV conduction Conduction tissue and atrial rate: May be normal, abnormal, or not measurable. Rate Paroxysmal Supraventricular Tachycardia (PSVT) may occur in the normal as well as diseased heart. Common causes: Stimulants Electrolyte imbalances Acute MI Cardiomyopathy Congenital anomalies Valvular heart disease Wolfe-Parkinson-White syndrome This rhythm is often transient and usually requires no treatment. Interventions include: Vagal maneuvers Digoxin, antiarrhythmics, adenosine Cardioversion Posey, RN, MSN, Andrea D. "Interactive Online Continuing Education for Nurse Professionals.Feb. 2009 <http://www.rnceus.com>. Springhouse. ECG Interpretation Made Incredibly Easy! Philadelphia: Lippincott Williams & Wilkins, 2007. Ventricular Tachycardia Rate P wave QRS Conduction Rhythm Usually between 100 to 220/bpm, but can be as rapid as 250/bpm Obscured if present and are unrelated to the QRS complexes. Wide and bizarre morphology Same as with PVCs Three or more ventricular beats in a row; may be regular or irregular. Ventricular tachycardia almost always occurs in diseased hearts. Patients usually have symptoms with this dysrhythmia. Ventricular tachycardia can quickly deteriorate into ventricular fibrillation and sudden cardiac death. Some common causes are: Coronary artery disease Acute MI Drug intoxication from digoxin, procainamide, or cocaine CHF Valvular heart disease Electrolyte imbalance such as Hypokalemia Interventions include: Immediate defibrillation and ACLS protocols. Identification and treatment of the underlying cause is also needed. Posey, RN, MSN, Andrea D. "Interactive Online Continuing Education for Nurse Professionals.Feb. 2009 <http://www.rnceus.com>. Springhouse. ECG Interpretation Made Incredibly Easy! Philadelphia: Lippincott Williams & Wilkins, 2007. Ventricular Fibrillation Rate P wave QRS Conduction Rhythm Unattainable May be present, but obscured by ventricular waves Not apparent Chaotic electrical activity Chaotic electrical activity This arrhythmia results in the absence of cardiac output and sudden cardiac death. Common causes: Myocardial ischemia MI Untreated ventricular tachycardia Heart disease Acid-base imbalance Severe hypothermia Electrolyte imbalances; hypokalemia, hyperkalemia, hypercalcemia Intervention includes: Immediate defibrillation and ACLS protocols. Identification and treatment of the underlying cause is also needed. Posey, RN, MSN, Andrea D. "Interactive Online Continuing Education for Nurse Professionals.Feb. 2009 <http://www.rnceus.com>. Springhouse. ECG Interpretation Made Incredibly Easy! Philadelphia: Lippincott Williams & Wilkins, 2007. Asystole/Ventricular Standstill Rate P wave QRS Conduction Rhythm None May be seen, but there is no ventricular response None None None Asystole is ventricular standstill. The patient is completely unresponsive, with no electrical activity in the heart and no cardiac output. Interventions include: Identify the cause CPR, 100% oxygen, IV Intubation Epinephrine 1.0 mg., IV push, q3-5 minutes Posey, RN, MSN, Andrea D. "Interactive Online Continuing Education for Nurse Professionals.Feb. 2009 http://www.rnceus.com. Springhouse. ECG Interpretation Made Incredibly Easy! Philadelphia: Lippincott Williams & Wilkins, 2007.