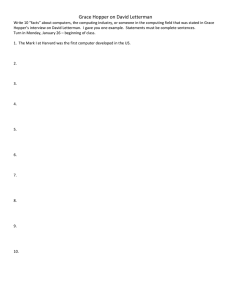
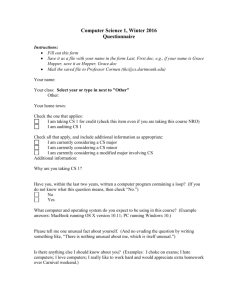
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/347512520 Error Risk Reduction: Concept and Case Study Article · December 2020 CITATIONS READS 0 805 1 author: Tim Sandle The University of Manchester 736 PUBLICATIONS 1,286 CITATIONS SEE PROFILE Some of the authors of this publication are also working on these related projects: Laboratory Management View project Pharmaceutical product recalls View project All content following this page was uploaded by Tim Sandle on 21 December 2020. The user has requested enhancement of the downloaded file. Error Risk Reduction: Concept and Case Study Tim Sandle Introduction This paper is concerned with human error and error risk reduction, centered on two case studies. Human error has long been identified as a contributing factor to incident causation, and pharmaceuticals and healthcare is no exception (1). Human error is a cause of substantial variation across the sector, impacting upon quality. To a degree it can be prevented by analyzing process for failure modes and implementing better training, clearer documentation and by increasing automation. Hence, no root cause investigation should end by concluding ‘human error’. With the first case study, during the filling of a batch of an aseptic liquid product a change of the receptacle used for holding rubber stoppers (a ‘hopper’) was carried out within the aseptic processing area. After unloading the stoppers, three clamps, three seals and a stainless steel ‘T’ piece were found to have been left inside the hopper. A deviation report was raised, and an investigation performed in order to examine the reason why the error happened and with a view to prevent the error from happening again. The process followed falls within the general approach of error risk reduction. Error risk reduction is associated foremost with human error and the ways to reduce the impact of human error on procedures and processes. With this approach, it is important that the people carrying out the assessment should understand the different types of failure and the factors that make them more or less likely to occur. The second case study looks at batch record errors, where the lesson to be learned is focused at the design stage. Both case studies draw om the human factors approach, which is discussed below. In terms of what an error is, there are competing definitions and understanding of ‘error’. It follows that the reason for errors occurring is a contested concept. In the context of this article, errors will be considered as divergences of events from (expected) standards. This fits in neatly with the GMP context. One of the common mistakes is that there is ‘no such thing as human error’ or ‘regulators will not accept human error’. This is not correct. It is possible for mistakes, errors, slips, or lapses to occur, and these describe one immutable aspect of the human condition: to err is human. However, the investigation process into an issue should not end here. It is necessary to find the root cause for the error, the underlying issue, the factor, or the context that caused the issue to arise in the first place. What is error? There are two schools of thought in relation to human error: the person and the system approaches. These can be defined as (2): • The person approach focuses on the errors of individuals, blaming them for forgetfulness, inattention, or moral weakness. This understanding of human error is • more generally connected with moral, cultural and religious perceptions of human frailty. The system approach concentrates on the conditions under which individuals work and tries to build defenses to avert errors or mitigate their effects. This approach has received considerable examination in terms of organizational theory and the sociology of work. An example is with the human factors approach, which is discussed below. There are different ways to classify an ‘error’ (3). One way of doing so is to divide error into ‘mistakes’ and ‘slips’ (and error itself is not the same as a deliberate act of not going something that should be done, such as committing fraud). As to how these concepts of ‘mistakes’ and ‘slip’ might be distinguished, Norman explains: "The division occurs at the level of the intention: A Person establishes an intention to act. If the intention is not appropriate, this is a mistake. If the action is not what was intended, this is a slip (4)" The author also identifies errors caused by an interface, as with a computer system; and scenario errors, where the activity has a degree of artificiality about it. Generally, as this article focuses on, mistakes can be addressed through revisions to procedures and training. Slips, on the other hand, are the result of an influencing factor. Slips can be described as: "most likely to occur (a) when we must deviate from a routine, and automatic processes inappropriately override intentional, controlled processes; or (b) when automatic processes are interrupted - usually as a result of external events or data, but sometimes as a result of internal events, such as highly distracting thoughts (5)." Human error and pharmaceuticals Human error will occur in pharmaceutical production as much as it will occur in other regulated sectors, although hopefully this will be at a rate lower than sectors where controls and regulations are less exacting or where the impact of the error matters less. In fact, regulations expect human error to occur, as with CFR 211.22 which states that: “[the quality control unit has]…the authority to review Production records to assure that no errors have occurred or, if errors have