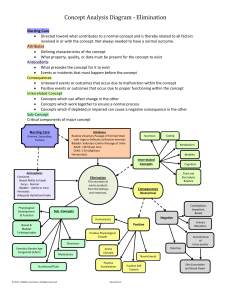
Foundations Exam 1 Lecture 1: Activity Mobility—moving freely & easily is fundamental to normal, daily functioning Independence—person’s ability to perform ADL’s; can meet his own basic everyday needs o Independent person can protect himself from trauma Best way to assess a patient’s ability to perform ADL’s is by watching him perform ROM Immobility—state of being dependent upon others for physical care Can negatively affect mental & physical well-being o Mental health—may affect self-esteem/emotional outlook o Physical health—physical disorders that may affect one’s mobility Therapeutic treatments Progressive disability (severe crippling rheumatoid arthritis, emphysema) Permanent changes (CVA or Stroke) Skeletal System—framework of bones, joints, cartilage, which protects organs and allows us to move Functions of Skeletal System 1. Maintains body form and posture—supports soft tissue of the body a. Soft tissue—tissues that connect, support, or surround other structures & organs of the body i. Muscles, tendons, ligaments, fascia, nerves, fibrous tissues, fat, blood vessels, synovial membranes 2. Protects components of the body a. Critical components: brain, lung, heart, and spinal cord 3. Furnishing surfaces—attachment of muscles, tendons, ligaments, which pull on bones for movement 4. Stores minerals—storage for calcium and fat 5. Producing blood cells—hematopoiesis Freely Movable Joints of Skeletal System 1. Ball-and-socket joint—shoulder and hip a. Assess flexion-extension, abduction-adduction 2. Condyloid joint—wrist and joints connecting fingers to palm a. Assess flexion-extension, abduction-adduction 3. Gliding joint—carpal bones of wrist and tarsal bones of feet a. Assess flexion-extension, abduction-adduction 4. Hinge joint—elbow, knee, ankle a. Assess flexion-extension Muscular System: 3 Types of Muscles 1. Skeletal—work with tendons and bones to move body 2. Cardiac—produces contractions that create the heartbeat 3. Smooth or Visceral—forms walls of organs (stomach and intestines), wall of blood vessels, hollow tubes (ureters) Muscles have 2 differing points: 1. Point of origin—attachment to stationary bone a. Origin is attachment site that doesn’t move during contraction b. Origin—proximal (closer) to body, relative to insertion 2. Point of insertion—attachment to move movable bone 3. a. Insertion is attachment site that does move when muscle contracts b. Insertion—distal (further away) When muscle contracts, usually one bone moves & other is stationary origin is where muscle joins stationary bone a. Insertion is where it joins moving bone Body Contraction of Muscles 1. Motion—skeletal muscle contraction pull tendons and move bone (swimming) 2. Maintenance of Posture—skeletal muscle contraction (kyphosis or scoliosis) 3. Support—skeletal muscle support 4. Heat Production—skeletal muscle contraction Nervous System—nerve impulse stimulate muscles to contract 1. Nerve cells called neurons conduct impulses from one part of body to another 2. Afferent neurons carry nerve impulses or information from sensory stimuli TOWARDS CNS/Brain information is from receptors in periphery of body to CNS 3. All neurons and information leading to responses is processed in CNS 4. Efferent neurons (motor neurons) carry neural impulses AWAY FROM CNS & towards muscle to cause movement of skeletal muscle through Somatic Nervous System a. Somatic NS—voluntary control of body movements via skeletal muscles Effects of Exercise on Major Body Systems 1. Cardiovascular System a. CV System meet challenges with: i. Increase heart rate ii. Increase contractility iii. Increase stroke volume iv. Increase cardiac output b. Over time with regular exercise produce: i. Increase efficiency of heart ii. Decrease heart rate and BP iii. Increase blood flow to all body parts iv. Improve venous return v. Increase circulating fibrinolysis (substance that breaks up small clots) 2. Respiratory System a. Works with CV system to increase oxygen available to the muscles b. Improves alveolar ventilation c. Decreases work of breathing d. Improves diaphragmatic excursion 3. Musculoskeletal System a. Exercise increases muscle mass, tone, strength, and increases joint mobility b. Increases muscle strength and flexibility c. Increase coordination d. Reduce bone loss e. Increase nerve impulse transmission 4. Metabolic Processes a. Metabolic rate increases during exercise so glucose & fatty acids can convert for needed energy for increase muscle function b. Increases triglycerides c. Increases gastric motility d. Increases production of body heat 5. GI System a. During exercise, blood is shunted away from the stomach and intestines to the muscles b. Increases appetite c. Increases intestinal tone d. Improves digestion and elimination e. Controls weight 6. Urinary System a. Increases blood circulation b. Improves blood flow to kidneys c. Maintain fluid balance & acid-base balance d. Excretes wastes 7. Skin a. Increases circulation to skin b. Nourishes skin & promotes general health of skin 8. Psychosocial Outlook a. Increases energy b. c. d. Improves sleep Improves body image and self-concept Increases positive health behaviors Effects of Immobility 1. Cardiovascular System a. Increases cardiac workload—compresses valves in the legs so they do not adequately contract to pump blood back to right side of the heart b. Orthostatic hypotension—blood pools in lower extremities resulting in a drop in blood pressure and increase in pulse rate i. Result of lack of vasoconstriction when changing from supine to upright position ii. ACTIVE PEOPLE: skeletal muscles constrict when they change from supine to sitting/standing position 1. Result: prevents pooling of blood in lower extremities & allows blood to flow BACK to heart 2. Maintains normal BP iii. INACTIVE PEOPLE: muscles atrophy and do not allow muscles to constrict decreases cerebral profusion (dizziness/fainting) iv. INTERVENTION: to minimize effects: 1. Advise gradual position changes 2. Encourage leg exercises before getting out of bed 3. Remain with patient after assisting them to a sitting/standing position c. Dependent edema—serous part of blood is forced out of vessel into the interstitial space because of an increase in venous blood pressure i. Most common in areas below the heart (feet, legs) ii. EDEMA SCALE: 1. 1+ barely detectable 2. 2+ slight indentation (5mm) 3. 3+ moderate indentation (5-10mm) 4. 4+ large indentation—slow return (>10mm) d. Venous stasis—blood to pool in veins, predisposes patients to thrombi formation i. Calcium leaving the bone to blood increases thrombus formation ii. Thrombus formation 1. Thrombus—blood clot within blood vessel that is attached to vein wall a. Most commonly originates in large veins of legs—Deep Vein Thrombosis (DVT) 2. Embolus—clot that has broken off of vein wall and enters circulation a. Coronary embolus—clot traveling in coronary artery b. Air embolus—air traveling in vein; enters right ventricle/atrium c. Pulmonary embolus—clot traveling in pulmonary artery or one of its branches i. SIGNS of PE: dyspnea, tachypnea, chest pains 3. Thrombophlebitis—blood clot loosely attached to an inflamed vein wall a. Frequently occurs in legs b. Results from: c. d. e. 2. 3. 4. 5. 6. 7. 