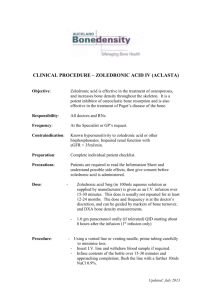
Aya Bassatne SHARP 321A Clinical Trial Protocol Administrative information 1- Title: A one year, multicenter, investigator, participants and data analyst blinded, randomized, parallel group, non-inferiority trial comparing the efficacy of zoledronate 5mg once yearly vs 4mg twice yearly on aromatase inhibitor induced bone loss in postmenopausal women with breast cancer 2- Trial Registration Intended registry: ClinicalTrials.gov NCT-------Table 1: WHO Trial Registration data Data Category Primary registration and trial identifying number Date of registration in primary registration Secondary identifying numbers Source(s) of monetary or material support Primary sponsor Secondary sponsor(s) Contact for public queries Contact for scientific queries Public title Scientific title Countries of recruitment Health conditions or problems studied Interventions Information ClinicalTrials.gov: NCT-------Pending Not applicable To be submitted to the Medical Practice Plan (MPP) and the University Research Board (URB) at the American University of Beirut (AUB) American University of Beirut Medical Center (AUBMC) Not applicable Marlene Chakhtoura: mc39@aub.edu.lb Marlene Chakhtoura: mc39@aub.edu.lb Different doses of zoledronate for prevention of aromatase inhibitor induced bone loss in postmenopausal women with breast cancer: a randomized controlled trial A one year, multicenter, investigator, participants and data analyst blinded, randomized, parallel group, non-inferiority trial comparing the efficacy of zoledronate 5mg once yearly vs 4mg twice yearly on aromatase inhibitor induced bone loss in postmenopausal women with breast cancer Lebanon Aromatase inhibitor induced bone loss Intervention 1: IV zoledronate 5mg once and then placebo IV infusion after 6 months Intervention 2: IV zoledronate 4mg every 6 months 1 Key inclusion and exclusion criteria Inclusion: Lebanese postmenopausal women Non metastatic estrogen receptor positive breast cancer (Stage I-IIIa) On (<6 months) or starting aromatase inhibitor therapy BMD T-score -1.5 OR T-score -1 with > 1 risk factor (age>65, low BMI (<20 kg/m2), family history of hip fracture, personal history of fractures or smoking) OR history of fragility fracture (lumbar spine fracture, hip fracture or ≥ 2 peripheral fractures) OR FRAX calculated MOF risk > age-dependent threshold using the Lebanese FRAX calculator Exclusion: Radiological or clinical evidence of metastasis Other malignancy Chronic conditions that could affect bone turnover (Cushing’s, uncontrolled thyroid disease, osteomalacia, hyperparathyroidism, diabetes mellitus…) Intake of medications that could affect bone turnover (anticonvulsants, bisphosphonates within the past 12 months, HRT within the past 12 months, chronic steroid use for 3-6 months) Liver impairment (LFTs three times upper normal limit) Renal impairment (GFR <35ml/min) Hypocalcemia Hypersensitivity reaction to bisphosphonate Study type Date of first enrolment Target sample size Recruitment status Primary outcome(s) Key secondary outcomes Phase III, triple blinded, randomized, controlled, noninferiority trial with two parallel groups Not applicable 92 participants per arm Not applicable Percent change lumbar spine BMD at 12 months Percent change total hip and femoral neck BMD at 12 months Percent change bone markers (osteocalcin, crosslaps) at 12 months Percent change lumbar spine BMD at 6 months Rates of adverse events Rates of fractures 2 3- Protocol Version September 28th 2019, Version 1 4- Funding To be submitted for funding from the Medical Practice Plan (MPP) and University Research Board (URB) at the American University of Beirut (AUB), Lebanon. We will contact Fattal & fils to provide the primary investigator with zoledronic acid ampoules manufactured by Novartis. 5- Roles and Responsibilities a) Protocol contributors - Ghada El Hajj Fuleihan, MD, MPH: gf01@aub.edu.lb Professor of Medicine Calcium Metabolism and Osteoporosis Program, Division of Endocrinology and Metabolism, Department of Internal Medicine American University of Beirut Medical Center, Beirut, Lebanon Principal investigator: responsible for study design and conception, protocol development and revision, oversight of subjects’ recruitment, data collection, data entry, data analysis and interpretation, review of manuscript drafts, revision and approval of the final versions. - Marlene Chakhtoura, MD, MSc: mc39@aub.edu.lb Instructor of Clinical Medicine Calcium Metabolism and Osteoporosis Program, Division of Endocrinology and Metabolism, Department of Internal Medicine American University of Beirut Medical Center, Beirut, Lebanon Co- investigator: responsible for study design and conception, protocol development and revision, oversight of subjects’ recruitment data collection, data entry, data analysis and interpretation, review of manuscript drafts, revision and approval of the final versions. - Aya Bassatne, MD: aaa144@mail.aub.edu Research Fellow Calcium Metabolism and Osteoporosis Program, Division of Endocrinology and Metabolism, Department of Internal Medicine American University of Beirut Medical Center, Beirut, Lebanon Co-investigator: responsible for proposal development, protocol update(s) and revision(s), subject recruitment, data entry, analysis and interpretation, and review of manuscript drafts and approval of the final versions. - Ziad Mahfoud, PhD: zrm2001@Qatar-med.cornell.edu Associate Professor of Medicine Weil Cornell, Qatar Consultant American University of Beirut, Lebanon. Co-investigator: trial statistician responsible for advice on clinical trial design, sample size 3 calculation and analysis plan, oversight of analyses with the principal investigator and the research fellow, and approval of the final version of manuscript. Co-investigators from the Hematology Oncology department at AUBMC will be contacted and added as contributors accordingly b) Trial Sponsor American University of Beirut Medical Center (AUBMC) Address: Hamra, Beirut, Lebanon POBox: 11-0236, Riad El Solh, Beirut, Lebanon. Email: aubmc@aub.edu.lb Phone: +9611350000 c) Role of study sponsor and funder The trial sponsor and the funding source will not have any role in the design, implementation, analyses, or publication of this study. d) Committees Trial Steering Committee: Dr. Ghada El Hajj Fuleihan Dr. Marlene Chakhtoura Dr. Aya Bassatne Responsible for agreeing the final protocol and amendments, providing overall supervision and monitoring the progress of the study. Trial management committee: Dr. Ghada El Hajj Fuleihan Dr. Marlene Chakhtoura Dr. Aya Bassatne Responsible for preparing and managing the budget, reporting and monitoring adverse events, assisting in IRB applications and verifying the data. Data manager: Responsible for maintenance of trial IT system, data entry and data verification. Data safety monitoring committee: Responsible for reviewing all trial adverse events, and making recommendations for unblinding and study termination. Introduction 6- Background and rationale 4 a) Description and justification of the research question Breast cancer is the most common cancer in women and accounts for 15% of all cancer related mortality worldwide (1, 2). It is therefore