EFFECTIVENESS OF EDUCATIONAL INTERVENTION ON
KNOWLEDGE ON FEBRILE SEIZURE AMONG THE MOTHERS OF
CHILDREN ATTENDING PRIMARY HEALTH CENTRE, PODANUR.
Mrs. A.S.ARUN SUBINI
Reg. No: 301818401
A Dissertation Submitted to
The Tamil Nadu Dr. M.G.R. Medical University,
Chennai - 32.
In Partial Fulfillment of the Requirement for the
Award of the Degree of
MASTER OF SCIENCE IN NURSING
BRANCH-II
PAEDIATRIC NURSING
2020
EFFECTIVENESS OF EDUCATIONAL INTERVENTION ON
KNOWLEDGE ON FEBRILE SEIZURE AMONG THE MOTHERS OF
CHILDREN ATTENDING PRIMARY HEALTH CENTRE, PODANUR.
Mrs. A.S.ARUN SUBINI
Reg. No: 301818401
A Dissertation Submitted to
The Tamil Nadu Dr. M.G.R. Medical University,
Chennai – 32.
In Partial Fulfillment of the Requirement for the
Award of the Degree of
MASTER OF SCIENCE IN NURSING
BRANCH-II
PAEDIATRIC NURSING
2020
EFFECTIVENESS OF EDUCATIONAL INTERVENTION ON
KNOWLEDGE ON FEBRILE SEIZURE AMONG THE MOTHERS OF
CHILDREN ATTENDING PRIMARY HEALTH CENTRE, PODANUR.
BY
Mrs. A.S.ARUN SUBINI
Reg. No: 301818401
A DISSERTATION SUBMITTED TO THE TAMILNADU DR.M.G.R. MEDICAL
UNIVERSITY, CHENNAI IN PARTIAL FULFILLMENT OF REQUIREMENT FOR THE
DEGREE OF
MASTER OF SCIENCE IN NURSING
BRANCH-II
PAEDIATRIC NURSING
2020
INTERNAL EXAMINER
EXTERNAL EXAMINER
EFFECTIVENESS OF EDUCATIONAL INTERVENTION ON
KNOWLEDGE ON FEBRILE SEIZURE AMONG THE MOTHERS OF
CHILDREN ATTENDING PRIMARY HEALTH CENTRE, PODANUR.
APPROVED BY THE DISSERTATION COMMITTEE
1. RESEARCH GUIDE : …………………………………….
Prof. Dr.D.CHARMINI JEBAPRIYA, M.Sc(N)., M.Phil, Ph.D.,
Principal,
Texcity College of Nursing,
Coimbatore - 23.
2. CLINICAL GUIDE : …………………………………….
Prof.Mrs.THEMOZHI.P, M.Sc (N), M.Sc (Psy), MA Sociology,
Professor cum Vice Principal,
Texcity College of Nursing,
Coimbatore – 23.
3. MEDICAL GUIDE : ……………………………………
Dr. MALLIKAI SELVARAJ, MBBS..DCH. Pgd. DN
Developmental paediatrician,
Royal Care Super Speciality Hospital,
Coimbatore – 18.
CERTIFICATE
Certified that this is the bonafide work of Mrs.A.S.ARUN SUBINI, Texcity College of
Nursing, Coimbatore, submitted as a partial fulfillment of requirement for the Degree of Master
of Science in Nursing to The Tamilnadu Dr.M.G.R.Medical University, Chennai under
Registration No: 301818401
College Seal
Prof. Dr. D. CHARMINI JEBAPRIYA, M.Sc (N)., M.Phil, Ph.D,
Principal,
Texcity College of Nursing,
Coimbatore – 23,
TEXCITY COLLEGE OF NURSING
Podanur Main Road
Coimbatore-23.
2020
DECLARATION
DECLARATION
I hereby declare that the dissertation entitled “A study to evaluate the effectiveness of
educational intervention on knowledge on febrile seizure among the mothers of children
attending Primary Health Centre, Podanur”.
Submitted to the Tamilnadu Dr.M.G.R Medical University, Chennai, in partial fulfillment
of the requirements for the award of the degree of Master of Science in Nursing is a record of
original research done by myself.
This is the study under the supervision and guidance of Prof. Mrs. THENMOZHI.P
M.Sc (N) Paed. Nsg M.Sc (Psy), MA(Socio), Vice Principal, Texcity College of Nursing,
Coimbatore and dissertation has not found the basis for the award of any degree / diploma /
associated degree / fellowship or similar title to any candidate of any university.
SIGNATURE OF THE PRINCIPAL
SIGNATURE OF THE GUIDE
CANDIDATE
Mrs. A.S.ARUN SUBINI
DEDICATION
THIS DISSERTATION IS
DEDICATED TO
ALMIGHTY GOD
OUR EVER LOVING TEACHERS,
PARENTS, HUSBAND AND FRIENDS
FOR THEIR
“VALUABLE SUPPORT AND
ENCOURAGEMENT”
THROUGHOUT THE STUDY.
ACKNOWLEDGEMENT
ACKNOWLEDGEMENT
The perfection of work and efforts molded by various persons to complete it successfully. It
will not be a fruitful one unless I extend my heartfelt thanks and gratitude to all who guided me
to the treasure of knowledge.
First of all, I would like to convey my sincere gratitude to ALMIGHTY GOD for His
grace, strength and wisdom throughout the completion of the study.
I
would
like
to
extend
my
sincere
thanks
to
Haji.Janab.A.M.M.Khaleel,
Chairman, Texcity Medical and Educational Trust, Coimbatore, for his support and providing
me an opportunity to utilize all the facilities in this esteemed institution for successful
completion of the study.
I express my sincere thanks to Major H.M. Mubarak, Manager, Texcity College of
Nursing, for supporting me to complete this study, as greater achievements comes from
experience and success.
With profound delight, I have immense pleasure to respect and heartfelt gratitude to my
beloved Prof. Dr. Charmini JebaPriya, M.sc (N)., M.Phil., Ph.D The Principal, Texcity
college of nursing, Coimbatore, for her appreciation, support and excellent, guidance
encouragement which enabled me to reach my objective.
With profound pleasure I express my deep sense and sincere heart full gratitude to my
research guide Prof. Mrs. P.Thenmozhi, M.Sc (N),[Paed], MSc (Psy), MA (Socio), Vice
Principal, Department of Child Health Nursing, Texcity college of Nursing, Coimbatore for
all the support rendered to during the endeavor. Her hard work, sincerity, inspiration, suggestion,
illuminating comments and support helped me to mould this study in a successful way. This
study could not have been presented in the manner it has been made and would have never taken
up the shape.
I extend my sincere and deep sense of thanks to Asst Prof. A.Vedha Darly, M.Sc (N),
[MHN], class Co-ordinator Texcity College of Nursing, Coimbatore for her extended
suggestions, constant support, timely help and guidance till the completion of this study.
I express my sincere and deep sense of gratitude to Mrs.Valarmathy, M.Sc(N), [CHN],
who encouraged and guided me to carry out the thesis in a successful manner in a given period.
I would like to extend my thanks to Mrs.Litterishia Balin, M.S.c (N), [MSN]., and
Mrs.Saranya M.Sc (N), [MHN]; Mrs.Akila, M.Sc (N) [OBG], Texcity College of Nursing,
Coimbatore, for their expert guidance, support and valuable suggestion given to me throughout
the study.
I express my sincere thanks to Ms.Delpa Alex, M.Sc (Statistics), Coimbatore for her
necessary guidance in statistical analysis.
I would like to thank all the experts who have done the content validity and contributed
their valuable suggestion in modification of tool even in their busy schedule.
I extend my cordial thanks to my medical guide, Dr. MALLIKAI
SELVARAJ,
MBBS., DCH. Pgd. DN, Developmental pediatrician. Royal Care Super Speciality Hospital,
Coimbatore for permitting me to do the data collection.
I would like to extend my thanks to Mrs.D.Muthumalni Alice, M.A(English)., B.Ed
Professor. Texcity College of Nursing, Coimbatore, for editing and for helping me to achieve
english language appropriateness in my dissertation.
I honestly express my sincere thanks and gratefulness to the mothers of under five children
who participated in my study for their co operation.
I express my heartful thanks to Mrs.Famy Carmel.F, M.Li.Sc, Librarian and
Ms.SUMAYA.A M.Sc (CS) computer staff for her kind cooperation in providing the necessary
materials.
Final and not the least my special thanks goes to my parents Mr.S.Arul peter, N.Suseela
and my husband Mr.M.John Manoj, for sparing their time and providing financial support for
my study.
I would like to extend my thanks to Star Color Park, Gandhipuram, for his full
cooperation and help in bringing in a printed form.
Above all, I express my deep sense of gratitude and indebtedness to our ever loving parents
and family members and friends for rendering emotional support during the hard working period
for preparation of this project.
ABSTRACT
ABSTRACT
The main aim of the present study was “To evaluate the effectiveness of educational intervention
on febrile seizure among the mothers of under five children at Primary Health Center, Podanur”.
OBJECTIVES
To assess the existing level of knowledge and practice on febrile seizure among the
mothers of under five children.
To evaluate the effectiveness of educational intervention on febrile seizure among
mothers of under five children.
To associate the pretest knowledge and practice score with selected demographic
variables.
To identify the Correlation between post test knowledge and practice on febrile seizure
among the mothers of under five children.
HYPOTHESIS
H1- There will be a significant difference between pretest and post test knowledge score on
febrile seizures.
H2- The mean post test practice score will be significantly higher than mean pretest practice
score.
H3- There will be a significant association between pretest scores of knowledge and selected
demographic variables.
H4- There will be a significant association between pretest practice score and selected
demographic variables.
H5- There will be significant relation between the post test knowledge and practice score.
METHODOLOGY
Pre-experimental one group pretest and post test design was used, 40 samples were
selected using non- probability convenient sampling method. A self administered
questionnaire and observational checklist was used to evaluate the knowledge and practice of
mothers. Descriptive and inferential statistics were used to analyze the data.
RESULTS
The study findings revealed that the educational intervention was effective on knowledge and
practice of mothers in prevention and care of children with febrile seizures.
The findings shows that among 40 mothers of under five children, 36(90%) had moderate
knowledge, 4(10%) had adequate knowledge in the pretest. The level of knowledge was
improved after intervention and in the post test 1(2.5%) had moderate knowledge and
39(97.5%) had adequate knowledge.
The findings shows that among the 40 mothers of under five children, 2 (5%) had
inadequate practice, 28 (70%) had moderate practice, 10 (25%) had adequate practice in
pre test. The level of practice improved after the intervention and in the post test 3 (7.5%)
had moderate practice and 37 (92.5%) had adequate practice.
The findings revealed that, the pretest knowledge score mean was 10.6 and post test mean
was 16.3, So mean difference 5.75 was a true difference. The standard deviation of
pretest was 2.340 and post test was 1.388. The calculated paired ‘t’ value was 24.01 was
highly significant than the table value (2.05) at 0.05 level. Hence the stated hypothesis
was accepted.
The findings revealed that, the pretest practice score mean was 9.10 and post test mean
was 12.77, So mean difference 3.67 was a true difference. The standard deviation of
pretest was 2.08 and posttest was 1.44. The calculated paired ‘t’ value 18.933 was highly
significant than the table value (2.05) at 0.05 level. Hence the stated hypothesis was
accepted.
The findings done by chi square test to find out the association between the pretest
knowledge score with the selected demographic variables, revealed that the pretest
knowledge score is associated with the reason of visit to primary health centre and
χ2value was 8.393 which is significant at level of p<0.05.
The findings revealed by, chi square analyzes to find out the association between the
pretest practice score with the selected demographic variables. The findings revealed that
there was no association between the pretest practice score with the selected demographic
variables.
The findings revealed that there is a positive correlation between the post test knowledge
and post test practice score.
CONTENTs
TABLE OF CONTENTS
CHAPTER
I
II
CONTENT
INTRODUCTION
PAGE NO
1
1.1
Background of the study
4
1.2
Significance and Need for the study
11
1.3
Statement of the problem
16
1.4
Objectives of the study
16
1.5
Hypothesis
16
1.6
Operational definition
17
1.7
Assumptions
17
1.8
Delimitations
18
1.9
Projected outcome
18
1.10
Conceptual frame work
18
REVIEW OF LITERATURE
2.1
Studies and literature related to febrile seizure in
21
22
children.
2.2
Studies and literature related to educational
26
intervention on febrile seizure.
III
METHODOLOGY
3.1
Research approach
35
3.2
Research design
36
3.3
Research variables
36
3.4
Setting of the study
36
3.5
Population
37
3.6
Samples
37
3.7
Sample size
37
IV
V
VI
VII
3.8
Criteria for selection of samples
37
3.9
Sampling technique
38
3.10
Description of the tool
38
3.11
Scoring procedure
38
3.12
Validity and reliability
39
3.13
Pilot study
40
3.14
Data collection procedure
40
3.15
Plan for data analysis
41
3.16
Ethical considerations
41
DATA ANALYSIS AND INTERPRETATIONS
43
FINDINGS AND DISCUSSION
66
SUMMARY AND CONCLUSION
6.1
Summary
68
6.2
Objectives
68
6.3
Major findings
69
6.4
Conclusion
71
6.5
Implication
71
REFERENCES
APPENDICES
73
76
LIST OF TABLES
TABLE
NO
TITLE
PAGE
4.1
Frequency and percentage distribution of samples with
demographic variables
45
4.2
Distribution of the samples according to their level of knowledge
in pretest and post test
55
4.3
Distribution of the samples according to their level of practice in
57
pretest and post test
4.4
Mean, Mean difference, Standard deviation and ‘t’ value of
pretest and post test level of knowledge among samples.
59
4.5
Mean, Mean difference, Standard deviation and ‘t’ value of
pretest and post test level of practice among samples.
60
4.6
Frequency, percentage and chi square distribution of pretest level
of knowledge score among mothers of under five children with
the selected demographic variables.
61
4.7
Frequency, percentage and chi square distribution of pretest level
of practice score among mothers of under five children with the
selected demographic variables.
63
4.8
Correlation between post test knowledge and post test practice of
mothers regarding febrile seizure.
65
NO
LIST OF FIQURES
FIQURE
TITLE
PAGE
NO
1.1
Prevalence and cumulative prevalence rates for febrile seizures
2
at different ages.
1.2
Prevalence of febrile seizures in children.
3
1.3
Depicting the causes of febrile seizure.
4
1.4
Recurrence rates of febrile seizures versus sex and the duration
9
after the first seizure.
1.5
Incidence rate of febrile seizures for different ages.
14
1.6
Frequency of consequative episodes of febrile seizure.
14
1.8
Conceptual frame work based on pender’s health promotion
20
model (1996)
3.1
Schematic representation of research methodology
4.1
The percentage distribution of sample in terms of age of the
42
48
mothers.
4.2
The percentage distribution of sample in terms of their
49
educational status.
4.3
The percentage distribution of samples in terms of their
50
occupation.
4.4
The percentage distribution of sample in terms of family history
51
of febrile seizure.
4.5
The percentage distribution of the sample in terms of previous
52
history of febrile seizure.
4.6
The percentage distribution of the sample in terms of reason of
53
visit to primary health center.
4.7
The percentage distribution of the sample in terms of having
thermometer at home.
54
NO
4.8
The percentage distribution of sample in terms of their pretest
56
and post test level of knowledge score.
4.9
The percentage distribution of sample in terms of their pretest
and post test level of practice score.
58
LIST OF APPENDICS
APPENDIX
I
TITLE
Plagirism certificate.
Letter seeking and granting permission to conduct the study.
II
III
IV
Letter requesting expert’s opinion for content validity.
List of experts given opinion for content validity.
Evaluation criteria check list for content validity
V
Tool-I demographic data
Evaluation criteria check list for content validity
VI
Tool-II self administered questionnaire and observational
checklist.
Evaluation criteria check list for content validity.[ Educational
VII
VIII
IX
X
XI
XII
Intervention]
Letter seeking consent for participation in this study.
Certificate for English Editing.
Research Tools.
Health teaching plan and module
AV Aids.
CHAPTER - I
INTRODUCTION
CHAPTER – I
INTRODUCTION
It‟s health that is real wealth and not pieces of gold and silver
-Mahatma Gandhi
A febrile seizure is a convulsion in a child caused by a spike in body temperature, often
from an infection. They occur in young children with normal development without a history of
neurologic symptoms. Children aged 3 months to 5 or 6 years may have seizures when they have
a high fever.
Febrile seizures are convulsions that can happen when a young child has a fever above
100.4°F (38°C). (Febrile means "feverish.") Febrile seizures (seizures caused by fever) occur in
3 or 4 out of every 100 children between six months and five years of age, but most often around
twelve to eighteen months old.
Children younger than one year at the time of their first simple febrile seizure have
approximate 50 percent chance of having another episode, while children over one year of age
when they have their first seizure have about a 30 percent chance of having a second one.
Nevertheless, only a very small number of children who have febrile seizures will go on to
develop epilepsy.
Alexander KC (2018) stated that febrile seizures are generally defined as seizures occurring
in children typically 6 months to 5 years of age in association with a fever greater than 38°C
(100.4°F), who do not have evidence of an intracranial cause (e.g. infection, head trauma, and
epilepsy).
Medscape (2018) updated pediatric essentials; Pediatric febrile seizures, which represent the
most common childhood seizure disorder, exist only in association with an elevated temperature.
Evidence suggests, however, that they have little connection with cognitive function, so the
prognosis for normal neurologic function is excellent in children with febrile seizures.
1
Diana K. Wells (2018) written that, febrile seizures usually occur in young children who are
between the ages of 3 months to 3 years. They‘re convulsions a child can have during a very
high fever that‘s usually over 102.2 to 104°F (39 to 40°C) or higher. This fever will happen
rapidly. The rapid change in temperature is more of a factor than how high the fever gets for
triggering a seizure. They usually happen when your child has an illness. Febrile seizures are
most common between the ages of 12 and 18 months of age. There are two types of febrile
seizures: simple and complex. Complex febrile seizures last longer. Simple febrile seizures are
more common.
John J Millichap (2019) revealed that febrile seizures are convulsions that occur in a child
who is between six months and five years of age and has a temperature greater than 100.4ºF
(38ºC). The majority of febrile seizures occur in children between 12 and 18 months of age.
Febrile seizures occur in 2 to 4 percent of children younger than five years old. They can be
frightening to watch, but do not cause brain damage or affect intelligence. Having a febrile
seizure does not mean that a child has epilepsy; epilepsy is defined as having two or more
seizures without fever present.
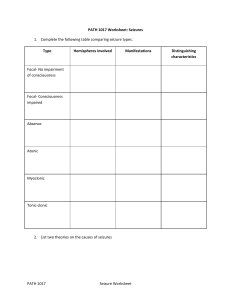
Fig:1.1
Prevalence and cumulative prevalence rates (reported as percentages) for
febrile seizures at different ages. The prevalence peaked (at 27.5%) among
those aged 2 years (age range 18-30 months).
2
National institute of health (2020) modified, febrile seizures are seizures or convulsions
that occur in young children and are triggered by fever. Young children between the ages of
about 6 months and 5 years old are the most likely to experience febrile seizures; this risk peaks
during the second year of life. The fever may accompany common childhood illnesses such as a
cold, the flu, or an ear infection. In some cases, a child may not have a fever at the time of the
seizure but will develop one a few hours later.
