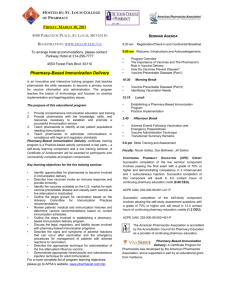
EDUCATION APhA Pharmacy-Based IMMUNIZATION DELIVERY A National Certificate Training Program Module 1. Pharmacists, Vaccines, and Public Health EDUCATION 16623 © 2017, American Pharmacists Association. All rights reserved. EDUCATION A Brief History of Vaccines Learning Objectives At the completion of this activity, participants will be able to: 1. Describe the effects of immunizations on morbidity and mortality rates of vaccine-preventable diseases in the United States. 2. Discuss Healthy People 2020 targets for vaccination rates in the United States. Most histories of vaccination trace their roots to Edward Jenner, who developed a vaccine that could protect against smallpox in the late 1700s (although there is evidence that vaccination was performed in other cultures centuries earlier). Jenner tested his theory that smallpox disease could be prevented by inoculating people with a related virus. He prevented smallpox by inoculating a child with liquid from a cowpox pustule from a milkmaid and published his work in 1798.3,4 Jenner’s work paved the way for additional research into vaccines, with the first licensed vaccines in the United States approved in 1914; before that time, other vaccinations had been used without regulatory oversight. These vaccines were followed by development of vaccines for a wide range of diseases (Table 1.1).3,4 Following the introduction of singleagent vaccines, many combination vaccines have been developed, such as the DTP vaccine, which protects against diphtheria, tetanus, and pertussis. Newer versions of vaccines also have been developed and in many cases have replaced the originally introduced versions.3,4 For a more complete history of vaccines, visit www.immunize.org/timeline and www.historyofvaccines.org/content/timelines/all. 3. Explain the expansion of the role of pharmacists as vaccine providers and describe the status of pharmacists’ authorization to administer vaccines throughout the United States. 4. Describe strategies for pharmacists to advocate for pharmacy-based delivery of vaccines. 5. Discuss the role of pharmacists as immunizers in emergency preparedness activities. 6. Identify resources that are useful for immunization providers and educators. Impact of Vaccines In the early to mid 1900s, people lived in fear of being stricken with polio, diphtheria, smallpox, tetanus, and other devastating diseases. With the licensure of the combined Vaccines and Public Health Immunization programs in the United States during the past century have nearly eliminated many of the vaccine-preventable diseases that were once common.2 In fact, routine vaccinations have prevented so much disease and averted so many deaths that many people may not even be aware of the devastation that can be caused by vaccine-preventable diseases. Despite the current successes, it is only through ongoing immunization efforts that these diseases will remain under control. Module 1. Pharmacists, Vaccines, and Public Health Death Rate per 100,000 Population per Year Immunizations are considered one of the greatest public health achievements in history.1 There have been significant reductions in the rates of infectious diseases in the Figure 1.1. U.S. Death Rate From Infectious Diseases 1900–1996 United States since the year 1900 (Figure 1.1).2 Many 1,000 40 States public health achievements have contributed to this Influenza Pandemic Have Health success, including improved sanitation and the advent Departments of antibiotics. The use of vaccines to prevent diseases 800 has been a key contributor to reducing rates of deaths caused by infectious diseases as well. Note the spike in the death rate that was associated with the 1918 600 Last Human-to-Human influenza pandemic, which resulted in 20 million Transmission of Plague deaths, including 500,000 in the United States.2 First Use of Penicillin 400 200 First Continuous Municipal Use of Chlorine in Water in the United States 0 1900 1920 Salk Vaccine Introduced Passage of Vaccination Assistance Act 1940 Year 1960 1980 2000 Source: Reference 2. 2 EDUCATION diphtheria and tetanus toxoids and pertussis vaccine in 1949, state and local health departments instituted vaccination programs that helped increase the distribution of vaccines. In 1955, the introduction of the Salk poliovirus vaccine led to federal funding of state and local childhood vaccination programs. In 1962, a federally coordinated vaccination program was established through the passage of the Vaccination Assistance Act—landmark legislation that has Table 1.1. Examples of Vaccines and Year Introduced a Year Disease 1798 Smallpoxa 1914 Rabies, tetanus, typhoid 1915 Pertussis 1923 Diphtheria 1935 Yellow fever 1945 Influenza 1955 Polio 1963 Measles 1967 Mumps 1971 MMR (including measles, mumps, and rubella) 1974 Meningococcal 1977 Pneumococcal 1981 Hepatitis B 1985 Haemophilus influenzae type b 1995 Hepatitis A, varicella 1998 Rotavirus 2006 Herpes zoster, human papillomavirus been renewed continuously and now supports the purchase and administration of a full range of childhood vaccines.3,4 Table 1.2 highlights accomplishments of vaccination efforts in the United States, comparing the recent number of cases with the historical peak number of cases for selected diseases.5-7 In addition to decreasing the number of cases of these diseases, the number of hospitalizations and deaths associated with them also have shown significant decreases. Despite these successes, work remains to be done. As shown in Table 1.2, there has been a recent resurgence of pertussis and there continue to be outbreaks of measles and mumps in this country. To date, smallpox is the only disease that has been eradicated from the planet, allowing vaccination to be discontinued. Smallpox was a devastating disease—approximately 30% of those who contracted smallpox died and those who survived were often scarred or blinded. After the development of the process of vaccination to prevent smallpox disease, the smallpox vaccine gradually reduced the viral menace around the world. Even so, 10 million people contracted smallpox worldwide in 1966, which resulted in 2 million deaths. A concerted global vaccination effort wiped out the virus completely, and the World Health Organization declared the global eradication of smallpox in 1980. In addition to avoiding the human toll of this disease, health care expenditures of $1 billion each year have been avoided because there is no longer any need to routinely vaccinate people against smallpox.8 Vaccines are incredibly cost-effective preventive health services. In addition to saving lives, vaccines prevent illness and reduce costs. It has been estimated that among children Not licensed in the United States until later. Source: References 3 and 4. Table 1.2. Rates of Selected Vaccine-Preventable Diseases in the 21st Century—United States Disease Max. Cases Year Cases 2012 Cases 2013 Cases 2014 Cases 2015 Cases 2016 Diphtheria 206,939 1921 1 0 1 0 0 Haemophilus influenza type b ~20,000 1980’s 30 18 27 16 22 Measles 894,134 1941 55 184 628 188 72 Mumps 152,209 1968 229 438 1,151 422 5311 Pertussis 265,209 1934 48,277 24,231 28,660 13,004 1,634 Rubella Congenital rubella syndrome 2.5 Million ~30,000 1964– 1965 9 3 9 0 8 1 4 1 2 0 Tetanus 601 1948 37 19 21 17 2 Varicella 221,983 1984 13,447 9,987 9,058 5,373 815 Source: References 5–7. Module 1. Pharmacists, Vaccines, and Public Health 3 EDUCATION born between 1994 and 2003, routine childhood vaccination has prevented: • • • • • 322 million cases of disease. 1.4 million hospitalizations. 