considered a major public health problem and is estimated to reach an annual incidence of 3.2 million by year 2050 (2). In Lebanon, breast cancer accounts for 37% of cancer cases among women and 20% of cancer cases overall (3). Incidence rates have been increasing for years among Lebanese women and are among the highest in the region and worldwide (3). Treatment of breast cancer involves various modalities including surgery, radiation, chemotherapy and hormone therapy. The selection of therapy is based on several factors such as menopausal state, cancer stage, grade, histology and the presence or absence of estrogen or progesterone receptors (4). Aromatase inhibitors (AIs) have been shown to be beneficial and superior to tamoxifen as adjuvant therapy in postmenopausal women with estrogen receptor positive breast cancer (5, 6). Despite their various benefits, AIs are associated with multiple side effects that are becoming more prevalent due to the increased survival of women with breast cancer (7). Estrogen’s role in maintaining bone metabolism and hemostasis is well established. At menopause, estrogen levels start to decrease leading to an increase in bone resorption and bone loss. In the postmenopausal state, the main source of estrogen becomes the peripheral conversion of adrenal androgens (7). AIs suppress the peripheral conversion of androgen into estrogen (7). This leads to a more abrupt decrease in estrogen levels, and therefore a faster rate of bone loss at the Lumbar Spine (LS) or hip (a drop by 1.7-5.8% yearly) compared to that seen in postmenopausal women not taking aromatase inhibitors (1-2% yearly decrease) (7, 8). Furthermore, several studies showed deleterious effects of AIs on multiple independent predictors of fractures. AIs were shown to significantly decrease bone mineral density (BMD), trabecular bone score and hip structural geometry while they increased bone turnover markers (9-11). The growing use of AIs in postmenopausal women with breast cancer, dictates the need for bone health assessment and prevention of bone loss in this population. Several guidelines were published for the evaluation and management of AI induced bone loss; however, these were inconsistent regarding the eligibility for treatment, timing of treatment initiation and monitoring of bone loss (12-14). Several antiresorptive medications were recommended for the prevention of AI induced bone loss (12). The effect of bisphosphonates on AI-induced bone loss in postmenopausal women was evaluated in multiple randomized controlled trials. Oral bisphosphonates at doses used for post-menopausal osteoporosis were shown to prevent bone loss at the LS in women on AI therapy (15-17). Intravenous (IV) Zoledronic acid is the most potent bisphosphonate and is approved for treatment of osteoporosis (7). It has also been investigated in AI induced bone loss but only at the 4mg twice yearly dose (18-20). Zoledronic acid increased LS BMD significantly by 2.7% at 12 months and 4.3% at 5 years in postmenopausal women (median age 58), receiving AI (19, 20). Most of the participants had well established menopause (83%) and normal BMD (65-70%) at study entry (19, 20). Starting zoledronic acid concomitantly with AI therapy was found to be more beneficial than delaying it until bone loss or fractures occur (18, 19, 21). IV zoledronate at a dose of 5mg once yearly is approved for treatment of osteoporosis but has not been investigated for the prevention of AI-induced bone loss in postmenopausal women. Since oral bisphosphonates at doses similar to those used in osteoporotic women have proven to be beneficial in preventing AI induced bone loss (15-17), we expect that zoledronic acid will be also effective at the 5 mg yearly dose. If proven to prevent AI induced bone loss, such dose would increase compliance and decrease cost and side effects compared to the twice yearly dose 5 b) Choice of comparators Two arms with different zoledronic acid dose: IV zoledronate 4mg every 6 months: This dose has been studied in multiple randomized clinical trials (19, 20) and was proven to be efficient in preventing AI induced bone loss. Its use is suggested by multiple societies and guidelines (12, 13). It is unethical to use a placebo arm in patients at risk for bone loss knowing that there is a beneficial treatment. IV zoledronate 5mg once yearly: This dose is approved by the Food and Drug Administration for use in osteoporosis. If proven to be efficacious against AI induced bone loss, it would increase compliance and decrease cost and side effects. 7- Objectives Hypothesis: IV Zoledronate at a dose of 5mg once yearly is non-inferior to 4mg twice yearly in preventing aromatase inhibitor induced bone loss at the lumbar spine in postmenopausal women with breast cancer. Primary Objective: To evaluate the effect of IV zoledronate 5mg once yearly compared to 4mg twice a year on lumbar spine bone mineral density using DXA at 12 months in postmenopausal women with breast cancer receiving aromatase inhibitors. Secondary Objectives: To evaluate the effect of IV zoledronate 5mg once yearly compared to 4mg twice a year on total hip bone mineral density using DXA and serum bone markers at 12 months in postmenopausal women with breast cancer receiving aromatase inhibitors. 8- Trial design This study is a one year phase III, multicenter, randomized, controlled, investigator, participant and data analyst blinded, non-inferiority trial with two parallel groups with a 1:1 allocation ratio to investigate the efficacy of zoledronate 5mg once a year versus zoledronate 4mg twice a year, on bone density loss at the lumbar spine. We chose to conduct an RCT because it is the highest level of evidence and the gold standard for assessing causality. Methods: Participants, interventions and outcomes 9- Study setting Postmenopausal women with breast cancer will be approached and recruited from the Oncology specialty clinics and the outpatient departments of all three participating hospitals (AUBMC, CMC and KMC to be contacted) in Beirut, Lebanon. The study visits, interventions, blood and urine collection will take place at all centers and samples collected at CMC or KMC will be sent to AUBMC for analysis. All BMD measurements will take place at AUBMC. 