occurred, that they have been fully investigated.” Similar phrasing is apparent in EU GMP. For example, in Chapter 14 (part xiv) it is stated: “Where human error is suspected or identified as the cause, this should be justified, having taken care to ensure that process, procedural or system-based errors or problems have not been overlooked, if present…” While these regulations acknowledge human error, it does not expect the process to end simply with the acceptance of error. It is expected that the error is investigated, as the error itself is rarely the root cause of the failure. Invariably some system or process is at fault, leading to the error occurring (hence human error should be recognized as an outcome of combined factors). This requires addressing through a correction and a preventative action, aimed at seeking avoidance of the error in the future (6). The IVT Network have a useful ‘Voices In Validation’ featuring James Vesper, which takes an in-depth look into root cause analysis (7). Techniques like the iterative questioning approach – the 5-Whys – can help to unpick the underlying reasons for employee errors and crystalize what needs to be done to correct the triggers for errors. For example (8): • • • • • • • • • • Human Error? Accidental – why? Application of a bad practice for the right reason- why? Wrong tool/ equipment-why? Improvisation in unfamiliar circumstances-why? Omitting, forgetting or losing place-why? Distracted at a critical point-why? Incorrect assumption or perception-why? Common practice not to follow procedure for that step-why? Lack of appreciation on importance of following procedure-why? This approach alone may lead to changes, or it might be that a more detailed error risk reduction approach is required. In terms of making changes, examples include: • • • • • • Improved change management Review of training The inclusion of refresher training Intruding employee mentoring systems Ensuring procedures are in place to handle complex situations Putting in place the supervision of key activities Error risk reduction Human error is a persistent challenge even for companies with successful continuous improvement procedures. Even experienced people working with established processes can make occasional errors, and such errors can be costly. Typical responses to human errors include retraining; increasing the number of checks or sign offs required; or even the issuing of warnings to staff. These generally produce disappointing results because they do not address the underlying causes of the errors (9). Time spent on error risk reduction allows an organization to (10): • • • Identify the causes of error in an organization’s operations, Provide managers with the necessary tools for preparation and understanding of outcomes, Provide the organization with the tools necessary to implement and sustain continuous error risk reduction improvements. Most approaches to human error are qualitative; however, a quantifiable approach can be used. Here this can take the form of (11): Human error probability (HEP) = Number of times an error has occurred / Number of opportunities for an error to occur The case study in this paper is qualitative. With this, the approach is: 1. Identify the human failures that could be made in the task which might lead to an incident and the performance influencing factors that make those failures more or less likely to occur. 2. Identify appropriate control measures which prevent or mitigate the human failures that have been identified. 3. Where possible aim to design out the potential for human failure and design in the potential for recovery should human failure occur. This includes design of the plant, system, environment and task, taking into account the needs and capabilities of users. Reliance on procedures and training are unlikely to be sufficient. Change the ‘performance-shaping factors’ (PSFs). 4. Check the control measures work. Regularly review your risk assessment to see if any further improvements can be made. The use ergonomics/ engineering judgment and redesign is useful. Such analysis can reveal subtleties like more errors occurring close to the end of a shift of at the changeover of shifts. Improvement measures can include finding better ways to communicate between staff leaving at the end of their shift and with new staff joining at the start of a new shift. From a different standpoint, it could be that the analysis of operations reveals that certain operations are best executed using two, and that using two operators in place of one is necessary as an error prevention mechanism. With procedures, improving procedures is an iterative process and there is a balance to be struck between sufficient detail and straightforward, easy-to-follow instructions, and with the linking procedures to effective training. According to Gallant, it is useful to ask (12): • • • • • Did the procedure specifically require the step to be performed? Does the procedure reflect the actual process? Can the process really be executed by the number of personnel described? Did the procedure describe how the step should be performed? Do the procedure and the way the operation is being performed match? In considering the process or procedure, it is important to consider the environmental context. Is the environment suitable for a person to concentrate in, or do special measures need to be taken to enable a person to concentrate? Influencing factors here could be excessive noise, or areas that are too hot or too cold. Everyday complex and stressful real-life situations can overwhelm the human brain leading to distraction or a failure to able to accurately evaluate the situation