56,300 deaths. $4.2 billion of direct health care costs. $1.5 trillion of societal costs. Despite the successes of vaccination efforts across the United States, risks remain. More than 40,000 adults in the United States die each year from vaccine-preventable diseases, such as influenza or pneumococcal diseases, or complications from the diseases, such as pneumonia.9 Increasing vaccination rates could help reduce the toll from these illnesses. Importantly, many diseases that are rare in the United States remain endemic in other parts of the world. International travelers may contract diseases overseas and infect unvaccinated or under-vaccinated individuals upon their return to the United States, resulting in an outbreak.10 For example, worldwide, there are estimated to be 20 million cases of measles and 164,000 measles-related deaths each year; several recent measles outbreaks in the United States have been traced to international travelers. In 2011, there were 222 measles cases in the United States that arose from 16 different outbreaks of 3 to 21 cases per outbreak. Of these cases, 39% occurred in individuals older than 20 years of age and 14% were in those younger than 1 year of age, who were too young to be vaccinated. It is important to note that in 84% of these cases, the individuals were unvaccinated or their status was unknown. The same year, there were 28,000 cases of measles in Europe. Additionally, there were a total of 5,311 mumps cases reported in 2016 in the United States.7 The number of pertussis cases in the United States is increasing with the highest incidence in infants. In 2012, there were more than 48,000 cases of pertussis reported, resulting in the deaths of 14 infants, who were too young to be vaccinated. These recent outbreaks of measles, mumps, and pertussis demonstrate that vulnerability to these diseases still exists, highlighting the need for continued vaccination efforts. Current Vaccination Rates Due to several national programs and concerted efforts to fully immunize children, immunization rates for young children are high in the United States. In 2014, rates were 90% or greater for children aged 19 to 35 months for many of the routinely recommended childhood vaccinations, although room for improvement remains (Table 1.3).11 While childhood immunization rates are reasonably high, vaccination rates for adolescents vary. For some vaccines, such as hepatitis B, vaccination coverage is above 90%. For others, such as human papillomavirus (HPV), vaccination rates remain disappointing (Table 1.4).12 Rates are also suboptimal in adults, leaving many patients vulnerable to vaccine-preventable diseases (Table 1.5).13 Notably, vaccination rates are lower for minorities than they are for whites. Table 1.3. Vaccination Rates in U.S. Children 19–35 Months of Age—2014 Vaccine Rate Diphtheria, tetanus, pertussis (4+ doses DTP, DT, or DTaP) 84% Polio (3+ doses) 93% Measles, mumps, and rubella (1+ doses) 92% Haemophilus influenzae type b (primary series +booster dose) 82% Hepatitis B (3+ doses) 92% Varicella (1+ doses) 91% Pneumococcal conjugate vaccine (4+ doses) 83% Combined 7-vaccine series 72% Source: Reference 11. Table 1.4. Vaccination Rates in U.S. Adolescents 13–17 Years of Age—2011 and 2014 Vaccine 2011 2014 Tdap ≥1 dose after age 10 years 78% 88% Meningococcal (MenACWY) ≥1 dose 71% 79% Human papillomavirus coverage Females ≥3 doses Males ≥3 doses 35% 1% 40% 22% Measles, mumps, and rubella ≥2 doses 91% 91% Hepatitis B ≥3 doses 92% 91% Varicella ≥2 doses among adolescents with no history of disease 80% 85% Tdap = tetanus and diphtheria toxoids and acellular pertussis. Source: Reference 12. Module 1. Pharmacists, Vaccines, and Public Health 4 EDUCATION Table 1.5. Vaccination Rates in U.S. Adults—2014 Vaccine (Target Group) Vaccination Rate Influenza (aged ≥19 years) 43% Influenza (aged 50–64 years) 48% Influenza (aged ≥65 years) 62% Influenza (HCP) 65% Pneumococcal (aged ≥65 years) 61% Pneumococcal (aged 19–64 years, high risk) 20% Tetanus in past 10 years (aged ≥19 years) 62% Tdap in past 9 years (aged ≥19 years) 20% Tdap (HCP) 2005–2011 42% Hepatitis B (≥3 doses, 19–49 years) 32% Hepatitis B (HCP) 61% Human papillomavirus (≥1 dose, aged 19–26 years) Females Males Herpes zoster (aged ≥60 years) Target vaccination rates have been established by Healthy People 2020, a national public health initiative that provides science-based, 10-year national objectives for improving the health of all Americans. Healthy People 2020 provides measurable objectives and goals intended to promote high-quality, longer lives free of preventable disease, disability, injury, and premature death. Table 1.6 shows the Healthy People 2020 goals for selected adult vaccination parameters along with baseline data from 2008.9 Pharmacists as Immunizers Pharmacists can advance public health through immunizations in several ways: educating and advocating, facilitating vaccinations by other health care professionals in their pharmacies, and administering vaccines to their patients. Pharmacists are logical providers of immunization services due to their accessibility and role as medication experts and experience providing high-quality patient care services. 40% 8% A Brief History of Pharmacists as Vaccine Providers 28% In the late 1800s and early 1900s, pharmacists supplied physicians with smallpox and other vaccines as well as diphtheria and other antitoxins. In later decades, the profession adopted several roles involving immunizations: storage, preparation, distribution, and education.14 This early involvement of HCP = health care personnel; Tdap = tetanus and diphtheria toxoids and acellular pertussis. Source: Reference 13. Table 1.6. Healthy People 2020 Baseline Data and Vaccination Goals for Adults Objective Baseline Data Targets for 2020 Increase the percentage of adults vaccinated annually against seasonal influenza Noninstitutionalized adults aged 18–64 years 25% in 2008 80% Noninstitutionalized high-risk adults aged 18–64 years 39% in 2008 90% Noninstitutionalized high-risk adults aged ≥65 years 67% in 2008 90% Institutionalized adults aged ≥18 years in long-term or nursing homes 62% in 2006 90% Health care personnel 45% in 2008 90% Increase the percentage of adults vaccinated against pneumococcal disease Noninstitutionalized adults aged ≥65 years 60% in 2008 90% Noninstitutionalized high-risk adults aged 18–64 years 17% in 2008 60% Institutionalized adults 66% of persons in long-term care facilities and nursing homes certified by the Centers for Medicare and Medicaid Services reported having up-to-date pneumococcal vaccinations in 2006 90% 7% of adults aged ≥60 years reported having ever received zoster (shingles) vaccine in 2008 30% Increase the percentage of adults vaccinated against zoster Source: Reference 9. Module 1. Pharmacists, Vaccines, and Public Health 5 EDUCATION pharmacists with immunology was short-lived and few pharmacists administered immunizations during much of the 1900s. The end of the 20th century saw a slow return of pharmacists to vaccine advocacy and delivery (Figure 1.2).14-24 While there were pockets of activity at the state level, a major meeting in 1994 stimulated a rethinking of the role of pharmacists. The meeting was initiated when the U.S. Secretary of Health and Human Services (HHS), Donna Shalala, contacted the American Pharmacists Association (APhA) to examine ways that pharmacists could help the country increase immunization rates. This led to the development of a model national immunization program for teaching pharmacists to immunize. Within a year, more than 1,000 pharmacists across the country had been taught to immunize through the APhA program. In 1996, at APhA’s Annual Meeting and Exposition, the Association called on pharmacists to get involved with immunizations. At the time, there were many more restrictions on pharmacists’ ability to immunize than there are today. APhA emphasized that all pharmacists, regardless of setting, can be involved in immunization advocacy and host others in the pharmacy. This remains true today. Many pharmacists are actively involved in administering a wide range of vaccines. In situations where pharmacists cannot administer vaccines themselves, they can educate patients and caregivers about the benefits of vaccines, and work to facilitate immunizations for patients. In August 1997, the APhA Board of Trustees adopted guidelines for pharmacy-based immunization advocacy and administration (Figure 1.3).25 APhA’s certificate training program, Pharmacy-Based Immunization Delivery, is a national