8. i. Post-op venous stasis ii. Prolonged sitting/lying down iii. Immobilization iv. Prolonged IV therapy How to avoid: i. Early ambulation 2-3x/day ii. ROM exercises in immobilized patients iii. Proper positioning to decrease venous stasis iv. Elevate lower extremities approximately 30 degrees Assessment: i. Inflammation, tenderness, aching ii. Treatment i. Anticoagulant therapy—Heparin SQ or IV; Warfarin (Coumadin) PO ii. Bed rest—lay flat iii. Anti-embolic stockings—helps force blood from superficial veins to deeper veins iv. Avoid popliteal pressure v. Vital Signs—check q4 hours; use doppler if necessary Respiratory System a. Decreased respirations—reduced vital capacity (amount of air expelled after full inspiration) i. Rarely breathe deeply lungs not fully expanded ii. Pooled secretions leads to respiratory congestion b. Atelectasis—collapse of lung tissue i. Collapse of alveoli thereby decreasing the oxygen and CO2 exchange ii. Prevention: encourage deep breathing and coughing exercises every 2 hours c. Poor exchange of CO2 and O2—leads to acid-base imbalance d. Pneumonia—inflammation of lung caused by bacteria, viruses, and chemical irritants i. Pooled secretions are excellent media for bacteria growth ii. Intervention: encourage coughing/deep breathing q2hours iii. Patients on prolonged bed rest & receiving narcotics such as morphine—assess for pneumonia e. Loss of lung muscle tone—from patient’s position in bed or medications Musculoskeletal System a. Atrophy i. Disuse atrophy—decrease in muscle size and strength from disuse b. Tone and strength c. Decrease joint mobility and flexibility i. Contracture—progressive shortening of a muscle and loss of joint mobility 1. Impaired blood flow to muscle or joint speeds up the formation of contractures 2. Usually irreversible d. Bone demineralization e. Limited endurance f. Problems with ADL g. Osteoporosis Metabolic Processes GI System a. Constipation—frequent problem because of decreased peristalsis b. Straining (Valsalva Maneuver)—increases intra-abdominal/thoracic pressure placing undue stress on heart Urinary System a. Urinary retention—inability to completely empty the bladder b. IMMOBILE PATIENTS: must push upward (against gravity) i. Unable to completely empty the bladder which may lead to development of renal calculi c. Leads to urinary infection—static urine provides excellent media for bacterial growth i. Improper perineal care and indwelling catheters d. Encourage fluid intake of 2500ml/day unless contradicted Skin a. Pressure ulcer—bed sore b. Ischemia—blood flow (& thus oxygen) is restricted or reduced in part of body like tissue or organ i. Can be blocked by clot, embolus, or constriction of artery Psychosocial Outlook a. Body image b. Decrease self-concept and self-esteem c. Stress, social, coping Fall Risk Assessment for Older Adults Confusion (4) Symptomatic Depression (2) Altered Elimination (1) Dizziness (1) Gender—male (1) Antiepileptics (2) Benzodiazepines (1) SCORE OF 5 OR GREATER = HIGH RISK Hendrich II Fall Risk Model—determines risk for falling based on gender, mental status, medication side-effects, and disease symptoms such as dizziness Physical Assessment for Mobility 1. General ease of movement and gait—is patient’s movement quick and sure or slow and dilate? a. Is patient’s movement while walking coordinated? Is posture well-balanced? 2. Alignment—observe while standing, sitting, lying 3. Joint structure and function—use inspection/palpation to assess joint a. Use ROM & document any limitation s 4. Muscle mass and strength a. Muscle mass = muscle strength assessed by asking patient to move actively against resistance 5. Endurance—patient’s ability to turn in bed a. Maintain correct body alignment when sitting, standing, and lying b. Ability to perform self-care activities Positioning Patients Reposition every 2 hours prevents: o Muscle discomfort o Pressure ulcer formation o Damage to vessels o Contractures Seek assistance when repositioning a patient (2 or more to move/turn) Assess the patient’s condition BEFORE repositioning o Size & reason for repositioning o Mental & physical status Muscle Movement 1. FLEXION—bending elbow/knee at the joint 2. ABDUCTION—moving the arm/leg away from midline of the body 3. ADDUCTION—moving arm/leg towards the midline of the body Transferring from bed to chair or stretcher assess patient & seek assistance Assess patient’s tolerance for moving (physical/mental capabilities) When moving from prone to sitting, wait a few minutes Place chair on STRONGEST side Patient with paralysis—stand on weak side Need 4 people to transfer unconscious patient to support head Types of Exercises: Isotonic exercise—muscle shortening and active movement o Benefits: Increased muscle strength/tone Increased cardiac/respiratory function Increased circulation Joint mobility Examples: ADL, ROM, ambulating, swim/bike Isometric exercise—muscle contraction without shortening o Benefits: Increased muscle mass/tone Increased circulation to exercised area Examples: contraction of quadriceps and gluteal muscles ROM Exercises o Active ROM—isotonic; patient is able to move each joint to full extent of intended function Perform these exercises systematically/same sequence—2x a day o Goal: maximally stretch all muscles Rationale: these muscles maintain/increase muscle strength Passive ROM—patient is unable to move for himself Prevent contractures Helps maintain cardio-respiratory functions in immobilized patients Move joints SLOWLY/SMOOTHLY Do these exercises to point of SLIGHT resistance—not beyond Each movement should be repeated 3-4 times—2x a day No value in maintaining muscle strength Assistive Devices Pillows—provides support and/or elevates an extremity Adjustable beds—can elevated to desired degree o Elevate HOB, lower extremities, Trendelenburg Bed (side) rails—can assist the patient in rolling from side to side or sitting up in bed Trapeze bar—hand grip suspended from a frame near the HOB o Patient can raise his trunk from bed or pull himself up Support for feet (footdrop)—feet unsupported in dorsoflexed position o Toes drop forward; boots Trochanter rolls—used to support hips and legs so that femurs do not rotate outward Restraints—physical devices limiting a patient’s movement Side rails Geriatrics chairs with attached trays Appliances tied to wrist, ankles, or waist Physiological hazards associated with restraints: Suffocation from entrapment Impaired circulation Altered skin integrity Pressure ulcers Contractures Fractures Using restraints as a last resort Use least resistive restraint Evaluate potential for injury Consult family members Must be ordered by physician Documentation Date and time applied Alternatives Notification of family members Type of restraint Frequency of assessment Date and time removed Basic positions Fowler’s Position—head/trunk raised 45-90 degrees o Gravity pulls diaphragm downward o This increases chest expansion o Example: respiratory/cardiac patients; pneumonia/CHF Semi-Fowler’s Position—head/trunk raised 15-45 degrees o Example: cardiac and respiratory patients o Remember: in Fowler’s positions, do not raise knees with knee catch High Fowler’s Position—head/raised 90 degrees o Example: emphysema patient Orthopneic Position—patient sits with head resting over a table o Example: smoker with severe emphysema (barrel chest) Dorsal recumbent/supine position—head/shoulders are slightly elevated Prone position—lying on abdomen with head turned to side o DO NOT use for cardiac/respiratory patients Chest cannot be fully expanded during respirations o DO NOT use for lumbar/cervical patients Lateral position Head is rotated laterally Lecture 2: Hygiene Factors affecting personal hygiene: 1. Culture—ID culture variations o High value on personal hygiene 2. Socioeconomic class—financial resources, homeless people o Define options available to individual 3. Spiritual practices 4. Developmental level—family practices, adolescents, older person 5. Health state—weakness, dizziness, DM (footcare) 6. Personal preferences—shower v. bath, time of day, self-concept Components of Hygiene Care Skin Care—largest organ multiple functions o First line of defense o INSPECT & PALPATE Oral Care—history, patient conditions (comatose, paralyzed) Teeth Care—contributes to intact body image o Beginning of digestive processes are enhanced when mouth and teeth are in good condition Nail care Foot care Musculoskeletal Care Environmental Care Ticks—Lyme disease Piercings—anywhere on body Perineal Care—dark, warm, and moist love bacterial growth physical and psychological discomfort o Skin breakdown and offensive odors o Both: examine while patient is in bed; clean before catheter insertion, bath, and PRN o Female: least contaminated area to most contaminated area o Male: tip of penis, moving in circular motion from meatus outward Wash shaft of penis downward toward pubic area Denture care—24 hour not recommended because can cause stomatitis o Keep clean, remove/rinse after meals Eye care—clean first; specific care measures redness, swelling, blink reflex, remove contact lenses Unconscious patients—requires frequent eye care every 4 hours; keep moist (can cause corneal ulceration from drying_ Eyeglass care Ear care—clean outer ear, little intervention for ear care Nose care Hair care—cultural considerations Key Terms Alopecia—means loss of hair from head or body o Cause: autoimmune disease (Lupus) treatment: corticosteroids, Rogaine o Cause: drugs (chemo) treatment: none Dental