FREE NCLEX Cram Guide NurseInTheMaking 7e2214f5-fb68-4d3b-b84b-af40d94e219a
advertisement

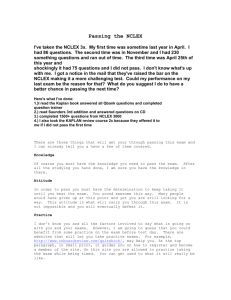
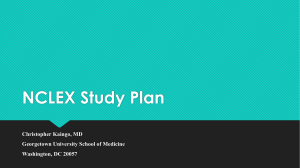
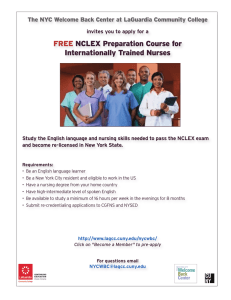
NCLEX Cram Guide ® what is the nclex? test tips The NCLEX exam is the licensure examination that nursing school graduates in the US and Canada have to take to recieve their license. There are two types: the NCLEX -RN and the NCLEX -PN. ® ® ® Questions • Minimum questions: 75 • Maximum questions: 145 Time Limit • 6 hours Breaks • 2 optional breaks: • First break @ 2 hours • Second break @ 3.5 hours You can take unscheduled brea ks at any time! It jus t counts against yo ur testing time. Day of the exam • Have your ATT email ready • Arrive 30 minutes before the exam • Bring an acceptable ID 4,500 - 11,000 /µL RBCs 4.5 - 5.5 x10 /µL PLTs 150,000 - 450,000 /µL Hemoglobin (Hgb) Female: 12 - 16 g/dL Male: 13 - 18 g/dL Hematocrit (HCT) Female: 36% - 48% Male: 39% - 54% 6 Do not ignore or “PASS THE BUCK” • If there is a nursing task you can do to fix the problem BEFORE contacting the HCP, do that! Don't add information • There are no “hidden meanings” in the questions. Don't add something to the scenario that's not written. How long to study for • You don't want to study for too long. Aim to study anywhere from 4 - 6 weeks. This way, all the things you have studied are fresh for the exam. Avoid answers with absolutes • Avoid answers with absolutes like always, never, every, none, only, all, etc. Schedule Mock exams • Take a few mock exams. Put your phone away, don't get up, and do 75 random questions. This will truly prepare you for the NCLEX exam. You will get questions that bounce from pediatrics to pharmacology to mental health. Train your brain to bounce between these different subjects. Saved by the suffix • Don't memorize every medication name; know the suffixes & prefixes for each mediation class. vital signs ® must-know numbers maternity Therapeutic Drug Levels Blood Pressure (BP) Systolic 120 mmHg Diastolic 80 mmHg Fetal heart rate 120 - 160 BPM Fetal respiratory rate 30 - 60 breaths/min Heart Rate (HR) 60 - 100 bpm Amniotic fluids 500 - 1200 mL Respiratory rate (RR) 12 - 20 breaths/min Temperature (T) 97.8 - 99 °F (36.5 - 37.2 °C) Contraction Oxygen (O2) 95 - 100% Duration: 2 - 5 minutes apart with duration of < 90 seconds Intensity: <100 mmHg Apgar score 7 - 10 = excellent condition 4 - 6 = moderately depressed 0 - 3 = severely depressed electrolytes ANTICOAGULANT THERAPY Sodium 135 - 145 mEq/L PT 10 - 13 sec Potassium 3.5 - 5 mEq/L PTT 25 - 35 sec Phosphorus 2.5 - 4.5 mg/dL Calcium 9 - 11 mg/dL aPTT Not on heparin: 30-40 sec On heparin: 47 - 70 sec Magnesium 1.5 - 2.5 mg/dL Chloride 95 - 105 mEq/L © 2022 NurseInTheMaking LLC Practice questions • Do a lot of practice questions. Have a goal for how many you want to do each day. • Read all the rationales, even if you got it correct. Don't read into the questions • Don't assume or add information that is not there. Take the question for as it is. complete blood count (cbc) WBCs study tips INR Not on warfarin: < 1 sec On warfarin: 2 - 3 sec Cardiac Biomarkers CK-MB 0 - 5 ng/mL Troponin T <0.1 ng/mL Troponin I <0.03 ng/mL Myoglobin 5 - 70 ng/mL BNP <100 pg/mL acid-base balance pH 7.35 - 7.45 PaCO2 35 - 45 mmHg PaO2 80 - 100 mmHg HCO3 22 - 26 mEq/L Digoxin 0.5 - 2.0 ng/mL (> 2 = Toxic) Lithium 0.6 - 1.2 mEq/L Theophylline 10 - 20 mcg/mL Dilantin (Phenytoin) 10 - 20 mcg/mL Magnesium sulfate 4 - 7 mg/dL Acetaminophen (Tylenol) 10 - 20 mcg/mL Gentamicin 5 - 10 mg/L Salicylate (aspirin) 100 - 300 mcg/mL Vancomycin Peak: 20 - 40 mcg/mL Trough: 5 - 15 mcg/mL Valproic acid 50 - 100 mcg/mL NCLEX Cram Guide ® Common Signs & Symptoms Angina Chest pain relieved by NTG Myocardial Infarction (MI) Crushing pain, pressure & tightness unrelieved by NTG Diabetic Ketoacidosis Acetone breath Parkinson’s Disease Pill-rolling tremors Cerebrospinal Fluid (CSF) Leakage A "halo” or “ring” will occur when CSF is mixed with blood (commonly seen on a gauze) Osteomyelitis High fever Acute Respiratory Distress Syndrome (ARDS) Refractory hypoxemia Pulmonary Tuberculosis (TB) Night sweats Gastric Ulcer Pain immediately after eating Duodenal Ulcer Relief of pain after eating (2-3 hours after) Any Renal Damage ↑ BUN & creatinine Bladder Cancer Painless hematuria Depression Anhedonia (loss of pleasure in activities usually found enjoyable) Constipation ↑ fiber, ↑ fluid, ↑ fruits Diarrhea ↓ fiber, ↑ fluid and electrolyte replacement Celiac Disease Gluten-free diet Burns ↑ protein, ↑ calories Acute Kidney Injury Protein-restricted, ↑ calories COPD Small, frequent meals ↑ calories, ↑ fat Pancreatitis Small, frequent meals, ↓-fat Vomiting or Diarrhea ↑ fluids & electrolyte replacement Gallbladder Issues (cholecystitis) ↓ fat Underweight ↑ protein, ↑ calories Hyperlipidemia ↓ fat, ↓ calories Hypertension ↓ fat, ↓ sodium, heart-healthy diet Cystic Fibrosis ↑ fluids Kidney Stones ↑ fluids fluid restriction Sickle Cell Anemia ↑ fluids Clients with Ostomies ↑ fluids & ↓ intake of odorous & gas forming foods (onions, broccoli, spinach, etc) Gout ↓ intake of purine foods (seafood, shellfish, organ meats) Strawberry tongue & sandpaper rash Cirrhosis ↓ heart & ↓ blood pressure Avoid foods high in protein (milk products, broccoli, eggs, tuna, chicken breasts, etc.) Ulcerative Colitis ↓ fiber (low-residue diet) Beefy (red), smooth tongue Fetal Alcohol Syndrome Thin upper lip & smooth philtrum Spina Bifida Occulta Small tuft of hair, a dimple, or a hemangioma at the base of the spine Epiglottitis Tripod position Scarlet Fever Neurogenic Shock Miscellaneous Tips Delegation Only the RN can do the initial teaching and the discharge education. The RN should care for unstable clients & the LPN should care for stable clients Potassium Never give potassium IV push Cardiac Catheterization Assess for allergy to iodine or shellfish NSAIDs NSAIDs (naproxen, ibuprofen, celecoxib) should be avoided in those with a cardiovascular history (stroke, MI, coronary artery disease, etc.) Pheochromocytoma Do not palpate these clients' abdomens, it can cause a hypertensive crisis Meningitis If a client is suspected to have meningitis, place them on droplet precaution right away Traction The weights must always be free-hanging (not resting on anything) COPD It’s typical for COPD clients to have lower than normal O2 levels. BUT any O2 level less than 60 mmHg indicates hypoxia Barley rye oat NO BROW wheat Heart Failure Pernicious Anemia © 2022 NurseInTheMaking LLC common diet modifications NCLEX ® Study Notebook or click here so you can be the first to be notified when it's released! Scan coming Mid-ma y 2022 What’s included? • Study Calendar • NCLEX Quick Guides ® (“Must-knows” for the NCLEX exam) • Practice Questions for each section • NCLEX overview ® They will sell out quickly! • NCLEX topic checklist ® • How to make a study plan • How to answer NCLEX questions ® • Exam day tips Did you know... ) LOGY MY & PHYSIO (SIDS MEPEDIATRIC ANATOBRONCHIOLITIS (RSV) REYES SYND NDROIN1 year of age SIZE disease VARIAT ROM SYIONS HEAD Rare affecting INTEUSS young children ATH t younger than USCEPT recovering RY NT DE hy infan from a viral ARE ION RE illness (flu CORD INFA RESPIRATO Infl THE y healt or MS! part of growing the body!) is the fastest proportion to (large in are not well an infant & neck muscles INFA Lead h deat developed EPIGL unknow EPI the n n OTTIT lead GLOTTI WHA T upp ing to S ↓IS THE EPIG IS obs er airw an inflammation tru HS) LOT ctio ay MONT NEURAL TUBE DEFECTS TIS? n ↓ FEVER MAN FETAGEM AL CIR ENT ↓ CULATI ON IN↓ UTERO ↓ ↓ • • SPINAL fused Exact not completely cause amm of atio HO BRAIN & chicken ILEUM to the skull for hemorrhage intake = ↑ risk or salicylatemakes the such containing of salicylates & fontanels as aspirin for growth products to and allows flexible • Sutures of the brain treat a (Flu / Chickenp viral illness mobile ox) is very • The spine cervical spin injury for Viral illness usually PAT ADU L T bones vascular BRONCHIOLITISCranial Triggered is highly The brain due COMP CAU SES cartilage (<12 PEDIATRIC CPR✹✹ PATH O rst for the fi from sless airways • Floppy statu nose breathers omic care • Obligatory econ rate d) • ↑ metabolic atal pren • Socio here r) requirements • ↑ O 2of smot • Lack tic be is bette • Gene ing (can (cooler • Bedd temp Room •EARS • Head NO PTO SYM h S OR deat SIGN Sudden e of caus ts ingtheinfan small airways in in lungs adult airways than an have ↓ alveoli grow each day • Newborns of alveoli life! • Thousands few months of TELESC OPES • Head NT • Narrow PATHO Sudd TORS K FAC (↑ risk) ths mon -6 :1 • AGE rm ion • Prete p posit h • Slee g deat sure • Siblin tine expo • Nico EDEMA NORMAL iousl EN prev SUDD en death of a pox) TELES COPES INTO THE CECUM OBSTR UCTIO at thePieceN = PAIN back of carti lage of RESSIO Close N ✹ caused = by↑Respiratory syncytial OF BLOOD the s the Func virus (RSV) Mos tong Very contagious FORA BP Spina t com VITAL SIGNS durin entry tionVESSE ue ✹ Bifida BLOODAKA NORMAL SPINE IC MEN Stre LS g to : is a general term for NORM mon Systolic FLOW Blood a pto ✹ Starts asPEDIATR SYSTEM birth defect preveswall the OVAL an upper respiratoryPulse AL ENCEPHAL owin trach IMMUNE infection DECRE caus istypically diagnosed TEMP ✹ Interm moves 80 to&INFECTION cocc nts into E during pregnancy the OPATHY 60 -SHUN chest g.... ea ASES aspir FOR the where the e: Hae / CEREBRAL left TED 97.5°F spinal RISK - 160 us column fails to close. ↑✹ systems 120 ittent atrium ation Blood from pne to immune EDEMAFEVER Child 80 -98.6°F mopBOWEL ISCHE 30 - 50 70 Spina the“split pain bifiby bypas • Immature da✹ Tach means umo 36.4°C response the right spine” RECTA draw It's alread - 140 hilu newborn ses /✹cram 120 foram to MIA ycar atrium inflammatory 37.0°C > 100.4°F the Sore Lnia disease • ↓the s up CAUSES30 - 40 BLEED abdo 95 s infl -to lungs. ping en Ovale y80 exposure their oxyge maternal ..why? dia yr NOT KNOWN... men (38.0°C Limited - 110 • while from nated HowING (CURR CONTINUED 6 mo - 1 ✹ Hig 100 legs thro NT = harbors immunity in100 ) can blood ANTuenza ✹ (losingcrying - 30 be towaat "CHILDS" VE blood 90 - severEMERGENT ✹ Upper respiratory symptoms SIGNS BUT20 MANY h feve FACTORSVomi HINDER from shunted JELLY typ ✹ Anx NORMAL CNS DEVELOPMENT ✹& - 100 Lower fromrd 2 - 4 yr pain ting SYMPTO respiratory •eGrunting 90antibodies) tract symptoms eB STOOL atriumthe right ✹ Curra • Nasal congestion / PRE • Drugs r the