and persists in irrational actions or strategies. Preventative actions need to be appropriate, based on some form of error classification. For instance, training and competency can be an effective prevention and mitigation control for mistakes made while planning an action (that is some form of knowledge-based or rule-based mistake). Running simulations, as an example, can help to improve training and to reduce error rates (13). However, this form of preventative measure is generally less effective for skill-based errors of the type that occur during action execution (such as slips of action or memory lapses). To identify the relative risks of potential errors, some form of systematic approach is required. One such approach is based on human factors. Human factors approach The approach taken to human factors in risk assessment should be proportionate to hazards that the organization faces. For most industries a qualitative approach will be sufficient for this type of analysis (14). Human factors derives from the problems of designing equipment operable by humans during World War II. The types of ‘human failures’ or ‘human factors’ that can lead to error include (the list is not exhaustive): • • • • • • • • • • • • • • • • • • • • • • • • • • • • Impatience Limited memory Limited concentration Changes in mood The need for motivation Prejudices Fears Misjudgment Near-sightedness Color-blindness Distraction The ability only to perform a limited number of concurrent tasks Short-term memory, which works differently than long-term memory Appreciating all users are all different Thinking in terms of ideas composed of words, numbers, multimedia, and intuitions. Fatigue The need to both see and hear to fully understand Avoiding presenting information in more than sets of threes The need for complex information to be presented hierarchically Requiring practice to become good at doing things Resistance to change Concern that a person could be physically harmed by some tasks People often prefer to learn by doing than by explanation Missing details when tasks are memorized and performed cursorily Can be affected by socio/political climate. Constrained by time Require tasks to be modularized in order to work in groups Associating unrelated things Systems, process, procedures, training, environmental context and so on each need to be considered to address those factors appropriate to a given situation and hence may be connected to the chance of error. Of course, this is not inferring that some element of personal discipline is not required (15). Once steps 1 to 4 have been followed, the final task is to reassess the system risk level and iterate until the risk is acceptable. This concerns ‘error risk reduction’. Error risk reduction Error risk reduction is sometimes used as part of a wider ‘human reliability assessment’, which embraces: • • • Human error identification – to identify what errors can occur, Human error quantification – to say how likely the errors are, Human error reduction – to improve human reliability. Underpinning error risk reduction is the presumption that human failure is normal and predictable and hence it can be identified and managed. This means that the pharmaceutical and healthcare sectors should tackle error reduction in a structured and proactive way. This means identifying poorly designed activities might be prone to a combination of errors. Perhaps the best way to do this is to involve workers in the design of tasks and procedures. Whilst a proactive approach is best, there will also be circumstances where a reactive approach is required to investigate an error and to identify the root cause so that a corrective action can be set (16). Such incident investigations should seek to identify why individuals have failed rather than stopping at ‘operator error’. Making changes such as introducing labelling and color coding; ensuring any distractions are removed so that the employee can undertake complex work tasks; and considering where an automatic device can be used which makes it impossible for an error to occur, represent the types of changes that can be implemented from error risk reduction exercises. Human reliability assessment can be used to integrate ‘human factors’, like human error, into risk assessments. The assessment of human factors differs slightly to classic approaches to risk assessment, as shown in Table 1. Human Factors Approach Task analysis Human error identification Error representation Human error quantification Human error reduction Risk Assessment System analysis Hazard identification Risk modeling Risk assessment Risk reduction Table 1: Differences between the human factors approach and the standard approach to risk assessments. What error risk reduction should avoid is concluding the following: • • • • • Treat operators as if they are superhuman. Assume that an operator will always be present, be able to detect a problem and immediately take appropriate action. Rely on operators being well-trained, when it is not clear how the training provided relates to prevention or control. Rely on training to effectively tackle slips/lapses. State that operators are highly motivated and thus not prone to unintentional failures or deliberate violations. • • • Ignore the human component completely and failing to discuss human performance at all in risk assessments. Inappropriately apply techniques, such as detailing every task on site and therefore losing sight of targeting resources where they will be most effective. In quantitative risk assessment, provide precise probabilities of human failure (usually indicating very low chance of failure) without documenting assumptions/data