caries—tooth decay/cavity; causes demineralization of hard tissues Cerumen/earwax—yellowish waxy substance secreted in the earl canal Cheilosis—causes: yeast or bacterial infection, vitamin deficiencies, bad habits, malnutrition, GI disorders, chronic pancreatitis Gingivitis—inflammation of gum tissue; initial stage of gum disease, easiest to treat Periodontitis—gum disease; receding gum lines; serious gum infection that damages the soft tissue and bone that supports the tooth Glossitis—inflammation of the tongue; swell and change color, smooth appearance on surface o Poor hydration and low saliva Pediculosis—infestation of lice; medication and environmental control Halitosis—bad breath Dental plaque—plaque produces toxins that can irritate gum tissue causing gingivitis Tartar (calculus)—formed when minerals such as calcium in saliva combine with plaque and make it hard Stomatitis—inflammation of mucous lining of any structures in mouth, which may involve the cheeks, gums, tongue, lips, throat, and roof or floor of mouth Personal hygiene Promotes physical and psychological wellbeing Reduce illness rates Modified during illness and hospitalization Scheduled Hygiene Care Early morning care, morning care, afternoon care (PM care) Hour of sleep care (HS care) As needed care (PRN care) Giving Bed Bath Bedpan Gather supplies/equipment Privacy Personal preferences Back massages Purpose Promoting Skin Health Emollient ingredients—increase skin’s hydration by reducing evaporation (moisturizers) Soap substitutes—chlorhexidine, liquid antiseptic soap, reduce incidence of hospital-acquired infections Barrier products—creams, ointments, protect vulnerable skin Bath cloths—heated before use, not required rinsing, self-contained package Teaching Self-care—informally during assessment Address specific topics—DM feet or dry skin Dry skin Deodorants Cosmetics Nursing Process 1. Assessment—Oral Cavity, eyes, ears and nose, hair, nails, and feet; perineal and vaginal areas 2. Diagnose—problem from assessment 3. Outcome identification and Planning—sense of wellbeing 4. Implementing—encourage self-care 5. Evaluation Lecture 3: Skin Integrity and Wound Care Factors that Influence Wound Healing 1. Age o Infant’s skin and mucus membranes are easily injured and subject to infection o Adult’s tissue becomes thinner and easily injured 2. Chronic illness o Leads to: Easily damaged skin, slow wound healing, circulation and oxygenation 3. Medication o Steroids (prednisone), anticoagulants (heparin, coumadin), antibiotics (vancomycin) 4. Nutrition—poor nutrition reduces red blood cells (RBC) o Results in decreased oxygenation essential for wound healing 5. Weight o Obesity—leads to increased adipose tissue which impairs blood supply resulting in slow wound healing Pressure ulcers—a lesion caused by unrelieved pressure Risk factors for developing pressure ulcers: Immobility o Always place a pillow between the legs or feet o Turn patient every 2 hours o Assess bony areas every 4 hours Malnutrition o Weight loss, muscle atrophy, loss of subcutaneous tissue Fecal or urinary incontinence o Leads to increased urinary microorganisms, resulting in infection Altered level of consciousness o Unable to respond to painful stimuli Advanced age o Weight loss, thinning epidermis, diminished pain perception Poor nursing care o Incorrect lifting/moving techniques o Repeated injections in same area Stages of Pressure Ulcer 1. Stage 1—nonblanchable erythema of intact skin 2. Stage 2—partial-thickness skin loss 3. Stage 3—full-thickness skin loss; not involving underlying fascia 4. Stage 4—full-thickness skin loss with extensive destruction Braden Scale—universally accepted tool to assist in identifying individuals at risk for developing pressure ulcers Scoring patient’s risk of pressure ulcer Numerical score assigned to each category depending on patient’s needs and level of assistance Lower the score, the more unlikely patient will develop a pressure ulcer Cleaning a pressure ulcer 1. Clean with each dressing change 2. Use careful, gentle motions to minimize trauma 3. Use normal saline to irrigate & clean ulcer 4. Report any drainage or necrotic tissue How a wound heals: Primary intention—little tissue loss Secondary intention—much tissue loss Phases of Wound Healing Hemostasis phase—occurs immediately following injury o Blood vessels constrict and blood clotting is initiated o Blood vessels dilate and capillary permeability increases Inflammatory phase—WBC move to wound o Individual may present with an elevated body temperature and generalized malaise Proliferation (Regenerative) Phase—begins within 2-3 days after injury and may last up to 2-3 weeks o New tissue begins to fill wound space o Capillaries begin growing across wound o Granulation tissue forms across wound Maturation phase—collagen remodeled making healed wound stronger o Begins approximately 3 weeks after injury o Continues for months or years Types of Wound Drainage 1. Serous—consists mostly of serum 2. Purulent—drainage containing pus 3. Sanguineous—consisting of large amount of RBC 4. Serosanguinous—consisting of serum & blood tinged drainage (pinkish) Surgical Drains—Provide drainage from wounds 1. Penrose drain—open drainage system 2. Jackson Pratt and Hemovac—closed system collection devises that utilize suction Wound Complications External hemorrhage—persistent bleeding; easily recognized Internal hemorrhage—swelling or hematoma Infection—elevated temperature o Warmth & swelling, pain, erythema, foul odor Dehiscence—partial or total rupturing of the abdominal surgical wound Evisceration—protrusion of intestines through abdominal wound Wound Care—Color Code Red—proliferative stage of healing; wound has granulation tissue Yellow—characterized by oozing; purulent drainage Black—covered with thick eschar; necrotic tissue Mixed—contains components of RYB wounds Purpose of Wound Dressings 1. Protect wound form further injury 2. Prevent, eliminate, or control infection 3. Absorb drainage 4. Prevent hemorrhage 5. Protect skin surrounding wound Types of Dressings Location and size of wound Amount of drainage Whether or not wound is infected Type of wound edges Cleaning Wounds Doctor's orders Clean to dirty Solutions should be body temperature Don’t clean wound with granulation tissues Don’t clean wound with cotton Wound Assessment—inspect for sight and smell Palpation for appearance, drainage, and pain Suture, drains or tubes, manifestations of complications Applying heat—causes vasodilation and increases blood flow Applying cold—causes vasoconstriction and decreases the blood flow Situations when you would NOT use heat/cold Patients who have neurosensory or mental impairment Patients who have impaired circulation When applying heat/cold: Determine patient’s ability to tolerate therapy Identify conditions that would contraindicate therapy Assess area reassess after 15 minutes Instruct patient to report discomfort Record patient’s response to therapy Lecture 4: Nursing Process 5 step process that provides an orderly, logical problem-solving approach for administering nursing care so that the client’s needs are met comprehensively and effectively STEP 1: ASSESSMENT—systematic and continuous collection, analysis, validation, and communication of patient data Complete subjective & objective data Reflects data that comes from a number of difference sources: o Patient/family o Chart—notes from staff, labs, medications, radiology Observations: vital signs, Gait, speech, interactions DATA: o o Subjective—what your patient says Objective—what you observe (physical assessment, labs, x-rays, meds, abdomen tender to touch, decreased bowel sounds, etc.) 4 types of assessments: 1. Initial assessment 2. Focused assessment 3. Emergency assessment 4. Time-lapsed assessment STEP 2: DIAGNOSIS—begins after nurse has collected and recorded patient data Identify how a person, group, or community responds to actual or potential health and life processes Identify factors that contribute to health problems (etiologies) Identify resources or strengths that the person, group, or community can draw on to prevent or resolve problems Types of Nursing Diagnoses 1. Problem-focused—ex: ineffective breathing pattern 2. Risk—ex: risk for infection 3. Health Promotion—ex: readiness for enhanced family coping PED Format 1. P—Problem or need identified from the NANDA list 2. E—Etiology