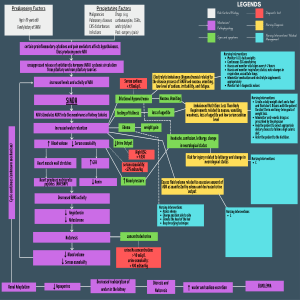
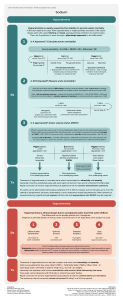
Diabetes Insipidus vs. Syndrome of Inappropriate Antidiuretic Hormone (SIADH) Prepared by Fidel Lim Common Causes Pathophysiology Diagnosis Manifestations Urine output Serum Sodium DI Brain injury/surgery/tumor (neurogenic/central), inadequate renal response to ADH (nephrogenic), excess water intake (primary) Lack of ADH Lab values (see below), water deprivation test Dilute urine Altered mental status Polyuria - Up to 20 liters/day = can lead hypovolemic shock High (which can lead to cerebral shrinkage) = neuro changes Serum Potassium Serum Osmolality Urine Osmolality Urine Specific Gravity Weight Medicine/Treatment Variable, could be increased High (greater than 295 mOsm/L) Low Low (typically <1.0005) Loss Synthetic antidiuretic hormones (desmopressin), chlorpropamide, and carbamazepine If treatment works Urine output will decrease and return to normal amount Fluids Increase intake (oral or IV) Other Monitor weight SIADH Small cell lung cancer, head injury, brain tumors, thiazide diuretics, SSRI, pneumonia, TB, GBS, brain infections Too much ADH Lab values (see below) Concentrated urine Altered mental status Reduced = can lead to pulmonary edema Low (dilutional hyponatremia) which can lead to cerebral edema) = neuro changes Variable Low (less than 275 mOsm/L) High High Gain ADH antagonist (conivaptan, tolvaptan). If sodium is critically low give hypertonic saline (3%). Loop diuretics may be use. Increase salt in the diet Urine output will improve or increase and sodium returns to normal Restrict Intake (800-1000 mL/day) Monitor weight