sources. This is because such conclusions will not result in the error being addressed and the mistake or slip could reoccur. Building a focused workplace culture The workplace culture and influence how well an organization operates and how a employee is feeling. The totality of employee beliefs, values, unwritten rule, are influencing factors upon employee behavior. When these factors are out of synchronicity, they can create conditions whereby errors are more likely. Central to the appropriate culture is strong communication. Often messages need to be delivered in different forms and at different times. Moreover, there can be a benefit in repeating and confirming instructions to create clarity and to avoid confusion. Using human factors for preventative actions Once analysis has taken place, the proactive approach is to identify different error types and consider how they can be addressed. A genetic example is as per Table 2 (17): Table 2: Classification of errors Type of error Eliminate / Action Mistake Competency assurance Slip Memory lapse Prevent Communication conventions Reduce Software interface logic and layout Design for tactile Confirm action Error differentiation prompt management training Checklist Independent Alert/Alarm check system Mitigate Automate process the Automate process the Automate process the Case study #1 With this case study, of material found inside the device for holding, sterilizing and transferring stoppers, the organization had six hopper devices. Following use, the hoppers are sent for cleaning and preparation by personnel in the technical services department. For this, the hopper is taken from an interlock area that separates technical services from the aseptic filling area (a transfer from an ISO class 7 to an ISO class 8 cleanroom [operational states]). Once in the technical services area two filters, stainless clamps, triclover seals, stainless ‘T’ piece and tray are removed from each hopper. The hopper and components are then manually rinsed using Water for Injection Bulk (WFI). The components are placed in the hopper and dried inside a drying oven. This is shown in figures 1 and 2. Figure 1: After cleaning the components are left in the hopper during drying. Figure 2: The hopper tray is washed and placed back into the hopper during drying. The investigation into how the error occurred was subject to an analysis of Risk Influencing Factors. Such an analysis is integral to the Error Risk Reduction Process. The exercise identified the following: Process Risk Influencing Factors a) There was no formal process in place for the stripping of the hopper and for the washing and drying of the components. This meant that an informal process was used. Therefore, process reliability and consistency of application was not assured. b) Individuals used their own sequence. This was shown to cause ambiguity, especially if task is handed over between staff during shift change-overs. c) The process was not standardized. Here individuals were adapting the basic method in order to achieve the required outcome in their own way. The exact characteristics of outcome and confidence in consistency were shown to depend upon who executes the task. d) There was also a danger of people working on ‘autopilot’ when the task became ‘second nature’. The consequence of this was that minimum monitoring fails to detect something wrong unless it conflicts strongly with what is expected. Information Risk Influencing Factors a) It was discovered that there was an inappropriate level of detail in documentation. This meant that too little information led to assumptions were being used to fill gaps. b) The instruction was not visible in workplace, resulting in dependence on memory. c) Which staff carry out which function was not specified meaning that some actions were not taken by anyone. The obvious corrections here were to add appropriate level of detail to the relevant batch processing record and to the Standard Operating Procedure. Supervisors needed to ensure that instructions were visible. Importantly, clear documented instructions decrease dependence on memory. Resource Risk Influencing Factors a) It was noted that processes with differing requirements share a nearby workspace. This was found to increase risk factors arising on one process to be imposed on others. Distracting factors included noise and concentration. Sounds can lead to interruption or distraction from task. The correction here was to limit the number of different processes sharing the same workspace and to organize individual tasks to limit the risk of one process being imposed on another. Task segregation was used to achieve this. Competence Risk Influencing Factors a) It was found that staff training did not cover all aspects of processes, therefore, increasing risk of error. b) Competence on some tasks was assumed to extend to all others meaning that specific competence deficits were not identified or addressed. c) There was no specific training for individual tasks. Instead it was assumed that staff only needed ‘common sense’. d) There was also a degree of complacency among some personnel, with experienced staff seeing the job as very routine with only a low perceived risk. To address these, deficiencies in competence were assessed and specific training, for each individual task, associated with the cleaning, preparation and autoclaving of the hopper was implemented. Supervisors also re-enforced the need for a visual check of the hopper to address specific competence deficit. Good Practice Risk Influencing Factors Upon review, some examples of best practice were found to be with the implementation of a formal process to ensure that