placen & diarrh MSACUTE -✹110 14 - 20 • Tachypnea • Chemicals ious flaring • 100 to the Folic S!) RIGH acid deficiency left C Confusion • Nasal • Runny nose5 - 8 yr ✹ Flushed (Vitamin ON ion als 100 FATTY atrium? • Malnutrition pressu 80 -nt-jel eaDiffi / app THIS B9) ta (mom) T ATRIU ✹ Letha • Genetics LIVER • Diabetes (changes ATI e posit ly stool 20 • Cough FAILURE • Cough 120 ✹inNOT •cult Cyanosis re IS Blood ✹-TREATM d anim t 12 - skin 100 mental TELESBECAU ENT rehe HSUPERIO • Wheezing rgy ✹ Diaphore Blood differ y spe Hyperrefl MSYSTEM PEDS status) 90 SE infan LABS s Nas goes ✹• Obesity • Sneezing 8 - 12 yr ✹ Sausa SCULAR 60 -NERVOUS COMP interio INTER COPIN EDUCp in supin ence! fallin incid incomplete nsiv exia al• flHypoxia or stuffe the fromAdministe ✹ is(bloo sis (sweating FORAME akin CARDIOVA high flows from VENA G R e r vena ✹ May MITTE 12 -20 LETE fetal ✹ Fever PULSE arin ws, ↑ LIVER theStrid •rdy) rightge-sh IS Myelinization ✹ Dro ✹ singfrom longer CAVA Hib g due ent resista / agit • Slee ing OVALE N I gIrritability yr Chills in the Respiratory ) • at NT LY KNOW cava ENZYMES or antipyreti no circulation atrium pillo ✹ Monitor ress IN birth vaccin to be dres→ normal in g csfailure • The transition deoxy SPINA> 12BIFIDA (ibuprofe DUCTUS to(Fro ↑ aped olin to nce Check pulse uppe AST atiocause due to happens as well OCCULTA ✹ Triplow matt the kets, ✹circulation MILDEST for• S&S ation ✹ Restlessn • Bedd Apneic episodes genat /MIN the BEATS/M L Lethargyn)ARTERIODo g-lik nts) pulse &mass g /N or over 10 seconds electrolyt s swell FORM nAORTA of dehydrati not blan a virus mid-a as some direction ↑• rMyelinization ed administer super BREATHS • Firm ALT ess pare dysp ling atthan birth od resista Lungs ✹SUSCond ee imbalance (risk brachial ✹ Sitti croa D thinner toys, ing on bdom iorcephalocaudal aspirin for ✹ Lethargy arethe ✹blood that So the pos nce hag Sponge heartsCheck comin vena from : High to tail) Infant: ✹ May k on s Diarrhea & Provide Reye's • No over bund itionSyndrome en • Infants from carotid pulse ition ng (oxyge blood (head resista g from ✹ Nev ia cava. bath vomiting compliant Typically exte ) all the d childblood asymptomatic less ing Check forw rate the vertebral spon ✹ Self-limitedDefect and child: is✹ n-rich nce Remove • adequate illnessof now S insp & supportive Diver ✹ Seizures nde does fluid. care (Pass • Avoi d smok ng Does sepa fluids!is born er excess irati & oxygen body WITHOUT ardSo the need ✹ Ass MIXED May ✹ taneo agehave Hydration dimpling, & coverings leav not Tepid • Polyp ticuluRetrgo not dwith clothingimmediateon) usly with ✹ medical ✹ Airway sleep water to eddi in of Avoi want maintenance care protrusion -poor if asymptomatic. help • IV flabnormal of the e the es blood) ✹ m acti the lungs! norm for s20-30 Increase be patches to Squeeze fluid of ✹✹IV nearby ↓ to the co-b should (oral uids orthe oxyaudal reduc IV) temp ons breath min. Cool intake Cephaloc over back Nas hair, orSmeninges. shout for✹ • Oxygenspinal cord ✹ If symptoms t temp use FOR HELP (risk foral, compress are present, dehydration) • No brow near al fl gen acce ed clien system / Early recognit (che Antib or discoloration ✹ Abs & body - mouneck CALL ✹ May direction (Infan al room on the the ier arin response the spine. client t an MRI. RIGHT mayforehead stat ssn stool get st) iotics • Suctioning the AED✹ ion tail) ✹ Educatio / get g ent th Liver nee (head to treatme s) usATRIUM Deco DUC & ✹ Hospitalization e pacif ✹ Active the emergencySaline call 911 ✹ Calm not fully before walking! ope drops & then suctionnthe • Norm urag else to nose nt Head on preventi DUC cough! SKIN functioni TUS Only control mpre d the child is thinner n necessary someone nares ✹ne INTERIO Monitor the with a bulb ✹ TUS Umbil ng yetif eme VEN ssion syringe • Epidermis to remove • Enco ✹ Delegate are closer to VENA the R has OSUS Blood flProvi ARTE severeenv k on! uid Educate symptoms rgen de ical alo vessels oxyge easily! MENINGOCELE CAVA status before✹ vein via• Stay feeding very secretions comf or atsupp • Blood is NG ironmen ratio Swelling RIOS bedtime bac productDiagn on the isrescuer loses heat • Position carryin irnated ort ort • Don tube pulmoSHUNTED withproximodcyistal US ofplacen intu s that surface Do the ✹ blood ✹ Moni Use&contact tosingle into - 40° t outward) angle standard g’t &n-to-breath IONS the child at a 30•WHAT the ta. brain contain nary emot not bati Salicyla ostic (Some from Maintain pare LIVER IS Itthe • from compressio occurs IT? passes Helpthe precautions paren visua the the aorta artery rest (inward Take tor 30:2 ional / Trea Onbut during the AED on Most children ingblood carents ✹ May CHEST COMPRESS cerebral Seizures • Managin lize ductus AIR tes: Sac theherniate oral tmen retrieving by ts Meninges protruding mostfor to rain signs will •perfusio Mos can be managed or LIVER associate temp the to need avo the go crib will through of CPR before from the & preventi /minspinal throa arterio of • Seizure t com to area. the a defect works BARIU agdinferi Aspirin be SHUN n id cryin child perfo the M ENEM eratut t with sus with (usu at home It can air ✹ 2 minutes ✹ protection compressionNot related the sternum ng In SIGNS precauti less a 120 the liver) or rescuers in ratio = • the to FEVER re Do increase vertebrae. Ductu or Surgical correction & also Most forta 100 ally ration Two areon bariu coveredto: Provi diagn TED or & SYMPTO cause A thumbs ons vena DUCTUS a tongu Alka-Seltz to2abdomen n-to-breath DESCEN not cava d ICP ✹ Rate of g des educ KIDNEYS • chest's tripo m or relationor AORTWhy take throa Venos helps bleshock ose & It bec with skin. VENOSU of the lesion Usually theMSerAORTA minor compressio ofintracran larger 2infingers dehydration (cutti REFLA ? e areeither 15:2 pos intuss DING reduc us placenem S one-third= ↑ risk for ial infection ation ✹ NPO Rapid • metaboli EX Pepto-Bism ✹ Using no neurological a d pos ✹ t cultublade • Kidneys ometo deficits. ebythem diameter c Usually Equal to reabsorb ition ↑ in core uscep Mixed eng off LARY . terior ol imbalanc itionUMBILIC is slowerInfant: urine & re. FROM does s hard child • viral • GFR tion the ✹ NGO aorta blood ✹tempera AL ✹ Depth: Child illness PLACENT have e Kaopectate not to concentrate anterior-pos )VEIN may Med ture & in airwa is and SPAS family sup postictal THE • ↓ ability erPLACENT to oxyge be drowsy icat TO being now complilong y) in the term inches to A → ine MS PLAC s abou during such cations Child: 2 pushe brea nate period A← • Ant ions pos pre-o MOST BETW compression ENTA MYELOMENINGOCELE as epilep RISK FACTOR the the. tition or intellec between SEVERE fetus d out • Ant ibio sy for recoil FORM IS THE S EEN MOT . p & post✹ Allow ✹ 6 months disabil tual ipyr tics • UMBILIC The "LIFE Corop HER ity - 5 yearsfor Placen- thumb ARTERIE AL etic LINE & • Multiple ✹ Rapidly the 2 ta is surgical (dec tico S ster s BLOO procedures " TREATM like handBABY fetus develope The encircling "tempo • Paralysis • IV reas oids whileoften BACK D GOES spinal