The vast majority of febrile seizures are convulsions. Most often during a febrile seizure, a
child will lose consciousness and both arms and legs will shake uncontrollably. Less common
symptoms include eye rolling, rigid (stiff) limbs, or twitching on only one side or a portion of the
body, such as an arm or a leg. Sometimes during a febrile seizure, a child may lose
consciousness but will not noticeably shake or move.
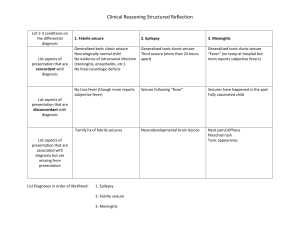
Fig:1.2 Prevalence of febrile seizures in children younger than 5 years in Korea
during 2009-2013.
3
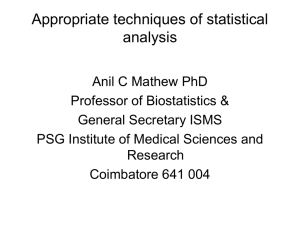
causes of febrile seizure
45
40%
40
35
28%
PERCENTAGE
30
RESP.TRACT.INF
24%
25
CNS Inf
20
UTI
15
Others
10
8%
5
0
RESP.TRACT.INF
CNS Inf
UTI
Others
Fig 1.3: Depicting the causes of febrile seizure
Most febrile seizures last only a few minutes and are accompanied by a fever above 101°F
(38.3°C). Although they can be frightening for parents, brief febrile seizures (less than 15
minutes) do not cause any long-term health problems. Having a febrile seizure does not mean a
child has epilepsy, since that disorder is characterized by reoccurring seizures that are not
triggered by fever. Even prolonged seizures (lasting more 15 minutes) generally have a good
outcome but carry an increased risk of developing epilepsy.
1.1 BACK GROUND OF THE STUDY
Children comprise one third of our population and all of our future and their health is our
foundation. The childhood period is also a vital period because many of the health problems will
arise from this period and most of the studies reveal that many children are suffering from one or
the other disease. Our responsibility is to maintain certain specific biological and psychological
4
needs to ensure the survival and healthy development of the child, future adult and also to
maintain optimum health of the children to enjoy their childhood. But unfortunately children are
at risk of diseases, the reason may be many. One of such disease is febrile seizure which
threatens life of the child.
Hackett R (2011) conducted a study one thousand four hundred and three children
participated in a home-based survey of psychiatric disorders in 8- to 12-year-old children in
Calicut District, Kerala, India. One thousand one hundred and ninety-two consecutive children
underwent neurological and psychometric assessments. The projected number of children with a
history of febrile seizures was 120 giving a lifetime incidence of 10.1%. Recurrent febrille
seizures predominated and these were strongly associated with a history of perinatal adversity.
Febrile seizures were independently association with indices of infective illness and mothers'
education. Epilepsy developed in 2.7% of children with febrile seizures, but no evidence was
found that febrile seizures had adverse intellectual or behavioural sequelae.
Srinivas.M (2011) found out that febrile seizures are defined as ―an event in neurologically
healthy infants and children between 6 months and 5 years of age, associated with fever >38ºC
rectal temperature but without evidence of intracranial infection as a defined cause and with no
history of prior afebrile seizures. Febrile seizures are to be distinguished from epilepsy which is
characterized by recurrent non febrile seizures. All seizures with fever are not febrile seizures.
Generally, febrile seizures occur during early phase of rising temperature and are uncommon
after 24 hours of onset of fever.
National Survey (2011) found out the Prevalence of febrile seizure in the countries are,
India it is 360/100,000,in Japan it is 89/1000 in children younger than 13 years, in Peru it is
2016/100,000 in children younger than 15 years and 10.1% is estimated to be life time
prevalence of febrile convulsion in India. Iranian journal of public health says that in a study the
life time prevalence of febrile convulsion was 32/1000 population, approximately 60% of case
reported febrile convulsion as the presumptive cause.
Manikam K (2011) conducted a cross sectional study in Andhra Pradesh showed that the
prevalence
rate
of
epilepsy as
6.2/1000
population,
where
as
in
Kerala
it
is
4.9/1000population.School age children are most affected with a slight male preponderance. In
5
America 300,000 people have a first convulsion each year and 120,000 of them are under the age
of eighteen.
Child Welfare Report (2011) elated that discrimination against persons suffering from
febrile seizure is common. This is often due to sudden falls and convulsive episodes at
unexpected times in public places 6resulting in rejection. Sometimes, the social discrimination
against these persons with epilepsy may be more devastating than the disease itself. Children
with epilepsy may be rejected from their classes because of frequent seizures which makes their
teachers and fellow students uncomfortable with their presence in class. Also, some children are
not allowed in schools once the school authority become aware that the child has epilepsy.
World Health Organization (2012) stated that febrile seizures (FS) are common, with a life
time prevalence of 2-6%. The definition of FS is controversial. The International League against
Epilepsy (ILAE) defines FS as ―an epileptic seizure occurring in childhood associated with fever,
but without evidence of intracranial infection or defined cause. Seizures with fever in children
who have experienced a previous non-febrile seizure are excluded (ILAE, 1993). British
Pediatric Association suggested "an epileptic seizure occurring in a child aged from six months
to five years, precipitated by fever arising from infection outside the nervous system in a child
who is otherwise neurologically normal‖ (Joint Working Group of the Research Unit of the
Royal College of Physicians and British Pediatric Association, 1991). Although it is important to
distinguish "seizures with fever" and "febrile seizures" in terms of management and prognosis,
this is often not possible in many primary health facilities in resource poor countries (Joint
Working Group of the Research Unit of the Royal College of Physicians and British Pediatric
Association, 1991). Seizures with fever include any seizure in a child of any age with fever of
any cause.
World Health Organization (2012) revealed that febrile Seizure is a common neurological
problem in children. Many seizures disorders have their origin in childhood. Nearly two-third of
febrile seizure disorder can be treated easily by them without the need for the specialist. In
ancient times convulsions are considered as curse of evils. Today also people with seizure
disorders are facing superstitions to this disease, this attitude can be changed once the scientific
cause of this condition is defined and the public is aware through education.
6
Fernandocendes (2012) pointed that febrile seizure promotes temporal lobe epilepsy
through the retrospective study: The sequence of febrile seizures followed by intractable
temporal lobe epilepsy is rarely seen from a population perspective. There is a significant
relationship between a history of prolonged febrile seizures in early childhood and mesial
temporal sclerosis. This association results from complex interactions among several genetic and
environmental factors. Early febrile seizure damages the hippocampus, and therefore the child
has a prolonged febrile seizure because the hippocampus was previously damaged. A
retrospective study of a series of 167 consecutive patients with lesional epilepsy supports the
concept of prolonged febrile seizure leading to mesial temporal sclerosis in a predisposed
hippocampus. In the study, febrile seizures were recurrent in five patients: three had simple and
two had complex febrile seizures. There is a strong correlation between mesial temporal sclerosis
and the severity of the epilepsy. Although there is a high incidence of complex febrile seizures
among patients with mesial temporal sclerosis, it is still not clear whether complex febrile
seizures are an epiphenomenon or a causative factor.
Peter Camfield (2012) conducted a study on Antecedents and Risk Factors for Febrile
Seizures; One child in 28 will have a febrile seizure. It would be an enormous clinical boon to be
able to predict accurately which child would develop febrile seizures so that parents could be
counseled and potentially preventive treatment could be offered. There are a significant number
of independent risk factors, such as day-care attendance, parental education, prenatal maternal
smoking, maternal alcohol intake, late neonatal discharge, slow development, degree of fever,
gastroenteritis, and family history of febrile seizures. In a study described in the chapter, an
interview with 13,135 parents who gave birth to children in the same week revealed that 303
children were known to have had at least one febrile seizure. The effect of low birth weight
seemed to be the result of a brain injury from complications of prematurity or premature birth in
children with existing brain abnormalities. The strongest association with febrile seizures is a
history of febrile seizures in the mother. Risk factors provide an insight into the pathophysiology
of febrile seizures, which will eventually yield all the secrets of this common and frightening
disorder.
Carl E.Stafstrom (2012) said that nearly every article or text written about febrile seizures
contains a statement about febrile seizures being the most common type of seizure in childhood,
7
occurring in 2–5% of children. The prognosis of febrile seizures in the early literature was fairly
pessimistic because of the inclusion of symptomatic causes of seizure other than fever and
patient selection bias. The consensus that febrile seizures do not constitute a form of epilepsy is
an important conceptual advance with relevance to the consideration of febrile seizure incidence
and prevalence. A disproportionate number of patients with temporal lobe epilepsy have febrile
seizures as young children. According to the International League, febrile seizures are an acute,
symptomatic type—that is, a ―special,‖ situation-related—seizure. Febrile seizures are not
associated with a structural or developmental anomaly of brain, though the existence of such
pathology may enhance the susceptibility to febrile seizures. The majority of febrile seizures
occurs between 6 months and 3 years of age, with the peak incidence at about 18 months. The
data obtained from epidemiological studies can help in the understanding of the genetics and
prognosis of febrile seizures.
Wongs (2013) pointed out another treatment option for seizure is surgical removal of the
brain tissue where the seizures originate (i.e., temporal lobectomy) but this technique is not often
used in children. Another possible preventive measure for epilepsy in children is avoidance of
triggers for seizures. Many children with epilepsy have triggers for seizures such as foods,
scents, or other environmental factors. If these triggers can be identified, seizures may be more
easily controlled. When used in some combination, all of these treatment methods have shown
effectiveness, however, there are few treatments that keep individuals entirely seizure free.
Ali Delpisheh (2014) said febrile seizures are the most common neurological disorder
observed in the pediatric age group. The present study provides information about
epidemiological and clinical characteristics as well as risk factors associated with FS among
Iranian children. On the computerized literature valid databases, the FS prevalence and 95%
confidence intervals were calculated using a random effects model. A meta regression analysis
was introduced to explore heterogeneity between studies. The important viral or bacterial
infection causes of FSs were; recent upper respiratory infection 42.3% (95% CI: 37.2%–47.4%),
gastroenteritis21.5% (95% CI: 13.6%–29.4%), and otitis media infections15.2% (95% CI: 9.8%20.7%) respectively. The pooled prevalence rate of FS among other childhood convulsions was
47.9% (95% CI: 38.8–59.9%). The meta–regression analysis showed that the sample size does
not significantly affect heterogeneity for the factor ‗prevalence FS‘.
8
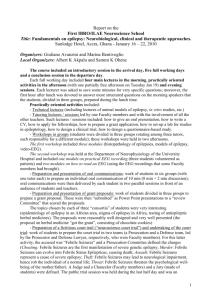
Fig:1.4
Recurrence rates of febrile seizures versus sex and the duration after the first
seizure. The recurrence rate was more than halved in patients with no
recurrence for 6 months after the first seizure.
Hocken Berry and Wilson (2015) stated that Febrile seizure management techniques
include the use of deep brain stimulators and vagus nerve stimulators. Deep brain stimulators are
implanted within the brain and send impulses to the cerebellum to increase seizure control by
stimulating deep brain structures, while vagus nerve stimulators are implanted near the clavicle
and send an electrical impulse to stimulate the vagus nerve in the neck.
Subramaniyam (2016) revealed that there is a dramatic global disparity in the care of febrile
seizure between high and low income countries and in rural and urban setting. The burden of
epilepsy in developing countries has become obvious as nearly 75% of people with epilepsy
were residing in these countries, where the diagnostic and therapeutic facilities are poor. A large
proportion of patients with epilepsy do not get treatment because medical facilities are not
available or approachable to them. In many of the cases it was found that the people are unaware
regarding the care of febrile seizure.
9
Dr. Bhattia (2017) conducted two community based studies in India (both rural and urban)
showed that the prevalence rate of febrile seizure stands around 5/1000 population (at this rate
present estimate of total epileptics in this country is about 5 million) and incidence rate varies
from 38 to 49.3 per 100,000 population per year. Treatment gap, which is a measure of per cent
of patient populations not receiving the treatment, was estimated to be up to 73.7% to 78% in
India. In 2/3 of cases etiology was unknown. Hot water epilepsy is unique in South India and
single solitary ring enhancing lesion in brain imaging is a common feature in Indian
subcontinent.
Dutta (2018) stated that febrile Seizures are caused by malfunctions of the brain‘s electrical
system that results from cortical neuronal discharge. The manifestations of seizures are
determined by the site of origin and may include altered consciousness, involuntary 2
movements, changes in perception, behaviours, sensation and posture. A diagnosis of epilepsy is
made when a person has three or more seizures. A seizure is behaviorally characterized by an
abrupt unconscious change in behaviour, movement, autonomic function, or sensation.
Henry (2018) stated that febrile seizures are the most common pediatric neurologic disorder.
Four per cent to ten per cent of children suffer at least one febrile seizure in the first 3 years of
life. The incidence is highest in children less than 6 years of age, with a decreasing frequency in
older children.
Febrile Seizures associated with fever occur in one in every 30-50 children, and those
unassociated with fever occur in about 1/200 children. About 5% of children experience one or
more seizures before they reach adulthood. Febrile Seizures activity often involves the diagnosis
of potential for injury, both physical& psychosocial. A potential for injury can be minimized
with first aid measures. Thus school teachers should possess skills in observational assessment
and first aid.
World Health Organization report suggested that even though the febrile seizure are
managed with the help of technology in present era people who are staying at rural and remote
areas of developing countries are not accessible or approachable to them. People in the
developing countries like India, Pakistan and Bangladesh believe that febrile seizure is one of the
diseases caused due to mistakes done in the past life. It is also concluded from various studies
10
that, false belief have major implication regarding epilepsy in illiterate as well as in the minds of
the people from these countries.
The disease enrobed in superstition, discrimination, and stigma. There is a clear cut lack of
information programmes in the developing world about febrile seizure and its management. The
febrile seizure has an impact on many aspects of a child‘s development and functioning. As a
result many of these children are at risk for unsuccessful school experiences, difficulties in social
engagement with peers, inadequate social skills and poor self-esteem.
Many of the parents were not familiar with the initial procedures in attending a child during
febrile seizure. The initial procedures adopted by some parents were inappropriate, like to
pulling the tongue or to putting objects in the child's mouth. Some of these wrong procedures,
which are potentially harmful, are mainly related to mythical concepts. As the parents are always
in touch with febrile seizure children, public enlightenment program on health issues especially
recognition and management of febrile seizure must be created in order to ensure that people
have sufficient knowledge about this disease. This will helps to improve the quality of life of
children with febrile seizure.
1.2 SIGNIFICANCE AND NEED FOR THE STUDY
Becker (2011) revealed that febrile seizure affects all age groups, but for children a variety
of issues exists that can affect one‘s childhood. Some epilepsy ends after childhood, some forms
of epilepsy are associated only with conditions of childhood that cease once a child grows up.
Approximately 70%of children who suffer epilepsy during their childhood eventually outgrow.
There are also some seizures, such as febrile seizures, that have one-time occurrence during
childhood and do not result in permanent febrile seizure. The worldwide prevalence of active
febrile seizure is between four and ten per thousand populations. Epidemiologic studies of febrile
seizure have done much to define the frequency of seizures and seizure disorders in the
population and to provide a far more accurate understanding of prognosis. Although the majority
of individuals with febrile seizure do very well with respect to seizure control, they still face
many challenges in everyday life. A recent meta-analysis of published and unpublished studies
puts the overall prevalence rate of febrile seizure in India as 5.59 per 1,000 populations, with no
statistically different rates between men and women or urban and rural residence. Based on the
11
total projected population of India in 2001 the estimated number of people with epilepsy is 5.5
million.
Midhun Lal (2011) conducted a population based cohort study was conducted to examine the
effect of pregnancy and neonatal factors on the subsequent development of childhood febrile
seizure in Nova Scotia, Canada were followed up to December 2001. Data on pregnancy and
neonatal events and on diagnosis of childhood febrile seizure were obtained through record
linkage of 2 population based databases; the Nova Scotia Atlee Perinatal Database and the
Canadian febrile seizure Database and Registry. Factors analysed included events during the
prenatal, labor and delivery, and neonatal time periods. Cox proportional hazards regression
models were used to estimate relative risks at 95 per cent confidence interval. There were 648
new cases of febrile seizure diagnosed among 124,207 live births, for an overall rate of 63 per
100,000 persons. Incidence rates were highest among children <1 year of age.
Bahadhoor (2011) done a home based survey was done on psychiatric disorders in 8 to12
year old children in Calicut District, Kerala, India. One thousand one hundred and ninety-two
consecutive children underwent neurological and psychometric assessments. The projected
number of children with a history of febrile seizures was 120 giving a lifetime incidence of
(10.1%). Recurrent febrile seizures predominated and these were strongly associated with a
history of perinatal adversity. Febrile seizures were 9 independently associated with indices of
infective illness and mother‘s education. Epilepsy developed in (2.7%) of children with febrile
seizures.
Journal of Pediatrics (2012) the article on advances in febrile seizure states that the
prevalence rate of febrile seizure in countries of Asia was (4.4), Japan (1.7), Pakistan (4.7),
Kashmir in India (2.4), Srilanka (9.0) and Guan (4.9) million. This prevalence rate indicates that
prevalence of febrile seizure in Asian countries is comparatively higher than the prevalence in
the world.
Daisy (2012) said that in India, there are 30 million people affected by febrile seizure in 2004.
About one in two hundred school children are affected with febrile seizure, about one person in
twenty has a seizure of some type during life, and in the population at large about one in 200 has
febrile seizure. Most of those who develop idiopathic febrile seizure do so before the age of 20
12
years. The general systemic conditions in which seizures most commonly occur in children is
due to hypoxia or high fever. As the understanding of its physical and social burden has
increased, it has moved higher up in the world health agenda. 8 Seizure disorders are more
common among children between 6 months of age and 15 years and in new-born period. It has
been estimated that about 4 to 6% of all children will have fits during their lifetime and 90% of
convulsive disorders have their onset in early life. One in 15 or 20 children admitted in hospitals
give a history of convulsion.
Jung Hye Byeon (2018) published Febrile seizures are the most common type of seizure
during childhood, reportedly occurring in 2–5% of children aged 6 months to 5 years. However,
there are no national data on the prevalence of FS in Korea. This study determined the
prevalence, incidence, and recurrence rates of FS in Korean children using national registry data.
Methods The data were collected from the Korea National Health Insurance Review and
Assessment Service for 2009–2013. Patients with febrile convulsion as their main diagnosis were
enrolled. The overall prevalence of FS in more than 2 million children younger than 5 years was
estimated, and the incidence and recurrence rates of FS were determined for children born in
2009. Results The average prevalence of FS in children younger than 5 years based on hospital
visit rates in Korea was 6.92% (7.67% for boys and 6.12% for girls). The prevalence peaked in
the second to third years of life, at 27.51%. The incidence of FS in children younger than 5 years
(mean 4.5 years) was 5.49% (5.89% for boys and 5.06% for girls). The risk of first FS was
highest in the second year of life. The overall recurrence rate was 13.04% (13.81% for boys and
12.09% for girls), and a third episode of FS occurred in 3.35%. Conclusions Our study
determined the overall prevalence of FS using data for the total population in Korea. The
prevalence was comparable to that reported for other countries. Patients with three episodes of
FS need to be monitored carefully.
Many parents still have a negative attitude about febrile seizure. Some of them feel it is
contagious. Hence during the episodes of seizures the children are not given any assistance or
care. The availability of antiepileptic drugs and the prolonged medical care needed by children
with febrile seizure justify the careful planning of a social program.