6 10- Eligibility criteria Inclusion criteria: Lebanese postmenopausal women Non metastatic estrogen receptor positive breast cancer (Stage I-IIIa) On (<6 months) or starting aromatase inhibitor therapy BMD T-score -1.5 OR T-score -1 with > 1 risk factor (age>65, low BMI (<20 kg/m2), family history of hip fracture, personal history of fractures or smoking) OR history of fragility fracture (lumbar spine fracture, hip fracture or ≥ 2 peripheral fractures) OR FRAX calculated MOF risk > age-dependent threshold using the Lebanese FRAX calculator Exclusion criteria: Radiological or clinical evidence of metastasis Other malignancy Chronic conditions that could affect bone turnover (Cushing’s, uncontrolled thyroid disease, osteomalacia, hyperparathyroidism, diabetes mellitus…) Intake of medications that could affect bone turnover (anticonvulsants, bisphosphonates within the past 12 months, HRT within the past 12 months, chronic steroid use for 3-6 months) Liver impairment (LFTs three times upper normal limit) Renal impairment (GFR <35ml/min) Hypocalcemia Hypersensitivity reaction to bisphosphonate 11- Intervention a) Intervention for each group We will contact Fattal & Fils to provide us with zoledronic acid and placebo ampoules manufactured by Novartis. Participants will be randomly allocated in equal proportions to two different interventions administered by a trained nurse in the oncology outpatient department at each of the participating centers. One group will receive an IV infusion of Zoledronic acid 4 mg dissolved in 105mL 0.9% NaCl over 30 minutes at study entry and after 6 months. The other group will receive an IV infusion of Zoledronic acid 5 mg dissolved in 100mL 0.9% NaCl over 30 minutes at study entry and a placebo infusion after 6 months containing 100mL 0.9% NaCl over 30 minutes. All patients will receive 1,000 mg acetaminophen IV 15 minutes before the infusion and will be instructed to take 2 pills (500mg each) every 8 hours thereafter for the following 48 hours to prevent or minimize manifestations of acute reactions. Calcium and Vitamin D supplementation will be encouraged in both treatment arms depending on their dietary intake and baseline 25(OH)D levels. 7 b) Intervention modifications Intervention should be discontinued in any participant experiencing a decline in renal function reaching a GRR <35ml/min confirmed on two consecutive readings. Participants who develop progression of breast cancer to stage >IIIa (locally invasive, or metastatic) or participants who discontinued aromatase inhibitor therapy should be evaluated by their oncologist who would assess the risks and benefits of remaining in the study. All participants discontinuing interventions due to the above criteria, severe side effects or personal request should be followed till the end of the study with assessment of protocol endpoints. c) Adherence Both intervention groups will receive infusions in a hospital setting and therefore adherence to the intervention itself should not be a problem. Participants would be called in advance by the research team and reminded of their infusion appointment one week and one day prior to the actual infusion date. The second infusion will be given after 6 months ± 2 weeks to increase compliance. Participants will also be called one week prior and then one day prior to each visit and reminded of the procedures (blood tests, interview, BMD…) occurring at each visit. Acetaminophen pills will also be provided to participants upon infusion of zoledronic acid, IV acetaminophen will be given before the infusion by the nurse and a box of 12 pills will be given to participants to take following the infusion. The research team will explain the importance of adherence to acetaminophen in decreasing side effects of zoledronic acid. d) Concomitant care Participants will be advised to take vitamin D3 (cholecalciferol) 800 IU/d and/or calcium 1,000 mg/d depending on baseline 25(OH)D levels and dietary intake. Participants should continue to take their home medications. The research team should be made aware of any medication changes particularly initiation of medications affecting bone metabolism such as steroids, antiresorptives, anticonvulsants, chemotherapy and hormone therapy. 12- Outcomes a) Primary outcome: Bone loss at the lumbar spine as measured by DXA scan (BMD) at the lumbar spine expressed as mean percent change from baseline to12 months in both intervention groups. The lumbar spine is thought to be the first site that is most sensitive to sex steroids deficiency and therefore would be more prone to changes with aromatase inhibitors and was therefore chosen as the primary outcome of this study (7). b) Secondary outcomes: BMD and bone markers are surrogates for fractures and are therefore used as secondary outcomes to prove the efficacy of zoledronic acid. - Bone loss at the lumbar spine as measured by DXA scan (BMD) at the lumbar spine expressed as mean percent change from baseline to 6 months in both intervention groups. - Bone loss at the total hip as measured by DXA scan (BMD) expressed as mean percent change from baseline to 12 months in both intervention groups. 8 - Serum levels of osteocalcin expressed as mean percent change from baseline to 12 months in both intervention groups. Serum levels of crosslaps (CTX) expressed as mean percent change from baseline to 12 months in both intervention groups. Fracture rates and adverse events throughout the study. 13- Participant timeline Participants will be approached by their treating oncologist. Those who are interested will meet the research assistant for recruitment and further details: Pre-Screening visit: The research team would explain the study to participants, obtain informed consent and screen for eligibility criteria. Screening visit: Measure weight, height, vital signs, BMD, VFA, TBS, collect blood and urine studies. Blood and urine studies include bone markers, CBC, 25(OH)D, Calcium, Phosphorus, Magnesium, Parathyroid hormone (PTH), hemoglobin A1C, Alkaline phosphatase, liver enzymes, thyroid stimulating hormone (TSH), BUN, Creatinine, and total protein and 24 hours urine collection for calcium, creatinine and sodium. Randomization and Intervention visit: Measure weight, height, vital signs, administer IV zoledronic acid as per randomization protocol, and IV acetaminophen. 3 months visit: Measure weight, height, vital signs and collect blood studies. Blood studies include liver enzymes, creatinine, calcium and bone markers. 6 months visit: Measure weight, height, vital signs, BMD, TBS, administer IV zoledronic acid or IV placebo, and IV acetaminophen and collect blood studies. Blood studies include liver enzymes, creatinine, calcium and bone markers. 12 months visit: Measure weight, height, vital signs, BMD, TBS and collect blood studies. Blood studies at the 3, 6 and 12 months visits include liver enzymes, creatinine, calcium and bone markers. A delay of a maximum of 2 weeks will be allowed between each follow up visit. All visits including a BMD measurement will be done at AUBMC. For other visits (prescreening, intervention and 3 months), each participant will present to their original recruitment center. Blood and urine samples collected in KMC and CMC will be sent to AUBMC for analysis. During each visit, the importance of adherence to the protocol will be highlighted by the research personnel and adverse events would be assessed through questionnaires. Food frequency questionnaire to assess calcium and vitamin D intake along with questionnaires recording demographic and any change in home medications will also be performed at each visit. Height will be measured at each visit, if there is a decrease of 2 cm or more between visits a spine radiograph will be taken to assess for any asymptomatic vertebral fracture. 