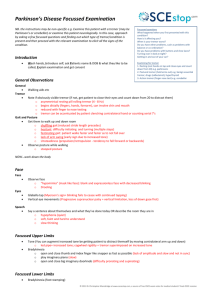
Deep Brain Stimulation for Movement Disorders Esmiralda Henderson, M.D. Mercy Medical Center Neurological Surgery Disclosures • No financial relationships. • Investigational treatments will be discussed. Overview • Deep brain stimulation (DBS) uses a surgically implanted medical device, similar to a cardiac pacemaker, to deliver a carefully controlled electrical stimulation to precisely targeted areas in the brain. • It works by electrically stimulating specific structures in a neural circuit that is involved in producing unwanted symptoms. Overview • • • • Parkinson’s Disease – FDA approved, 2002. Essential Tremor – FDA approved, 1997. Dystonia – FDA approved (HDE), 2003 Other conditions: Chronic pain, OCD (HDE, 2009), depression, Tourette's disease, Alzheimer’s, obesity, addiction, cluster headache, secondary tremors. Neuromodulation Dystonia Parkinson’s disease Essential Tremor Chronic Migraine * Chronic Pain RSD Failed back Gastroparesis Obsessive Compulsive Disorder Depression * Epilepsy * Bradycardia Heart Failure Tachycardia Angina Obesity * Bowel Disorders * Interstitial Cystitis * Urinary Incontinence History of stereotactic surgery and deep brain stimulation Progression • Understanding that deep brain structures are involved in the movement disorders. • Destruction of structures. • Stereotactic focused destructions. • Delineating the circuits involved in the disease. • Focused deep brain stimulation. Meyer’s approach to the basal ganglia. (Meyers R. The surgery of the hyperkinetic disorders. In: Vinken PJ, Bruyn GW, eds. Diseases of the Basal Ganglia. New York: North-Holland Publishing, 1968: 844-878.) The Horsley-Clarke Stereotactic Device was first reported in Brain (31:45-124, 1908) First DBS implants • 1975 – fist chronic therapy via DBS by Russian neuroscientist Natalia Bekhtereva. • Stimulation at high frequency inhibited activity of the tremor causing area of the brain. Effects were similar effects to the ablation with reversibility of the therapy. Pacemakers: 1957 Model 5800 1957 History • 1980’s - deep brain stimulation for tremor is systematically used in France and popularized by Dr. Alim Benabid. Present • > 100,000 DBS implants worldwide. • >7000 published articles on DBS. • Well established safety profile for three decades. • Technological evolution. • Therapy that is reversible and adjustable. A B D C A B D C DBS electrical stimulation A B D C Candidate Selection via Multidisciplinary Approach • • • • • • • Neurologist Movement Disorder Neurologist Neurosurgeon Neuropsychiatrist/psychologist Neurophysiologist PM&R Specialized OR suite Parkinson’s Disease • Neurodegenerative disorders that begins with the destruction of substantia nigra pars compacta. • Progressive loss of dopamine results in abnormal electrical activity in the brain. • Medications help, but many of patients become treatment resistant over time. • 50,000-60,000 new cases each year. • Over one million people who currently have PD. Parkinson’s Disease • Motor symptoms: • • • • • Tremor (resting) Rigidity (stiffness) Akinesia/bradykinesia (absence/slowness of movements Gait shuffling, freezing. Postural instability. • Non-motor symptoms: dementia, impulsivity, depression – late stages. Patient Selection –Parkinson’s Disease • Idiopathic PD • Bradykinesia, tremor, rigidity – maximized on medical management with poor symptomatic control. • Medication response: >30%. • Significant tremor that never responded to medications. • ON/OFF fluctuations and bothersome dyskinesias. Disease Severity Mild Signs of levodopa “wearing-off” Patient Symptoms Treatment Moderate Agonists Levodopa, COMT inhibitors, others Severe Dyskinesia, “On-Off” Motor Fluctuations DBS Postural Instability, Freezing, Falls, Dementia Target Hamani C et al. Brain 2004;127:4-20 Essential tremor • Very common. • Prevalence – 0.4-5.5%, in population over 65 – up to 14%. • Often under-diagnosed and undertreated. • Progressive. • 50% of patients fail medical management. Essential Tremor • It is characterized by an action or postural tremor in the frequency range of 4 to 12 Hz. • Alcohol transiently diminishes tremor amplitude in 50% to 90% of cases, although this may worsen after the effect of alcohol has worn off. • The location varies. Approximately 90% of patients have tremor in their upper extremities, 30% have a head tremor, 20% have a voice tremor, 10% have a face or jaw tremor, and 10% of ET