13
Fig:1.5
Incidence rate of febrile seizures for different ages. The cumulative incidence
rate was 5.49% among those aged 4 years (age range 42-54 months).
Fig:1.6
Frequencies of first, second, and third episodes of FS. The recurrence rates
of FS (second and third episodes of FS) were highest among those aged 3
years (age range 30-42 months). FS: febrile seizures.
14
It is also found that society‘s misconceptions have a major impact on peoples view
towards febrile seizure and its management in rural areas in various parts of the country. Parental
fear of convulsion is the major problem with serious negative consequences in their daily life. In
early times people believed febrile seizure as a divine origin and were called the sacred disease
because someone with epilepsy was thought to be ―seized‖. Majority of mothers have false belief
about febrile seizure and they have different knowledge, attitude and practices especially in low
socio-economic families. Global campaign against febrile seizure in Senegal, Zimbabwe and
Argentina showed that the training and education programmes of parents of children suffering
with febrile seizure effective and disseminating the knowledge regarding febrile seizure.
The parents should involve themselves in matters concerning their Childs febrile seizure.
It is important to involve the siblings of the febrile seizure, child helps to develop better
understanding of condition as they may have all kinds of fears and misinformation about the
disease. In many families, the mother tends to come closer to the situation. Often, she is the
parent who visits the doctor, or meets the teacher or 10 talks to other parents at the local level.
As she learns more about the febrile seizure, it becomes much easier to adjust with the idea of
having a child with febrile seizure.
Febrile seizure children express anxiety and embarrassment and see themselves as being
different and inferior. A thorough evaluation of the patient‘s attitude and expectations
concerning health maintenance is essential. The attitude and expectations of family members
should also be evaluated since their understanding and support is crucial to the patient‘s ability to
adjust to his condition. It is important for the nurse to be aware of potential prejudices which
may be encountered by the client and his family.
During the clinical posting the investigator noticed that during the year of 2015 there
were 184 admissions of children with seizure disorders, 253 cases of febrile seizures and 63
cases of convulsions of new-born. The mothers of children were anxious about the disease
condition and also they had many doubts regarding the etiology, risk factors and both medical
and home management of children with seizure disorder. It is very important to adhere with
therapeutic regimen and the care giver should reinforce to avoid skipping of antiepileptic drugs.
It is also important to give attention to the emotional aspect of the child. So it is found that a
15
structured Teaching Programme will be a guide for mothers regarding management of febrile
seizure at home.
1.3 STATEMENT OF THE PROBLEM
―Evaluate the effectiveness of educational intervention on febrile seizure among the
mothers of under five children at Primary Health Center Podanur.
1.4 OBJECTIVES
To assess the existing level of knowledge and practice on febrile seizure among the
mothers of under five children.
To evaluate the effectiveness of educational intervention on febrile seizure among
mothers of under five children.
To associate the pretest knowledge and practice score with selected demographic
variables.
To identify the correlation between post test knowledge and practice on febrile seizure
among the mothers of under five children.
1.5 HYPOTHESIS
H1- There will be a significant difference between pretest and post test knowledge score on
febrile seizures.
H2- The mean post test practice score will be significantly higher than mean pretest practice
score.
H3- There will be a significant association between pretest scores of knowledge and selected
demographic variables.
H4- There will be a significant association between pretest practice score and selected
demographic variables.
H5- There will be significant relation between the post test knowledge and practice score.
16
1.6 OPERATIONAL DEFINITIONS
•
Evaluate: It means judgment of the value of that which is being assessed. In this study, it
means judging the effectiveness of learning package regarding febrile seizure.
•
Effectiveness: It refers to the extent of which the learning package on febrile seizure
gives the desired effect in improving knowledge of mothers attending in Primary Health
Center, Podanur.
•
Educational Intervention: It is a teaching module developed by the researcher to impart
knowledge on febrile seizure. In this study it is referred as organized content with
relevant audio visual aids to provide information on febrile seizure among mothers of
children.
•
Knowledge: It refers to the response received from the mothers regarding febrile seizures
in their children as measured by a structured knowledge questionnaire.
•
Practice: It refers to the activities reported by mothers in relation to prevention,
compliance with therapeutic regimen, and management of child with febrile seizure as
measured by checklist.
•
Mothers: It refers a mothers of under five children attending primary health center,
podanur.
•
Febrile Seizure: A febrile seizure is a convulsion in a child caused by a 100.4˚f in body
temperature, often from an infection.
1.7 ASSUMPTIONS
This study assumes that, knowledge is the basis of practice
Parents of children may have inadequate knowledge regarding febrile seizure.
Educational intervention is interactive and effective way to gain knowledge regarding
febrile seizure and related health problems.
17
1.8 DELIMITATIONS
The study is limited to
Mothers of children attending Primary Health Center, Podanur.
Sample size is 40.
Data collection period is limited to 4 weeks.
Educational intervention will be evaluated by self administered questionnaire.
1.9 PROJECTED OUTCOME
This study will help to evaluate the level of knowledge regarding febrile seizure.
This study will help the mothers of children to gain knowledge regarding febrile
seizure.
The study will help to prevent complications of febrile seizure such as impaired
growth and development.
1.10 CONCEPTUAL FRAME WORK
Based on the Nola J. Pender (1996)
Health promotion model was designed to be a ―Complementary counterpart to models of health
protection‖. The health promotion model describes the multi dimensional nature of persons as
they interact with in their environment to pursue health.
It defines ―Health as a ―positive dynamic state not merely the absence of disease‖.
This model focuses on following three areas:
Individual characteristics and experiences.
Behavioral specific cognition and affect.
Behavioral out comes.
Individual characteristics and experience:- The health promotions model notes that each
person has unique personal characteristics and experience that affect subsequent action. In this
study we are focusing the factors influencing the mother and child on biological, psychological,
and socio cultural.
18
Behavioral specific cognition and affect:- The set of variables for specific knowledge and
affect have important significance. In this we evaluate the specific cognition and affects related
to febrile seizure.
Behavioral outcomes:- It is the end point. In this we are evaluating the mothers health promoted
behaviours through post test questionnaires on prevention of febrile seizure.
19
Individual characteristics and
experience
Behaviour specific cognitive and
affect
Behaviour outcome
Perceived benefits of action
Pre test
Prior related behavior
Mothers may have inadequate
knowledge
and
practice
on
prevention and care during febrile
seizure.
Intervention
Perceived barrier to action
Inadequate exposure to health
education related to prevention and
care of children during febrile seizure
Perceived self efficacy
Personal Factors
Biological factors; Age, Sex, type of
family.
Immediate competing demands
and preference
Mothers of children will be able to
gain adequate knowledge on febrile
seizure
Mothers of children are able to
execute health promotion behavior
related to febrile seizure
Psychological factors; knowledge,
beliefs, Personal norms.
Teaching programme related affect
Socio-cultural factors Consists of
occupational status, family income,
educational status.
By
administering
the
educational
intervention mothers of children will gain
adequate knowledge regarding febrile
seizure.
Low control : environmental factors:age, sex, religion, type of family, bread
winner, food habits.
High control: education, monthly
income
Post test
Commitment to a
plan action
Implementation of
educational intervention
on prevention of febrile
seizure group with the
duration of 60 Minutes.
Health Promotion behaviour
Accomplishing of health promotion
behavior on knowledge regarding
prevention of febrile seizures
Prevent the febrile seizure for children
and care of childhood febrile seizure.
Encourage the children to take healthy
foods like milk, cereals, pulses eggs,
fish, etc.. and prevent the infections.
Interpersonal Influences
Encouragement and support from primary
health care personnel, mothers and children
Inadequate
knowledge
Situational influences
Favorable family and Primary Health
Center environment
Moderately
adequate
knowledge
Adequate
knowledge
FEED BACK
Figure 1.8 Conceptual frame work based on modified Pender‟s Health Promotion Model (1996)
20
CHAPTER - II
REVIEW OF LITERATURE
CHAPTER - II
REVIEW OF LITERATURE
“Every moment is an experience” - Jake Roberts
INTRODUCTION
Review of literature is a broad systematic and critical collection and evaluation of
important scholarly published literature as well as unpublished materials. The review serves as
an essential background for any research. The review of literature is essential to all steps of the
research process. It is an account of what is already known about a particular phenomenon. The
main purpose of literature review is to convey to the reader about the work already done and the
knowledge and ideas that have been already established on a particular topic of research. From
this prospective the review is based on broad, systemic and critical collection and evaluation of
the important published scholarly literature and unpublished research findings, critically reading
the literature is to develop a sound study that contribute to development of knowledge in the
aspect of theory, research, evaluation and practice.
According to Polit and Hungler (2010) review of literature is a critical summary of
research on a topic of interest generally prepared to put a research problem in context to identify
gaps in prior studies to justify a new investigation.
According to Suresh.K.Sharma (2013) literature review is defined as a broad,
comprehensive, in depth, systematic and critical review of scholarly publication, unpublished
printed or audio visual materials and personal communication.
THE LITERATURE WAS REVIEWED AND PRESENTED UNDER THE FOLLOWING
SECTIONS
Section-I: Studies and literature related to febrile seizure in children
Section-II: Studies and literature related to educational intervention on febrile seizure
21
SECTION-I: STUDIES AND LITERATURE RELATED TO FEBRILE SEIZURE IN
CHILDREN
European Journal of Pediatrics (2011) modified and published assessment of febrile
seizure in children; Febrile seizures are the most common form of childhood seizures, affecting
2-5% of all children and usually appearing between 3 months and 5 years of age. Despite its
predominantly benign nature, a febrile seizure (FS) is a terrifying experience for most parents.
The condition is perhaps one of the most prevalent causes of admittance to pediatric emergency
wards worldwide. The risk of epilepsy following FS is 1-6%. The association, however small,
between febrile seizure and epilepsy may demonstrate a genetic link between febrile seizure and
epilepsy rather than a cause and effect relationship. The effectiveness of prophylactic treatment
with medication remains controversial. There is no evidence of the effectiveness of antipyretics
in preventing future febrile seizure. Prophylactic use of paracetamol, ibuprofen or a combination
of both in febrile seizure, is thus a questionable practice. There is reason to believe that children
who have experienced a simple febrile seizure are over-investigated and over-treated. This
review aims to provide physicians with adequate knowledge to make rational assessments of
children with febrile seizures.
Lalith. K (2011) conducted a prospective study which carried out in a tertiary hospital to
evaluate the knowledge and attitudes of parents toward children with febrile seizure.
Questionnaires were administered to all the parents who attended the hospital with their children
diagnosed of febrile seizure. Two hundred and eighty parents whose children suffered from
febrile seizure participated in the study. The investigator concluded that more than 90% of
parents and caregivers know about febrile seizures. There is a need to disseminate more
information to the public about 22 its causes, clinical manifestation, approach to managing a
convulsing child, and its outcome and periodic medical campaigns aimed at educating the public
about febrile seizure through the media could go a long way in reducing the morbidity and
mortality associated with this disorder.
Misle. K. et.al., (2012) anthropological study was conducted to analyse current parental
perceptions of febrile seizures in order to improve the quality of management, care, and
explanations provided to families at paediatric emergency unit. Investigators analysed
22
interviews of 37 parents, whose child was admitted to the paediatric emergency unit due to a first
seizure. The parental experience of the crisis was marked by upsetting memories of a "scary"looking body and the perception of imminent death. The meaning attributed by parents to the
word "seizure" and "epilepsy" usually referred to an exact clinical description of the
phenomenon, but many admitted being unfamiliar with the term or at least its origin.
Understanding and integrating these parental interpretations seems essential to improving care
for families who first experience this symptom.
Reese C. Graves (2012) published febrile seizures; risk, evaluation and prognosis for that
Febrile seizures are common in the first five years of life, and many factors that increase seizure
risk have been identified. Initial evaluation should determine whether features of a complex
seizure are present and identify the source of fever. Routine blood tests, neuro imaging, and
electroencephalography are not recommended, and lumbar puncture is no longer recommended
in patients with uncomplicated febrile seizures. In the unusual case of febrile status epilepticus,
intravenous lorazepam and buccal midazolam are first-line agents. After an initial febrile seizure,
physicians should reassure parents about the low risk of long-term effects, including neurologic
sequelae, epilepsy, and death. However, there is a 15 to 70 percent risk of recurrence in the first
two years after an initial febrile seizure. This risk is increased in patients younger than 18 months
and those with a lower fever, short duration of fever before seizure onset, or a family history of
febrile seizures. Continuous or intermittent antiepileptic or antipyretic medication is not
recommended for the prevention of recurrent febrile seizures.
Joshua R. Francis. (2016) conducted an observational study of febrile seizures: the
importance of viral infection and immunization, Children aged 6 months to 5 years presenting to
the Emergency Department of a tertiary children‘s hospital in Western Australia with febrile
seizures were enrolled between March 2012 and October 2013. Demographic, clinical data and
vaccination history were collected, and virological testing was performed on per-nasal and perrectal samples. The result was one hundred fifty one patients (72 female; median age 1.7y; range
6 m-4y9m) were enrolled. Virological testing was completed for 143/151 (95%). At least one
virus was detected in 102/143 patients (71%). The most commonly identified were rhinoviruses
(31/143, 22%), adenovirus (30/151, 21%), entero viruses, (28/143, 20%), influenza (19/143,
13%) and HHV6 (17/143, 12%). More than one virus was found in 48/143 (34%). No significant
23
clinical differences were observed when children with a pathogen identified were compared with
those with no pathogen detected. Febrile seizures occurred within 14 days of vaccine
administration in 16/151 (11%). At least one virus was detected in over two thirds of cases tested
(commonly picorna viruses, adenovirus and influenza). Viral co-infections were frequently
identified. Febrile seizures occurred infrequently following immunization.
Alexander KC Leung (2018) published febrile seizure overview; To provide an update on
the current understanding, evaluation, and management of febrile seizures. In that results ,
Febrile seizures, with a peak incidence between 12 and 18 months of age, likely result from a
vulnerability of the developing central nervous system to the effects of fever, in combination
with an underlying genetic predisposition and environmental factors. The majority of febrile
seizures occur within 24 hours of the onset of the fever. Febrile seizures can be simple or
complex. Clinical judgment based on variable presentations must direct the diagnostic studies
which are usually not necessary in the majority of cases. A lumbar puncture should be
considered in children younger than 12 months of age or with suspected meningitis. Children
with complex febrile seizures are at risk of subsequent epilepsy. Approximately 30–40% of
children with a febrile seizure will have a recurrence during early childhood. The prognosis is
favorable as the condition is usually benign and self-limiting. Intervention to stop the seizure
often is unnecessary.
J.Clin Neurol (2018) conducted a study which determined the prevalence, incidence, and
recurrence rates of FS in Korean children using national registry data. The data were collected
from the Korea National Health Insurance Review and Assessment Service for 2009–2013.
Children with febrile convulsion as their main diagnosis were enrolled. The overall prevalence of
FS in more than 2 million children younger than 5 years was estimated, and the incidence and
recurrence rates of FS were determined for children born in 2009. Results of the average
prevalence of febrile seizure in children younger than 5 years based on hospital visit rates in
Korea was 6.92% (7.67% for boys and 6.12% for girls). The prevalence peaked in the second to
third years of life, at 27.51%. The incidence of FS in children younger than 5 years (mean 4.5
years) was 5.49% (5.89% for boys and 5.06% for girls). The risk of first FS was highest in the
second year of life. The overall recurrence rate was 13.04% (13.81% for boys and 12.09% for
girls), and a third episode of febrile seizure occurred in 3.35%. Our study determined the overall
24
prevalence of febrile seizure using data for the total population in Korea. The prevalence was
comparable to that reported for other countries. Children with three episodes of febrile seizure
need to be monitored carefully.
Dr. Nurun Nahar (2019) conducted a study on clinical aspects of febrile seizures,
knowledge, attitude, practice and its impact in admitted children and Socio-demographic
characteristics of the parents; febrile seizures are common and mostly benign. They are the most
common cause of seizures in children less than five years of age. There are two categories of
febrile seizures, simple and complex. 116 Children‘s with FS were listed within the study WHO
(World Health Origination) were aged matched to four controls to work out risk factors for a
primary febrile seizure. The mean (±SD) age of youngsters underneath the study was 22.4± 14.3
months. 63 (54.3%) of the Children‘s were aged 18 months and below, mean (±SD) age of onset
of seizures was 16.1 ± 9.6 months. Male to feminine ration was 1.5: 1.70 Children‘s (60.3%) of
febrile seizure were simple seizures whereas 46 Children‘s (39.7%) were complicated. In
Children‘s with perennial febrile seizure, 25 had complicated seizures representing 54.3% of
total children with complicated seizures and seventeen children had a simple seizure. 6.9%
connected the cause on to looking and another 6.9% to witch craft. 33.6% of oldsters thought of
febrile seizure as a kind of brain disease. 26.7% of the oldsters recognized aspiration as associate
acute complication of seizure. Injuries (19.8%) and cardiopulmonary arrest (2.6%) were
recognized to a lesser degree. Health institutes and personnel (12.9%) and media (9.5%) were
weak sources of data. Ancient treatment was advocated by 30.2% of oldsters. Care to be applied
throughout a seizure was renowned by few and performed by fewer. Non-recommended or
perhaps harmful practices were thus prevalent (82%).
Navneet Kumar (2019) conducted a study and found out that febrile seizures are commonly
seen in children and about one-third of the children develop a recurrence of febrile seizures. The
main objective is to study the risk factors associated with recurrence of febrile seizures in Indian
children. This prospective, longitudinal study was carried out in the Department of Pediatrics,
GSVM Medical College, Kanpur. All children, 6 months to 5 years of age, attending the
department from February 2015 to January 2016 presenting with first febrile seizures were
included in the study and followed up for recurrence. Results of 528 children, 174 (32.9%) had
recurrence and 354 (67.1%) had a single episode of febrile seizures. Recurrence was more in
children <18 months (41.3%) as compared to children ≥18 months (24.1%). Children with
25
temperature 101°F during the seizure had a recurrence rate of 52.5% while recurrence was seen
in only 17.2% in children with temperature ≥105°F. There was a significant declining trend of
recurrence with increase in temperature. Recurrence was significantly more common in children
with a family history of febrile seizures (45.5%) as compared to those without family history
(27.8%). Multiple logistic regression analysis revealed that younger age at onset of first seizure,
lower temperature during the seizure, brief duration between the onset of fever and the initial
seizure, and family history of febrile seizures were risk factors significantly associated with
recurrence of febrile seizures in children.
SECTION-II: STUDIES AND LITERATURE RELATED TO EDUCATIONAL
INTERVENTION ON FEBRILE SEIZURE
R C Parmar (2011) conducted the study on knowledge, attitude and practices of parents of
children with febrile convulsion. In that Parental anxiety and apprehension is related to
inadequate knowledge of fever and febrile convulsion. Prospective questionnaire based study in
a tertiary care centre carried over a period of one year. 140 parents of consecutive children
presenting with febrile convulsion were enrolled. Chi-square test used. It result, 83 parents
(59.3%) could not recognise the convulsion; 90.7% (127) did not carry out any intervention prior
to getting the child to the hospital. The commonest immediate effect of the convulsion on the
parents was fear of death (n= 126, 90%) followed by insomnia (n= 48, 34.3%), anorexia (n= 46,
32.9%), crying (n= 28, 20%) and fear of epilepsy (n= 28, 20%). Fear of brain damage, fear of
recurrence and dyspepsia were voiced by the fathers alone (n= 20, cumulative incidence 14.3%).