or cause of human responses identified from assessment data 3. D—Defining characteristics: Signs and Symptoms Writing Diagnostic Statements 1. ONE-PART: ex: readiness for enhanced breastfeeding 2. TWO PART: risk for infection related to compromised host defenses 3. THREE PART: impaired physical mobility related to decreased muscle control as evidenced by inability to control lower Common errors in writing nursing diagnoses: Combining 2 nursing diagnoses (anxiety and fear R/T separation from parents) Relating one nursing diagnosis to another (immobility R/T pain) Making assumptions (impaired skin integrity R/T not being turned frequently) Using the medical diagnosis (self-care deficit R/T stroke) Relating the problem to an unchangeable situation (Risk for injury R/T blindness) Lack of specificity (constipation R/T nutritional intake) STEP 3: PLANNING/OUTCOMES Goal—aim or an end Patient outcome—expected conclusion to a patient health problem o Goal, outcome, objective are often used interchangeably Expected outcome—more specific, measurable criteria used to evaluate the extent to which a goal has been met Standard—for every Nursing Diagnosis we create: 2 short term goals—hours/days o Focus on patient problem goals designed to alleviate problem o STO must dictate nursing interventions o Examples: By end of shift, patient will consume 5 cups of fluid Patient will ambulate in the hall 30 feet 3 times by end of shift 1 long term goal—1 week or greater in time o By discharge, patient will verbalize 5/5 side effects of opioid use o Within 3 weeks, caregiver will return demonstrate with 100% accuracy the digital stimulation technique STEP 4: IMPLEMENTATION/INTERVENTIONS Implementing—evidence-based nursing actions planned are carried out Purpose: help patient achieve valued health outcomes, prevent disease and illness, restore health, & facilitating coping with altered functioning MEPLAN: Medications, Education, Procedures, Lab and other diagnostic data, Assessments, Nutrition Independent—actions that the nurse is able to initiate independently Dependent—interventions that require an order from another health care provider such as a physician Collaborative—require participation of multiple members of the health care team Nursing Interventions Specific and clearly stated Begins with action verb What will the nurse do how, when, where, time, frequency, amount? Implementation—performing a task and documentation of each intervention o BEFORE: consider communication barriers, diverse cultural practices, & scope of nursing practice Providing Indirect Care Indirect care—nursing interventions that are performed to benefit patients but do not involve face-to-face contact with the patients Communication & collaboration Referrals Research Advocacy Delegation Prevention-oriented interventions—prevent illness or complications & promote health activities or lifestyles o Risk factor modification o Placing infants on back to sleep o Immunization programs o Being current in evidence-based practice enhances nurse’s ability to include preventative interventions in plans of care Interventions Diversity considerations: assess needs & collaborate with patient/family Life span: interventions must always be age or developmental level appropriate Culture, Ethnicity, & Religion: consider how they affect communication & provision of care Disability: individualized care is essential **MUST be supported by scientific rationales o Ensures that the intervention is based on accepted nursing practice reflecting knowledge of scientific principles, nursing standards of care, & agency policies STEP 5: EVALUATION—nurse & patient together measure how well patient has achieved the outcomes specified in the care plan Care plan evaluation: o Patient goal/outcome attainment? o Continue? o Revise/adapt? o Discontinue? Based on patient’s responses to care plan, nurse decides to o Terminate care plan when each expected outcome is achieved o Modify care plan if there are difficulties achieving outcomes o Continue the care plan if more time is needed to achieve outcomes Nurse should make 1 of 3 decisions/judgments: o Outcome was achieved. o Outcome was not achieved. o Outcome was partially achieved. Revising: o Changes in patients condition & status of goal achievement determine whether the care plan should be revised EXAMPLES: 1. GOAL: patient’s pain level with be reported as 4/10 or less in 4 hours a. Goal fully met: patient reports pain level as 2/10 in 4 hours. 2. GOAL: patient will report decreasing tobacco use from 2 packs of cigarettes per day to 1 pack per day in 2 months. a. Goal partially met: patient reports decreasing tobacco use from 2 packs a day to 1.5 packs per day in 2 months continue to implement & monitor plan. 3. GOAL: patient will report pain level as 4/10 or less in 4 hours. a. Goal not met: patient reports pain level as 6/10 in 4 hours. i. REVISION: contact provider to change pain medication regimen in order to enhance effective pain control methods OR change goal (4/10 5/10) Lecture 5: Asepsis & Infection Infection—invasion of the body by microorganisms & the subsequent proliferation of these microorganisms Infection occurs by way of a cyclic process that involves a chain of infection: 1. Infectious agent (bacteria, viruses, fungi) 2. Reservoir (animals, soil, food, water) 3. Portal of exit (respiratory, GI, genitourinary) 4. Means of transmission (direct contact/indirect contact) 5. Portals of entry (skin, GI, respiratory, & urinary) 6. Susceptible host (hospitalized patient with a weakened immune system) Stages of Infection 1. Incubation Period—interval between pathogen’s invasion of the body and appearance of symptoms of infection a. Length of incubation period varies depending on illness 2. Prodromal Stage—period when individual is most infectious a. Could see fatigue and low-grade fever b. During this phase, patient is unaware of being contagious 3. Full Stage of Illness—presence of specific signs and symptoms a. Patient may display severity of manifestations from the infectious agent b. Symptoms may be local or systemic 4. Convalescent Period—recovery from infection a. Signs & symptoms disappear and patient returns to healthy state Drug-Resistance Microbial Strains Over prescription of antibiotics Inappropriate or incomplete use of antibiotics Individuals harboring/spreading resistant microorganisms Increased use of antibiotics in farming EXAMPLE: Methicillin-resistant Staphylococcus aureus (MRSA) Nosocomial infections—infections that develop within a healthcare setting or shortly following discharge Risk factors contributing to spread of nosocomial infections: Environment Therapeutic regime Patient resistance Populations predisposed to infections: older adults o Pulmonary infections o Urinary tract infections o Skin infection Diagnosing an Infection 1. Vital signs o Increased temp localized, elevated blood sugar, delayed wound healing, systemically, increased oral temperature, increased respiratory rate 2. Lab values o WBCs: neutrophils, leukocytes, monocytes, lymphocytes, granulocytes, basophils, eosinophils 3. Cultures v. analysis o Difference: specific organism & most effective antibiotic Standard Vital Signs Temperature o Oral—98.6 (plus or minus 1 degree) o Rectal—99.6 o Axillary—97.6 Pulse—60-100 beats/minute Respiration—10-20 breaths/minute Presence of Infectious Agents Gram-Positive Bacteria (Staphylococci)—commonly found in wound infections/food poisoning o Streptococci—contribute to skin, wound, and respiratory infections Gram-Negative Bacteria—commonly associated with nosocomial infections o Most common: UTI Wound Culture Some bacteria are aerobic, some anaerobic Some bacteria in clusters, some in chains Cultures can distinguish and discern types of bacteria Asepsis—make free from disease-producing organisms Absence of disease-causing microorganisms Medical asepsis—measures taken to either control and/or reduce the number of pathogens present Surgical asepsis—an area that is free of all microorganisms o Use to prevent introducing microorganisms from the environment into the patient Anatomic & Mechanical Barriers Intact skin, mucus membranes, tears, saliva, urine, bowel peristalsis Inflammatory Response—our body’s response to tissue injury caused by microbial invasion Attempts to limit the tissue injury’s extent Redness & warmth Swelling & pain Fever **erythrocyte sedimentation