9 Pre-Screening visit Screening: Baseline BMD, VFA, blood and urine studies Randomization Zoledronic 5mg IV Zoledronic 4mg IV 3 months visit: Follow up, blood studies 3 months visit: Follow up, blood studies 6 months visit: Placebo IV, follow up, blood studies, BMD 6 months visit: Zoledronic acid 4mg IV, follow up, blood studies, BMD 12 months visit: Follow up, BMD, blood studies Figure 1: Flow diagram of the study visits 10 12 months visit: Follow up, BMD, blood studies Table 2: Participants timeline PreScreening -t2 Enrolment Eligibility screen Informed consent Allocation Interventions IV Zoledronic 4mg IV Zoledronic 5mg IV Placebo Assessments Questionnaires Vitals BMD Bone markers LFTs Creatinine Calcium Other labs1 1st visit -t1 Study period Randomization & Intervention t0 3 mo visit 6 mo visit 12 mo visit t1 t2 t3 x x x x x x x x x x x x x x x x x x x x x x x x x x x x x 1full x x x x x x x set of blood studies including CBC, 25(OH)D, Calcium, Phosphorus, Magnesium, Parathyroid hormone (PTH), hemoglobin A1C, Alkaline phosphatase, liver enzymes, thyroid stimulating hormone (TSH), BUN, Creatinine, and total protein and 24 hours urine collection for calcium, creatinine and sodium 14- Sample Size Sample size was calculated for our primary outcome, percent change LS BMD at 12 months using an online calculator (22). Several superiority trials investigated the effect of IV zoledronic acid 4mg twice a year in preventing bone loss at the LS in postmenopausal patients with breast cancer on aromatase inhibitors (18-20, 23). These trials compared zoledronate 4 mg twice a year given immediately when starting AIs to delaying it until a drop in BMD or a fracture occur. Only 13-14% of the patients randomized to the delayed group actually received zoledronate we therefore could consider these trials as comparing zoledronate 4 mg twice a year to placebo (18-20). The difference in percent change LS BMD at 12 months between the two treatment arms were 4.4%, 5.3%, 5.4% and 5.7% in each of these trials (18-20, 23). These differences between arms were significant, we therefore considered that dividing these values by two would give us a non-significant difference (2.2%, 2.65%, 2.7% and 2.85% respectively), to be considered as the non-significant change in our calculations, a method commonly used in non-inferiority trials since it would increase the sample size required by 4 folds and would therefore be more conservative (24). To be more conservative with our sample size calculations, we used the smallest value (2.2%) as the non-significant change (18). Only one 11 study reported the standard deviation of the percent change LS BMD in each arm (4.3% for immediate vs 5.2% for the delayed group) (18). We used the average of these standard deviations (5%) in our calculations. We calculated the sample size based on different scenarios and based on non-significant change ranging between 1 and 2.2% (Table 1). Table 3: Different scenarios for sample size calculation Dinf SD Power 2.2 5 90% 2 5 80% 90% 1.75 Total N N (20% loss to follow up) N (30% loss to follow up) 5% 178 223 255 5% 128 216 160 270 183 309 5 80% 90% 5% 156 280 195 350 223 400 1.5 5 80% 90% 5% 202 382 253 478 289 546 1.25 5 80% 90% 5% 276 550 345 688 395 787 5 80% 90% 5% 396 858 495 1073 566 1226 620 775 886 1 alpha 80% In a double blind placebo controlled trial, postmenopausal women were randomized to receive different doses of denosumab subcutaneously (25). The two optimal doses that provided maximal effect on bone parameters were found to be 30 mg every 3 months and 60 mg every 6 months. The percent change LS BMD at 12 months was 6.7% and 4.6% in these groups respectively (25). The 2.1% difference between these two doses is therefore considered nonsignificant and is very closed to the assumption (2.2%) used in our calculations. Therefore, to perceive non-inferiority between the two groups, with a 2.2% least significant change, 5% standard deviation, 80% power and a type I error of 5%, 64 participants per arm are needed. With a 30% drop out rate we would need 92 patients per arm. If we consider that 50% of patients approached in the clinics will be eligible and willing to enroll in the study, a total of 368 patients should be screened initially. Assuming that only 30% will accept to join the study, 1226 patients should be approached. 15- Recruitment Postmenopausal women with breast cancer on aromatase inhibitor therapy for less than 6 months or to start aromatase inhibitor therapy will be approached by their treating oncologist in the Oncology specialty clinics or outpatient departments at AUBMC, KMC and CMC. Information about the trial will be available at the entrance of each medical center in the form of billboards and in the waiting areas and inside the clinics as English or Arabic flyers and brochures. Oncologists will refer interested patients to the research team for more information, assessment, 12 screening and consent. The research team will approach the oncologists on a weekly basis to monitor the process and the recruitment progress. The recruitment process will extend over 1236 months and might continue further until the sample size is achieved. Methods: Assignment of interventions 16- Allocation a) Sequence generation Participants will be randomly allocated to either one of the intervention groups in a 1:1 allocation ratio. Due to the difference in patient load in the three centers, we will enroll patients from AUBMC, CMC and KMC in a 4:1:1 ratio respectively. We will generate a randomization sequence using restricted fixed permuted block randomization through an online sequence generator for each center separately. The number of blocks and blocks sizes will not be disclosed to insure concealment. Randomization will be stratified by time since menopause (≤ 5 or >5 years) and by steroid use in chemotherapy. Information about the randomization will be available in a separate document with limited access only to the pharmacy. b) Concealment mechanism To ensure concealment, the pharmacy will not check the treatment allocation until the participant undergoes the screening visit and is enrolled in the study. Once the participant is enrolled and presents to the intervention visit, the pharmacy would provide the research assistant with the appropriate IV bag which will then be transported to the research nurse. c) Implementation The statistician will generate the randomization sequence. He will then mail the list to the pharmacy at AUBMC where the list will be stored. The pharmacist is responsible for treatment allocation and concealment. Once an eligible patient is enrolled and presents to the intervention visit, the research team will notify the pharmacist at AUBMC through an email with the participant’s code. The pharmacist will then prepare the appropriate ampoule according to the predetermined sentence and present it to the research assistant in a sealed envelope to be transferred to the nurse performing the infusion. The research assistant is responsible for screening and enrolling eligible participants and transporting the IV bag to the nurse. The research nurse is responsible for performing the infusion. Both the research assistant and nurse will be kept unaware of the allocation. 