109 (77.9%) parents did not know the fact that the convulsion can occur due to fever. The longterm concerns included fear of epilepsy (n= 64, 45.7%) and future recurrence (n= 27, 19.3%) in
the affected child. For 56 (40%) of the parents every subsequent episode of fever was like a
nightmare. Only 21 parents (15%) had thermometer at home and 28 (20%) knew the normal
range of body temperature. Correct preventive measures were known only to 41 (29.2%).
Awareness of febrile convulsion and the preventive measures was higher in socio-economic
grade (P< 0.05). At last concluded that parental fear of fever and febrile convulsion is a major
problem with serious negative consequences affecting daily familial life.
26
Magnil. L (2011) conducted a quasi-experimental study to assess the impact of health
education on knowledge and home management of febrile convulsion amongst mothers in a rural
community in North Western Nigeria. A one in three samples of fifty mothers that met the
eligibility criteria where selected using systematic random sampling. Interviewer administered
same structured questionnaire with close and open-ended questions to obtain data during pre and
post-test. The study concluded that the use of effective educational intervention programmes and
parental support groups will go a long way in reducing the incidence of febrile convulsions
among children in our communities.
Kepler (2011) conducted a prospective cross – sectional study on parent‘s knowledge and
attitude towards children with febrile seizure, and to identify contributing 21 factors to negative
attitudes conducted among parents attending the paediatric neurology clinics of king Abdul-Aziz
university Hospital, Jeddah, Saudi Arabia. A structured 40-item questionnaire was designed to
examine their demographics, knowledge, and attitudes. A total of 117 parents were interviewed,
57% were mothers. The level of knowledge among parents of epileptic children needs
improvement. Many have significant misconceptions, negative attitudes, and poor parenting
practices. Increased awareness and educational programme are needed to improve the quality of
life of this family.
Lovera. D (2011) conducted a cross sectional study to determine the knowledge, attitudes
and practices of parents and guardians of children with febrile seizure regarding the illness
conducted in Paediatric Clinic at Kenyatta National Hospital revealed that more than 77% of
the parents/guardians had some knowledge on the type of illness their children were suffering
from, the features of a febrile convulsion, the alerting features before febrile convulsions, the
type of antiepileptic drug treatment their children were receiving and the potential hazards to an
seizure child during a febrile convulsion. Samples consisted of 116 parents and guardians and
they were interviewed using a semi-structured questionnaire. Focused group discussions were
also carried out on 42 other parents and guardians. The study concluded that higher level of
formal education of the Parent/Guardian had a positive influence on their Knowledge and
practice towards febrile convulsion.
27
Swetha. K (2011) conducted a study which entitled the effectiveness of informational
booklet on cure and management of febrile seizure children was conducted in Karnataka. The
objectives were to assess the knowledge of mothers of febrile seizure children using the
structured knowledge questionnaire, to develop and validate a booklet on epilepsy care and home
management for mothers of febrile seizure children. Population comprised of mothers of children
with febrile seizure, who were in the age group of 2 to 12 years. Non probability purposive
sampling technique was utilised. Tools used for the study included, Background Information,
Structured Knowledge 23 Questionnaire and an Opinionnaire. The study concludes that the
information booklet on epilepsy care and home management and reinforced teaching was an
effective strategy for enhancing the knowledge of the mothers of febrile seizure children
regarding care and rehabilitation of their children.
Pooja. R (2012) conducted a prospective questionnaire-based study to evaluate the
knowledge, attitude and practice of mothers of under-five children suffering with febrile
convulsion at the Mofid children hospital. Sample consisted of 126 mothers of children with
febrile convulsion. The study result shown that most common cause of concern among parents
was the state of their child‘s health in the future, followed by the fear of reoccurrence, mental
retardation, paralysis, physical disability and learning dysfunction. Awareness of preventive
measures was higher in mothers with high educational level. Majority of mothers (76%) did not
know anything about the 19 necessary measures in case of recurrence. This study concluded that
parental fear of febrile convulsion is the major problem, with serious negative consequences
affecting daily familial life.
Misbha. K (2012) conducted a cross sectional study to evaluate the concerns and home
management of childhood convulsions among mothers in Tesbesun, Nigeria. Samples consisted
of 500 mothers of children with convulsion. A structured questionnaire was used for
interviewing the study subjects and the study period was 10 weeks. A result of the study showed
that fear of death was the commonest concern (450, 90%) among mothers. Putting the hand
and/or a spoon into the mouth of the convulsing child was the commonest unwholesome practice
(74, 61.2%). None of the subjects safely put the convulsing child on his/her side. The study
concluded that mothers concerns are precursors of mismanagement of childhood convulsions,
28
and health education regarding seizure management is required for the mothers for effective
management.
Arash Najimi(2013) published the study on the effect of educational program on
knowledge, attitude and practice of mothers regarding prevention of febrile seizure in children,
an experimental and prospective study conducted on mothers with children under 2 years of age
referred to the Health Care Centers of Isfahan City in 2009.The result was this study mean age of
mothers in the intervention and control groups was 26.75 ± 3.9 and 26.84 ± 4 years, receptively,
and also mean age of children in the intervention and control groups was 11.93 ± 5.5 and 12.91 ±
5 months, respectively. Mothers of the intervention and control groups were identical in terms of
education (P = 0.344). The results showed that mothers of both groups had no significant
difference in terms of employment status, educational level and history of seizure. Employment
status was of high importance due to duration of implemented cares by mothers so that previous
studies have shown that there was a significant relationship between educational level and
knowledge of mothers about febrile seizure.
Ninan. N (2013) conducted a descriptive survey to assess the knowledge and practices
regarding febrile convulsions among parents of children below 5 years admitted in the
emergency service unit of Behcetz Children Hospital, Turkey. Sixty three parents whose children
a febrile convulsion had for the first time included in first group and fifty nine parents whose
children had recurrent febrile convulsions included in second group. The study concludes that
there is an efficacy of parental first aid practices regarding epilepsy can improve the knowledge
and practices of parents of children who is suffering from convulsive disorder.
Romen. L. P (2013) conducted a randomized, controlled trial in Santiago, Chile to test the
impact of a child-centered, family-focused educational program for children aged 7-14 years
with febrile seizure and for their parents. The objectives of the program developed and pilottested in Los Angeles, California were to increase the children's knowledge, perceptions of
competency, and skills related to dealing with febrile seizures. All participants were pretested
and then retested 5 months after completion of the educational intervention. The study concluded
that Children in the experimental group without serious behavioural problems also reported
significantly better behaviour after the intervention than the control children.
29
Mishel. P (2013) conducted a descriptive cross sectional community based study to assess
the knowledge, attitude and practice among parents of Sudanese epileptic patients. Three
hundred and thirteen samples were included in the study. The study result reveals that most of
the respondents know the disease and had witnessed 26 an attack. Most of the respondents
mentioned loss of consciousness as the major symptom. More than two thirds mentioned that it is
not contagious. Most of the respondents claimed that it can be controlled, and two thirds
preferred medical treatment. The study revealed that half of the respondents had shown favorable
attitudes and practice. The study concluded that the level of knowledge, attitude and practice
towards epilepsy needs community educational programmes to fill the gaps, and minimize the
stigma.
Wolens Moor (2014) conducted a pre experimental study to evaluate the usefulness of the
Seizures and Epilepsy Education (SEE) program in improving quality of life, management of the
seizure condition, and health care utilization in families having a child with family represented.
Children attended if they were at least 12 years of age. Both parents and children reported
improvement in quality of life relating to child mental health after attending the SEE program.
Results suggest that attending the SEE program may be beneficial to families having a child with
epilepsy.
Hannef V B (2014) conducted a study to verify the effectiveness of the support group in the
identification of family variables linked to febrile seizure, Pre-test were applied to parents of 21
children with benign febrile seizure of childhood recently diagnosed, from 5 24 to 15 years, who
participated in the groups at HC/Unicamp. There was a presentation of an educational video,
discussion and application of the post-test 1. After six months, the post-test 2 was applied. The
study concluded that the demystification of beliefs supplied from the groups influenced the
family positively, prevented behaviour alterations and guaranteed effective care in the attendance
to the child with febrile seizure.
Mohith. P (2014) conducted a study to evaluate the efficacy of the modular educational
program for children with febrile seizure and their parent. This program was developed by an
interdisciplinary project group to improve knowledge, coping, and treatment outcome, emotional
and practical adaptation to the condition. A prospective, controlled, multi-centre, pre-post study
30
design was used to examine the efficacy of the program in the treatment group compared to the
control group. Parents of the treatment group showed significant enhancement in knowledge
regarding febrile seizure, attitude towards febrile seizure, management of febrile seizures and
significant reduction of fear and restrictions of their child with febrile seizure.
Martin. C (2014) descriptive study was conducted to assess knowledge and attitude among
parents of children with febrile seizure in Ethiopia. Sample consisted of 300 parents of children
with febrile seizure. A structured knowledge questionnaire and attitude rating scale was used to
collect data. The results showed that majority of parents (77%) had a positive attitude towards
febrile seizure and had complete seizure control after treatment. Delay in treatment and poor
compliance due to false religious beliefs, ignorance and superstitious was observed in 33%.
Eighty percentage (80%) cases felt that religion had helped them in coping with febrile seizure.
Zaker. A (2014) conducted a cross sectional study to evaluate knowledge, perceptions, and
attitudes of families toward epilepsy and then to correlate knowledge with quality of life and
stigmatization of children with epilepsy. Specific questionnaires were administered to children
aged 8 to 17 with epilepsy and their parents. Poor school performance, less social support, less
self-esteem, higher anxiety, greater stigmatization, and more depressive symptoms were
documented in children who were less knowledgeable. Parents were found to be more
knowledgeable about the antiepileptic drugs used, understanding both the effects and the side
effects of the medications. Knowledge about epilepsy is associated with less perceived
stigmatization and social isolation, as well as fewer depressive symptoms and misperceptions.
Raghupathi. H (2015) conducted a pre experimental study in the Paediatric Neurological
unit and the paediatric outpatient clinic to explore the effect of maternal practice on their
epileptic children's quality of life. A convenient sample of 50 epileptic children of 8-12 years and
their mothers were included in the study. Four tools were used to collect the required data.
Structured interview sheet is used to 25obtain the socio demographic characteristics, medical
history of children and their families and mothers practice questionnaire sheet were used to
assess mothers' practices regarding care of epileptic children. Seizure severity scale is used to
assess severity of epileptic fits and Ped's quality of life inventory version 4.0 TM is used to
assess children quality of life. Results of the study revealed that, the educational program showed
31
significant improvement of mothers' practices and improved children quality of life. Correlation
between quality of life of the epileptic children and mothers' practice score and seizure severity
scores was statistical significant correlation between mothers 'practices score and quality of life
of epileptic children immediately and three months after the program.
Maria Kelly (2016) conducted the study in which semi-structured interviews were
conducted with 23 parents at six ante-natal clinics in the south west of Ireland during March and
April 2015. The Francis method was used to detect data saturation and thereby identify sample
size. Thematic analysis was used to analyse the data. It result was twenty-three parents
participated in the study. Five themes emerged from the data: assessing and managing the fever;
parental knowledge and beliefs regarding fever; knowledge source; pharmaceutical products;
initiatives. Parents illustrated a good knowledge of fever as a symptom. However, management
practices varied between participants. Parents revealed a reluctance to use medication in the form
of suppositories. There was a desire for more accessible, consistent information to be made
available for use by parents when their child had a fever or febrile illness.
Mohammed Barzegar (2016) the effects of two educational strategies on knowledge,
Attitude, Concerns, and practices of mothers with febrile convulsive children, the study adopts a
quasi-experimental research design. A total of 102 mothers of children presenting with febrile
seizure and admitted to a teaching hospital in Iran were equally assigned to three groups: Group I
received no intervention (control group), Group II received a febrile seizure information
pamphlet, and Group III received the febrile seizure information pamphlet plus verbal
instruction. Knowledge, attitudes, concerns, and practices of participants regarding febrile
seizure were measured as primary outcomes in the pre- and post- intervention stages. The results
showed that although only a slight change in attitudes toward febrile seizures was found, both the
febrile seizure information pamphlet alone and the febrile seizure information pamphlet plus
verbal instruction were significantly effective in improving the knowledge, attitudes, concerns,
and practices of mothers with febrile convulsive children toward febrile seizures.
Mahbobeh Sajadi, (2017) mothers‘ Experiences about Febrile Convulsions in Their
Children: A Qualitative Study., This study was based on a qualitative content analysis. 12
mothers in Amir Kabir hospital of Arak city participated in the study and shared their
32
experiences through semi-structured interviews. The gathered data were analysed using
Graneheim and Lundman‘s (2004) method.Its result was exploring the experiences of mothers
whose children suffered from febrile convulsion reflected three themes: perceived threat, seeking
solution, and difference in adaptation.
Srinivas S. (2018) conducted a study on parental knowledge, attitude and
practices
regarding febrile convulsion, It was a prospective questionnaire study conducted over a period of
one year from January 2016 to January 2017 in Department of Paediatric of a tertiary care
hospital KIMS, Bangalore. 110 children with febrile convulsion in the age group of 6 months to
5 years were enrolled. The study result was out of 110 children, 82 had single convulsion and 28
had recurrent convulsions. Mean age of onset of first febrile convulsion was 20 months. About
50 (45.45%) had experienced convulsion with one-episode of fever. Only 46 (41.8%) of parents
recognized convulsion. Others interpreted convulsion as shivering (20.9%), evil effect (7.2%),
excessive cry tantrum (10.9%), fainting spell (8.18%) and lethargy (20%). 88 (80%) did not
carry out any intervention prior to getting the child to hospital. Effect of convulsion on parents
was fear of death (82.7%), fear of epilepsy (17.3%), fear of recurrence (34.5%). 85% parents did
not know that convulsion can occur due to fever. 32% thought that traditional treatment would
help. Only 38% had thermometer at home and 23% knew the normal range of body temperature.
Preventive measures were known to 44%.
Noor (2019) conducted the study was Parental knowledge and practice regarding febrile
seizure in their children, Febrile seizure (FS) is a benign convulsive disorder in under 5-year-old
children, but at the same time, it is an alarming event in the lives of both child and parents. Lack
of parent's knowledge about the nature of febrile seizure and how they should deal with it can
lead to poor management. Regarding maternal age and paternal age, they ranged between 15–43
and 20–50 years, respectively. More than half of them live in urban areas, and concerning
educational level of mothers, 70% were either illiterate or had a primary level of education.
Majority of FS children were presented with first attack who represent a percentage of about
69%. About half of the respondents have good level of knowledge. Fifty-two percent of them
considered that FS is equivalent to epilepsy, 69% stated that it is a life-threatening event, and
80% knew that it occurs during febrile occasions. Only 25% of parents took their children to
doctor during attack of fit without first aids.
33
Manasa Godati (2019) conducted the study was ―To assess the effectiveness of structured
teaching programme on Care of Children with Febrile Seizures among mothers of under five‘s at
selected Urban slum areas, Suryapet‖. A Quasi -experimental single group pre-test, post-test
design was adopted. The population were mothers‘ of children under five years numbered 50.
Convenient sampling technique was adopted for the study. The study was carried out by using a
structured interview schedule and structured teaching programme on care of children with febrile
seizures among mothers having under-five‘s. After 7 days of the structured
teaching
programme, the post –test were conducted by using the same pre-test questionnaire. Major
findings of the study are: In pre-test, regarding knowledge, 22% (11) had inadequate knowledge,
70% (35) had moderately adequate knowledge and only 8% (4) had adequate knowledge.
Regarding knowledge on practices, 2% (1) had inadequate knowledge, 84% (42) had moderately
adequate knowledge and 14% (7) had adequate knowledge. In post-test, 44% (22) had
moderately adequate knowledge, only 56% (28) had adequate knowledge and none were having
inadequate knowledge on care of children with febrile seizures. Whereas 4% (2) had moderately
adequate knowledge 96% (48) had adequate knowledge and none were having inadequate
knowledge on practices. The effectiveness of structured teaching programme on care of children
with febrile seizures was significant at p <0.0001.The study concluded that the data proved that
the structured teaching programme was a primary measure which markedly improve the
knowledge and practices on care of children with febrile seizures among mothers of under-fives.
34
CHAPTER – III
METHODOLOGY
CHAPTER III
RESEARCH METHODOLOGY
Research methodology is the overall plan for addressing the research problem.
Methodology of research refers to way of obtaining, organizing and analyzing data.
Methodological studies address the development, validation and evaluation of research tool and
methods. It includes the descriptions of the research approaches, research design, dependent and
independent variables, sampling design, sampling criteria, description of the tool, pilot study and
a planned format for data collection and a plan for data analysis. The research methodology
involves systematic procedure in which the researcher starts from initial identification of the
problem to its final conclusion.
(Polit and Beck, 2004).
Research methodology is the development and evaluation of data collection instrument,
scale or technique. The role of methodology consists of procedure and technique for conducting
a study.
(Feedith Haber, 2006).
This chapter deals with the methodological approach of the study. The purpose of the
present study was to evaluate the effectiveness of educational intervention on febrile seizures
among the mothers of under five children at primary health center podanur,Coimbatore.
3.1 RESEARCH APPROACH
The research approach instructs the researcher from where the data is to be collected and
how to analyze the data. It also suggest possible conclusion and helps the researcher in ensuring
specialist question in the most accurate and efficient way.
(Celia. E. Willis, 2004).
The term evaluation implies that the worth or merit something being judged.
The quantitative research approach was used to evaluate the effectiveness of educational
intervention on febrile seizure among the mothers of under five children.
35
3.2 RESEARCH DESIGN
Research design is a blue print to conduct a study that maximizes control over factors that
could interfere with the validity of the findings.
(Nancy Burns 2005).
The research design used for the study was Pre experimental one group pre test and post
test design.
It is relatively straight forward research design in which there is a treatment group
without control group. All subjects were given a pre test, receive the treatment and was given a
post test.
The research design adopted for the present study was as follows
E = O1 X O2
E - Experimental group.
O1-Pre test assessment of knowledge and practices of mothers regarding febrile seizure.
X - Implementation of educational intervention on mothers of children.
O2- Post test assessment of knowledge and practices of mothers regarding febrile seizure.
3.3 RESEARCH VARIABLES
According to B.T.Basavanthappa, ―A variable is a characteristic or attribute that
differs among the persons, objects, events and so forth that are being studied‖.
Dependent variables
Knowledge and practice of mothers regarding febrile seizure occurring among the
children.
Independent variables
Educational intervention on prevention and care of children with febrile seizure.
3.4 STUDY SETTINGS
Setting is the physical location and condition in which data collection take place.
(Polit and Hungler 2004).
The study was conducted at Primary health centre, Podanur. This study was conducted
among 40 mothers of under five children attending primary health centre, podanur.
36
3.5 STUDY POPULATION
Population is defined as the entire aggregation of cases that meet a designated set of
criteria.
(Polit and Hungler2004).
The population for the present study was mothers of under five children attending primary
health centre in podanur.
3.6 SAMPLE
Sample is a selected proportion of the defined population.
(B.T. Basavanthappa,2010).
In this study the sample was mothers of under five children attending in primary health
center, podanur.