lab is reviewed to see if inflammation is present Stages of Inflammatory Response 1. Vascular response—small blood vessels dilate o Increased fluid in the interstitial spaces o Blood flow slows down 2. Exudate production o Serous, purulent (dead phagocytes & tissue cells), sanguineous, serosanguineous 3. Reparative phase—granulation process is the replacing the injured/destroyed tissue with identical cells o Scar tissue develops when injured/destroyed tissue cannot be repaired Individuals who might be compromised: 1. Breaks in skin or mucus membrane o Invasive devises—provides portal of entry for microorganisms 2. Static body fluids o Stasis of body fluids—stagnant body fluids (secretions in lungs or urine from bladder) in body provides warm, moist environment fostering bacterial growth 3. Poor nutritional state o Resistance to infection depends upon a healthy nutritional state 4. Stress o Increases levels of cortisone in blood thereby increasing a person’s susceptibility to infection o Prolonged elevation of cortisone levels inhibit the inflammatory process 5. Medications o Drug therapy may compromise a person’s response to infection o Chemotherapy, steroid therapy, antibiotic therapy 6. Chronic disease o Diseases lessen the body’s defense against infection places the patient at risk o Diabetes, Leukemia Types of Infection 1. Local v. Systemic 2. Acute v. Chronic Standard precautions—used when caring for all patients regardless of their diagnosis Airborne precautions—used to protect against microorganisms transmitted by small-particles that can remain suspended and become widely dispersed by air currents TB or Measles 1. Handwashing after all patient/environmental contact & glove removal 2. Negative pressure room with door closed 3. N95 particulate respirator required prior to room entry Droplet precautions—used to protect against microorganisms transmitted by larger-particle droplets Droplets are usually larger than 6 microns Mumps, pneumonia, influenza 1. Handwashing after all patient/environmental contact & glove removal 2. Surgical mask and eye protection required when within 3 feet of patients 3. Gloves required for all patient/environmental contact Contact precautions—used when the organism can be transmitted by hand or skin-to-skin contact Used when patients are known or suspected of having an illness (drug-resistant pathogen) transmitted by direct contract or by contact with items in the room 1. Wear gown when entering the room 2. Wear gloves when entering the room 3. Wash hands before leaving the room Clostridium difficile (C-Diff) Exposure to antibiotics Frequent cause of hospital-acquired diarrhea Accounts for almost 25% of antibiotic-associated diarrhea Treatment: o Antibiotics—Flagyl P.O. for 10-14 days o Force fluids to prevent dehydration Prevention—wash hands frequently o Use detergent/bleach to wash clothing soiled with stool o Wipe bathrooms surfaces with chlorine-based cleaners o If taking antibiotics, eat yogurt containing live cultures Transmission—spread via infected humans Involves someone touching a contaminated surface and then touching their mouth Contaminated environmental surfaces—beds, doorknobs, tabletops, toilets, sinks, light switches, etc. Methicillin-Resistant Staphylococcus Aureus (MRSA)—Staph Bacteria carried commonly on skin or nose Frequent cause of skin infections Most infections are minor but staph can also cause serious infections Prevention o Practice good hygiene o Wash hands thoroughly o Cover wounds until healed o Avoid sharing personal items (dry clothes in hot dryer rather than airdrying—helps kill bacteria) Treatment o Antibiotic therapy, wound therapy Control Measures Patient is placed in contact isolation Transmitted by healthcare workers from infected patients and contaminated equipment Contact isolation is discontinued with 2 cultures from the site are negative 48 hours apart from each other Protective isolation—used to prevent infection for patients whose body defenses are known to be compromised Occupational risk: puncture wounds, contact with blood/bodily fluids, mucus membranes Lecture 6: Urinary and Bowel Elimination Kidneys & Ureters Kidneys—located on either side of vertebral column behind peritoneum in upper abdominal cavity Help maintain composition and volume of body fluids Once every 30 minutes, body’s total blood volume passes through kidneys for waste removal filter & excrete blood constituents not needed & retain those that are Body fluids remain relatively stable if kidneys are functioning properly Urine— contains organic, inorganic, and liquid wastes Urination—micturition or voiding; emptying the bladder Nerve centers for urination are situated in brain & spinal cord Largely involuntary act but control can be learned Voluntary control develops as higher nerve centers develop after infancy until then, voiding is purely reflex action Autonomic bladder—people whose bladders are no longer controlled by brain because of injury/disease; REFLEX ONLY Factors affecting Urination: 1. Developmental considerations a. Toilet training—voluntary control of urethral sphincters occurs between 18-24 months b. Effects of aging: i. Nocturia—urinating at night ii. Decreased muscle tone iii. Increased risk of UTI—women, catheters, poor hygiene, incontinence iv. Neuromuscular problems—brain/spine injury, neurogenic bladder 2. Food & fluid intake a. Kidneys help maintain careful balance of fluid intake & output—EQUAL b. When body is dehydrated, kidneys reabsorb fluid i. Urine produced Is more concentrated & decreased in amount c. Fluid overload, kidneys excrete large quantity of dilute urine d. DEHYDRATED = REABSORB FLUID e. CONCENTRATED = DECREASED AMOUNTS f. FLUID OVERLOAD = EXCRETION OF LARGE AMOUNTS OF DILUTED URINE 3. Psychological variables a. Individual preferences b. Family influences c. Social cultural variables d. Embarrassment e. Anxiety i. Stress can interfere with ability to relax perineal muscles & external urethral sphincter 4. Activity & muscle tone a. Aging: i. Bladder shrinks—holds about half of what younger bladder holds ii. Need to empty smaller amounts from bladders more frequently iii. Bladder becomes thinner and muscle tone decreases 5. 6. iv. Urine stream is weaker v. Bladder does not empty completely b. Benefits of regular exercise: i. Increased metabolism & optimal urine production/elimination c. Prolonged periods of immobility lead to decreased bladder/sphincter tone poor urinary control & urinary stasis d. People with indwelling catheters lose bladder tone because bladder muscle is not stretched by bladder filling with urine e. Other causes of decreased muscle tone: childbearing, muscle atrophy due to increased estrogen levels (menopause), & damage to muscles from trauma Pathologic conditions a. Congenital urinary tract abnormalities b. Polycystic kidney disease c. UTI d. Urinary caliculi e. Hypertension f. Diabetes mellitus g. Gout h. Renal Failure—kidneys fail to remove metabolic end products from blood & are unable to regulate fluid, electrolyte and pH balance i. Acute Kidney Injury—acute renal failure; sudden decline in kidney function 1. May be caused by severe dehydration, anaphylactic shock, sepsis & urethral obstruction ii. Chronic Kidney Disease—slow loss of kidney function over months or years as result of irreparable damage to kidneys 1. Caused by conditions such as diabetes, hypertension, & glomerulonephritis 2. Progression of CKD will eventually lead to final stage of CKD—End-Stage Renal Disease (ESRD) or kidney (renal) failure 3. ESRD—kidneys are unable to adequately excrete metabolic waste & regulate fluid and electrolyte balance Medications a. Nephrotoxicity—capable of causing kidney damage b. Diuretics—prevent reabsorption of water and certain electrolytes in the tubules i. Commonly used in treatment of hypertension/other disorders ii. Cause moderate to severe increases in production and excretion of dilute urine c. Cholinergic—stimulate contraction of detrusor muscles and produce urination d. Analgesics—aspirin or ibuprofen i. Abuse can cause nephrotoxicity e. Tranquilizers i. Some analgesics and tranquilizers suppress CNS interfering with urination by diminishing effectiveness of neural reflex f. Certain drugs can cause urine to change color: i. Anticoagulants—may cause hematuria (blood in urine) pink or red color ii. Diuretics can lighten color to pale yellow