17- Blinding (Masking) a) Blinding The participants, care providers (PI, treating oncologists and nurse performing the infusion), data collectors (research assistants), outcome assessors and data analysts will be blinded. Pharmacists will prepare unlabeled ampoules similar in size and color for both zoledronate doses (4mg and 5mg) and for placebo. Since one group of participants will receive 13 zoledronate 4mg twice (6 months interval), we will give those in the 5mg once a year group a placebo infusion at 6 months to insure blindness to the treatment. Zoledronic acid infusion is associated with acute phase reaction that occurs within the first 24 hours after the first infusion. The risk of acute reaction decreases with following injections but is not completely eliminated. Both groups are at risk of experiencing acute phase reaction at the first infusion visit since both groups will receive the active drug. At 6 months, participants receiving the placebo infusion will not experience acute phase reaction and will therefore not require acetaminophen while the group who receives treatment will experience side effects and the intervention could therefore be predicted and unblinded. We will therefore provide all participants with acetaminophen pills to be taken every 8 hours for 48 hours following each infusion instead of PRN to ensure blinding especially at the 6 months interventional visit (zoledronic acid 4mg v/s placebo). The lack of side effects could therefore be attributed to the prophylactic intake of acetaminophen rather than placebo infusion, which would limit the risk of unblinding. b) Emergency unblinding We will try to maintain blinding as far as possible to preserve the reliability and quality of our trial. Zoledronic acid infusion is commonly associated with acute phase reaction, and the management of this side effect is not affected by knowing to which arm the participant experiencing it is randomized to. Emergency unblinding will only occur in cases where the treatment of the severe adverse event is affected by the kind of intervention received. The primary investigator should be made aware of all code breaks and contact the pharmacy to receive the allocation information. The principal investigator should also fill an adverse event form. Un-blinding does not necessarily mean discontinuation of treatment and the actual allocation should not be disclosed to other research personnel, participants, data analysts and outcome assessors. Methods: Data collection, management and analysis 18- Data Collection methods a) Plans for data collection and assessment All data will be collected by trained personnel at the American University of Beirut Medical Center. Bone Mineral Density: BMD will be performed at the baseline, 6 months and 12 months visits at AUBMC, a center accredited by the International Society for Clinical Densitometry (ISCD). Lumbar spine and total hip BMD will be assessed by certified technicians using Dual energy Xray Absorptiometry (DXA) scans (Hologic, Horizon A, version 13.6.0.5). As part of the BMD quality control, precision and performance are checked using phantoms and duplicate measures on select patients on a daily basis. In 2018, the coefficient of variation derived from a total of 177 duplicate for the lumbar spine was 0.401± 0.587 and from a total of 202 duplicates fot the total hip was 0.383± 0.243. 14 Crosslaps (C-terminal telopeptides of type 1 collagen): Crosslaps an index of bone collagen degradation will be assessed at the baseline, 3 months, 6 months and 12 months visitis. Fasting serum crosslaps will be measured using ElectroChemiLuminescence ImmunoAssay (ECLIA), with a reference range of 104-1008 ng/mL in postmenopausal women. Intra-assay CV’s are 7.8%, 2.7%, 3.2% and 1.9% at 0.046, 0.292, 0.709 and 2.94 ng/mL respectively. Inter-assay CV’s are 7.7 %, 8.5% and 7.8% at 0.291, 0.679 and 2.77 ng/mL respectively. Osteocalcin: osteocalcin, an index of bone formation will be assessed at the the baseline, 3 months, 6 months and 12 months visits. Fasting serum osteocalcin will be measured using ECLIA, with a reference range of 8.0-55.9 ng/mL in women between 41 and 70 years of age. Intra-assay CV’s are 2.8%, 1.3%, 1.2%, and 1.7% at 1.62, 14.5, 83.4 and 178 ng/mL respectively. Inter-assay CV’s are 2.6 %, 3.2% and 3.9% at 15.8, 87.2 and 186 ng/mL respectively. Other laboratory measurements: A complete blood and urine workup will be performed at the baseline visit including: - 25(OH)D: assessed using ECLIA (Roche Total II) with the following reference range: deficient <10 ng/mL, insufficient 10-25 ng/mL, desirable >25 ng/mL. The inter-assay CVs are 4.1% and 2.5% for 11 and 29.6 ng/mL respectively and the intra-assay CVs are 5.6% and 3% for 11 and 29.6 ng/mL respectively. - Alanine Transaminase (ALT/SGPT): assessed using enzymatic rate spectrophotometry with a reference range of 0-50 IU/L. - Aspartate Transaminase (AST/SGOT): assessed using enzymatic rate spectrophotometry with a reference range of 0-50 IU/L. - Blood Urea Nitrogen (BUN): assessed using Spectrophotometry with a reference range of 8-25 mg/dL. - Calcium: assessed using Spectrophotometry, NM-BAPTA with a reference range of 8.5-10.5 mg/dL. - Complete Blood Count (CBC): assessed using Coulter-principle of counting/Volume conductivity and scatter. - Creatinine: assessed using the enzymatic colorimetric POCT method with a reference range of 0.5-1.0 mg/dL in women. - Magnesium: assessed using the colorimetric-xylidyl blue method with a reference range of 1.6-2.5 mg/dL. - Phosphate: assessed using the ammonium phosphomolybdate complex with a reference range of 2.7-4.8 mg/dL. - PTH: assessed ECLIA with a reference range 15-76 pg/mL. - TSH: assessed using ECLIA with a reference range of 0.27-4.2 µU/mL. - Total serum protein: serum albumin, globulin and total protein are assessed using Spectrophotometry with the following reference ranges: Protein total: 60-83 g/L; Albumin: 36-53 g/L; Globulin: 18-34 g/L. - 24 hours urine calcium: measured using Spectrophotometry, NM-BAPTA with a reference range of 20.0-275.0 mg/24 hour. - 24 hours urine creatinine: measured using the Jaffe rate with a reference range of 0.6-2.0 g/24 hour. 15 - 24 hours urine sodium: measured using Ion-selective electrode with a reference range of 40-220 mmol/24 hour. Questionnaires: An interviewer led questionnaire will be administered at the first visit, for each participant regarding demographic characteristics, medical history, medications, dietary and social habits. These questionnaires will also be filled at each follow up visit to capture any changes in the data previously collected. A validated food frequency questionnaire will also be administered to assess calcium and vitamin D requirements. b) Retention The research team will try to optimize and improve retention and follow up using the following measures: - Study participants will be provided with a calendar for all scheduled study visits. - Study participants will be contacted one week and then one day prior to each visit by phone calls and reminder messages. - Study participants will be constantly reminded of the importance of their adherence to the study protocol at each visit and phone call. - Study personnel will be constantly available for participants in case of any questions or complaints from 8am till 5pm on Monday-Friday. - Study personnel will be flexible in scheduling study visits according to the participant’s preference within 1-2 weeks from their assigned visit date. We would make every effort to coincide our follow up visits with patient’s clinical visits to their oncologists or chemotherapy visits to the center. - Study participants presenting from KMC and CMC will be offered transportation fees. Participants withdrawal is possible for any reason throughout the study. Study personnel will try to resolve the reason of withdrawal whenever possible. For participants who withdraw their consent, data will be collected until consent withdrawal. For those who discontinue or deviate from intervention protocol, data will be collected until the end of the study. All randomized participants who stick to their assigned treatment will be included in the per protocol analysis. 