3.7 SAMPLE SIZE
Sample size is the number of items to be selected form the universe to constitute a
sample.
The sample size was 40 mothers of under five children, attending primary health center,
podanur was considered as the sample for the present study.
3.8 CRITERIA FOR SELECTION OF SAMPLES
3.8.1 Inclusion criteria:
Mothers of under five children who are
Attending primary health center
Able to communicate freely in Tamil/English
Present at the time of data collection
Willing to participate in this study.
3.8.2 Exclusion criteria:
Not willing to participate in the study
Not available during the time of data collection procedure
Mothers of critically ill children
Mothers who are medical/ nursing profession
37
3.9 SAMPLING TECHNIQUE
The sampling technique is the process of selecting a portion of the Population to
represent the entire population.
( Polit and Hungler1999).
Convenient sampling technique was used in this study. In this method the researcher
selected those units of population in the sampling which appear convenient to her or to the
management of the organization where she is conducting research.
3.10 DESCRIPTION OF THE TOOL
The research tool consists of,
Section I: Demographic variables it included Age of the mothers, education, occupation,
religion, type of the family, family monthly income, history of maternal seizure,
previous history of febrile seizure in their family, febrile seizure attack is a life
threatening event, age of the child, child has previous history of febrile seizure, reason
of visit to primary health center, have thermometer at home.
Section II: Self administered questionnaire to assess the knowledge of mothers regarding febrile
seizure; structured questionnaire regarding febrile seizure. Total questions 20. A score
of one is given to each right answer and zero for wrong answer. Total score 20.
Minimum score zero Maximum score is 20. The obtained score was categorized with
the subject experts.
Section III: Checklist to assess the practice of mothers regarding febrile seizure in children. Total
questions 16. The correct answer carries one score and incorrect is zero. The
maximum score is 16 and minimum score is zero.
3.11 SCORING PROCEDURE
The self administered questionnaire consists of 20 questions. In which one mark was
given for correct answer and zero mark for incorrect options. The total score range from 0 -20.
To interpret that level of knowledge the score was distributed as;
38
S.No
Level of knowledge
Score
1.
Inadequate Knowledge
0 -6
2.
Moderate Knowledge
7-13
3.
Adequate Knowledge
14-20
The checklist consists of 16 questions. In that Correct Practice – 1, Incorrect Practice – 0.
S.No
Level of practice
Score
1.
Inadequate Practice
0 -5
2.
Moderate Practice
6-10
3.
Adequate Practice
11-16
3.12 VALIDITY AND RELIABILITY
3.12.1 CONTENT VALIDITY
According to Polit and Beck (2013) validity is a quality criterion referring to the degree
to which inferences made in a study are accurate and well founded in measurement, the degree to
which an instrument measures what it is intended to measure.
Validity is the most important simple methodological criteria for evaluating any
measuring instrument. Four experts from the field of child health Nursing and one expert from
pediatric medicine examined the tool for its relevancy and accuracy. Corrections given by the
experts were incorporated and based on the opinion of the experts, the tool was modified and
used for the main study.
39
3.12.2 RELIABILITY
Reliability reflects how accurately the measures yield the same result on repeated
measures.
( Polit and Hungler 2004).
The karl pearson‘s test and retest method was used to check the reliability of the tool and
it was found to be reliable. The reliability value was part A- [0.8] and part B- [0.9].
3.13 PILOT STUDY
According to Suresh. K. Sharma (2013), Pilot study is the miniature trial run of the
methodology planned for the major research study.
The pilot study was conducted to test the feasibility and reliability of the tool. Pilot study
was conducted among five mothers of under five children who were selected from
Nanjundapuram health center. The knowledge and practices regarding prevention and care of
children with febrile seizure were assessed with the prepared questionnaire. The pilot study
showed that inadequate knowledge and practices regarding prevention and care of children with
febrile seizure.
The sample selected for the pilot study was not considered as samples for the main study.
Based on the pilot study findings the main study was proceeded.
3.14 DATA COLLECTION PROCEDURE
The investigator obtained prior permission from the medical officer in primary health
center, Podanur and consent form was obtained from the samples.
Convenient sampling method was used to select the samples for the main study. The data
collection was done for a period of four weeks. The demographic profile was collected from the
mothers. In pre test, a self administered questionnaire was administered to each sample and
duration of 30 minutes was given. Whenever necessary, items was clarified by the investigator.
Immediately after pretest every sample received educational intervention regarding febrile
seizure. Educational intervention was given for about 45 minutes. The post test was conducted
after one week to assess the effectiveness of teaching in improving the knowledge and practices
regarding febrile seizure by using the same questionnaire.
40
3.15 PLAN FOR DATA ANALYSIS
Demographic variables were analysed by using frequency and percentage distribution.
Knowledge score was analysed by computing frequency, percentage, mean, and
standard deviation.
Effectiveness of educational intervention module was evaluated by paired ‗t‘ test.
Association was done through paired t test.
Correlation was done using the karl pearsons test.
3.16 ETHICAL CONSIDERATIONS
Research was conducted after approval from the higher authorities in Primary health
centre, podanur. Details of the study was informed to the authority of the center and the consent
was obtained from the samples and assurance was given to maintain the confidentiality of the
collected data.
41
a
Research Approach
Dependent variables
(Qualitative research approach)
Research Design
Dependent Variable
(Pre experimental one group pretest and
posttest design)
Knowledge and practice of
mothers regarding febrile seizure
occurring among the children
Research Variables
Independent Variable
Sampling Technique
Educational intervention on
prevention and care of children
with febrile seizure
(Convenient sampling technique)
Sample
(40 Mothers of under five children)
Intervention
Part A (Demographic variables
like Age of the mothers, education,
occupation, religion, type of the
family, family monthly income,
history of maternal seizure, etc.,)
(Educational intervention through the
pamphlet on prevention and care of children
with febrile seizure)
Data collection tool
Part B (Pretest & Posttest self
administered questionnaire on
febrile seizure among mothers of
under five children)
Structured questionnaire
Data Analysis
(Computing, frequency, percentage, mean,
standard deviation, paired ‗t‘ test, chisquare test, correlation)
Part C (Checklist to assess the
practice of mothers regarding
febrile seizure in children)
Interpreting the findings
Writing Report
Fig-3.1 SCHEMATIC REPRESENTATION OF RESEARCH METHODOLOGY
42
CHAPTER – IV
DATA ANALYSIS AND
INTERPRETATION
CHAPTER - IV
DATA ANALYSIS AND INTERPRETATION
A research study is no better that the quality of analysis
-Treece Treece
This chapter deals with the description of the study subjects, classification, analysis and
interpretation of the data collected to evaluate the effectiveness of educational intervention on
febrile seizure among the mothers of under five children attending Primary Health Center
Podanur.
The objectives of the study are,
To assess the existing level of knowledge and practice on febrile seizure among the
mothers of under five children.
To evaluate the effectiveness of educational intervention on febrile seizure among
mothers of under five children.
To associate the pretest knowledge and practice score with selected demographic
variables.
Identify the correlation between posttest knowledge and practice on febrile seizure
among the mothers of under five children.
ORGANIZATION OF FINDINGS
According to the objectives, the collected data is analyzed, organized, tabulated, and
presented under the following headings,
Section-I:
Distribution of socio demographic variables of the samples.
Section-II:
Description of sample, based on the level of knowledge on febrile seizures.
Section-III:
Description of sample, based on the level of practice on febrile seizures.
Section-IV:
Data on effectiveness of educational intervention on knowledge of mothers of
under five children regarding febrile seizure.
43
Section-V:
Data on effectiveness of educational intervention on practice of mothers of
under five children regarding febrile seizure.
Section-VI:
Data on association of pretest level of knowledge of mothers with their
selected demographic variables.
Section-VII:
Data on association of pretest level of practice of mothers with their selected
demographic variables.
Section-VIII:
Data on correlation of posttest knowledge and practice score of mothers of
under five children regarding febrile seizure.
44
SECTION - I
DISTRIBUTION OF SOCIO DEMOGRAPHIC VARIABLES OF THE SAMPLES
Table-4.1: Frequency and percentage distribution of samples with demographic variables
n=40
SL.NO
1.
2.
3.
4.
5.
6.
DEMOGRAPHIC VARIABLES
TOTAL
FREQUENCY
PERCENTAGE
(f)
(%)
Age of the mothers
(a) 20-30
(b) 31-40
(c) 41-50
17
23
0
42.5
57.5
0
Education
(a) Primary
(b) Secondary
(c) Graduate
(d) Illiterate
15
19
6
0
37.5
47.5
15
0
Occupation
(a) Government Job
(b) Private Job
(c) House wife
(d) Coolie
2
11
24
3
5
27.5
60
7.5
Religion
(a) Hindu
(b) Christian
(c) Muslim
(d) Others
15
18
7
0
37.5
45
17.5
0
Type of family
(a) Nuclear family
(b) Joint family
23
17
57.5
42.5
Family monthly income
(a) <Rs.10000/month
(b) Rs.10000-15000/month
(c) Rs.16000-20000/month
(d) Rs.20000 above/month
3
16
17
4
7.5
40
42.5
10
45
7.
8.
9.
10.
11.
12.
13.
History of maternal seizure
(a) Yes
(b) No
0
40
0
100
Previous history of febrile seizure in their
family
(a) Yes
(b) No
11
29
27.5
72.5
Do you think febrile seizure attack is a
life threatening event?
(a) Yes
(b) No
22
18
55
45
Age of the child
(a) Birth to 1year
(b) 1year to 3year
(c) 3years to 5 years
9
12
19
22.5
30
47.5
Does the child has previous history of
febrile seizure
(a) Yes
(b) No
17
23
42.5
57.5
Reason of visit to primary health center?
(a) Immunization
(b) Febrile illness
(c) Others
16
18
6
40
45
15
Do you have thermometer at home?
(a) Yes
(b) No
31
9
77.5
22.5
The data presented in table-4.1 shows that distribution of the samples by demographic variables
Among the samples with regards to age 17(42.5%) were in the age group of 20-30 years,
23(57.5%) were in the age group of 31-40 years.
Regarding educational status 15(37.5%) had of primary level education, 19(47.5%) had
secondary education, 6(15%) were graduates.
Among the samples with regards to occupation 2(5%) were working in government job,
11(27.5%) working in private job, 24(60%) were house wife and 3(7.5%) were coolie.
46
Among the samples with regards to religion 15(37.5%) belongs to hindu, 18(45%)
belongs to Christian and 7(17.5%) belongs to muslim religion.
Regarding the type of family 23(57.5%) of samples were living in nuclear family and
17(42.5%) of samples living in joint family.
With regards to family monthly income 3(7.5%) earns more than Rs.10000/month,
16(40%) earns Rs.10000 -15000/month, 17(42.5%) earns Rs.16000 -20000/month, and
4(10%) earns above Rs.20000/month.
Among the samples there was no history of maternal seizures.
Regarding the previous history of febrile seizure in the family 11(27.5%) had a history
and 29(72.5%) doesn‘t have any history of febrile seizure.
With regards to the samples opinion about febrile seizure as life threatening event
22(55%) said yes and 18(45%) said it is not a life threatening event.
With regards to age of the child 9(22.5%) belongs to age between birth to 1 year,
12(30%) between 1 year-3 years, and 19(47.5%) between 3years-5years.
Among the samples 17(42.5%) responded that the child has a previous history of febrile
seizure and 23(57.5%) said there was no history of febrile seizure.
With regards to the reason of visit to primary health center 16(40%) came for
immunization, 18(45%) for the treatment of febrile illness, and 6(15%) came for other
reasons.
Among the samples 31(77.5%) had thermometer at home and 9(22.5%) doesn‘t possess a
thermometer at home.
47
100
90
0
80
70
57.50%
60
50
PERCENTAGE
42.50%
40
20 - 30 YEARS
30
31 - 40 YEARS
41 - 50 YEARS
20
10
0%
0
20 - 30 YEARS
31 - 40 YEARS
41 - 50 YEARS
AGE
Fig-4.1:
A bar diagram showing the percent age distribution of sample in term of
their age of the mothers
48
15%
37.5%,
PRIMARY
SECONDARY
GRADUATE
ILLITERATE
47.5%
Educational Status
Fig-4.2: A pie diagram showing the percentage distribution of sample in terms of their
educational status
49
100
90
0
80
70
60
50
PERCENTAGE
40
GOVERNMENT JOB
60%
30
PRIVATE JOB
HOUSE WIFE
COOLIE
20
27.5%
10
5%
7.5%
0
GOVERNMENT
JOB
PRIVATE JOB
HOUSE WIFE
COOLIE
OCCUPATION
Fig-4.3: A conical diagram depicting the percentage distribution of samples in terms of
their occupation.
50
100
90
72.5%
0
80
70
PERCENTAGE
60
50
27.5%
YES
40
NO
30
20
10
0
YES
NO
PREVIOUS FAMILY HISTORY OF FEBRILE SEIZURE
Fig-4.4: A cylindrical diagram showing the percentage distribution of sample in terms of
their family history of febrile seizure
51
42.50%
YES
NO
57.50%
PREVIOUS HISTORY OF FEBRILE SEIZURE
Fig-4.5: A doughnut diagram showing the percentage distribution of the sample in terms of
their child has previous history of febrile seizure
52
15%
40%
IMMUNIZATION
FEBRILE ILLNESS
OTHERS
45%
REASON OF VISIT TO PRIMARY HEALTH CENTRE
Fig-4.6: A pie diagram showing the percentage distribution of the sample in terms of visit
to primary health center
53
100
90
80
77.5%
70
PERCENTAGE
60
50
YES
40
NO
30
22.5%
20
10
0
0
0.5
YES
1
1.5
NO
2
2.5
THERMOMETER AT HOME
Fig-4.7: A bubble diagram showing the percentage distribution of the sample in terms of
having thermometer at home
54
SECTION -II
DATA ON DISTRIBUTION OF SAMPLES, BASED ON THE LEVEL OF
KNOWLEDGE IN PRETEST AND POSTTEST
Table-4.2: Distribution of the samples according to their level of knowledge in pretest and
post test
n=40
PRE TEST
POST TEST
LEVEL OF
KNOWLEDGE FREQUENCY PERCENTAGE FREQUENCY PERCENTAGE
(f)
(%)
(f)
(%)
Inadequate
0-6
Moderate
7 - 13
Adequate
14 - 20
0
0
0
0
36
90
1
2.5
4
10
39
97.5
The data presented on the table shows that among 40 mothers of under five children,
36(90%) had moderate knowledge, 4(10%) had adequate knowledge in the pretest. The level
of knowledge was improved after intervention and in the post test 1(2.5%) had moderate
knowledge and 39(97.5%) had adequate knowledge.
55
97.5%
100
90%
90
80
PERCENTAGE
70
60
50
PRETEST
40
POSTTEST
30
20
10
10%
0%
0%
2.5%
0
INADEQUATE
MODERATE
ADEQUATE
LEVEL OF KNOWLEDGE
Fig-4.8: A cylindrical diagram showing the percentage distribution of sample in terms of
their pretest and posttest level of knowledge score
56
SECTION -III
DATA ON DISTRIBUTION ACCORDING TO THE SAMPLES, LEVEL OF PRACTICE
IN PRETEST AND POSTTEST
Table-4.3: Distribution of the samples according to their level of practice in pretest and
post test
n=40
PRE TEST
POST TEST
LEVEL OF
FREQUENCY PERCENTAGE FREQUENCY PERCENTAGE
PRACTICE
(f)
(%)
(f)
(%)
Inadequate
0-5
Moderate
6 - 10
Adequate
11 - 16
2
5
0
0
28
70
3
7.5
10
25
37
92.5
The data presented on the table shows that among the 40 mothers of under five
children, 2 (5%) had inadequate practice, 28 (70%) had moderate practice, 10 (25%) had
adequate practice in pre test. The level of practice improved after the intervention and in the
post test 3 (7.5%) had moderate practice and 37 (92.5%) had adequate practice.
57
100
92.5%
90
80
70%
PERCENTAGE
70
60
50
PRETEST
40
POSTTEST
30
25%
20
10
7.5%
5%
0%
0
INADEQUATE
MODERATE
ADEQUATE
LEVEL OF PRACTICE
Fig-4.9: A bar diagram showing the percentage distribution of sample in terms of their
pretest and posttest level of practice score
58
SECTION -IV
DATA ON EFFECTIVENESS OF EDUCATIONAL INTERVENTION ON
KNOWLEDGE REGARDING FEBRILE SEIZURE AMONG THE MOTHERS
Table-4.4: Mean, Mean difference, Standard deviation and „t‟ value of pretest and
posttest level of knowledge among samples
(n= 40)
Variables
Test
Mean
Pre test
10.60
Mean
Standard
Paired „t‟
Difference
Deviation
Test Value
2.340
Knowledge
5.75
Post test
16.35
24.01**
1.388
**Significant at p<0.05 level
The data presented on the table 4.4 revealed that, the pretest knowledge score
mean was 10.6 and posttest mean was 16.3, So mean difference 5.75 was a true
difference. The standard deviation of pretest was 2.340 and posttest was 1.388.
The calculated paired ‗t‘ value was 24.01 was highly significant than the table
value (2.05) at 0.05 level. Hence the stated hypothesis was accepted.
It was inferred that educational intervention on prevention and care of febrile
seizure was effective in improving the knowledge of the mothers of under five
children.
59
SECTION – V
DATA ON EFFECTIVENESS OF EDUCATIONAL INTERVENTION ON
PRACTICE AMONG MOTHERS OF UNDER FIVE CHILDREN IN TERMS
OF CARE DURING FEBRILE SEIZURE
Table-4.5: Mean, Mean difference, Standard deviation and „t‟ value of pretest
and posttest level of practice among samples
(n=40)
Variable
Test
Mean
Pre test
9.10
Mean
Difference
Standard
Deviation
2.08
3.67
Practice
Post test
„t‟ Value
18.933**
1.44
12.77
**Significant at p<0.005
The data presented on the table 4.5 revealed that, the pretest practice score mean was
9.10 and posttest mean was 12.77, So mean difference 3.67 was a true difference. The standard
deviation of pretest was 2.08 and posttest was 1.44.
The calculated paired ‗t‘ value 18.933 was highly significant than the table value
(2.05) at 0.05 level. Hence the stated hypothesis was accepted.
It was inferred that educational intervention on prevention and care during febrile
seizure was effective in improving the practice of the mothers of under five children.
60
SECTION – VI
DATA ON ASSOCIATION OF THE PRETEST KNOWLEDGE LEVEL OF
MOTHERS WITH SELECTED DEMOGRAPHIC VARIABLES
Table-4.6: Association of the pretest knowledge score with the selected demographic
variables
(n=40)
LEVEL OF
KNOWLEDGE
S.NO
1.
2.
3.
DEMOGRAPHIC
VARIABLES
Above
Mean
Below
Mean
Primary
7
8
Secondary
9
10
Graduate
4
2
Illiterate
0
0
Government job
1
1
Private job
6
5
House wife
12
12
Coolie
1
2
8
3
12
17
CHI -SQUARE
TABLE VALUE
0.786#
5.99
Education
Df=2
Occupation
0.424#
7.81
Df=3
Previous history of
febrile seizure in
their family
Yes
No
61
3.135#
3.84
Df=1
4.
Child has
previous history
of febrile seizure
Yes
No
5.