certificate program for pharmacists that has been designed around these guidelines. As of 2017, more than 300,000 pharmacists have been trained through the program. Successes of Pharmacy-Based Immunization Delivery Pharmacists in many health care delivery settings are well-positioned to provide vaccination programs and services.15,26-28 The unique and essential contributions of pharmacists to immunization advocacy and delivery include: • Pharmacists are repeatedly cited among America’s most trusted professionals. • Pharmacists are considered one of America’s most accessible health care professionals. • Pharmacists have received extensive education and training about medications. Vaccines are medications and pharmacists are responsible for the effective use of all medications. Module 1. Pharmacists, Vaccines, and Public Health • Pharmacists are experienced in product storage, handling, and safeguarding inventory. • Pharmacists can identify specific people who need vaccines based on knowledge of the patient medication history or patient-specific disease-related risk factors. • Pharmacists can offer a useful bridge between patients and physicians by identifying an individual patient’s needs and facilitating referrals to health care providers when appropriate. • Pharmacists can offer extended hours of access in the evening, on the weekends, and during holidays, if immunizations are offered at those times. • Pharmacists are often located in local neighborhoods, providing convenient access for most patients. • Pharmacists are adept at electronic communications and can offer computerized records, facilitating the delivery of documentation. • Most pharmacies are capable of billing Medicare and other third-party payers for the vaccine product as well as administration of the vaccine. Because of these benefits, pharmacists can help to improve immunization rates. Research conducted when pharmacists began to offer influenza vaccinations found that overall vaccination rates improved.29 Today, pharmacists are widely accepted as providers of vaccines. Patients are satisfied with pharmacists’ services and believe that pharmacists are appropriate providers of vaccines.30-32 In addition, the physician community now generally welcomes pharmacists as immunizers. In 2002, the American College of Physicians–American Society of Internal Medicine position paper on the pharmacist’s scope of practice stated that their group “supports the use of the pharmacist as immunization information source, host of immunization sites, and immunizer, as appropriate and allowed by state law.”33 However, continued advocacy is needed with organized medicine and other stakeholders to support expanded immunization roles for pharmacists. Pharmacists’ accessibility and promotion of vaccines have had a substantial effect on public health. Community pharmacies in the United States offer convenience, accessibility, and extended hours of operation for the delivery of clinical services. The equivalent of the population of the United States enters a pharmacy each week. Pharmacies are geographically located in places where care is needed, including inner cities and rural communities. Additionally, 6 EDUCATION Figure 1.2. Historical Perspective of Pharmacy-Based Immunization Delivery Pharmacists oversee depots for diphtheria antitoxin. Pharmacists serve as vaccine advocates and facilitate vaccine delivery by hosting other health care providers to administer the vaccines in pharmacies. Mid to late 1800s Late 1800s to early 1900s 1984 Mid 1980s to mid 1990s Multiple breakthrough events occur: • More than 70 pharmacists are trained in injection technique through the GPhA Pharmacy and Immunization Program; 3 weeks later, these pharmacists help administer hundreds of doses of tetanus-diphtheria toxoids (Td) during a flood emergency. • The Washington State Pharmacists Association and the University of Washington develop a formal training program that leads to a certificate of competence for pharmacist immunizers. Georgia Pharmacy Association (GPhA) members help distribute meningococcal vaccine to 22,000 residents of Douglas County, Georgia, during a disease outbreak. 1995 APhA and the West Virginia University School of Pharmacy partner on a 5-year grant from the Centers for Disease Control and Prevention (CDC) to develop the Pharmacy Immunization Project—a demonstration project that involved nurses from public health departments immunizing children and adults in community pharmacies. • The American Pharmacists Association (APhA) is approached by the U.S. Secretary of Health and Human Services to examine ways that pharmacists can help the country increase immunization rates, prompting APhA to adopt immunization within its strategic activities. 1996 One of the most significant recognitions of the role of the pharmacist in immunizations is the inclusion of APhA as a liaison member of the CDC Advisory Committee on Immunization Practices (ACIP). Stephan L. Foster, PharmD, FAPhA, is named as the first pharmacist to represent APhA on ACIP and he continues to serve on the committee. 2001 American College of Physicians–American Society of Internal Medicine publish a joint position paper supporting pharmacists as immunization information sources, hosts of immunization sites, and immunizers. More than 300,000 pharmacists and student pharmacists have been trained through APhA’s Pharmacy-Based Immunization Delivery, a national certificate program for pharmacists. By year-end 1997 2002 2009­­­­–10 By 2017 Pharmacy-based immunizations on a large scale first occur through the Colorado Influenza Alert Campaign, with pharmacies hosting nurses to administer influenza vaccine injections. 1993 1994 APhA partners with the Mississippi Board of Pharmacy, the Mississippi Pharmacists Association, and the University of Mississippi to develop a model immunization program for teaching pharmacists to immunize. Pharmacists supply physicians with smallpox vaccine. More than 5 million doses of influenza vaccine are administered in America’s pharmacies each year. An estimated 15,000 pharmacies participate in vaccine advocacy and facilitation. More than 1,000 pharmacists across the country have been taught to immunize through the APhA program that was developed in 1996. Through a collaborative effort of multiple organizations, the Association of State and Territorial Health Officials releases a document titled “Operational Framework for Partnering With Pharmacies for Administration of 2009 H1N1 Vaccine” that serves as a guide for state and territorial health departments to establish partnerships with pharmacies to administer vaccinations during the 2009 H1N1 influenza pandemic. Pharmacists administer 10% of all H1N1 vaccine doses in the United States and are viewed as a crucial public health asset for their vital role in the response to the pandemic. Source: References 14–24. Module 1. Pharmacists, Vaccines, and Public Health 7 EDUCATION pharmacists are increasingly practicing in new models of care that can expand patient access. This widespread access has been recognized as a benefit by the Centers for Disease Control and Prevention (CDC). As of November 2015, nearly one in four adults who received an influenza vaccine were vaccinated in a community pharmacy or retail setting.34 In a 2016 open letter to pharmacists, HHS recognized pharmacists’ contributions to public health and thanked pharmacists for their role in improving immunization rates; (Figure 1.4).34 In this letter, HHS called upon pharmacists to help increase immunization rates by finding new ways to assess for vaccination needs, recommend, offer and document additional immunizations. Figure 1.3. Guidelines for Pharmacy Immunization Advocacy Guideline 1. Priority to Prevention Pharmacists should protect their patients’ health by being vaccine advocates. Pharmacists should adopt one of three levels of involvement in vaccine advocacy: • Pharmacist as educator (motivating people to be immunized). • Pharmacist as facilitator (hosting others who immunize). • Pharmacist as immunizer (protecting vulnerable