19- Data management Data collected during the study through laboratory measurements and DXA scans done at AUBMC will be transferred from EPIC health care system into a password secured electronic database (RedCap). Password will be changed periodically and only accessible to study personnel. We will assign a specific code for each participant to ensure confidentiality. Demographics and other data collected through questionnaires will be directly entered into tablets to decrease transcription errors and then transferred to the same electronic database and will resemble the paper form approved by the study committees and IRB. Manual entry will be done in duplicate independently by two research assistants to minimize possible data entry errors. The printed data and questionnaires will be locked in a storage only accessible by study personnel and destroyed 5 years after study completion. Data integrity will be improved by performing range checks and checks for missing data periodically. We will also include alarm triggers on RedCap for any data entered outside a pre-set range. In addition, a manual checking of a subset of already entered data will be done periodically to further improve reliability. A 16 complete backup of data will be done twice weekly to insure proper storage of data and avoid losing information. 20- Data analysis a) Outcomes Normality for all variables will be assessed visually using histograms. Baseline demographics and clinical characteristics will be summarized using mean ± standard deviation (or median and range) for continuous variables or frequencies and percentages for categorical variables. These variables will be compared between treatment arms using the independent t-test (or Wilcoxon ranked sum test) for continuous data and the chi-squared test (or Fisher’s exact test) for categorical data. Any imbalances between these variables will be adjusted for in the primary analysis of this study. The primary analysis will consist of comparing the primary outcome, the percent change in lumbar spine BMD at 12 months between the two treatment arms using the independent t-test (or Wilcoxon ranked sum test). 95% confidence interval will also be calculated and IV zoledronate 5mg will be considered non-inferior to the 4mg dose if the confidence interval lies below our non-inferiority limit of 2.2%. Secondary outcomes including percent change in lumbar spine BMD at 6 months, percent change in total hip BMD at 12 months, percent change osteocalcin at 12 months and percent change Crosslaps at 12 months will also be compared between treatment arms using the independent t-test (or Wilcoxon ranked sum test). Adverse reactions and fracture rates will be compared between arms using the chi-squared test (or Fisher’s exact test). 95% confidence interval will be calculated for continuous variables and relative risks will be calculated for categorical variables. Analysis will be carried out using SPSS version 25.0 (IBM, USA) and p-value<0.05 will be considered statistically significant. We will no adjust p-value for secondary outcomes. b) Additional analyses We will perform subgroup analyses according to variables that may affect bone metabolism. We will compare percent change lumbar spine BMD at 12 months according to time from menopause, time from start of AI therapy and type of chemotherapy received (especially if steroids were used). We will also adjust our primary analysis for any imbalances in baseline characteristics using linear regression analysis for continuous outcomes. We will perform paired t-test (or Wilcoxon signed rank sum test) to compare the percent change in lumbar spine BMD, total hip BMD, Osteocalcin and Crosslaps at different time points (baseline, 3 months, 6 months and 12 months) within each treatment group. c) Analysis population and missing data The primary analysis will be a Per Protocol analysis, meaning that participants who deviate from protocol will not be analyzed and only participants who receive the treatment assigned to them at the beginning of the study will be included in the analysis. Per Protocol analysis is the preferred analysis for non-inferiority trials (26). In case of missing data, we will include participants with complete data in our final analyses. We will compare characteristics of participants with complete data to those of participants with missing data or who were loss to follow up. We will perform multiple 17 imputation methods (using linear regression, the last reading carried forward or the means of the missing variables) and compare analyses using these imputations to those resulting from participants with complete data. Adverse events will be collected and analyzed in all randomized participants regardless of adherence to protocol. Methods: Data collection, management and analysis 21- Data monitoring a) Formal committee The study investigators will appoint a Data Safety Monitoring Board (DSMB), which will include experts from various disciplines (clinical experts in endocrinology and oncology, a biostatistician, a patient advocate and a bioethicist), independent of the trials’ investigators and sponsors. The role of this committee is to review and approve the protocol, to monitor safety and effectiveness of the trial, to make sure that all adverse events are clearly documented, to review the trial’s conduct and to evaluate any emerging problems and suggest solutions. This committee also assessed serious adverse events and their relation to the intervention. This committee will meet every 6 months to monitor the progress of the trial. After each meeting, the DSMB will contact the study sponsor and the investigators and provide them with its observations and recommendations as to continuation, modification or termination of the trial. This committee can also request a number of additional interim analyses. b) Interim analysis An interim analysis will be planned when half of the total sample size has been randomized and completed the 12 months visit with BMD measurement. The interim analysis will be performed by an independent blinded statistician using independent t-test to compare the primary outcome between the two treatment arms. Since we only plan to perform one interim analysis, we will not adjust the p-value for our primary outcome. The statistician will then share the results with the DSMB. The DSMB will have access to unblinded data and will then give recommendations on continuing, stopping or modifying the trial accordingly. The steering committee will decide on the continuation of the trial. 