10
7
9
14
5
11
8
10
6
0
1.520#
3.84
Df=1
Reason of visit to
primary health
center
Immunization
Febrile illness
Others
8.393*
5.99
Df=2
NOTE: # Not significant at 0.05 level
* Significant at 0.05 level
Table: 4.6 revealed that, chi square analyzes was done to find out the association
between the pretest knowledge score with the selected demographic variables. The findings
revealed that the pretest knowledge score is associated with the reason of visit to primary
health centre.
62
SECTION - VII
DATA ON ASSOCIATION OF THE PRETEST PRACTICE LEVEL OF MOTHERS
WITH SELECTED DEMOGRAPHIC VARIABLES
Table-4.7: Association of the pretest practice score with the selected demographic
variables
(n=40)
S.NO
1.
2.
3.
4.
DEMOGRAPHIC
VARIABLES
LEVEL OF
PRACTICE
Below
Above
Mean
Mean
CHI -SQUARE
TABLE VALUE
2.924#
5.99
Df=2
0.195#
7.81
Df=3
Education
Primary
Secondary
Graduate
Illiterate
4
8
4
0
11
11
2
0
Occupation
Government job
Private job
House wife
Coolie
1
5
10
1
1
6
14
2
Previous history
of febrile seizure
in their family
Yes
No
7
10
4
19
2.774#
3.84
Df=1
Child has
previous history
of febrile seizure
Yes
No
7
11
10
12
0.175#
3.84
Df=1
63
5.
Reason of visit to
primary health
center
Immunization
Febrile illness
Others
5
7
5
11
11
1
5.018#
5.99
Df=2
NOTE: # Not significant at 0.05 level
Table: 4.7 revealed that, chi square analyzes was done to find out the association between
the pretest practice score with the selected demographic variables. The findings revealed that
there was no association between the pretest practice score with the selected demographic
variables.
64
SECTION - VIII
DATA ON CORRELATION OF POSTTEST KNOWLEDGE AND POSTTEST
PRACTICE LEVEL OF MOTHERS OF UNDER FIVE CHILDREN
Table-4.8: Correlation between post test knowledge and post test practice of mothers
regarding febrile seizure.
S.No
Variables
Mean
Standard
Deviation
1
Knowledge
16.3
1.38
Correlation (r)
0.464**
2
Practice
12.7
1.44
**Significant at P< 0.05
Table 4.8 revealed that there is a positive correlation between the post test knowledge and
post test practice score.
65
CHAPTER – V
FINDINGS AND DISCUSSION
CHAPTER – V
FINDINGS AND DISCUSSION
The present study was an effort to evaluate the effectiveness of educational intervention
on febrile seizure among the mothers of under five children At Primary Health Center Podanur.
The self administered questionnaire was used to evaluate the effectiveness of educational
intervention on febrile seizure. The sample size were 40 mothers of under five children. The
investigator adopted pre experimental one group of pretest and posttest design. The data
collected for the study were analyzed statistically and discussed below based on the objectives.
The first objective of the study was to assess the existing level of knowledge and practice on
febrile seizure among the mothers of under five children
The study shows that among 40 mothers of under five children, 36(90%) had moderate
knowledge, 4(10%) had adequate knowledge in the pretest. The level of knowledge was
improved after intervention and in the post test 1(2.5%) had moderate knowledge and 39(97.5%)
had adequate knowledge. The pretest and posttest knowledge mean score was 10.6 and 16.3.
The study shows that among the 40 mothers of under five children, 2 (5%) had
inadequate practice, 28 (70%) had moderate practice, 10 (25%) had adequate practice in pre test.
The level of practice improved after the intervention and in the post test 3 (7.5%) had moderate
practice and 37 (92.5%) had adequate practice. The pretest and posttest practice mean score was
9.10 and 12.77.
The second objective of the study was to evaluate the effectiveness of educational
intervention on febrile seizure among mothers of under five children
Paired ‗t‘ test was used to compare the pretest and posttest knowledge and practice scores
the ‗t‘ value is 24.01 which is significant at p<0.05 level for knowledge and 18.933 which is
significant at p< 0.05 level for practice. It means that there is a significant difference in the
knowledge and practice of mothers among prevention and care of febrile seizure before and after
the educational intervention.
66
The third objective of the study was to associate the pretest knowledge and practice
score with selected demographic variables
The chi square analyses was done to find out the association between the pretest
knowledge score with the selected demographic variables like education, occupation,
previous family history of febrile seizure, child has previous history of febrile seizure, reason
of visit to primary health center. The findings revealed that the pretest knowledge score is
associated with the reason of visit to primary health centre and χ2value was 8.393 which is
significant at level of p<0.05.
The chi square analyses was done to find out the association between the pretest practice
score with the selected demographic variables. The findings revealed that there is no
association between the pretest practice score with the selected demographic variables.
The fourth objective of the study was to identify the Correlation between posttest
knowledge and practice on febrile seizure among the mothers of under five children
Karl Pearson‘s correlation indicates that there is a positive correlation (r = 0.464)
between the posttest knowledge and practice scores which reveals that the knowledge
significantly influence the practice of mother regarding prevention and care of child with
febrile seizures.
67
CHAPTER – VI
SUMMARY AND CONCLUSION
CHAPTER – VI
SUMMARY, CONCLUSION AND RECOMMENDATION
This chapter deals with summary, conclusion, and implication, limitation and
recommendations. The essence project is based on the study findings, limitation, interpretation of
the research and recommendation that cooperate in the study implications. It also gives meaning
to the result obtained in the study. Further it includes implications for the nursing practice,
nursing education, nursing administration and nursing research.
6.1 SUMMARY
The present study was done to evaluate the effectiveness of educational intervention in
improving the knowledge regarding febrile seizure among the mothers of under five children.
6.2 OBJECTIVES
To assess the existing level of knowledge and practice on febrile seizure among the
mothers of under five children.
To evaluate the effectiveness of educational intervention on febrile seizure among
mothers of under five children.
To associate the pretest knowledge and practice score with selected demographic
variables.
To identify the correlation between post test knowledge and practice on febrile seizure
among the mothers of under five children.
The selection of research design is an important and essential step in research. Pre
experimental one group pretest and post test design was chosen for this study. Convenient
sampling techniques was used in this study, the sample consisted of 40 mothers of under five
children who visited Primary Health Center, Podanur and fit into inclusion criteria.
The prepared tool and educational intervention was validated by nursing experts of
various specialties based on the suggestions the tool was modified and used for the main
study. The research tool consist of
68
Part A:
Demographic variables like age, education, occupation, religion, type of family,
family monthly income, history of maternal seizure, previous history of febrile
seizure in their family, febrile seizure attack is a life threatening event, age of the
child, child has previous history of febrile seizure, reason of visit to primary
health center, having thermometer at home.
Part B:
Knowledge related self administered questionnaire on febrile seizure among the
mothers of under five children.
Part C:
Checklist to assess the practice of mothers regarding febrile seizure in children.
Part D:
Educational intervention on knowledge regarding febrile seizure among the
mothers of under five children.
Data was analyzed and interpreted. Demographic variables was analyzed by using
frequency and percentage distribution. Knowledge was analyzed by computing frequency,
percentage, mean, median and standard deviation. The effectiveness of educational
intervention module was evaluated by paired ‗t‘ test. Association between the pretest level of
knowledge and pretest practice score with the selected demographic variables was analyzed
by chi-square test. Correlation between posttest knowledge and posttest practice level of
mothers of under five children regarding febrile seizure.
6.3 MAJOR FINDINGS
Among the samples with regards to age 17(42.5%) were in the age group of 20-30 years,
23(57.5%) were in the age group of 31-40 years.
Regarding educational status 15(37.5%) had of primary level education, 19(47.5%) had
secondary education, 6(15%) were graduates.
Among the samples with regards to occupation 2(5%) were working in government job,
11(27.5%) working in private job, 24(60%) were house wife and 3(7.5%) were coolie.
Among the samples with regards to religion 15(37.5%) belongs to hindu, 18(45%)
belongs to Christian and 7(17.5%) belongs to muslim religion.
Regarding the type of family 23(57.5%) of samples were living in nuclear family and
17(42.5%) of samples living in joint family.
69
With regards to family monthly income 3(7.5%) earns more than Rs.10000/month,
16(40%) earns Rs.10000 -15000/month, 17(42.5%) earns Rs.16000 -20000/month, and
4(10%) earns above Rs.20000/month.
Among the samples there was no history of maternal seizures.
Regarding the previous history of febrile seizure in the family 11(27.5%) had a history
and 29(72.5%) doesn‘t have any history of febrile seizure.
With regards to the samples opinion about febrile seizure as life threatening event
22(55%) said yes and 18(45%) said it is not a life threatening event.
With regards to age of the child 9(22.5%) belongs to age between birth to 1 year,
12(30%) between 1 year-3 years, and 19(47.5%) between 3years-5years.
Among the samples 17(42.5%) responded that the child has a previous history of febrile
seizure and 23(57.5%) said there was no history of febrile seizure.
With regards to the reason of visit to primary health center 16(40%) came for
immunization, 18(45%) for the treatment of febrile illness, and 6(15%) came for other
reasons.
Among the samples 31(77.5%) had thermometer at home and 9(22.5%) doesn‘t possess a
thermometer at home.
The findings shows that among 40 mothers of under five children, 36(90%) had moderate
knowledge, 4(10%) had adequate knowledge in the pretest. The level of knowledge was
improved after intervention and in the post test 1(2.5%) had moderate knowledge and
39(97.5%) had adequate knowledge.
The findings shows that among the 40 mothers of under five children, 2 (5%) had
inadequate practice, 28 (70%) had moderate practice, 10 (25%) had adequate practice in
pre test. The level of practice improved after the intervention and in the post test 3 (7.5%)
had moderate practice and 37 (92.5%) had adequate practice.
The findings revealed that, the pretest knowledge score mean was 10.6 and post test mean
was 16.3, So mean difference 5.75 was a true difference. The standard deviation of
pretest was 2.340 and posttest was 1.388. The calculation paired ‗t‘ value was 24.01 was
highly significant than the table value (2.05) at 0.05 level. Hence the stated hypothesis
was accepted.
70
The findings revealed that, the pretest practice score mean was 9.10 and post test mean
was 12.77, So mean difference 3.67 was a true difference. The standard deviation of
pretest was 2.08 and posttest was 1.44. The calculation paired ‗t‘ value 18.933 was highly
significant than the table value (2.05) at 0.05 level. Hence the stated hypothesis was
accepted.
The findings done by chi square test to find out the association between the pretest
knowledge score with the selected demographic variables revealed that the pretest
knowledge score is associated with the reason of visit to primary health centre and
χ2value was 8.393 which is significant at level of p<0.05.
The findings revealed by, chi square analyzes to find out the association between the
pretest practice score with the selected demographic variables. The findings revealed that
there was no association between the pretest practice score with the selected demographic
variables.
The findings revealed that there is a positive correlation between the post test knowledge
and post test practice score.
6.4 CONCLUSION
The following conclusion was drawn from the study. The study proved that educational
intervention on febrile seizure was effectiveness in improving the knowledge and practices of the
mothers of under five children. The study findings reveled that knowledge and practice was
significantly improved by educational intervention on febrile seizure.
6.5 IMPLICATION
The present study findings have several implication in nursing practice, nursing education,
nursing administration and nursing research.
6.5.1 NURSING PRACTICE
Nurses can carry out health education programme to care takers of children to provide
knowledge on prevention and care during febrile seizure.
Nurses can demonstrate the correct practice of prevention and care of febrile seizure to
the mothers of under five children as part of their conventional counseling.
71
Mass health education campaigns should be organized regularly by health team to
provide education towards febrile seizure and clear the doubts regarding management and
them to practice it.
The present study result can be used to improve the mothers knowledge and practice of
prevention and care of febrile seizure.
6.5.2 NURSING EDUCATION
The nurse educator can use the educational intervention to teach nursing students and
other staff members.
The findings of the study indicate that more emphasis should be placed in the curriculam
for prevention and care of febrile seizure.
6.5.3 NURSING ADMINISTRATION
Nurse administration can disseminate the research knowledge to the nurse working in the
primary health center.
Nurse administration can formulate protocol incorporate the study findings in nursing
intervention.
Educational intervention can be used to orient new nurses who handle pediatric clients.
6.5.4 NURSING RESEARCH
This study provides a basis for further studies.
The findings of the study serves as a basis for the professional and student nurses to
conduct further studies regarding care and prevention of the child with febrile seizure.
6.6 LIMITATION
The study was conducted on a small representative group.
The researcher could not use randomized sampling techniques in this study.
6.7 RECOMMENDATION
A similar study can be conducted with large number of samples.
A study can be conducted at different settings.
A comparative study can be conducted between rural and urban mothers of under five
children.
Similar study can be undertaken by descriptive study.
An experimental study can be undertaken with control group for effective comparison.
72
References
REFERENCES
BOOKS
Adelepillitteri (2007) ― Maternal and child health‖, 5th edition, Lippincott Williams and
Wilkins publishers.
B.T.Basavanthapa (2007) ―Nursing Research‖ 7th edition Lippincott Williams and
Wilkins publishers.
Dorothy R. Marlow and Barbara A.Redding.Textbook of pediatric nursing. New
Delhi, Elsevier‘s publication.
Denis.F. Polit (2009) ―Nursing Research‖ 2nd edition Jaypee Brothers Medical
publishers.
Hockenbery Wilson. Wong‟s nursing care of infants and children. Missouri, Elseviers
publication.
Jefferies,A.L.,october
2016.Going
home:facilitating
discharge
of
the
preterm
infant'.paediatric child health.
Nicki.L.Potts (2007) ―Pediatric Nursing caring for children and their families‖ 2nd
edition, Sanat printing publishers.
Nelson ―text book of pediatrics, 20th edition.
O.P.Ghai. Essential pediatrics. Delhi; Published by Dr. Ghai.
Piyush gupta (2004) ―The essential peadiatrics nursing‖, 1st edition, new delhi A-P.
jainand co publications.
Paruldutta (2010) ―Pediatric Nursing‖, 2nd edition, Jaypee brothers medical publishers.
Parthasarathy.A ―Textbook of pediatrics‖, 7th edition.
Suraj gupta (2005) ―Textbook of paediatrics‖ 7th edition, jaypee brothers.
73
JOURNALS
Anup D. Patel, MD; M. Scott Perry, MD; Febrile Seizures: Evaluation and Treatment,
Journal of Clinical Outcomes Management (2017).
Vaswani RK, Dharaskar PG, Kulkarni S, Ghosh K. Iron deficiency as a risk factor for
first febrile seizure. Indian Pediatrics. (2010)
Millichap JG, et al. Treatment and prognosis of febrile seizures. American Academy of
Pediatrics (2017)
Albarraq,A.A., january ,2014. Knowledge and attitude on chilidhood febrile seizure a
survey among Saudi parents in Taif Region.Saudi Arabia pharmacy practice and drug
research.
Batool Karimi 1,*; Melika Zarei Sani 1; Raheb Ghorbani 1; Navid Danai,, 2013. The
Mothers' Knowledge About febrile seizure in Semna Iran.
Karsten Lunze1,2,3*, Kojo Yeboah-Antwi2,3, David R. Marsh4, Sarah Ngolofwana
Kafwanda5, Austen Musso3, Katherine Semrau2,3, Karen Z. Waltensperger4 ,
Davidson H. Hamer1, 2012. Prevention and Management of Febrile Seizure in Rural
Zambia.
Maryam Bagheri1, Mahin Tafazoli2, Zahra Sohrabi3*,, 2016. Effect of Education on
the Awareness of Febrile Seizure Care)).
Onalo, R., 2013. Febrile Seizure in sub-Saharan Africa: A review.
Solomon , Nigatu, AG Worku, AF Dadi - BMC, 2015. Level of mother's knowledge
about febrile seizure danger signs and associated factors in North West of Ethiopia.
Solomons, N. and Rosant, C. , 2012. Knowledge and attitudes of nurse staff and
mothers towards febrile seizure care in the eastern sub-district of Cape Town..
Vijayalakshmi, T Susheela, 2015. Knowledge, attitudes, and febrile seizure management
practices of mothers: A cross sectional survey. International journal.
74
WEBSITE
http://www.pediatricneurosciences.com
http://www.hindawt.com
http://indianpediatrics.net
http://www.pubmed.ncbi.nlm.nih.gov
http://www.ljpediatrics.com
http://www.ninds.nih.gov/disorders/febrile_seizures
https://www.uptodate.com/contents/search
https://www.healthychildren.org/English/health-issues/conditions/Febrile-Seizures
http://www.ncbi.nlm.nih.gov
http://www.annalsofian.org
http://www.bmcpediatr.biomedcentral.com
http://www.nhsinform.scot/febrileseizure
http://www.msdmanual.pediatrics.com
75
appendices
APPENDIX - I
SIGNATURE OF THE PRINCIPAL
SIGNATURE OF THE GUIDE
APPENDIX - II
APPENDIX – III
LETTER REQUESTING EXPERT OPINION FOR ESTABLISH
CONTENT VALIDITY
To,
Coimbatore.
(Through – Principal Texcity College of Nursing)
Respected sir/madam,
SUB: Nursing Education – M.Sc.(N) II year – Content Validity Req. – Reg.
I wish to state that I am M.Sc.(N) II year student of Texcity College of Nursing has to
carry out a research project. This is to be submitted to the TN DR. MGR Medical University,
Chennai in partial fulfilment for the requirement for the award of Master of Science in Nursing.
The topic of research project is :
To evaluate the effectiveness of educational intervention on febrile seizures among
mothers of under five children at primary health center Podanur.
I have enclosed,
1. Statement of the problem, objectives, hypothesis and conceptual framework
2. Research tool
3. Teaching module
I request you to go through the items and give your valuable suggestions, modifications,
additions and deletions, if any, in the remark column.
Thanking you,
Place : Coimbatore
Yours faithfully,
Date :
Mrs.A.S.Arun Subini
APPENDIX-IV
LIST OF EXPERTS
1. Mrs.Mallikai Selvaraj
Developmental Paediatrician,
Royal Care Super Speciality Hospital,
Coimbatore.
2. Mrs.Muthumaheswari,
Professor,
SCPM College of Nursing,
Uttar Pradesh.
3. Mrs. C. Valarmaathy,
Professor,
KG College Of Nursing,
Coimbatore.
4. Mrs.Blanshie Rajila William,
Associate professor,
KG College Of Nursing,
Coimbatore.
5. Mrs. Nisha Rachel.C,
Assistant professor,
Westfort College Of Nursing,
Thirussur.
APPENDIX-V
EVALUATION CRITERIA CHECK LIST FOR CONTENT VALIDITY TOOL
INSTRUCTION:
Expert is requested to go through the following evaluation criteria check list prepared for
the intervention there are columns given for the response and facilitate in the remarks column
given.
RESEARCH TOOLS
RELEVANT
IRRELEVANT
REMARKS
Section: A
Demographic Variables
1 – 13
ANY OTHER SUGGETIONS:
EXPERT SIGNATURE WITH DATE AND SEAL
APPENDIX - VI
EVALUATION CRITERIA CHECK LIST FOR CONTENT VALIDITY TOOL
INSTRUCTION:
Expert is requested to go through the following evaluation criteria check list prepared for
the intervention there are columns given for the response and facilitate in the remarks column
given.