people, consistent with state law). Pharmacists should: • Focus their immunization efforts on diseases that are the most significant sources of preventable mortality among the American people, such as influenza, pneumococcal, and hepatitis B infections. • Routinely determine the immunization status of patients, then refer patients to the most appropriate provider for immunization. • Identify high-risk patients in need of targeted vaccines and develop an appropriate immunization schedule. • Protect themselves and prevent infection of their patients by being appropriately immunized themselves. Guideline 2. Partnership • Identify high-risk patients in nursing homes and other facilities and ensure that needed vaccinations are considered either upon admission or in drug regimen reviews. Guideline 3. Quality Pharmacists must achieve and maintain competence to administer immunizations. Before administering vaccines, pharmacists should: • Be properly trained and evaluated in disease epidemiology, vaccine characteristics, injection technique, and related topics. • Be properly trained in emergency responses to adverse events; they should provide this service only in settings equipped with epinephrine and related supplies. • Question the patients and their families about contraindications and inform them in specific terms about the risks and benefits of immunization. • Receive additional education and training on current immunization recommendations, schedules, and techniques at least annually. Guideline 4. Documentation Pharmacists should document immunizations fully and report important events appropriately. Pharmacists should: Pharmacists who administer immunizations do so in partnership with their community. Pharmacists should: • Maintain perpetual immunization records and offer a personal immunization record to each patient. • Support the immunization advocacy goals and other educational programs of health departments in their cities, counties, and states. • Report adverse events following immunization to any appropriate primary care provider and to the Vaccine Adverse Event Reporting System (VAERS). • Collaborate with community prescribers and health departments. • Assist their patients in maintaining a medical home, including care such as immunization delivery. • Consult with and report immunization delivery, as appropriate, to primary care providers, state immunization registries [now known as immunization information systems], and other relevant parties. • Identify high-risk patients in hospitals and other institutions and ensure that appropriate vaccination is considered either before discharge or in discharge planning. Guideline 5. Empowerment Pharmacists should: • Educate patients about immunizations and respect patients’ rights. • Encourage appropriate vaccine use through information campaigns for health care practitioners, employers, and the public about the benefits of immunizations. • Educate patients and their families about immunization in readily understood terms. • Document any patient education provided and obtain written informed consent as recommended in their state before immunizing. Source: Reference 25. Module 1. Pharmacists, Vaccines, and Public Health 8 EDUCATION Immunization Success Stories Each year, APhA recognizes pharmacists who have made remarkable contributions to improve vaccination rates in their communities through the Immunization Champion Awards. APhA issues a call for Immunization Champion Award nominations in November, announces winners in February, and presents awards at the APhA Annual Meeting and Exposition in March. Expanding Opportunities to Administer Vaccines Opportunities for pharmacists to administer vaccines have expanded over the past few decades regarding locations where pharmacists immunize, types of vaccines administered by pharmacists, and age-groups to which pharmacists administer vaccines. Opportunities Based on Location Opportunities for pharmacists to educate, facilitate, or immunize exist at all levels of care. Every pharmacist can and should identify patients who are vulnerable to vaccinepreventable diseases and routinely recommend vaccination at every appropriate encounter. Initial pharmacy-based vaccination efforts took place in community pharmacies. However, pharmacists’ immunization efforts are not limited to community pharmacy sites. Today, pharmacists administer vaccines in a wide variety of practice settings and processes of care such as: • • • • • • • • • • • • Community pharmacies Ambulatory care clinics Community health centers Health systems Long-term care facilities Home health care settings Corporate sites Community sites (shopping areas, airports, health fairs, schools) Patient-centered medical homes and other innovative care models MTM encounters Medication reconciliation Travel health clinics Module 1. Pharmacists, Vaccines, and Public Health Vaccine Needs for Travel Health Patients traveling abroad often require specific vaccines related to their destination. For training to meet patients’ unique travel-related health care needs, see APhA’s Pharmacy-Based Travel Health Services advanced competency training in the Continuing Education section of www.pharmacist.com. Opportunities for pharmacists in various settings are numerous. For example, community pharmacists can use information in their pharmacy database to determine immunization needs for individual patients. Pharmacists can identify individuals who need vaccines just by completing a review of the patient’s age, medications, and medical history. Patients with chronic diseases such as cardiovascular disease, chronic lung disease, or diabetes are potential candidates for many vaccines, and these patients can be easily identified by the medications they take to manage their disease. (More information about identifying patients who require vaccines will be discussed in Module 4.) Patients admitted to hospitals or long-term care facilities will be cared for by a pharmacist at some point during their stay. These settings provide ample opportunity for pharmacists to promote, and often provide, immunizations. Although the institutional setting is different from the community pharmacy setting, the general roles of pharmacists in promoting immunizations are the same: to educate, to facilitate, and/or to administer. Just as community pharmacists can identify vaccine needs by reviewing a prescription profile, institutional pharmacists can identify a patient’s vaccination status while conducting medication reconciliation upon admission, unit transfer, or discharge. They can advocate vaccinations on ward rounds and at grand rounds for inpatients or get involved with discharge planning to ensure patients receive necessary vaccinations prior to discharge. When allowed by their state pharmacy practice act and employer, institutional pharmacists can become involved in administering vaccines to patients. Pharmacists in this setting also can supply drug information about vaccines; provide in-service training for pharmacy, nursing, or other personnel; and become involved in committees concerned with infection control. Other potential roles include developing policies on vaccination for employees, patients, and visitors. Institutional pharmacists 9 EDUCATION Figure 1.4. Letter to Pharmacists From the Department of Health and Human Services Requesting Help in Promoting and Providing Vaccinations DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Centers for Disease Control and Prevention (CDC) Atlanta, GA 30341-3724 September 29, 2016 Dear Pharmacist, The Centers for Disease Control and Prevention (CDC) recognizes and appreciates the increasingly important role that you play in public health, including vaccinating the public against seasonal influenza and other vaccine-preventable diseases. In fact, as of November 2015, nearly one in four adults who received an influenza vaccine were vaccinated in a community pharmacy or retail setting (http://www.cdc.gov/flu/fluvaxview/nifs-estimates-nov2015.htm), and there are now more than 280,000 immunization trained pharmacists. As