22- Harms Data on adverse events will be collected at each study visit by the study personnel. Participants will be asked to immediately contact the study team to report any adverse event that occurs between visits. Participants will be called 24 hours after the infusion to document any adverse event. An adverse event is any “untoward medical occurrence associated with the use of a drug in humans, whether or not considered drug related defined by symptoms and signs associated with the intake of a medication”(27). All cases will be recorded in “an adverse event record form” which will be assessed based on its severity, anticipation and relation to the study drug by the investigators. We will also assess whether any intervention was done to treat the adverse event and its resolution. Serious adverse events are life threatening, require hospitalization, cause severe impairment or result in death. All adverse events will be reported to the DSMB and the Institutional Review Board (IRB) as soon as possible within no more than 5 days of its occurrence. In our study, we expect that some participants will have acute phase reaction to IV 18 zoledronic acid a well-known a common side effect of the infusion. This reaction includes fever (17.2%), chills (4.4%), flu-like illness (7.8%), myalgia and arthralgia (15.7%) and headache (5.8%) that occur within the first two days after the infusion (28). Rare side effects include osteonecrosis of the jaw (1%), atrial fibrillation (1.3%) and atypical femoral fracture (2.3/10,000) (29). 23- Auditing The study investigators will meet with the research assistants on a weekly basis and will audit all CRFs and consent forms. They will also audit data collected on 10% of participants during that week. The investigators along with the will designate independent members for auditing. The auditing members will plan at least one onsite visit to each center participating in the study during the trial period. Each site will be notified 2-3 weeks prior to the monitoring visit to ensure the availability of the research personnel on the scheduled date. During this visit, the monitor will evaluate and review the accuracy of the data collection and entry and adherence to protocol. The monitor will also review all documents and make sure that the regulatory binder is complete and up to date. The monitor will raise any problem identified and assist the center in solving the issue. If violations are found during these visits, research personnel will be offered a more extensive training and another auditing process will be performed at a later time to ensure resolution of the violations. Ethics and dissemination 24- Research ethics approval The final protocol along with the consent forms and all related documents (SOPs, CRFs, advertisement materials…) will be submitted and reviewed by the IRB at AUBMC with regards to compliance with human subjects regulations. The trial will not be implemented before obtaining the IRB approval from each site. The IRB will then review the protocol at least annually and the principal investigators will also submit progress reports to the IRB including the number of participants and the DSMB reviews and decisions. 25- Protocol amendments After approval, any modifications to the protocol that could affect the conduct of the study or patient safety will be submitted to the IRB as a formal amendment to the protocol prior to implementation. These modifications include changes to the design, analysis, sample size, outcomes, eligibility criteria and outcomes. The primary investigator will notify the IRB of any minor changes that have minimal effect on study conduct. A list of the amendments will be stored by the principal investigator to track these changes. Amendments of the protocol will also be communicated with the trial sponsor and updated on the trial registries. 26- Consent or assent a) Consent The oncologists will introduce the study to their eligible patients during their follow up visits. Interested patients will be approached by a trained research assistant who will explain the trial protocol in a lay language in a private room. The research assistant should make sure that the 19 patients understand he trial and that their participation is voluntary and that they can withdraw from the trial at anytime. Patients will then be able to make an informed decision and participants who are willing to participate will sign the informed consent or take it home to review it and make a decision on their own. All participants will receive a copy of the signed informed consent. All consent forms will be available in English or Arabic whichever each participant prefers. Participants will be informed that the withdrawal of their consent is possible at anytime. b) Ancillary studies Additional blood will be collected and stored for use in future studies. Participants will be able to opt or decline permission for the use of their specimens for any future protocol, or request to be contacted in the event their stored specimens are to be used for any future studies. 27- Confidentiality All study visits will take place in private rooms. All study files (consent forms, test results…) will be stored in a locked compartment only accessible by the research team. All information to be entered in the databases will be de-identified and labeled with a code specific to each participant to ensure confidentiality. These databases will be secured by passwords with restricted access to research personnel only. One master sheet with all participants names and corresponding codes will be available with restricted access. Participant’s study information will not be released without permission. 28- Declaration of interests The investigators report no conflict of interest. 29- Access to data The principal investigator will have access to the full clean trial dataset with the de-identified data. Co-investigators will have access to their own site’s datasets and will have access to other sites data by requesting from the principal investigators. Access to data will be password protected. 30- Ancillary and post-trial care We do not expect any significant adverse event resulting from zoledronic acid infusion. Some participants may develop acute phase reaction which rarely necessitates hospitalization. In case of any adverse event as a result of the study, there will be no compensation to cover these expenses in case it is not covered by third party or governmental insurance. During the trial, we will share results of blood work and tests with those who request it. However, results of our outcomes (BMD and bone markers) will not be shared until the end of the trial to prevent any contamination with co-interventions. Once the study is completed and analyses are performed, participants will be contacted by the research team and asked whether they would like to know their individual results. 