RESEARCH TOOLS
RELEVANT
IRRELEVANT
REMARKS
Section: B
Self Administered
Questionnaire
1- 20
Section: C
Checklist to assess the
practice of mothers
regarding febrile seizure
in children
1 - 16
ANY OTHER SUGGETIONS:
EXPERT SIGNATURE WITH DATE AND SEAL
APPENDIX - VII
EVALUATION CRITERIA CHECK LIST FOR CONTENT
VALIDITY- EDUCATIONAL INTERVENTION MODULE
INSTRUCTION:
Expert is requested to go through the following evaluation criteria check list prepared for the
intervention, there are three columns given for the response and facilitate suggestion in the
remarks column given.
CRITERIA
REMARKS
S.NO
CONTENT
MEET PARTIALLY DOES
MEET
NOT
I
SELECTION OF
CONTENT
a. Content reflect the objectives
b. Content has update knowledge
c. Content is comprehensive for
the learning needs
d. Content provides correct and
accurate information
e. Content coverage
II
ORGANIZATION OF
CONTENT
a. Logical sequence
b. Continuity
c. Integration
III LANGUAGE
a. English language is used to
simple and comprehensive
b. Technical terms are explained
at the level of learners ability
IV FEASIBILITY /
PRACTICABILITY
a. Is suitable to subjects
b. Permit self- learning
c. Acceptable and useful to the
students
d.
Suitable for setting
ANY OTHER SUGGESTIONS:
EXPERT SIGNATURE WITH DATE AND SEAL
APPENDIX - VIII
LETTER SEEKING CONSENT OF SUBJECTS FOR
PARTICIPATION ON THIS STUDY
INTRODUCTION
I would like to inform you that I’m doing ―To evaluate the effectiveness of educational
intervention on febrile seizure among mothers of under five children at primary health center
podanur, Coimbatore‖.
Your kind cooperation is highly esteemed and your honest responses are valuable. If you
are willing to participate in this study, please sign the content from given below.
Yours truly
CONSENT FORM
I understood whatever you explained and I am accepting to participate in your study with
my full cooperation.
I am declaring this with my full conscious and clear knowledge and the above.
Thanking you,
Signature of the sample
Date :
Place:
APPENDIX- IX
CERTIFICATE FOR ENGLISH EDITING
TO WHOM SO EVER IT MAY CONCERN
This is to certify that the tool developed by Mrs.Arun Subini A.S, M.Sc Nursing Student
of Texcity College of Nursing for dissertation “To evaluate the effectiveness of educational
intervention on febrile seizure among mothers of under five children at primary health
center Podanur, Coimbatore.” is edited for English language appropriateness by
Mrs. D. Muthumalni Alice, M.A (English)., B.Ed. Texcity College of Nursing Coimbatore.
SIGNATURE
APPENDIX- X
RESEARCH TOOL
SECTION - A
DEMOGRAPHIC DATA OF MOTHER
Instruction: (Read following questions carefully and place a tick mark in the
appropriate space provided at each time)
Sample Number:(n=40)
1. Age of the mothers
a) 20-30
b) 31-40
c) 41-50
2. Education
a) Primary
b) Secondary
c) Graduate
d) Illiterate
3. Occupation
a) Government Job
b) Private Job
c) House wife
d) Coolie
4. Religion
a) Hindu
b) Christian
c) Muslim
d) Others
5. Type of family
a) Nuclear family
b) Joint family
6. Family monthly income
a) < Rs.10000 / month
b) Rs.10000 – 15000
c) Rs.16000- 20000
d) Rs. 20000 and above
7. History of maternal seizure?
a) Yes
b) No
8. Previous history of febrile seizure in their family?
a) Yes
b) No
9. Do you think febrile seizure attack is a life threatening event?
a) Yes
b) No
10. Age of the child
a) At birth to 1 year
b) 1 year to 3 year
c) 3 years to 5 years
11. Does the child has previous history of febrile seizure?
a) Yes
b) No
12. Reason of visit to primary health center?
a) Immunization
b) Febrile illness
c) Others
13. Do you have thermometer at home?
a) Yes
b) No
SECTION B
SELF ADMINISTERED QUESTIONNAIRE
Instruction: (Read the following questions and tick any one option)
1. What is meant by febrile?
a) Seizure
b) Cyanosis
c) Fever
2. What is febrile seizure?
a) It is a communicable disease
b) A seizure occurring in young children with a fever
c) It is a mental illness
3. What are the causes of febrile seizure?
a) Viral and Bacterial Infection
b) Indigestion
c) Diarrhoea
4. Which age group of children is more prone for febrile seizure?
a) 5-10 years
b) Above 10 years
c) 3months -5 years
5. What are the types of febrile seizure?
a) Primary or secondary
b) Simple and complex
c) High and low grade
6. What is the warning sign of febrile seizure attack?
a) Headache
b) Visual disturbances
c) Fever above 100.4˚F
7. What are the changes in the eyes during febrile seizure?
a) Up rolling of eyes
b) Shrunken eyes
c) Closed eyes
8. What would be the conscious level during febrile seizure?
a) Alert and conscious
b) Semi conscious
c) Loss of conscious
9. What are the changes in the skin during febrile seizure?
a) Rashes
b) Bluish discoloration of the skin
c) Erythema
10. What are the changes in the extremities during febrile seizure?
a) Jerking movements
b) Deviation of angles hands and legs
c) Shivering
11. What is immediate observation made during febrile seizure?
a) Color of the child
b) Body Temperature
c) Watch for nearby sharp objects
12. What are the changes in the excretory system during febrile seizure?
a) Involuntry pass urine
b) Urinary incontinence
c) Anuria
13. What are the changes occur in the breathing pattern during febrile seizure?
a) Increase breathing
b) No breathing
c) Irregular breathing
14. What is the most common complication when the febrile seizure lasts for more than 30
minutes?
a) Status epilepticus
b) Brain damage
c) Cerebro vascular accident
15. What is the consequency of recurrent febrile seizure?
a) Brain damage
b) Meningitis
c) Mental retardation
16. Why we should loosen the clothing around the head and neck during the febrile seizure
attack?
a) Easy to give sponge bath
b) To prevent chocking
c) To stimulate the child
17. How to position a child after an episode of febrile seizure?
a)
Supine
b)
Prone
c)
Side lying, turn child head to the side and the face downward
18. What is the diagnostic test available to rule out febrile seizure?
a) Electro Cardio Gram
b) Electro Encephalo Gram
c) Echo Cardio Gram
19. What is the complication of recurrent episodes of febrile seizure?
a) Dysarhtria
b) Delayed vocabulary development
c) Dyslalia
20. When should the parent call for emergency help?
a) Seizure more than 30 minutes, trouble breathing chocking
b) Temperature above 100.4˚f
c) The child going pale color
SCORING KEY
SELF ADMINISTERED QUESTIONNAIRE
Question number
Answer
Question number
Answer
1
c
11
c
2
b
12
a
3
a
13
c
4
c
14
a
5
b
15
a
6
c
16
b
7
a
17
c
8
c
18
b
9
b
19
b
10
a
20
a
S.No
Level of knowledge
Score
1.
Inadequate Knowledge
0 -6
2.
Moderate Knowledge
7-13
3.
Adequate Knowledge
14-20
SECTION - C
CHECKLIST TO ASSESS THE PRACTICE OF MOTHERS REGARDING FEBRILE
SEIZURE IN CHILDREN
Instruction: (Read the following questions and mark any one option)
S.No
Questions
1.
Lower the child body temperature
2.
Protect the child on a soft and safe surface
3.
Place the child on his/her side
4.
Keep calm
5.
Observe febrile seizure manifestation and duration
6.
Remove any nearby objects
7.
Place your child on the floor
8.
Loosen any clothing around the head and neck
9.
Rush the child to a doctor
10.
Shake and rouse the convulsing child
11.
Attempt mouth-to-mouth resuscitation
12.
Pry the convulsing child’s clenched teeth apart and put something in
his / her mouth
13.
Suck discharge from the child’s nose and mouth
14.
Cardiac massage
15.
Restrain the convulsing child
16.
Stimulating the child immediately after febrile seizure
Yes No
OBSERVATIONAL CHECKLIST
Question Number
Answer
Score
1
Yes
1
2
Yes
1
3
Yes
1
4
Yes
1
5
Yes
1
6
Yes
1
7
Yes
1
8
Yes
1
9
No
1
10
No
1
11
No
1
12
No
1
13
No
1
14
No
1
15
No
1
16
No
1
S.No
Level of practice
Score
1.
Inadequate Practice
0 -5
2.
Moderate Practice
6-10
3.
Adequate Practice
11-16
ிரிவு – அ
குிப்பு:-{ின்யரும்
முளமம்
கேள்யிேள
யமங்ேப்ட்ட
ேயநாேப்
வாருத்தநா
டித்து,
இடத்தில்
ஒரு
ஒவ்வயாரு
(√
)
குி
ளயக்ேவும்}
1.
தானின் யனது
அ) 20 - 30
ஆ) 31 – 40
இ) 41 – 50
2.
ேல்யி தகுதி
அ) ஆபம்க்ேல்யி கற்யர்
ஆ) உனர் ில கல்யி கற்யர்
இ) ட்டதாரி
ஈ) டிக்ோதயர்
3.
கயள தகுதி
அ) அபசு வயல
ஆ) தினார் வயல
இ) இல்த்தபசி
ஈ) கூி வதாமிாி
4. நதம்
அ) இந்து
ஆ) கிிஸ்தயர்
இ) இஸ்ாநினர்
ஈ) ி நதத்தயர்
நாதிரி ண்:...............
5. குடும்த்தின் யலக
அ) திக்குடும்ம்
ஆ) கூட்டுக்குடும்ம்
6. குடும்த்தின் நாத யமநாம்
அ) < Rs. 10000/ஆ) Rs.10000 – 15000/இ) Rs.16000 – 20000/ஈ) >Rs. 20000/7.
ேற் ோ யிப்பு யபாறு உள்தா?
அ) ஆம்
ஆ) இல்ல
8.
குடும்த்தில் காய்ச்சல் யிப்பு தாக்ேத்தின் முந்ளதன யபாறு உள்தா?
அ) ஆம்
ஆ) இல்ல
9.
காய்ச்சல் யிப்பு தாக்குதல்
உனிமக்கு ஆத்தா ிகழ்வு ன்று ீ ங்கள்
ிலக்கிீர்கா?
அ) ஆம்
ஆ) இல்ல
10. குமந்லதனின் யனது?
அ) ிப்பு முதல் 1யனது யளப
ஆ) 1யனது முதல் 3யனது யளப
இ) 3யனது முதல் 5யனது யளப
11.
குமந்லதக்கு காய்ச்சல் யிப்புதாக்கத்தின் முந்லதன யபாறு
இருக்ேிதா?
அ) ஆம்
ஆ) இல்ல
12. ஆபம் சுகாதாப லநனத்திற்கு யந்ததற்ோ ோபணம்?
அ) வாய்த்தடுப்பு ஊசி
ஆ) காய்ச்சல்
இ) நற் உடல் குளப்ாடு
13. ீ ங்கள் யட்டில்
ீ
ததர்வநாநீ ட்டர் (
லயத்திமக்கிீர்கா?
அ) ஆம்
ஆ) இல்ல
ோய்ச்சல் ார்க்கும் ேருயி
)
ிரிவு – ஆ
குிப்பு:- (ேீ ழ்யரும் யிாக்ேள யாசித்து சரினா யிளடனிக்ேவும்)
நாதிரி ண்:...............
1.
காய்ச்சல் ன்ால் ன்?
அ) யிப்பு
ஆ) உடின் ிம் ீ நாக நாறுதல்
இ) உடல் தயப் ில அதிகரித்தல்
2.
காய்ச்சல் யிப்பு ன்ால் ன்?
அ) இது எம ததாற்று வாய்
ஆ) காய்ச்சிால் சிறு குமந்லதகளுக்கு ற்டும் யிப்பு
இ) இது எம ந வாய்
3.
காய்ச்சல் யிப்புக்கா காபணம் ன்?
அ) லயபஸ் நற்றும் ாக்டீரினா ததாற்றுகள்
ஆ) அஜீபணம்
இ) யனிற்றுப்வாக்கு
4. ந்த யனதில் உள் குமந்லதகளுக்கு காய்ச்சல் யிப்பு யப அதிக
யாய்ப்புள்து?
அ) ந்து முதல் 10 யலப
ஆ) 10 யனதுக்கு வநல்
இ) 3 நாதம் முதல் 5 யலப
5.
காய்ச்சல் யிப்புத்தாக்கத்தின் யலககள் னாலய?
அ) முதன்லந நற்றும் இபண்டாம் ில
ஆ) ின நற்றும் சிக்கா
இ) உனர் நற்றும் குலந்த தபம்
6. காய்ச்சல் யிப்புத் தாக்குதின் ச்சரிக்லக அிகுி ன்?
அ) தலயி
ஆ) ேண்ார்ளய இலடமறு
இ) 100.4˚f க்கு வநல் காய்ச்சல் இருப்து
7. காய்ச்சல் யிப்புத்தாக்கத்தின் வாது கண்கில் ற்டும் நாற்ங்கள் ன்?
அ) ேண்ேள கநல்காக்ேி உருட்டுயது
ஆ) சுமங்கின கண்கள்
இ) மூடின கண்கள்
8. காய்ச்சல் யிப்புத்தாக்கத்தின் வாது ிலவு ில ன்யாக இமக்கும்?
அ) ச்சரிக்லக நற்றும் உணர்வு
ஆ) அலப உணர்வு
இ) சுன ிலவு இமப்பு
9. காய்ச்சல் யிப்புத்தாக்கத்தின் வாது வதாில் ற்டும் நாற்ங்கள் ன்?
அ)
தடிப்புகள்
ஆ) வதாின் ீ ிநாற்ம்
இ) கதால் சியந்த ிள
10.
காய்ச்சல் யிப்புத்தாக்கத்தின் வாது லக நற்றும் கால்கில் ற்டும்
நாற்ம் ன்?
அ) லக நற்றும் கால் திடீதபன்று தயட்டி இழுத்தல்
ஆ) லக நற்றும் கால் வகாணங்கின் யிகல்
இ) லக நற்றும் கால்கில் டுக்கம் ற்டுதல்
11. காய்ச்சல் யிப்பு தாக்கத்தின் வாது உடடினாக கயிக்க வயண்டினது
ன்?
அ) குமந்லதனின் ிம்
ஆ) உடல் தயப்ில
இ) அமகிலுள் கூர்லநனா தாமள்கள
12. காய்ச்சல் யிப்பு தாக்கத்தின் வாது சிறுீ பக அலநப்ில் ற்டும் நாற்ம்
ன்?
அ) தன்ிச்லசனாக சிறுீர் ேமித்தல்
ஆ) சிறுீர் அடிக்கடி தயிவனறுயது
இ) சிறுீ ர் கமித்தில் தலட
13. காய்ச்சல் யிப்பு தாக்கத்தின் வாது சுயாச முலனில் ற்டும் நாற்ம்
ன்?
அ) சுயாசத்லத அதிகரிக்கும்
ஆ) சுயாசம் யிடுயதில் தலட
இ) எழுங்கற் சுயாசம்
14. காய்ச்சல் யிப்பு 30 ிநிடங்களுக்கு வநல் ீ டிக்கும் வாது தாதுயா
சிக்கல் ன்?
அ) ததாடர் யிப்பு
ஆ) மூல ாதிப்பு ற்டுதல்
இ) க்கயாதம்
15. ததாடர்ச்சினா காய்ச்சல் யிப்ிால் ற்டும்
யிலவு ன்?
அ) மூல வசனிமப்பு
ஆ) மூல காய்ச்சல்
இ) ந குலாடு
16. காய்ச்சல் யிப்பு தாக்கத்தின் வாது ாம் ன் தல நற்றும் கழுத்து
குதினில் ஆலடகல தர்யாக லயக்க வயண்டும்?
அ) உடல துலடப்தற்கு
ஆ) மூச்சு திணல தயிப்தற்கு
இ) குமந்லதலன தூண்டுயதற்காக
17. காய்ச்சல் யிப்பு தாக்கம் ற்ட்ட ிகு குமந்லதலன ந்த ிலனில்
டுக்க லயக்க வயண்டும்?
அ) வபாக ிநிர்ந்த ிலனில்
ஆ) கயிழ்ந்து டுக்க லயத்தல்
இ) குமந்லதனின் உடலமம் தலலனமம் எம க்கயாட்டில் திமப்ி
முகத்லத கீ ழ்புநாக திமப்புயது
18. காய்ச்சல் யிப்பு தாக்கத்லத கண்டிமம் ரிவசாதல ன்?
அ) இமதன சுமள் டம்
ஆ) மூலக்கா சுமள் டம்
இ) இருதன எதிவபாி ஆய்வு
19. ததாடர்ச்சினா காய்ச்சல் யிப்பு தாக்கத்திால் ற்டும் ின்யிலவு
ன்?
அ) நந்தநா வச்சு
ஆ) வச்சு யர்ச்சி தாநதநாதல்
இ) திக்கு யாய்
20. தற்வார் ப்வாது அயசப உதயிக்கு அலமக்க வயண்டும்?
அ) காய்ச்சல் யிப்பு 30 ிநிடங்களுக்கு வநாக இமந்து மூச்சு யிடுயதில்
சிபநம் ற்ட்டால்
ஆ) காய்ச்சல் 100.4˚f க்கு அதிகநாக இமந்தால்
இ) குமந்லதனின் உடல் தயிின ித்தில் இமந்தால்
ிரிவு – இ
குிப்பு:-(ேீ ழ்யரும் யிாக்ேள யாசித்து சரினா யிளடனிக்ேவும்)
நாதிரி ண்:...............
யிாக்ேள்
ய.
1.
குமந்ளதனின் உடல் வயப்ிளளனக் குளக்ேவும்.
2.
வநன்ளநனா நற்றும் ாதுோப்ா கநற்பப்ில் குமந்ளதளனப்
ாதுோத்தல்.
3.
குமந்ளதளன வற்காரின் க்ேத்தில் ளயத்தல்.
4.
குமந்லதலனச் சுற்ிலும் அலநதினா சூழ்ிலலன உமயாக்குதல்.
5.
ோய்ச்சல் யிப்புத்தாக்ேதின் அிகுிேள் நற்றும் ோ அளயக்
ேயிக்ேவும்.
6.
அருேிலுள் கூர்ளநனா வாருள்ேள அேற்றுயது.
7.
குமந்ளதளன தளபனில் டுக்ே ளயத்தல்.
8.
தள நற்றும் ேழுத்ளத சுற்ிமள் ஆளடேள தர்யாே ளயத்தல்.
9.
குமந்ளதளன நருத்துயரிடம் அளமத்துச் வசல் துரிதப் டுயது..
10.
ோய்ச்சல் யிப்ின் காது குமந்ளதளன அளசத்து எழுப்புயது
11.
யாய்மூநாே சுயாசம் வோடுக்ே முனற்சித்தல்.
12.
ோய்ச்சல் யிப்பு தாக்ேத்தின் காது குமந்ளதனின் ற்ேள திந்து
யானில் ஏதாயது ளயப்து.
13.
குமந்ளதனின் யாய் நற்றும் மூக்ேில் இருந்து யரும் திபயத்ளத
உிஞ்சுயது.
14.
இருதனத்ளத கதய்த்து ிளசந்து யிடுதல்.
15.
ோய்ச்சல் யிப்பு தாக்ேத்தின் காது குமந்ளதளன ேட்டுப்டுத்துயது.
16.
