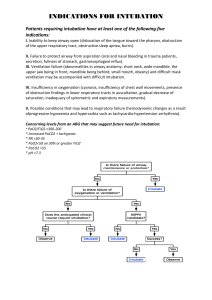
Preparation
The clinician should have all the necessary equipment, using the mnemonic STOP IC BARS =
Suction; is turned on and is close proximity to the patients head and the rigid suction catheter
has been checked by the thumb port. Tubes; of all sizes is checked with a half or full size smaller
and a syringe attached to the pilot line. Oxygen; a cylinder is available that is attached to a high
flow O2 reservoir bag (BVM). Pharmacology; all drugs needed for RSI, pain and sedation must be
drawn up and labelled. IV; intravenous access must be established with 18G or larger and preload the patient with 5-20ml/kg of fluid to migrate the offset that the RSI drugs does to the
blood pressure. Connect monitors and confirmation; such as ECG, blood pressure and pulse
oximeter. Confirmation devices such as capnography and EDD. Blades, should be checked for
light intensity. The clinician should also make sure that there is a Macintosh blade (size 3 and
size 4) and a straight blade. A bougie must also be easily accessible during all intubation
attempts. An alternate devices; this includes Airtraq and LMA fastrach. Rescue oxygenation;
such as LMA and I-Gel must be within reach for incase of failed intubation attempts. Surgical
cricothyrotomy for cases of failed ventilation and failed intubation scenario.
Secondly, it is essential that the clinician assembles adequate personnel in the roles that they
are going to participate in to assist during the process.
Preoxygenation
Begins with the initiation of 100% in order to de-nitrogenate the function residual capacity over
3-5 minutes with a tight-fitting facemask.
BVM with positive pressure ventilation must be avoided during preoxygenation unless patients
become apneic or there is ineffective spontaneous breathing because there is a risk of gastric
insufflation or regurgitation.
Pre-intubation optimization
Drugs such as fentanyl and atropine help to mitigate the negative physiological responses to
intubation. Atropine is given to infants or pediatric patients who have significant bradycardia if
succinylcholine is given.
Fentanyl are given to patients who have went through a recent trauma for pain or who may
have a sympathetic response to the ETT tube during intubation.
Paralysis and induction
As an induction agent such as a potent sedative-hypnotic (etomidate) or a dissociative amnestic
(ketamine) in order to induce unconsciousness. This is weight- dose based as it minimizes the
side effect profile and helps to prevent exacerbating the patients underlying condition.
A paralyzing agent such as succinylcholine or rocuronium can be given; however with
succinylcholine it has a rapid onset and the patient can resume spontaneous ventilation if there
is a failed airway situation.
Positioning
Placing the patient head and neck in the right position is important because this helps to achieve
the best view for the glottis opening. In addition this must be done when there are no C-spine
precautions.
The neck must be flexed at the lower cervical spine and extended at the upper cervical spine
(C1-C2); known as the sniffing position.
Placement with proof
A best look for intubation is done; it is important that an assistant gives the clinician the ETT
correctly so that the cords are always seen to prevent time delay during the procedure.
To proof that tube placement is secured is done by objective (End tidal CO2) and subjectively by
auscultation; to ensure it does not sit within the right mid-stem bronchi.
Post-intubation Management
Obtain a post-induction vital signs early with 2.5 minute intervals to avoid critical cardiovascular
complications such as cerebral stroke, angina, and myocardial infarction.
It is essential that the practioner initiates positive pressure ventilation to assess lung compliance
but also not to hyperventilate as this may induce barotrauma, hypotension and lead to breathe
stacking especially in conditions such as bronchospasm and COPD.
 0
0