iii. Phenazopyridine—urinary tract analgesic; can cause orange or orange-red urine iv. Antidepressant amitriptyline or B-complex vitamins can turn urine green or blue-green v. Levodopa (L-dopa)—anti-Parkinson drug & injectable iron compounds can lead to brown or black urine g. Illegal drugs Intake & Output—Measurement and recording of all fluid intake and output during a 24-hour period; provides data about client’s fluid & electrolyte balance Unit of measurement: mL To measure fluid intake, nurses convert household measures such as glass, cup or soup bowl to metric units o Gauge fluid balance and give valuable information about patient’s condition Accuracy of total fluid intake/output from all sources aids in identifying potential alterations in fluid balance and is essential for planning patient’s care Gloves required when handling urine Measurement of intake/output may be delegated to unlicensed personnel but nurse is responsible for ensuring staff member understands and validating accuracy of measurements Measuring Urine Output 1. Patients who are continent—have self-control over urination o Ask patient to void in bedpan, urinal, or specimen hat (container) either in bed or in bathroom o Use gloves & pour urine from collection device into measuring device calibrated in milliliters o Place calibrated container on flat surface & record amount of urine voided in electronic record o Record total amount voided during EACH SHIFT total for 24-hour period is calculated in electronic documentation software o Discard unless specimen is required 2. Patients with an indwelling catheter o Put on glovesplace calibrated measuring device between urine collection bagplace drainage spout from collection bag above but not touching the calibrated measuring device & open clampallow urine to flow from bag to device reclamp drainage tube clean and replace tube into slot on drainage bag o Catharized patients who are acutely ill may require hourly/more frequent measurements Use special collection bag with built-in calibrated measuring chamber (urimeter) 3. Patients who are incontinent—involuntary or uncontrolled loss of urine from bladder o Note number of times patient is incontinent & any notable urine characteristics (color & odor) o Use scheduled toileting—can assist in obtaining urine for measurement and specimens and prevent incontinence o Alternative method: measurement of urinary output via weighing of absorbent pads Dry pad subtracted from wet pad weight The Nursing Process for Urinary Elimination 1. Assessing a. Function b. Nursing History c. Physical Assessment 2. Diagnosing 3. Outcome Identification and Planning 4. Implementing Urinary Problems Anuria—24-hour urine output is less than 50 mL Dysuria—painful or difficult urination Glycosuria—glucose in the urine Nocturia—awakening in the night to urinate Oliguria—24-hour urine output is less than 400mL Polyuria—excessive output of urine (diuresis) Proteinuria—protein in the urine Pyuria—pus in the urine Urgency—strong desire to void Urinary incontinence—involuntary loss of urine Urinary Retention Patient is voiding small amounts frequently Complains of LOWER abdominal pain Bladder is palpable Voiding 25-50 cc at frequent intervals Bladder does not empty completely 2 forms—acute & chronic Affects both men and women but occurs more often in men Post Void Residual (PVR)—amount of urine in the bladder after a voluntary void; functions as diagnostic tool Bedside scanner assesses fullness of bladder Results are more accurate when patient is in supine position Diagnosing 1. Urodynamic Studies—assesses how the bladder and urethra are performing their job of storing and releasing urine o Can help explain symptoms such as incontinence, frequent urination, or sudden, strong urges to urinate but nothing comes out 2. Cystoscopy—procedure that examines the lining of the bladder & urethra o Cystoscope—hollow tube equipped with a lens that is inserted into urethra and slowly advanced into bladder 3. Intravenous Pyelogram—excretory urogram; X-ray of urinary tract o Can view kidneys, bladder, & ureters 4. Retrograde Pyelogram—imaging that uses x-rays to look at bladder, ureters, and kidneys o Test is usually done during cystoscopy o Uses endoscope (long, flexible, lighted tube) 5. Renal Ultrasound—safe and painless test that uses sound waves to make images of the kidneys, ureters, and bladder Collecting Urine Specimens Routine Urinalysis Clean-Catch or Midstream Specimen Sterile Specimen Urine Specimens from Urinary Diversion 24-Hour Urine Specimens Urine specific gravity—fall between 1.002—1.030 if kidneys are functioning properly o Specific gravity results above 1.010 can indicate mild dehydration o Higher the number, more dehydrated you may be Types of Incontinence 1. Stress incontinence—due to increased abdominal pressure under stress (weak pelvic floor muscles) 2. Urge incontinence—due to involuntary contraction of bladder muscles 3. Overflow incontinence—due to blockage of urethra 4. Neurogenic incontinence—due to impaired functioning of nervous system Characteristics of Urine 1. Color a. Clear—drinking more water than the daily recommended amount of water b. Yellowish to amber—typical urine color c. Can be red/pink, orange, blue or green, dark brown, cloudy 2. Odor 3. Turbidity a. Cloudy or foamy urine—occasionally occur due to mild dehydration 4. pH—Normal urine pH: slightly acidic usual values of 6-7.5 but normal is 4.5-8 5. Specific gravity—measure of urine concentration a. Fall between 1.005—1.030 if kidneys are functioning properly b. Specific gravity results above 1.010 can indicate mild dehydration c. Higher the number, more dehydrated you may be 6. Check for abnormal constituents—protein, blood, glucose, ketone bodies, bacteria Urine Test Specific Gravity (1.005—1.030) Urinary pH (6.0) o 7.0—neutral, <7—acid, >7—alkaline Implementing—Promoting Normal Urination Maintaining normal voiding habits Promoting fluid intake Strengthening muscle tone o Weakening of pelvic floor muscles is common cause of urinary incontinence problems in men & women o PFMT (pelvic floor muscle tone) can improve voluntary control of urination and significantly reduce or eliminate problems with stress incontinence by strengthening perineal and abdominal muscle tone PFMT—Kegel exercises target inner muscles that lie under and support bladder Same muscles that patient contracts to stop urinating in midstream or to control defecation Encourage patient to perform these multiple times a day for at least 3 months Can also be accomplished by using vaginal weights When to Increase Fluid Intake 1. Profuse sweating—diaphoresis 2. Vomiting—diarrhea 3. Gastric suctioning 4. Excessive wound drainage 5. 6. 7. 8. UTI Renal stones Foley has dark urine **Skin Integrity & Hydration—check skin carefully for color, texture, and turgor o Problems with incontinence may result in severe excoriation Adults with no disease-related fluid restrictions should drink 2,000-2,400 mL(8-10 8oz glasses) of fluid daily o If good proportion of daily fluid intake is water, kidneys & urinary structures are well flushed waste products (including harmful bacteria) are removed When to Decrease Fluid Intake 1. Patients in renal failure 2. Patients in congestive heart failure (CHF) 3. Hyponatremia Catheterizing the Patient’s Bladders CAUTI’s are most common HAIs in the US best way to prevent is to avoid inserting an unnecessary indwelling urinary catheter When it is deemed necessary, it should be performed using strict aseptic technique and left in place only as long as needed Reasons for Urinary Catheterization 1. Urinary retention o Often temporary and common after surgery involving lower abdomen, pelvis, bladder, or urethra (especially if abdomen is delayed, fluid intake is minimal, or epidural analgesia is used for pain control) 2. Bladder outlet obstruction o Including mechanical obstruction (swelling at meatus) or enlarged prostate o Patients who are unable to use any other bladder management method (those with neurogenic bladder dysfunction related to disability) require long-term use of indwelling catheter 3. Obtaining a sterile urine specimen o When patient is unable to voluntarily void o Obtained from the catheter using the special port for specimens specimen from the drainage bag may not be fresh and give an inaccurate analysis 4. Accurate measurement of output—critically ill patients 