of the middle of September, manufacturers reported having already distributed more than 90 million doses of 2016-2017 flu vaccine. Please begin to vaccinate your patients as you receive the influenza vaccine. Vaccination by the end of October is recommended, if possible, however, please continue to vaccinate your patients throughout the influenza season. Vaccine administered in December or later, even if influenza activity has already begun, is likely to be beneficial during the majority of the influenza seasons. For the 2016-2017 season, ACIP has made several updates and clarifications to its seasonal influenza vaccination recommendations: • Only injectable influenza vaccines are recommended this flu season. People aged 6 months and older should receive an appropriate formulation of either an inactivated influenza vaccine (IIV) or the recombinant influenza vaccine (RIV) with no preference for any recommended vaccine over another. The various vaccines are approved for different age groups. An age-appropriate vaccine should always be used. While some LAIV may be available in the form of FluMist Quadrivalent, that vaccine is not recommended for use this season because of concerns about its effectiveness. • The composition of 2016-2017 flu vaccines has been updated to better match circulating viruses. • An influenza vaccine with MF59 adjuvant (FLUADTM) is available for adults 65 years and older. People 65 years of age and older may receive this vaccine, highdose inactivated influenza vaccine (Fluzone High-Dose), or standard-dose inactivated vaccine. (continued on next page) Module 1. Pharmacists, Vaccines, and Public Health 10 EDUCATION Figure 1.4. Letter to Pharmacists From the Department of Health and Human Services Requesting Help in Promoting and Providing Vaccinations (continued) • The recommendations for flu vaccination of people with egg allergies have been modified: o Anyone with egg allergy can receive any licensed, age-appropriate, and recommended flu vaccine. For those with a history of severe allergic reaction to egg (any symptom other than hives), vaccination should occur in a medical setting and be supervised by a health care provider who can recognize and manage severe allergic conditions. o CDC has prepared an algorithm summarizing the new recommendations which is available at http://www.cdc.gov/flu/protect/vaccine/eggallergies.htm. • Children 6 months through 8 years of age who have previously received two or more total doses of any trivalent or quadrivalent influenza vaccine before July 1, 2016, only need one dose of 2016-2017 seasonal influenza vaccine. Children 6 months through 8 years of age who have not previously received two or more total doses of any trivalent or quadrivalent influenza vaccine before July 1, 2016 will need two doses of 2016-2017 seasonal influenza vaccine. Children 9 years of age and older need only one dose. Vaccine manufacturers have projected that as many as 157 million to 168 million doses of injectable flu vaccine will be available for the 2016-2017 season. Based on these projections, the supply of injectable flu vaccine should be sufficient to meet any increase in demand resulting from the recommendation to not use LAIV this season. Influenza vaccine information for providers and patients is available at http://www.cdc.gov/flu. As you and your colleagues begin your seasonal influenza vaccination efforts, please take this opportunity to also assess the other vaccination needs of your patients. We encourage and appreciate every effort you can make to implement the Standards for Adult Immunization Practice in your pharmacy, i. e. to find new ways to assess for vaccination needs, recommend, offer and document additional immunizations. Many pharmacies are taking the opportunity to promote zoster, pneumococcal and Tdap vaccination to their adult patients. Thank you for all that you do for your patients and for your continued public health contribution to a well-functioning “immunization neighborhood” in collaboration with healthcare providers in your communities. Sincerely, Nancy Messonnier, MD (CAPT, USPHS) Director National Center for Immunization and Respiratory Diseases Centers for Disease Control and Prevention Source: Reference 39. Module 1. Pharmacists, Vaccines, and Public Health 11 EDUCATION should advocate for all health care workers at the site to be up to date with their immunizations. Consultant pharmacists can increase immunization delivery in a variety of ways. They can recommend vaccines during drug regimen reviews; encourage mass immunization programs for residents, staff, and visitors; and administer vaccines. Federal regulations require all long-term care facilities that receive funding from Medicare to offer influenza vaccine to their residents annually and offer pneumococcal vaccine at least once during each resident’s stay or risk losing federal funding.35 Consultant pharmacists should take the lead in helping facilities comply with this regulation, and they can support vaccinations for staff and visitors. Changes in Medicare rules have made it easier for institutions—both hospitals and nursing homes/long-term care facilities—to implement standing orders for the administration of influenza and pneumococcal vaccine to patients by nurses and pharmacists. The goal of these changes is to improve vaccination rates in these high-risk patient populations. Notably, Medicare rules recognize pharmacists as one of the providers in institutional settings that standing orders should empower to administer vaccines. Innovative health care delivery models, such as patientcentered medical homes and accountable care organizations, that reward quality and are moving away from fee-for-service payment models have dramatically expanded in recent years due to financial pressures and the Affordable Care Act. Performance-based payment for health care is growing, and this payment structure is based on achievement of various quality measures, many of which include vaccination rates. For example, influenza and pneumococcal vaccination rates are among the quality measures that are used to assess accountable care organization performance. Immunization rates also are considered by the Healthcare Effectiveness Data and Information Set (HEDIS), which is a set of performance measures widely used by the managed care industry and other organizations.36 These developments offer important opportunities for pharmacists to make an impact and assist providers, health care teams, and plans meet quality metrics resulting in enhanced compensation. Pharmacists can work to improve immunization rates in their practices to help the practices deliver high-quality care. Pharmacists’ patient care services offer excellent opportunities to advocate for immunizations and administer vaccines. Many pharmacists regularly consider a patient’s vaccine needs as part of any MTM encounter. Pharmacists who provide Module 1. Pharmacists, Vaccines, and Public Health disease-state management services for patients with chronic conditions such as diabetes and asthma can include an assessment of patients’ vaccination status in these efforts. Finally, as a profession, pharmacists need to be role models for patients. All pharmacists should receive an annual influenza vaccination and be up to date on their other vaccines unless they have valid medical contraindications. Expanding Vaccination Offerings Initially, pharmacists’ vaccination efforts focused on seasonal influenza programs for adults. Today, pharmacists’ services are expanding to offer year-round vaccines across the life span. When pharmacists began their immunization activities a few decades ago, many states did not allow pharmacists to immunize. That is no longer the case. As of July 2009, pharmacists in all 50 states, Puerto Rico, and the District of Columbia have the authority to administer vaccines to varying degrees (Figure 1.5).24 However, state-level limitations on a pharmacist’s authority to immunize remain, such as restrictions based on the age of the patient or the type of vaccine being administered; these