the hopper is checked before autoclaving. The previous practice was that the checking of the hopper, to ensure it is empty, was not formalized. It was agreed that it was necessary to reinforce the importance of a visual check. A revised procedure was required to ensure that the process steps were consistent, including documented evidence of a check taking place. This had the added benefit of preventing ambiguity if the task is handed over. Supervisors also undertook to ensure all team members are informed of the implications of performing the task incorrectly. Overall review At the end of the error risk reduction exercise, the following measures were put into place: 1. A separate hopper tray and components from hopper prior to going into the oven were put into practice. Designated drying ovens to dry the hopper tray and components were used. This ensured that no hopper ‘parts’ were left in the hopper during the drying process. 2. Stainless steel storage baskets were purchased to store hopper tray and components in. These were labeled to identify the components from each individual hopper. 3. Permanently labeling the tray, clamps and T piece. These were labeled with the hopper number. Therefore, assigning the parts to an individual hopper. 4. Adding an operator check on batch record. This included the requirement for a visual check to ensure the hopper is empty of components prior to going into the autoclave. 5. An update the appropriate Standard Operating Procedure to inform the operator to visually check the hopper before it enters the autoclave. 6. The retraining of all Personnel in the area to ensure the new procedure is followed. Reinforce the importance of visually checking the hopper prior to sterilization. With training, often a different approach needs to be taken as simply running the same training may not be effective (on the basis of ‘why didn’t it work the first time?’). Drawing on Gallant again, an effective review of training procedures should involve posting the following questions: • • • • • Did the training reflect the procedure content – and are all operators performing the task doing it the same way? Was it the operator’s first time performing the task independently? Were they allowed enough practice on the task, or was training rushed? Was training time used for appropriate training activities? Did the trainer verify the operator’s ability to perform each required element of the task? Against what standard? Is all the information the trainee needs to perform the task correctly accessible to them? Did the trainer teach them the correct way to do the task? Did the trainer have the knowledge and skills required to teach it? Case Study #2 The second case study considers pharmaceutical batch records. As a pharmaceutical product is manufactured, information relating to the batch manufacturing activity needs to be recorded. It is essential that everything is either written down or digitally captured, to enable the person tasked with batch release to undertake their duties in a compliant manner. Batch documentation needs to be reviewed at key steps to confirm, for example, compliance with GMP, procedures, specifications and licenses. This can be carried out in conjunction with Quality by design approaches, in relation to equipment and workspace optimization (18); process can also be designed so they are more continuous and less error-prone (19). In addition, space should be provided in the documentation to record any comments required to be brought to the attention of the reviewing manager. When comments are necessary, this should include information like: • • • • The nature of the issue. The reason it is or is not considered a concern. Reference to any deviation report (which must describe corrective action taken). Any preventive action taken or planned. Each review stage should be signed by the reviewer and dated. If errors or omissions are found, then the record must be completed and/or corrected by the relevant staff members. At the end of the last process stage/test, or as soon as practically possible, a supervisor or manager should review the record for at least the following: • • • • • • • Completion (that the process/test was satisfactorily completed and all required entries present) and accuracy (batch numbers and dates, etc. are correct). Compliance to procedure, specification and GMP. That critical parameters have been met (e.g. sterilizer charts). That any critical data such as weights or calculations are appropriately supported. (e.g. checked by second operator). Ensure any unexpected results, yields or reject material, any deviations, adverse results investigation, reconciliations and any other notes must be put to file. Review the record for any other entries and details as appropriate (e.g. expiry dates). All relevant information has been commented on the relevant page of the batch record. The supervisor or manager should sign and date each record pertaining to separate process stages. Where errors are recorded these should be trended and addressed. The reasons for errors, especially human error, should form part of training program for personnel. Errorproofing ways of structuring and writing knowledge documents, procedures, batch records, as well as practices for structuring, conducting, and documenting training to assure competence, are each useful activities. It can be hopeful if organizations shift form the common 'training for compliance' paradigm to a 'training for competence' paradigm, since training for competence focus is more likely to achieve GMP compliance (20). A focus on well-designed batch records as so to minimize errors and instigating regular checks and ensuring