5. Wound healing o Assist in healing open sacral or perineal wounds in incontinent patients o Emptying bladder before, during, or after select surgical procedures and before certain diagnostic examinations 6. Comfort at end-of-life care 7. Prolonged immobilization—unstable thoracic or lumbar spine, multiple traumatic injuries Indwelling-Catheter Specimen 1. Size of syringe depends on specific lab test—urine culture requires 3mL, but routine urinalysis requires at least 10mL 2. Check catheter to determine if access port for specimen removal is present 3. If urine is not present in the tube, clamp tube below the access port briefly to allow urine to accumulate (no more than 30 min) 4. Clean access port with antiseptic swab & carefully attach syringe to the port 5. Aspirate urine into the syringe & remove syringe 6. Release clamp if it was used and transfer specimen to appropriate container 7. LABEL SPECIMEN: name, date, time of collection Urinary Catheters 1. Straight catheter—just to empty bladder; also called in and out 2. Retention catheter—indwelling urinary catheter (IUC) or Foley catheter a. Closed sterile system with a catheter and retention balloon that is inserted either through urethra or suprapubically to allow for bladder drainage 3. Three-way catheter a. Long flexible tube with drainage eyes and retention balloon on one end & 3 collectors at other end b. Recommended for prostate tumor, post urological surgery or in situations where there is bleeding from bladder Catheter-associated Harm 1. UTI—#1 cause of nosocomial infection a. Indwelling catheters are associated with development of a biofilm (living layer of bacteria) increases infection risk b. When catheter is left in place, organisms may move up the catheter lumen or in space between catheter and urethral wall i. Bacteriuria—bacteria in urine; asymptomatic 2. Trauma—ureter or bladder 3. Pain 4. Bladder spasms 5. Sepsis Male urethra especially vulnerable to injury because of its longer length 1. Mucous membrane lining urethra is delicate and damaged easily by friction resulting from insertion of a catheter Caring for patients with Urinary Tract Infections Most common type of health care-associated infection (HAI) Risk factors 1. Sexually active women—perineal bacteria can migrate into urethra & bladder Women who use diaphragms for contraception—spermicide use decreases amount of normally protective vaginal flora 2. Postmenopausal women Urinary stasis (common at this age)—provides optimal environment for bacteria to multiply Decreased estrogen contributes to loss of protective vaginal flora 3. Indwelling urinary catheter Bacteria travel through or around catheter and into bladder 75% of UTI’s associated with presence of indwelling catheter Catheter-associated UTI (CAUTI)—increases healthcare costs & is associated with morbidity and mortality No additional payment is provided to hospitals for CAUTI treatment-related costs Most pathogens are introduced via handling of catheter and drainage device after placement 4. DM—changes in body’s defense system may increase risk 5. Older adults—physiological changes predispose older people to development of UTI’s Enlargement of prostate as men age can contribute to development of UTI’s in older men Clean Catch—Mid Stream Non-sterile urine collection Teach patients how to wipe Urinate into the toilet Urinate into the cup Finish in the toilet Patient Goals—MAINTIAN NORMAL VOIDING HABITS 1. Schedule—offer every 2 hours a. Support usual urinating pattern as much as possible 2. Identify and respond to urge to void 3. Provide privacy 4. Position (stand or sit) 5. Hygiene—prevent infection Nursing Interventions Maintain a closed system Provide catheter care Force fluids (if condition permits) Accurate I&O Urinary bag must remain lower than bladder Bowel Elimination Defecation—act of expelling feces from the body Anatomy and Physiology GI tract—extends from mouth to anus Stomach—J shaped, hollow, muscular organ located in left upper portion of abdomen o Stores foods during eating, secretes digestive fluids, churns food to aid in digestion and pushes partially digested food (chyme) into small intestine o Pyloric sphincter—muscular ring that regulates size of opening at end of stomach; controls movement of chyme from stomach to small intestine Small Intestine—duodenum, jejunum, ileum (part that connects with large intestine) o Secretes enzymes that digest proteins and carbohydrates o Digestive juices from liver and pancreas enter through small opening in duodenum o Responsible for digestion of food and absorption of nutrients into bloodstream Large intestine—colon; connected to ileum by ileocecal valve o Valve normally prevents contents from entering large intestine prematurely and prevents waste products from returning to small intestine o Primary organ of bowel elimination o 1st part of Large Intestine—cecum—digestive contents enter the colon consisting of several segments Ascending colon from cecum upward towards liver, turns to cross the abdomen at hepatic flexure Becomes transverse colon—crossing abdomen from right to left Turns at splenic flexure and becomes descending colon—passes down left side of body to sigmoid colon Sigmoid colon—contains feces o o Once excreted, feces are called stool Empties into rectum Rectum—last part of large intestine; 3 transverse folds of tissue to help hold in fecal material temporarily Vertical folds present—each contain an artery & veinhemorrhoids occur here Empty except immediately before and during defecation Excreted through anus Functions: Absorption of water, formation of feces, & expulsion of feces from body Bacteria reside and act on food residue while it makes its way through the large intestine Bacterial action produces vitamin K & some of the B-complex vitamins Approximately 1,500 mL of chyme enters large intestine daily Ascending = up (liquid) Transverse = across (foul smelling) Descending = down (semi-formed) Rectum (formed) Functions of Colon 1. Absorption of water and nutrients 2. Secretion of mucus 3. Elimination of flatus 4. Elimination of feces Nervous System Control—innervates muscles of the colon Contractions of the circular and longitudinal muscles of the intestine, peristalsis, occur every 3-12 minutes moving waste products along the length of the intestine continuously Mass peristalsis sweeps occur 1-4 times each 24-hour period in most people o Occurs after food has been ingested o 1/3 – 1/2 of ingested food is normally excreted in stool within 24 hours, remainder within the next 24-48 hours Waste products are stopped from exiting by anal sphincters o Internal sphincter—mostly of involuntary smooth muscle innervated by autonomic nervous system Motor impulses are carried by sympathetic system (thoracolumbar) and inhibitory impulses are carried by parasympathetic system (craniosacral) 2 divisions of ANS function antagonistically in dynamic equilibrium o External sphincter—striated muscle tissue; voluntary control Levator ani muscle reinforces action of external sphincter Peristalsis—wave like movement of intestinal wall Defecation 2 centers govern the reflex to defecate—one in medulla and a subsidiary one in spinal cord o Parasympathetic stimulation occursinternal anal sphincter relaxes & colon contracts fecal mass enters rectumrectum becomes distended by fecal mass (primary stimulus for defecation reflex) o Rectum distension increases intrarectal pressure causes muscles to stretch & stimulates defecation reflex/urge to eliminate External anal sphincter is constricted or relaxed at will o During defecation, several additional muscles aid in the process Voluntary contraction of abdominal wall by holding one’s breath, contacting diaphragm, & closing the glottis increase intra-abdominal pressure 3-4x the normal pressure helps expel feces Muscles on pelvic floor contract Defecation is eased by flexing the thigh muscles—increases abdominal pressure Eased by the sitting position—increases downward pressure on rectum o If urge to defecate is ignored, it can be delayed by voluntarily contracting external anal sphincter and pelvic floor muscles VALSALVA MANEUVER—bearing down to have a bowel movement o o o When a person bears down to defecate, the increased pressures in abdominal and thoracic cavities result in decreased blood flow to atria and ventricles reducing cardiac output Bearing down ceases pressure is lessened & lager