restrictions are subject to change at any time. Pharmacists must check with their state board of pharmacy before initiating any immunization service to determine their specific authority to immunize. As of July 2016, pharmacists in 48 states and territories may administer any vaccine.24 In other states, pharmacists are limited to certain subsets of vaccines. Pharmacists can administer influenza, pneumococcal, and herpes zoster vaccine in all states. Some states allow pharmacists to administer vaccines under protocol while others require a prescription to administer a vaccine. In many states, certain vaccines are allowed by protocol but other vaccines require a prescription. Additionally, pharmacists in 27 states may administer vaccines to patients of any age.24 Other states have age requirements for pharmacists’ vaccination authority, ranging from patients as young as 5 years of age in North Dakota, to patients at least 19 years of age in Wyoming. Research has found that parents are supportive of pharmacists vaccinating their children and that immunization rates for children increase with pharmacist involvement.37 Some states allow student pharmacists to administer vaccines if certain criteria are met. Common criteria include that the 12 EDUCATION student must be trained (e.g., through this certificate training program) and must operate under the direct supervision of a trained pharmacist. In 2017, Idaho because the first state to implement a pilot program allowing pharmacy technicians to administer immunizations. The results of this pilot may have important implications for future roles of pharmacy technicians. State laws and regulations are continually changing and pharmacists should regularly monitor their state rules and regulations. Collaborating to Improve Immunization Rates In areas where state practice acts continue to pose limitations regarding which vaccines pharmacists may administer, all pharmacies can serve as immunization information centers. This service involves educating patients and families about who needs specific vaccines, when they need them, and where these vaccines are available. Pharmacists practicing in states that limit their authority to administer vaccines are encouraged to work with the state pharmacy association, board of pharmacy, and colleges of pharmacy to change the state’s pharmacy practice act. Through such change, pharmacists can be in a position to better protect the public’s health. As barriers to pharmacists’ ability to administer vaccines are removed, pharmacists’ advocacy efforts in other arenas are gaining prominence. Pharmacists can explore opportunities to improve public health by advocating for vaccinations using a variety strategies including collaborating with other members of the health care team, becoming involved with state-level efforts, joining immunization coalitions, and partnering with health departments. (State and local health departments organize, administer, and maintain vaccine campaigns, registries, and educational activities. Immunization coalitions are organizations that foster collaboration among stakeholders to increase immunization rates.) The HPV vaccine provides one potential model for pharmacists’ collaboration with other members of the health care community to increase vaccination rates. Immunization with the HPV vaccine requires a 2- or 3-dose series; however, many adolescents do not complete the series. The need to schedule an appointment to obtain subsequent doses of the vaccine may be a barrier to immunization by medical providers. If the medical provider referred the patient to the pharmacist for the second and third doses, and communicated with the pharmacist, then the pharmacist could follow-up with the patient to support full immunization.38 Figure 1.5. States Authorizing Pharmacists to Administer Influenza Vaccine and Pharmacists Trained to Administer Vaccines NABP = National Association of Boards of Pharmacy. Source: Reference 24. Module 1. Pharmacists, Vaccines, and Public Health As pharmacists expand their immunization roles, they are becoming integrated in the “immunization neighborhood.” This term was coined by APhA and is gaining acceptance from a broad array of immunization stakeholders. The immunization neighborhood is defined as “collaboration, coordination, and communication among immunization stakeholders dedicated to meeting the immunization needs of the patient and protecting the community from vaccine-preventable diseases.” This conceptual neighborhood includes a variety of immunization stakeholders who are working to meet immunization needs of their communities. Supporting achievement of the immunization neighborhood, the HHS National Vaccine Advisory Committee released a new version of the 13 EDUCATION Adult Immunization Standards that identifies a role for every health care professional, organization, and health system (Table 1.7).39 Emergency Preparedness and Vaccines Immunizing pharmacists play a critical role in emergency preparedness efforts. During an emergency, pharmacists may be called on to administer vaccines as well as to help with the distribution of medications. For example, during a pandemic, pharmacists can support immunization efforts to protect the public. Pharmacists also could become involved in immunization efforts in the event of a bioterrorism attack with an agent such as anthrax or smallpox. Natural disasters such as hurricanes or floods also may call for mass vaccinations with tetanus vaccines.40 Additionally, public confusion surrounding the number of required doses of H1N1 vaccine and the target groups for vaccination compared with the seasonal influenza vaccine necessitated patient education for effective vaccination programs. Pharmacists played a critical role in promoting public health and wellness during this emergency. Pharmacists who are interested in taking a more active role in emergency preparedness efforts can join their local Medical Reserve Corps (https://mrc.hhs.gov/HomePage) or Disaster Medical Assistance Team (www.phe.gov/Preparedness/ responders/ndms/teams/Pages/dmat.aspx). In an emergency, these teams and the Strategic National Stockpile may be brought into the affected areas to provide medications and mass vaccinations. Sources of Immunization Information To maintain a high-quality practice in immunizations, a commitment must be made to stay up to date with ongoing developments in immunization practice. Practice recommendations and immunization schedules are updated frequently as new research and vaccines become available. In preparation to become immunizers, pharmacists need to locate resources to identify regularly updated information. Many high-quality resources are available, but it is important to be aware that a substantial amount of misinformation is also widely distributed. More information about myths and misperceptions regarding vaccines, and how to address them, will be discussed in Module 4. Selected reputable resources are provided in the following section. Module 1. Pharmacists, Vaccines, and Public Health Vaccine Recommendation Sources National evidence-based vaccination recommendations are written by the CDC Advisory Committee on Immunization Practices (ACIP) and the Committee on Infectious Diseases of the American Academy of Pediatrics (AAP). Other major policy-setting groups include the American College of Physicians (ACP), the American Congress of Obstetricians and Gynecologists (ACOG), and the American Academy of Family Practitioners (AAFP).41,42 The harmonized pediatric immunization schedule (indicating who should receive which vaccines when) is a collaborative effort of ACIP, AAP, ACOG, and AAFP. It is usually published in January of each year with updates published as situations warrant. The adult immunization schedule is also updated annually and published every January or February. ACIP meets multiple times per year to review newly available information and update recommendations as necessary. These recommendations and updates are published in Morbidity and Mortality Weekly Report (MMWR), which can be