cord ✹Protrusion d fever HIGH of rary ENT in Flui e • Bladder PLACE TO THE lungs"✹ /NOT bowel incontinence fever ends at technique the point utero ds infl 2 - fingern ✹the meninges, amm NTA anticonv 2 Umbil • Neurogenic bladder Family fluid, of the defect. OXYG atioTO GET ulsants compressio cerebrospinalhistory ✹ Rectal ical• Meningitis A think (infection) therapy and spine. of febrile ENATn) Diazepam technique ✹ Certain AWAY = 1 Arteries • Hypoxia seizures AGAIN ED ✹Takes Umbil Skin may vaccines Educate Absent motor be • ! blood deoxythe ical Hemorrhage exposed C MS PTO SYM SIGN S& ES T G↓ ↓ MEN AGE Febril G MAN B SIN A CAUS MS & SYMPTO SIGNS ENT OF PIN ABC SLEE SAFE TREA TMEN T TREATMENT 3 TREATM 2 SIGN S & SYMP TOMS EVENTS ORDER OF 1 risk ns The neural tube closes: Respiratio 3rd -age 4th week of gestation SIGNS & SYMPTOMS usually INFECTION infants EAR FORin arrest ↑ RISK Cardiac tubes are y etiology • Eustachian respirator & flat stems from difficult short, wide, drainage s INITIAL = making ION microorganism NUR RIS d o w nl o l ita CAUSE di g bundle s ad – Kristine Tuttle, BSN, RN a s h c a r ds ↓ e Seizur e ↓ ↓ START • DTP as well. & MMR 4 y templat ud es You may be stressed, you may feel tired, and you may want to give up. Nursing school is hard, there's no doubt about it. Everyone cries, everyone has meltdowns, and there will be moments you don't feel qualified for the task at hand. But take heart, the challenge only makes you stronger. Put in the work, show up on time, and find an amazing study group. You got this! fl st Dear future nurse, NurseInTheMaking creates tons of other nursing school resources! ba CONTINUE UNTIL SIGNS OF HELP MEMORY TRICK genat & sensory function parents AVAILABLE • Freq. vein catheterization waste causes... from ed to seek • +Last beyond thatAED point.BECOMES ➥ Latexthe > min help if... allergy baby 5AWAY to the SHUN •/Repeated ➥ UTIs pyelonephritis placen back TS Gives ➥ Renal damageta seizures TO oxyge ARRIVE OR blood TO the n rich baby • Ductus KNOW • Foram venosus • Ductus en ovale arteri osus dge cards Scan to shop! By purchasing this material, you agree to the following terms and conditions: you agree that this ebook and all other media produced by NurseInTheMaking LLC are simply guides and should not be used over and above your course material and teacher instruction in nursing school. When details contained within these guides and other media differ, you will defer to your nursing school’s faculty/staff instruction. Hospitals and universities may differ on lab values; you will defer to your hospital or nursing school’s faculty/staff instruction. These guides and other media created by NurseInTheMaking LLC are not intended to be used as medical advice or clinical practice; they are for educational use only. You also agree to not distribute or share these materials under any circumstances; they are for personal use only. © 2021 NurseInTheMaking LLC. All content is property of NurseInTheMaking LLC and www. anurseinthemaking.com. Replication and distribution of this material is prohibited by law. All digital products (PDF files, ebooks, resources, and all online content) are subject to copyright protection. Each product sold is licensed to an individual user and customers are not allowed to distribute, copy, share, or transfer the products to any other individual or entity, they are for personal use only. Fines of up to $10,000 may apply and individuals will be reported to the BRN and their school of nursing.