31- Dissemination policy 20 a) Trial results The main investigators will review all papers and abstracts before publication. Trial results will be communicated to participants, participating physicians from all study sites, health care professionals and the public in Lebanon one year after completion of the trial in meetings and conferences. Results will be published in a peer-reviewed medical journal and will be presented in conferences and meetings. b) Authorship Individuals who fulfill the International Committee of Medical Journal Editors (ICMJE) criteria for authorship will be mentioned as contributing authors. These include contribution to the design, analysis and interpretation of the data, drafting or revising manuscripts, approval of final manuscripts and being accountable and responsible for the integrity of the data (30). c) Reproducible research Five years after the completion of analyses on our primary and secondary outcomes we will share a completely de-identified data set with the public in an appropriate data archive for use by other researchers. Appendices 32- Informed consent materials (to be developed) 33- Biological specimens Additional blood will be collected and stored with the specific participant code for use in future studies. References 1. Tao Z, Shi A, Lu C, Song T, Zhang Z, Zhao J. Breast Cancer: Epidemiology and Etiology. Cell Biochem Biophys. 2015;72(2):333-8. 2. Hortobagyi GN, de la Garza Salazar J, Pritchard K, Amadori D, Haidinger R, Hudis CA, et al. The global breast cancer burden: variations in epidemiology and survival. Clin Breast Cancer. 2005;6(5):391-401. 3. Fares MY, Salhab HA, Khachfe HH, Khachfe HM. Breast Cancer Epidemiology among Lebanese Women: An 11-Year Analysis. Medicina (Kaunas). 2019;55(8). 4. Board PDQATE. Breast Cancer Treatment (Adult) (PDQ(R)): Health Professional Version. PDQ Cancer Information Summaries. Bethesda (MD): National Cancer Institute (US); 2002. 5. Ball S, Arevalo M, Juarez E, Payne JD, Jones C. Breast cancer chemoprevention: An update on current practice and opportunities for primary care physicians. Prev Med. 2019;129:105834. 21 6. Yao LT, Wang MZ, Wang MS, Yu XT, Guo JY, Sun T, et al. Neoadjuvant endocrine therapy: A potential strategy for ER-positive breast cancer. World J Clin Cases. 2019;7(15):1937-53. 7. Perez EA, Weilbaecher K. Aromatase inhibitors and bone loss. Oncology (Williston Park). 2006;20(9):1029-39; discussion 39-40, 42, 48. 8. Hadji P. Aromatase inhibitor-associated bone loss in breast cancer patients is distinct from postmenopausal osteoporosis. Crit Rev Oncol Hematol. 2009;69(1):73-82. 9. Eastell R, Hannon RA, Cuzick J, Dowsett M, Clack G, Adams JE. Effect of an aromatase inhibitor on bmd and bone turnover markers: 2-year results of the Anastrozole, Tamoxifen, Alone or in Combination (ATAC) trial (18233230). J Bone Miner Res. 2006;21(8):1215-23. 10. Hong AR, Kim JH, Lee KH, Kim TY, Im SA, Kim TY, et al. Long-term effect of aromatase inhibitors on bone microarchitecture and macroarchitecture in non-osteoporotic postmenopausal women with breast cancer. Osteoporos Int. 2017;28(4):1413-22. 11. Lee SJ, Kim KM, Brown JK, Brett A, Roh YH, Kang DR, et al. Negative Impact of Aromatase Inhibitors on Proximal Femoral Bone Mass and Geometry in Postmenopausal Women with Breast Cancer. Calcif Tissue Int. 2015;97(6):551-9. 12. Shapiro CL, Van Poznak C, Lacchetti C, Kirshner J, Eastell R, Gagel R, et al. Management of Osteoporosis in Survivors of Adult Cancers With Nonmetastatic Disease: ASCO Clinical Practice Guideline. J Clin Oncol. 2019:Jco1901696. 13. Hadji P, Aapro MS, Body JJ, Gnant M, Brandi ML, Reginster JY, et al. Management of Aromatase Inhibitor-Associated Bone Loss (AIBL) in postmenopausal women with hormone sensitive breast cancer: Joint position statement of the IOF, CABS, ECTS, IEG, ESCEO IMS, and SIOG. J Bone Oncol. 2017;7:1-12. 14. Reid DM, Doughty J, Eastell R, Heys SD, Howell A, McCloskey EV, et al. Guidance for the management of breast cancer treatment-induced bone loss: a consensus position statement from a UK Expert Group. Cancer Treat Rev. 2008;34 Suppl 1:S3-18. 15. Lomax AJ, Yee Yap S, White K, Beith J, Abdi E, Broad A, et al. Prevention of aromatase inhibitor-induced bone loss with alendronate in postmenopausal women: The BATMAN Trial. J Bone Oncol. 2013;2(4):145-53. 16. Van Poznak C, Hannon RA, Mackey JR, Campone M, Apffelstaedt JP, Clack G, et al. Prevention of aromatase inhibitor-induced bone loss using risedronate: the SABRE trial. J Clin Oncol. 2010;28(6):967-75. 17. Sestak I, Singh S, Cuzick J, Blake GM, Patel R, Gossiel F, et al. Changes in bone mineral density at 3 years in postmenopausal women receiving anastrozole and risedronate in the IBIS-II bone substudy: an international, double-blind, randomised, placebo-controlled trial. Lancet Oncol. 2014;15(13):1460-8. 18. Brufsky A, Harker WG, Beck JT, Carroll R, Tan-Chiu E, Seidler C, et al. Zoledronic acid inhibits adjuvant letrozole-induced bone loss in postmenopausal women with early breast cancer. J Clin Oncol. 2007;25(7):829-36. 19. Llombart A, Frassoldati A, Paija O, Sleeboom HP, Jerusalem G, Mebis J, et al. Immediate Administration of Zoledronic Acid Reduces Aromatase Inhibitor-Associated Bone Loss in Postmenopausal Women With Early Breast Cancer: 12-month analysis of the E-ZOFAST trial. Clin Breast Cancer. 2012;12(1):40-8. 20. Coleman R, de Boer R, Eidtmann H, Llombart A, Davidson N, Neven P, et al. Zoledronic acid (zoledronate) for postmenopausal women with early breast cancer receiving adjuvant letrozole (ZO-FAST study): final 60-month results. Ann Oncol. 2013;24(2):398-405. 21. Bundred NJ, Campbell ID, Davidson N, DeBoer RH, Eidtmann H, Monnier A, et al. Effective inhibition of aromatase inhibitor-associated bone loss by zoledronic acid in 22 postmenopausal women with early breast cancer receiving adjuvant letrozole: ZO-FAST Study results. Cancer. 2008;112(5):1001-10. 22. Ltd SE. Power (sample size) calculators 2019 [Available from: https://www.sealedenvelope.com/power/continuous-noninferior/. 23. Wagner-Johnston ND, Sloan JA, Liu H, Kearns AE, Hines SL, Puttabasavaiah S, et al. 5year follow-up of a randomized controlled trial of immediate versus delayed zoledronic acid for the prevention of bone loss in postmenopausal women with breast cancer starting letrozole after tamoxifen: N03CC (Alliance) trial. Cancer. 2015;121(15):2537-43. 24. Jones B, Jarvis P, Lewis JA, Ebbutt AF. Trials to assess equivalence: the importance of rigorous methods. BMJ. 1996;313(7048):36-9. 25. McClung MR, Lewiecki EM, Cohen SB, Bolognese MA, Woodson GC, Moffett AH, et al. Denosumab in Postmenopausal Women with Low Bone Mineral Density. New England Journal of Medicine. 2006;354(8):821-31. 26. Detry MA, Lewis RJ. The intention-to-treat principle: how to assess the true effect of choosing a medical treatment. Jama. 2014;312(1):85-6. 27. NIH (National Heart LaBI. NHLBI Adverse Event and Unanticipated Problem Reporting Policy 2014 [Available from: https://www.nhlbi.nih.gov/grants-and-training/policies-andguidelines/nhlbi-adverse-event-and-unanticipated-problem-reporting-policy. 28. Reid IR, Gamble GD, Mesenbrink P, Lakatos P, Black DM. Characterization of and risk factors for the acute-phase response after zoledronic acid. J Clin Endocrinol Metab. 2010;95(9):4380-7. 29. Kotian P, Boloor A, Sreenivasan S. Study of Adverse Effect Profile of Parenteral Zoledronic Acid in Female Patients with Osteoporosis. J Clin Diagn Res. 2016;10(1):OC04OC6. 30. Editors ICoMJ. Defining the Role of Authors and Contributors 2019 [Available from: http://www.icmje.org/recommendations/browse/roles-and-responsibilities/defining-the-role-ofauthors-and-contributors.html. 23