accessed online at www.cdc.gov/mmwr. Immunizing pharmacists should remain current on recommendations from ACIP, and can sign up at www.cdc.gov/vaccines/acip/ to receive an e-mail whenever the website is updated. In addition, APhA conducts educational programs after each ACIP meeting to provide updates on the latest ACIP discussions and decisions. Selected Online Resources APhA provides multiple electronic resources that are indispensable for immunizing pharmacists. All of the following resources are easily accessible at www.pharmacist.com/ immunization-center, APhA’s Immunization Center. Pharmacists also can subscribe to APhA’s free electronic newsletter, Immunizing Pharmacists News, by filling out the online form available at this site. This newsletter scans the latest immunization information and provides items of interest to immunizing pharmacists. For member access only, APhA has a robust Immunizing Pharmacists e-Community that offers a forum for immunizing pharmacists to network with other immunization providers across the country, facilitated by the APhA Academy of Pharmacy Practice and Management’s special interest group for immunizing pharmacists. Participants in this certificate training program have access to a compilation of links and valuable resources for pharmacybased immunization delivery at www.pharmacist.com/ immunization-resources. 14 EDUCATION Table 1.7. Summary of the 2013 National Vaccine Advisory Committee’s Standards for Adult Immunization Practices Audience Summary of Standards All providers Incorporate immunization needs assessment into every clinical encounter Strongly recommend needed vaccines and either administer vaccines or refer patient to a provider who can immunize Stay up to date on, and educate patients about, vaccine recommendations Implement systems to incorporate vaccine assessment into routine clinical care Understand how to access immunization information systems (also known as IIS and immunizations registries) Non-immunizing providers Routinely assess immunization status of patients, recommend needed vaccines, and refer patient to an immunizing provider Establish referral relationships with immunizing providers Follow-up to confirm patient receipt of recommended vaccines Immunizing providers Ensure professional competencies in immunizations Assess immunization status in every patient care and counseling encounter and strongly recommend needed vaccines Ensure that receipt of vaccination is documented in patient medical record and immunization registry Professional health care–related organizations/associations/health care systems Provide immunization education and training of members, including trainees Provide resources and assistance to implement protocols and other systems to incorporate vaccine needs assessment and vaccination or referral into routine practice Encourage members to be up to date on their own immunizations Assist members in staying up to date on immunization information and recommendations Partner with other immunization stakeholders to educate the public Seek out collaboration opportunities with other immunization stakeholders Collect and share best practices for immunization Advocate policies that support adult immunization standards Insurers/payers/entities that cover adult immunization services should assure their network is adequate to provide timely immunization access and augment with additional vaccine providers if necessary Public health departments Determine community needs, vaccination capacity, and barriers to adult immunization Provide access to all vaccinations recommended by the Advisory Committee on Immunization Practices for insured and uninsured adults and work toward becoming an in-network provider for immunization services for insured adults Partner with immunization stakeholders and support activities and policies to improve awareness of adult vaccine recommendations, increase vaccination rates, and reduce barriers Ensure professional competencies in immunizations Collect, analyze, and disseminate immunization data Provide outreach and education to providers and the public Work to decrease disparities in immunization coverage and access Increase immunization registry access and use by vaccine providers for adult patients Develop capacity to bill for immunizations Ensure preparedness for identifying and responding to outbreaks of vaccine-preventable diseases Promote adherence to applicable laws, regulations, and standards among adult immunization stakeholders Source: Reference 47. Module 1. Pharmacists, Vaccines, and Public Health 15 EDUCATION The CDC website, www.cdc.gov/vaccines, is extensive, providing up-to-date information regarding immunization practices. Various e-mail subscriptions are available for free from the CDC, providing a convenient way to stay current. For example, to receive the table of contents of CDC’s publication MMWR, pharmacists can subscribe to a mailing list at www.cdc.gov/mmwr/mmwrsubscribe.html. The Immunization Action Coalition (IAC) website, available at www.immunize.org, offers a wide array of well-respected resources for immunization providers and other audiences. IAC provides several free e-mail publications and an e-mail service to inform subscribers of news involving immunizations. Pharmacists can sign up for the IAC e-mail publications by visiting www.immunize.org/subscribe/. IAC also publishes the quarterly newsletters Needle Tips and Vaccinate Adults! available in print and online. Other selected websites that offer useful information are listed in Table 1.8. Print Material APhA’s Immunization Handbook is a valuable resource that provides numerous guidelines, tips, and resources for building and sustaining a successful immunization practice. Written in a concise and quick look-up format, this handbook is an essential resource for busy pharmacists. APhA also publishes The Pharmacist in Public Health: Education, Applications, and Opportunities, which explores activities for pharmacists in public health and provides information to help pharmacists overcome challenges and embrace opportunities as public health pharmacists. Both books are available for purchase from the APhA Bookstore at www.pharmacist.com/shop with discounted pricing for APhA members. The CDC and IAC have excellent print resources for immunization providers, including ACIP statements, posters, brochures, and patient education materials. The majority of the materials can be downloaded for free from the previously listed websites. Epidemiology and Prevention of Vaccine-Preventable Diseases (also known as “The Pink Book”) is published by the CDC and is the most important reference for all Table 1.8. Websites of Selected Organizations Useful to Immunizing Pharmacists Organization Website American Academy of Pediatrics www.aap.org American College of Physicians www.acponline.org American Pharmacists Association Immunization Center www.pharmacist.com/immunization-center American Society of Consultant Pharmacists www.ascp.com Centers for Disease Control and Prevention www.cdc.gov/vaccines Centers for Medicare and Medicaid Services www.cms.gov Immunization Action Coalition www.immunize.org Immunization Coalition Directory www.izcoalitions.org Morbidity and Mortality Weekly Report www.cdc.gov/mmwr National Center for Immunization and Respiratory Diseases www.cdc.gov/ncird National Foundation for Infectious Diseases www.nfid.org National Disaster Medical System www.phe.gov/preparedness/responders/ndms/Pages/default.aspx National Vaccine Errors Reporting Program verp.ismp.org State health departments www.cdc.gov/mmwr/international/relres.html State immunization managers www.immunizationmanagers.org Vaccine Adverse Event Reporting System vaers.hhs.gov Vaccine Injury Compensation Program www.hrsa.gov/vaccinecompensation Module 1. Pharmacists, Vaccines, and Public Health 16 EDUCATION pharmacists to have available in their practice (it is also available online). It provides comprehensive information on vaccine-preventable diseases. The AAP’s Red Book: Report of the Committee on Infectious Diseases is another worthy reference that focuses on pediatric illness. Facts and Comparisons annually updates its major reference book, ImmunoFacts: Vaccines and Immunologic Drugs. Another recognized authoritative reference is Vaccines edited by Plotkin, Orenstein, and Offit. 