patients may have a lower limb tremor. Essential tremor subtypes • Hereditary ET, for patients who fulfill consensus criteria for definite or classic ET and also have a family of at least one affected relative in the immediate family. The onset of tremor in the patient and the family member must occur prior to age 65 years. • Sporadic ET, for patients who fulfill the consensus criteria for definite or classic ET, but do not have an immediate family member with ET, and whose age at onset of ET is younger than 65 years. • Senile ET, for patients who have definite or classic ET according to consensus criteria, but who develop ET at or after the age of 65 years. Patients may or may not have a family history of ET. Patient Selection – Essential Tremor • Proper diagnosis. • Tremor that is maximized on medical management with poor symptomatic control. • Medications are contraindicated or side effects are intolerable. • Tremor is severe enough to interfere with ADLs, job duties, social interactions. ET DBS Target Target: VIM Axial View DYSTONIA • A syndrome of spontaneous sustained muscle contractions, with frequently twisting and repetitive movements, or abnormal postures. • Third most common movement disorder • Repetitive patterned movements • Often exacerbated by voluntary motor activity • Genetic component – Autosomal dominant mutation – DYT genes Patient Selection - Dystonia • Primary and secondary dystonia. • Failed conservative management. • Functional incapacitation. • Children included. General considerations in patient selection • Stable medical co-morbidities. • Stable cognition and psychiatric illnesses. • Good social support system and commitment to programming sessions. • No structural lesions. Target Hamani C et al. Brain 2004;127:4-20 Procedural Overview In a frame-based system, the stereotactic arc is attached to the base of the frame. MACHADO A G et al. Cleveland Clinic Journal of Medicine 2012;79:S19-S24 ©2012 by Cleveland Clinic Post Operative Course and Recovery Programming takes place 4 weeks after the original surgery. Lesion effect. Patient has his/her own programmer to chose different programs and turn device on and off. Patients and caregivers are educated on device use. Outcomes – Parkinson’s Disease • Level I evidence demonstrating efficacy DBS Improvement in PD “ON” Time Without Dyskinesias Improves from 27% to 74% 19% 27% 7% 49% 74%* 23% Before Surgery (n=96) ‘ON’ with Dyskinesia 6 Months After Surgery Bilateral STN Activa® Implant (n=91) ‘ON’ without Dyskinesia ‘OFF’ * The Deep-Brain Stimulation for Parkinson’s Disease Study Group. Deep-brain stimulation of the subthalamic nucleus for the pars interna of the globus pallidus in Parkinson’s disease. N Eng J Med. 2001;345:956-63. Medtronic DBS Therapy Clinical Summary, 2009 PD Motor Symptoms Improvement Maintained After 5 Years • In a 5-year study, DBS significantly improved OFF-medication assessments of tremor, rigidity, and akinesia/bradykinesia OFF-Medication Motor Score Improvements* 6-month 1-year 3 years 5 years Tremor 79% 75% 83% 75% Rigidity 58% 73% 74% 71% Akinesia 42% 63% 52% 49% Essential Tremor Outcomes • Hand/arm tremor – 80% of patients have near complete tremor relief. 20% have significant relief of the tremor. • Head/neck/trunk/voice tremor – 50-60% relief of the tremor. May require bilateral implant. • Follow-ups of several years are established with good durability of the efficacy. • If disease progresses, then stimulation may be easily adjusted. Dystonia DBS • Improvement is not immediate – few months. • Primary/Idiopathic-best results: • DYT-1, generalized – 74% • Cervical, when it comes to focal dystonia. • Appendicular dystonia responds better than one with axial symptoms. • Secondary-inconsistent results: • Structural lesions – less responsive • Tardive dystonia are exceptions – best responder • Outcome 23-91% improvement. Adverse Reactions • • • • Every surgery has risks. Infection is most common: 3-4%. Major complications <1%. Hardware malfunctions. Frontiers • Same disease-new targets: pedunculopontine nucleus (PPN) DBS for gait abnormalities in PD. • New technology – Medtronic Activa PC+S • New movement disorders targeted – Tourette's disease. • MRI safety clinical studies. Conclusion • Multidisciplinary approach is essential. • Deep brain stimulation provides significant symptomatic relief and improves quality of life in well selected patients with certain movement disorders. • Thank You!