ோய்ச்சல் யிப்பு ஏற்ட்டு முடிந்த உடககன குமந்ளதளன தூண்டுதல்.
ஆம்
இல்ல
APPENDIX- XI
EDUCATIONAL INTERVENTION MODULE
FEBRILE SEIZURE IN CHILDREN
INTRODUCTION:
A febrile seizure is a convulsion in a child caused by a spike in body temperature, often from
an infection. They occur in young children with normal development without a history of
neurologic symptoms.
These are called febrile seizures (pronounced FEB-rile) and occur in 2% to 5% of all children
(2 to 5 out of 100 children). If a child's parents, brothers or sisters, or other close relatives have
had febrile seizures, the child is a bit more likely to have them.
Sometimes the seizure comes "out of the blue" before it is recognized that the child is ill. A
fever may begin silently in a previously healthy child. A seizure can be the first sign that alerts
the family that the child is ill.
DEFINITION:
Febrile seizures are convulsions that can happen when a young child has a fever above
100.4°F (38°C). (Febrile means "feverish.") The seizures usually last for a few minutes and stop
on their own. The fever may continue for some time.
Febrile seizures are not considered epilepsy (seizure disorder). Kids who have a febrile
seizure have only a slightly increased risk for developing epilepsy.
CAUSES:
Usually, a higher than normal body temperature causes febrile seizures.
Even a low-grade fever can trigger a febrile seizure.
A febrile seizure is a convulsion caused by abnormal electrical activity in the nerve
cells of the brain that is brought on by having a fever. The exact cause of febrile
seizures is not known. Seizures might occur when a child's temperature rises or falls
rapidly.
Infection: The fevers that trigger febrile seizures are usually caused by a viral infection,
and less commonly by a bacterial infection. Influenza and the virus that causes roseola,
which often are accompanied by high fevers, appear to be most frequently associated
with febrile seizures.
Post-immunization seizures: The risk of febrile seizures may increase after some
childhood immunizations. These include the diphtheria, tetanus and pertussis or measlesmumps-rubella vaccinations. A child can develop a low-grade fever after a vaccination.
The fever, not the vaccination, causes the seizure.
RISK FACTORS FOR FEBRILE SEIZURE
Febrile seizures are caused by fever, usually higher than 102°F (38.8°C). There are
several risk factors for febrile seizures. When more than one risk factor is present, the risk is
even higher. Recurrent febrile seizures are associated with an increased risk of delayed
vocabulary development.
Risk factors for febrile seizures include the following:
Age (occurs between the ages of 3 months and 5 years)
Developmental delays (e.g., cerebral palsy, mental retardation)
Family history of seizure disorders
Frequent fevers (e.g., caused by viral or bacterial infection)
High fever (above 102°F)
Maternal smoking and alcohol use during pregnancy (further research is needed to confirm
this link)
Meningitis (inflammation of the membranes that surround the brain and spinal cord)
Personal history (i.e., previous febrile seizure)
Certain pathogens (disease-causing organisms; e.g., viruses, bacteria) are associated with an
increased risk for febrile seizures. These pathogens include influenza A virus, which causes the
flu,
human
herpesvirus
6
(HHV-6),
which
causes
roseola,
and Shigella and Campylobacter bacteria, which cause gastroenteritis (e.g., diarrhea, nausea,
vomiting, fever).
Children who were hospitalized as newborns and children who are in day care are at increased
risk for fevers and febrile seizures. Childhood immunizations and urinary tract infections
(UTIs) also may increase the risk.
INCIDENCE OF FEBRILE SEIZURE
Febrile seizures, which affect approximately 3 percent of children, are most common
between the ages of 6 and 18 months.
A child's first febrile seizure rarely occurs before the age of 3 months or after the age
of 3 years.
Boys have a slightly higher risk for febrile seizures than girls.
About 30–50 percent of children who have a febrile seizure experience an additional
seizure.
Most children outgrow febrile seizures by the age of ten.
TYPES OF FEBRILE SEIZURE:
Febrile seizures have been divided two groups, simple or complex.
Simple febrile seizures last fewer than 15 minutes, do not recur within 24 hours, and are
generalized (i.e., affect a widespread area of the body). Following a simple febrile
seizure, the child may be drowsy or confused for a short period of time.
Complex febrile seizures last longer than 15 minutes, recur within 24 hours, or are
focalized (i.e., affect a specific area of the body). Complex febrile seizures can occur as a
result of a serious illness, such as meningitis (inflammation of the membranes that
surround the brain and spinal cord) or encephalitis (brain inflammation). Children who
experience complex febrile seizures have a slightly higher than normal risk for
developing epilepsy.
SYMPTOMS:
A child having a febrile seizure may:
Have a fever higher than 100.4 F (38.0 C)
Lose consciousness
Stiffen, jerk or twitch the muscles of the arms and legsarms and legs
A stiff neck
Extreme sleepiness
Flutter eyelids or roll the eyes
Their skin may look darker than usual and begin to turn blue
The child may cry or moan.
If standing, the child will fall.
The child may vomit or bite their tongue.
Have irregular breathing.
Lose bladder or bowel control.
Frothing and salivation from mouth.
DIAGNOSTIC EVALUATION:
o When a febrile seizure occurs, parents and caregivers should contact the child's
pediatrician immediately.
o Diagnosis may involve a history of symptoms and a thorough physical
examination, including a neurological exam.
o In some cases, laboratory tests (e.g., blood tests, urine tests, lumbar puncture) are
performed to rule out other possible causes for the seizure, such as dehydration
(e.g., caused by severe vomiting and/or diarrhea) and meningitis and determine
the cause for the fever.
Blood tests that may be performed include a complete blood count (CBC) and
blood cultures. These tests are used to detect viruses or bacteria and high levels of
white blood cells, which may indicate infection.
In some cases, a lumbar puncture (also called a spinal tap) is performed to rule
out meningitis. In this test, a needle inserted between two lumbar vertebrae in the
spinal column is used to withdraw cerebrospinal fluid for microscopic evaluation.
The fluid is examined for pathogens (e.g., virus, bacteria) and elevated levels of
white blood cells. Cerebrospinal fluid also may be cultured to identify the virus
or bacterium.
Further testing may not be needed if the child is developmentally normal, if the results of
the neurological exam are normal, and if the febrile seizure meets the following criteria:
Seizure is general, not focal (i.e., involves more than one part of the body).
Seizure does not last longer than 15 minutes.
Seizure does not recur within 24 hours.
Complex febrile seizures may require more extensive diagnostic testing. If the results of
the physical examination and laboratory tests are inconclusive, or if the physician suspects a
neurological condition, such as epilepsy, an electroencephalogram (EEG) may be performed.
EEG is a noninvasive test that detects, measures, and records brain wave activity. In this
test, electrodes are placed on the head and attached by wires to a machine that converts
electrical signals from the brain into wavy lines on a moving sheet of graph paper.
Electroencephalogram usually is performed about 1 week after a febrile seizure because
high fever or the seizure itself can affect the results.
MANAGEMENT:
If your child has a febrile seizure, stay calm and:
1. Gently place your child on the floor or the ground.
2. Remove any nearby objects.
3. Place your child on his or her side to prevent choking.
4. Loosen any clothing around the head and neck.
5. Watch for signs of breathing problems, including bluish color in the face.
6. Try to keep track of how long the seizure lasts.
If the seizure lasts more than 5 minutes, or your child turns blue, it may be a more serious
type of seizure — call Pediatrician right away.
It's also important to know what you should not do during a febrile seizure:
Do not try to hold or restrain your child.
Do not put anything in your child's mouth.
Do not try to give your child fever-reducing medicine.
Do not try to put your child into cool or lukewarm water to cool off.
When the seizure is over, call your doctor for an appointment to find the cause of the
fever. The doctor will examine your child and ask you to describe the seizure. In
most cases, no other treatment is needed. The doctor might order tests if your child is
under 1 year old and had other symptoms, like vomiting or diarrhea.
The
doctor
may recommend
the
standard
treatment
for
fevers,
which
is acetaminophen or ibuprofen. Giving these medicines around the clock is not
recommended and won't prevent febrile seizures.
If your child has more than one or two febrile seizures that last more than 5 minutes,
the doctor might prescribe an anti-seizure medicine to give at home.
COMPLICATIONS:
In most cases, febrile seizures resolve without complications. If the child is standing,
eating, or drinking when the seizure occurs, he or she may be injured by the fall, may
choke, or may inhale fluid into the lungs. The child also may bite his or her tongue,
lips, or inside of the cheek during a febrile seizure.
Febrile seizures increase the risk for epilepsy slightly. However, more than 95% of
children who have febrile seizures do not develop a seizure disorder. Febrile seizures
do not increase the risk for brain damage or mental retardation.
In rare cases, a condition called status epilepticus can occur during a febrile
seizure. Status epilepticus is a medical emergency in which a seizure lasts longer than
30 minutes or seizures recur without recovery for 30 minutes or longer. This
condition is more common in children under the age of 1 year. Status epilepticus can
cause brain damage and may be fatal.
Febrile seizures are provoked seizures and don't indicate epilepsy. Epilepsy is a
condition characterized by recurrent unprovoked seizures caused by abnormal
electrical signals in the brain.
The most common complication is the possibility of more febrile seizures. The risk of recurrence
is higher if:
Your child's first seizure resulted from a low fever.
The period between the start of the fever and the seizure was short.
An immediate family member has a history of febrile seizures.
Your child was younger than 18 months at the time of the first febrile seizure.
RECOMMENDED PRACTICES
1. Lower the child body temperature
2. Protect the child on a soft and safe surface
3. Place the child on his/her side
4. Keep calm
5. Observe febrile seizure manifestation and duration
6. Remove any nearby objects
7. Place your child on the floor
8. Loosen any clothing around the head and neck
NON-RECOMMENDED PRACTICE
1.
Rush the child to a doctor
2.
Shake and rouse the convulsing child
3.
Pry the convulsing child’s clenched teeth apart and put something in his/her mouth
4.
Attempt mouth-to-mouth resuscitation
5.
Suck discharge from the child’s nose and mouth
6.
Cardiac massage
7.
Restrain the convulsing child
8.
Stimulate the convulsing child
WHEN TO CALL FOR HELP
Have someone call pediatrician for emergency help if any of these things happens:
o The seizure lasts more than5minutes. The emergency squad can give medicine to stop
the seizure.
o Your child has trouble breathing during the seizure and his skin or lips change in
color.
o Your child chocks on secretions (blood, vomit, etc.)
o Your child is injured during a fall or during the seizure and requires first aid ( cut,
broken bone ).
Call your child’s pediatrician if he/she
o
Has a febrile seizure for the first time
o
Has more than one febrile seizure
o
Looks very ill, is very fussy or is hard to wake up
o
Has a stiff neck, bad headache, very sore throat, painful stomachache, unusual rash
or keeps vomiting and has diarrhea
o
Is younger than 2 months of age and has a rectal temperature of 100.4˚f or higher
o
Fever comes back and lasts for 3 days or longer
o
Shows signs of dehydration – dry or sticky mouth, sunken eyes, or not urinating.
PREVENTION:
Most febrile seizures occur in the first few hours of a fever, during the initial rise in body
temperature.
Most children who have febrile seizures do not require daily treatment with seizure
medicines. However, children who have a history of prolonged febrile seizures and those who
live in more remote areas with poor access to prompt medical care should be given a rescue
medication.
Giving your child medications
Giving your child infants' or children's acetaminophen (Children's Non-Aspirin Tylenol,
others) or ibuprofen (Infants' Motrin, Children's Motrin, others) at the beginning of a fever may
make your child more comfortable, but it won't prevent a seizure.
Prescription prevention medications
o Rarely, prescription anticonvulsant medications are used to try to prevent febrile
seizures. However, these medications can have serious side effects that may outweigh
any possible benefit.
o Rectal diazepam (Diastat) or nasal midazolam might be prescribed to be used as needed
for children who are prone to long febrile seizures. These medications are typically
used to treat seizures that last longer than five minutes or if the child has more than one
seizure within 24 hours. They are not typically used to prevent febrile seizures.
o Sponge baths, applying cool cloths and using fever-reducing medications such as
acetaminophen (Tylenol) or ibuprofen (Advil, Motrin). It make a feverish child feel
better.
o If your child has frequent febrile seizures, talk to your health care team about the best
approach to prevent or treat seizures.
Follow up
The regular follow up is very important in after febrile seizure attack, in that the
pediatrician check up child health and nutritional status.
குமந்லதகளுக்கு ற்டும் காய்ச்சல் யிப்பு
ற்ின க்கல்யி
முன்னுளப:
காய்ச்சல் யிப்பு ன்து உடல் தயப்ில காபணநாக
குமந்லதக்கு ற்டும் யிப்பு.
யலபனல:
காய்ச்சல் யிப்புத்தாக்கம் ன்து எம சிறு குமந்லதக்கு
100.4 ˚F க்கு வநல் காய்ச்சல் யமம்வாது ற்டக்கூடின யிப்பு ஆகும்.
காபணங்கள்:
எரு குமந்ளதனின் உடல்
வயப்ிள உனரும்காது
அல்து
கயேநாே யழ்ச்சினளடமம்
ீ
காது யிப்பு ஏற்டாம்
ோய்ச்சல்
யிப்புத்தாக்ேங்ேள்
வாதுயாே
ளயபஸ்
வதாற்றுகானால் ஏற்டுேின், கநலும் வாதுயாே ாக்டீரினா
வதாற்ாலும் ஏற்டுேின்.
சி குமந்ளதக்கு ருய காய்த்தடுப்பு நருந்துேளுக்குப் ிகு
ோய்ச்சல் யிப்புத்தாக்ேங்ேின் ஆத்து அதிேரிக்ேக்கூடும்
ோய்ச்சல் யிப்புக்ோ ஆத்து ோபணிேள்:
வதாடர்ச்சினா ோய்ச்சல் யிப்புத்தாக்ேங்ேள் கச்சு திள
ாதிக்ேிது.
ஒழுங்ேற் சுயாசம்
யனது
யர்ச்சி தாநதங்ேள்
யிப்புத்தாக்ேக் கோாின் குடும் யபாறு
அடிக்ேடி ோய்ச்சல்
அதிே ோய்ச்சல்
ேர் ோத்தில் தாய் புளேிடித்தல் நற்றும் நது குடித்தல்
தண்டு மூளச் சவ்வுக் ோய்ச்சல்
ோய்ச்சல் யிப்பு யளேேள்:
1. எின ோய்ச்சல் யிப்பு
15 ிநிடங்ேளுக்கும் குளயாது, 24 நணி கபத்திற்குள் நீ ண்டும்
ிேமக்கூடாது.
2. சிக்ோ ோய்ச்சல் யிப்பு
15 ிநிடங்ேள் ீடிக்கும், 24 நணி கபத்திற்குள் நீ ண்டும் ிேமாம்.
அிகுிேள்:
100.4˚F க்கு கநல் ோய்ச்சல்
சுனிளவு இமப்பு
ளே நற்றும் ோல்ேள் இழுத்தல்
ேண்ேள கநல் காக்ேி உருட்டுயது
கதால் ீநாே நாறுதல்
தன்ிச்ளசனாே சிறுீ ர் ேமித்தல்
குமந்லத அழுயது
யானிிமந்து உநிழ்ீர் சுபத்தல்
காய் ேண்டிமம் கசாதள:
உடல் ரிகசாதள
இபத்த கசாதள
யபாறு கசேரிப்பு
மூளக்ோ சுருள் டம்
சிறுீ ர் கசாதள
முதுவேலும்பு திபய குப்ாய்வு
ின்யிளவுேள்:
யிப்பு ஏற்டும்காது குமந்ளத ின்று வோண்டிருந்தால்,
யழ்ச்சினால்
ீ
ோனநளடனக்கூடும்.
யிப்பு ஏற்டும்காது குமந்ளத சாப்ிட்டால் புளப ஏ
யாய்ப்புள்து
யிப்பு ஏற்டும் காது குமந்ளத தது ாக்கு நற்றும்
உதடுேளக் ேடிக்ேக்கூடும்.
ோய்ச்சல் யிப்புத்தாக்ேங்ேள் ோல்-ளே யிப்புக்ோ ஆத்ளத
சிிது அதிேரிக்கும்.
ோய்ச்சல் யிப்புத்தாக்ேங்ேள் மூள ாதிப்பு நற்றும்
ந குளாட்டிற்ோ ஆத்ளத அதிேரிக்ோது.
அரிதா சந்தர்ப்ங்ேில், ோய்ச்சல் யிப்புத்தாக்ேத்தின் காது
வதாடர் யிப்பு ிள ஏற்டாம். யிப்பு 30 ிநிடங்ேள்
ீடிக்கும்.
ரிந்துளபக்ேப்ட்ட ளடமுளேள்:
குமந்ளதனின் உடல் வயப்ிளளனக் குளக்ேவும்.
வநன்ளநனா நற்றும் ாதுோப்ா கநற்பப்ில்
குமந்ளதளனப்
ாதுோத்தல்.
குமந்ளதளன வற்காரின் க்ேத்தில் ளயத்தல்.
குமந்லதலனச்
சுற்ிலும்
அலநதினா
சூழ்ிலலன
உமயாக்குதல்.
ோய்ச்சல்
யிப்புத்தாக்ேதின்
அிகுிேள்
நற்றும்
ோ
அளயக் ேயிக்ேவும்.
அருேிலுள் கூர்ளநனா வாருள்ேள அேற்றுயது.
குமந்ளதளன தளபனில் டுக்ே ளயத்தல்.
தள நற்றும் ேழுத்ளத
சுற்ிமள் ஆளடேள தர்யாே
ளயத்தல்.
ரிந்துளபக்ேப்டாத ளடமுளேள்
குமந்ளதளன நருத்துயரிடம் அளமத்துச் வசல் துரிதப்
டுயது.
ோய்ச்சல் யிப்ின் காது குமந்ளதளன அளசத்து
எழுப்புயது.
யாய்மூநாே சுயாசம் வோடுக்ே முனற்சித்தல்.
ோய்ச்சல் யிப்பு தாக்ேத்தின் காது குமந்ளதனின் ற்ேள
திந்து யானில் ஏதாயது ளயப்து.
குமந்ளதனின் யாய் நற்றும் மூக்ேில் இருந்து யரும் திபயத்ளத
உிஞ்சுயது.
இருதனத்ளத கதய்த்து ிளசந்து யிடுதல்.
ோய்ச்சல் யிப்பு தாக்ேத்தின் காது குமந்ளதளன
ேட்டுப்டுத்துயது
ோய்ச்சல் யிப்பு ஏற்ட்டு முடிந்த உடககன குமந்ளதளன
தூண்டுதல்.
ப்வாது உதயிக்கு அலமக்க வயண்டும்?
யிப்பு 5 ிநிடங்களுக்கு வநல் ீடிக்கும் காது
யிப்புத்தாக்கத்தின் வாது உங்கள் ிள்லக்கு சுயாசிப்தில்
சிக்கல் ஏற்ட்டு, கதாின் ிம் ீ நாே நாறுதல்.
காய்ச்சல்
யிப்புத்தாக்கத்தின்
வாது
உங்கள்
குமந்ளத
யானிிமந்து ீர் அல்து இபத்த சுபப்பு யருயது.
காய்ச்சல்
யிப்புத்தாக்கத்தின்
கானம் ஏற்ட்டால்.
வாது
உங்கள்
குமந்ளதக்கு
Thank you