4. College of Physicians of Philadelphia. The History of Vaccines. Timelines. Available at: http://www.historyofvaccines.org/content/ timelines/all. Accessed May 19, 2017. 5. Centers for Disease Control and Prevention; Atkinson W, Wolfe C, Hamborsky J, eds. Epidemiology and Prevention of Vaccine-Preventable Diseases. 12th ed., 2nd printing. Washington, DC: Public Health Foundation; May 2012. 6. Roush SW, Murphy TV; Vaccine-Preventable Disease Table Working Group. Historical comparisons of morbidity and mortality for vaccinepreventable diseases in the United States. JAMA. 2007;298:2155– 63. 7. Centers for Disease Control and Prevention. Notifiable diseases and mortality tables. MMWR Morb Mortal Wkly Rep. 22017;66(05):ND82-ND-101. 8. Grabenstein JD. Milestones in immunologic history: antiquity to 1919. Hosp Pharm. 1994;29:477–8, 480–3. 9. Healthy People 2020. Immunization and Infectious Diseases. Available at: http://healthypeople.gov/2020/topicsobjectives2020/ overview.aspx?topicid=23. Accessed May 19, 2017. Video Resources Live CDC-sponsored video conferences are broadcast by satellite (and online) several times a year. Titles include Epidemiology and Prevention of Vaccine-Preventable Disease and Vaccines for International Travel. Pharmacists may check the CDC website for a listing of viewing sites and times. The CDC offers live, video, and teleconference programs with continuing pharmacy education (CPE) credit for pharmacists. APhA also offers annual updates and CPE credit for educational activities related to vaccines through its website; go to www.pharmacist. com/education and click on APhA’s Educational Library. Conclusion Vaccines have significantly decreased the morbidity and mortality associated with many diseases. Despite these successes, shortfalls in vaccination rates still exist and more needs to be done to avert needless vaccine-preventable diseases and deaths. Pharmacists in all settings have an opportunity to significantly affect patient care by getting involved with immunizations as educators, facilitators, and in many instances, immunizers. Participating in this certificate training program is an important first step toward becoming an immunizing pharmacist. Identifying resources that support immunizing pharmacists and using them to remain abreast of developments are also critical steps toward providing highquality patient care. References 1. Centers for Disease Control and Prevention. Ten great public health achievements—United States, 1900–1999. MMWR Morb Mortal Wkly Rep. 1999;48:241–3. 2. Centers for Disease Control and Prevention. Control of infectious diseases. MMWR Morb Mortal Wkly Rep. 1999;48:621–9. 3. Immunization Action Coalition. Historic Dates and Events Related to Vaccines and Immunization. Available at: http://www.immunize.org/ timeline. Accessed May 19, 2017. Module 1. Pharmacists, Vaccines, and Public Health 10. Centers for Disease Control and Prevention. Update: measles— United States, January–July 2008. MMWR Morb Mortal Wkly Rep. 2008;57:893–6. 11. Centers for Disease Control and Prevention. Immunization. Available at: https://www.cdc.gov/nchs/fastats/immunize.htm. Accessed March 21, 2017. 12. Centers for Disease Control and Prevention. Health, United States, 2015. Available at: https://www.cdc.gov/nchs/data/hus/hus15. pdf#067. Accessed March 21, 2017. 13. Centers for Disease Control and Prevention. Surveillance of vaccination coverage among adult populations--United States, 2013. MMWR Morb Mortal Wkly Rep. 2016;65(1):1-36. 14. Grabenstein JD. Pharmacists and immunization: increasing involvement over a century. Pharm Hist. 1999;41:137–52. 15. Hogue MD, Grabenstein JD, Foster SL, Rothholz MC. Pharmacist involvement with immunizations: a decade of professional involvement. J Am Pharm Assoc. 2006;46:168–82. 16. Shaffer M. Flu shot fever. Am Druggist. 1994;209:30–1, 35. 17. Debrovner D. Beyond chicken soup. Am Druggist. 1994;209:21–4. 18. Spring B. Washington state pharmacists train to offer immunizations. Pharm Today. 1995;1(Aug):10. 19. Ukens C. Immunization programs shot in arm for community RPhs. Drug Topics. 1994;138:39. 20. Reagan MR. Creating immunization programs in pharmacies. Pharm Times. 1995;61:16, 19, 22–3. 21. Stover KA. West Virginia to study pharmacists’ impact on immunizations. Pharm Today. 1996;2:10. 22. Study of pharmacists’ impact on immunizations. J Am Pharm Assoc. 1996;36:216. 23. Powell J. Local pharmacists volunteer time and expertise during Douglas County health crisis. Georgia Pharm J. 1993;15:16. 24. American Pharmacists Association. Data on file. Updated October 2013. 17 EDUCATION 25. American Pharmacists Association. Guidelines for pharmacy-based immunization advocacy. Available at: http://www.pharmacist.com/ guidelines-pharmacy-based-immunization-advocacy. Accessed September 17, 2013. 26. Grabenstein JD, Hayton BD. Pharmacoepidemiologic program for identifying patients in need of vaccination. Am J Hosp Pharm. 1990;47:1774–81. 27. Etzel JV, Brocavich JM. Pharmacist’s role in immunization. US Pharmacist. 1994;Nov(suppl 3):3–18. 28. Knapp KK, Paavola FG, Maine LL, et al. Availability of primary care providers and pharmacists in the United States. J Am Pharm Assoc. 1999;39:127–35. 29. Steyer TE, Ragucci KR, Pearson WS, Mainous AG. The role of pharmacists in the delivery of influenza vaccinations. Vaccine. 2004;22:1001–6. 30. Bounthavong M, Christopher ML, Mendes MA, et al. Measuring patient satisfaction in the pharmacy specialty immunization clinic: a pharmacist-run immunization clinic at the Veterans Affairs San Diego Healthcare System. Int J Pharm Pract. 2010;18:100–7. 31. Grabenstein JD, Guess HA, Hartzema AG. People vaccinated by pharmacists: descriptive epidemiology. J Am Pharm Assoc. 2001;41:46–52. 32. Blake EW, Blair MM, Couchenour RL. Perceptions of pharmacists as providers of immunizations for adult patients. Pharmacotherapy. 2003;23:248–54. 33. Keely JL; American College of Physicians–American Society of Internal Medicine. Pharmacist scope of practice. Ann Intern Med. 2002;136:79–85. 35. Centers for Medicare and Medicaid Services. Immunization standard for long-term care facilities. 42 CFR §483. Final rule. Fed Regist. 2005;70:58834–52. 36. National Committee for Quality Assurance. Summary Table of Measures, Product Lines, and Changes. Available at: http://www. ncqa.org/Portals/0/HEDISQM/HEDIS2013/List_of_HEDIS_2013_ Measures_7.2.12.pdf. Accessed May 19, 2017. 37. Deshpande M, Schauer J, Mott DA, et al. Parents’ perceptions of pharmacists as providers of influenza vaccine to children. J Am Pharm Assoc. 2013;53:488–95. 38. Centers for Disease Control and Prevention. Human papillomavirus– associated cancers—United States, 2004–2008. MMWR Morb Mortal Wkly Rep. 2012;61:258–61. 39. Centers for Disease Control and Prevention. Standards for Adult Immunization Practice. Available at: https://www.cdc.gov/vaccines/ hcp/adults/for-practice/standards. Accessed March 20, 2017. 40. Terriff CM, Newton S. Pharmacist role in emergency preparedness. J Am Pharm Assoc. 2008;48:702–10. 41. American Academy of Pediatrics; Pickering LK, Baker CJ, Kimberlin DW, Long SS, eds. Red Book: 2012 Report of the Committee on Infectious Diseases. 29th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2012. 42. Kroger AT, Duchin J, Vázquez M. General Best Practice Guidelines for Immunization. Best Practices Guidance of the Advisory Committee on Immunization Practices (ACIP). https://www.cdc.gov/vaccines/ hcp/acip-recs/general-recs/index.html. Accessed May 19, 2017. 34. American Pharmacists Association. CDC releases Dear Pharmacist letter for seasonal influenza vaccination efforts. Available at: http:// www.pharmacist.com/cdc-releases-dear-pharmacist-letter-seasonalinfluenza-vaccination-efforts?dfptag=imz. Accessed May 19, 2017. Module 1. Pharmacists, Vaccines, and Public Health 18