that deviations and out-of-specification incidences have been carefully examined, represent important steps for making the batch review process more robust and for consequentially making recalls that could have been prevented due to issues with batch release procedures less likely. Potentially a move away from traditional paper records to electronic records allows pharmaceutical manufacturers to more easily review data and provides a higher level of data security. Nonetheless, electronic data can also present problems in terms of control, security and safety, and careful attention needs to be paid to the design phase. Summary Human error is probably unavoidable; however, it can be reduced down to an acceptable level and the impact of the error minimized. This can only be achieved through an analysis of systems and work processes. Such an analysis can be (ideally) proactive or reactive (as in the case studies presented). There are different approaches to error analysis, and these will have their own merits and disadvantages. An approach based on human factors has been presented here, but it is far from the only method. This paper has explored how seemingly straightforward error risk reduction approaches can help address human error related issues. This was through a general description of the approach to error risk reduction and through a case study involving a stopper holding device. The case study illustrates the dangers that can arise when people become complacent and where operations are based on experience or head knowledge. The primary corrective action was with producing clear instructions and in briefing staff. Error risk reduction can be approached in different ways and it is very much situation dependent, although the general approach outlined in this paper provides a useful framework to adopt. References 1. Taylor, J.T. (2015) Human Error in Process Plant Design and Operations: A Practitioner’s Guide, CRC Press: Boca Raton, pp281–286 2. Reason, J. (2000) Human error: models and management, BMJ 320 doi: https://doi.org/10.1136/bmj.320.7237.768 3. Hollnagel, E. (1993). Human reliability analysis: Context and control. Academic Press, USA 4. Norman, D. (2013). The design of everyday things: Revised and expanded edition. Basic books, USA 5. Cooke J.A., McMahon C.A., North M.R. (2003) Sources of Error in the Design Process. In: Gogu G., Coutellier D., Chedmail P., Ray P. (eds) Recent Advances in Integrated Design and Manufacturing in Mechanical Engineering. Springer, Dordrecht 6. Khoja SS, Khoja S, Khoja FS, Khoja S, Pirani N (2017) Impact and management tool for identification and reduction of human Errors in pharmaceuticals Industry; PharmaTutor; 5(2); 7-13 7. Voices in Validation podcast (2020) Addressing the Root Cause, Not the Symptoms: Root Cause Investigations for CAPA, IVT Network: https://www.ivtnetwork.com/article/addressing-root-cause-not-symptoms-root-causeinvestigations-capa 8. Serrat, Olivier (2017). "The Five Whys Technique". Knowledge Solutions. pp. 307– 310. doi:10.1007/978-981-10-0983-9_32 9. David, B.A., Rodriguez, A. and Marks, S.W. (2008) Risk Reduction and Systematic Error Management: Standardization of the Pediatric Chemotherapy Process. In Henriksen K., Battles, J.B., Keyes, M.A., and Grady, M.L. (Eds.) Advances in Patient Safety: New Directions and Alternative Approaches (Vol. 2: Culture and Redesign). Rockville (MD): Agency for Healthcare Research and Quality (US), pp1-10 10. Kim G, Chen A, Arceci R, et al. (2006) Error reduction in pediatric chemotherapy. Arch Pediatr Adolesc Med.;160: 495–498 11. Kirwan, B. (1996) The validation of three human reliability quantification techniques - THERP, HEART, JHEDI: Part I -- technique descriptions and validation issues. Applied Ergonomics. 27(6) 359-373 12. Gallant, J. (2014) Human Error Is The Leading Cause Of GMP Deviations – Or Is It?, Pharmaceutical Online, at: https://www.pharmaceuticalonline.com/doc/human-erroris-the-leading-cause-of-gmp-deviations-or-is-it-0001 13. Mecugni Daniela, Turroni Elena Casadei, Doro Lucia, Franceschini Lorenza, Lusetti Simona, Gradellini Cinzia, Amaducci Giovanna (2021) The Use of Simulation for Teaching Therapy Management: An Observational Descriptive Study on 2nd and 3rd Year Students of the Nursing Degree Course of Reggio Emilia, Methodologies and Intelligent Systems for Technology Enhanced Learning, 10th International Conference. Workshops, 10.1007/978-3-030-52287-2_13, (127-137) 14. Sanders, M. and McCormick, E. (1987) Human Factors In Engineering and Design 7th Edition, McGraw-Hill Education, USA 15. Marx D. (1997) Discipline: Why Process Is More Important than Outcome. Ground Effects 2(5):2-6 16. Fantin, I. (2014). Applied Problem Solving: Method, Applications, Root Causes, Countermeasures, Poka-Yoke and A3. Milan, Italy: Createspace, an Amazon company 17. NOPSEMA (2020) Human error risk reduction to ALARP at: https://www.nopsema.gov.au/assets/Information-papers/A424182.pdf 18. Djuris, J. and Djuric, Z. (2017) Modeling in the quality by design environment: Regulatory requirements and recommendations for design space and control strategy appointment, International Journal of Pharmaceutics, 10.1016/j.ijpharm.2017.05.070, 533, 2: 346-356 19. Capozzi, L. C., Trout, B. L. and Pisano, R. (2019) From Batch to Continuous: FreezeDrying of Suspended Vials for Pharmaceuticals in Unit-Doses. Industrial & Engineering Chemistry Research, 58 (4): 1635-1649 20. Bodmann, K.; Reinhard, C.; Mödler, M.; Tinson, K.; and Johnson, M. (2016) Lonza Error Prevention System (EPS) – Changing Human Performance in Pharmaceutical Operations, CHIMIA International Journal for Chemistry, 70 (9): 610-615 View publication stats