than normal amount of blood returns to the heart This may cause the heart rate to slow and result in syncope in some patients This maneuver may be contraindicated in people with cardiovascular problems Stool: Normal Characteristics & Special Considerations for Observation 1. Volume 2. Color 3. Odor 4. Consistency 5. Shape 6. Constituents Warning Signs of Colon Cancer 1. Rectal bleeding 2. Change in bowel elimination pattern 3. Blood in the stool 4. Cramping pain in the lower abdomen Factors Affecting Bowel Elimination 1. Age a. Affects what a person eats and the body’s ability to digest nutrients and eliminate wastes b. Older adult constipation—often a chronic problem for older adults i. Rectal receptors have decreased response to stretching which leads to a decreased urge to move the bowels despite a large amount of stool in the rectum c. Diarrhea, fecal impaction or fecal incontinence can also result from physiologic or lifestyle changes i. Fecal impaction—prolonged retention or an accumulation of fecal material that forms a hardened mass in the rectum ii. Fecal incontinence—involuntary or inappropriate passing of stool of flatus 2. Daily patterns a. Most people have individual patterns of bowel elimination involving frequency, timing considerations, position, and place changes may upset a person’s routine/lead to constipation b. Many people defecate after breakfast when gastrocolic and duodenocolic reflexes cause mass propulsive movements in the large intestine 3. Food and fluid a. Type and amount of foods eaten & number of fluids ingested affect elimination i. High fiber diet of 25-30g & daily fluids intake of 2000-3000mL facilitate bowel elimination b. High fiber foods increase bulk in fecal material bulkier feces increase pressure on intestinal wall which serves as stimulus for peristalsis i. Feces moves more quickly through colon, allowing less time for water to be reabsorbed stool is soft and easy to pass ii. There is also less time for toxins to be absorbed from feces by colon preventing their absorption by colon is a key part of cancer prevention c. People digest & tolerate foods differently (determined in part by culture) d. Food intolerance may alter bowel elimination—lactose intolerance e. Certain foods are associated with specific effects on bowel elimination i. Constipating foods: cheese, lean meat, eggs, pasta, rice, white bread, iron, calcium supplements ii. Laxative effect: certain fruits/vegetables, bran, chocolate, spicy foods, alcohol, coffee 4. 5. 6. 7. iii. Gas producing foods: onions, cabbage, beans, cauliflower Activity and muscle tone a. Regular exercise improves GI motility and muscle tone, inactivity decreases both b. Adequate tone in abdominal muscles, diaphragm, and perineal muscles are essential for ease of defecation c. Bedrest patients—constipation risk Lifestyle a. Individual, family, & sociocultural variables can influence a person’s usual elimination habits b. Long-term effects of bowel-training may result in a person’s: i. Acceptance of bowel elimination as a normal life process ii. Preoccupation with bowel elimination iii. Feeling that bowel elimination is a dirty process c. A person’s daily schedule, occupation, & leisure activities can contribute to a habit of defecating at regular times or to an irregular pattern Psychological Variables a. Pathologic processes may change a person’s usual bowel elimination habits i. Changes in stool characteristics may be one of the 1st clinical manifestations of a disease b. Medications also influence of stool for variety of reasons i. Any drugs that may cause GI bleeding (anticoagulants/aspirin products) may cause stool to appear pink to red to black ii. Bismuth subsalicylate (treats diarrhea) may cause black stools iii. Antacids—may cause white discoloration or speckling in stool iv. Antibiotics—may cause green-gray color related to impaired digestion c. Diarrhea or constipation are common signs of potential disease processes i. Diarrhea—may result from: 1. Bacterial & viral infection 2. Malabsorption syndromes—inability of digestive system to absorb 1 or more of the major vitamins, minerals, or nutrients 3. Neoplastic diseases—tumors 4. Diabetic neuropathy—damage to nerve cells 5. Hyperthyroidism 6. Uremia—retention of urea in blood 7. Outbreaks of food poisoning ii. Severe abdominal cramping followed by watery or bloody diarrhea may signal a microbial infection iii. Constipation—may be caused by: 1. Disease within colon or rectum 2. Injury to or degeneration of the spinal cord 3. Megacolon—extremely dilated colon iv. Mechanical obstructions—blocks normal flow of intestinal contents through the intestinal tract 1. Result from pressure on intestinal walls 2. Common causes: tumors, diverticulum, adhesions from scar tissue, stenosis, strictures, & hernia and volvulus (twisting of part of the colon) v. Nonmechanical obstructions—inability of the intestinal musculature to move contents through the bowel 1. Disease that weakens or paralyze the intestinal walls—muscular dystrophy, DM, Parkinson’s vi. Manipulation of the bowel during surgery may result in paralytic ileus Medications a. Narcotics i. Opioids—common cause of medication-induced constipation ii. The enteric neurons control major body functions such as bowel control 1. Opioid-binding receptors are found in enteric neurons in GI tract binding of these interrupts peristalsis, causing slowed movement of stool through the colon & increased reabsorption of fluid in the large intestine b. Laxatives—promote peristalsis i. Antidiarrheal medications—inhibit peristalsis c. Antibiotics i. Diarrhea is a potential adverse effect of treatment with antibiotics ii. Antibiotics are used so extensively in health care settings, many patients are at risk for Clostridium difficile 1. Disruption in normal intestinal flora allowing microorganisms to flourish in the intestine 2. Causes intestinal mucosal damage/inflammation results in diarrhea & abdominal cramping 3. C. difficile spores are shed in feces & relatively resistance to disinfectants a. Can be spread on hands of health care providers after contact d. Antacids—containing aluminum, iron sulfate, and anticholinergic medications also decrease GI motility i. Over the counter antacids may cause magnesium which can cause diarrhea e. Metformin—common medication to treat DM Type II; can cause diarrhea Surgery & Anesthesia Paralytic ileus—temporary stoppage of peristalsis; can be caused by direct manipulation of bowel during surgery o Often, patients are receiving antibiotics which can exacerbate the situation o If this persists, distension & symptoms of acute obstruction may occur may need surgical intervention Inhaled general anesthesia can also inhibit peristalsis by blocking parasympathetic impulses to intestinal musculature o Local & regional anesthetics have little effect on peristalsis Stool Collection 1. Practice medical asepsis a. Disposable gloves, hand hygiene before and after 2. Do not contaminate container 3. Label specimen 4. Hematest for occult blood Direct visualization Studies Endoscopy—direct visual examination of body organs or cavities o Done using a fiberoptic endoscope—long, flexible tube containing glass fibers that transmit light to the organ & return an image o Pincers may be inserted to obtain a tissue sample for biopsy o View integrity of mucosa, blood vessels, & specific organ parts o Helpful for diagnosing inflammatory, ulcerative, & infectious diseases, benign & malignant neoplasms, & other lesions of the esophageal, gastric, & intestinal mucosa o Include: EGD, colonoscopy, sigmoidoscopy Esophagogastroduodenoscopy (EGD)—visual examination of the esophagus, stomach & duodenum Colonoscopy—visual examination of the large intestine from the anus to the ileocecal valve Sigmoidoscopy—visual examination of the sigmoid colon, rectum, & anal canal Upper GI Barium Enema Enemas—introduction of a solution into the large intestine, usually to remove feces Can also administer certain medications Instilled solution distends the intestine and irritates the intestinal mucosa, increasing peristalsis Generally classified as cleaning or retention enemas Discouraged for use with myelosuppressed patients and/or patients at risk for myelosuppression & mucositis because they can lead to bleeding, anal fissures, or abscesses Should also be avoided in those with bowel obstruction or paralytic ileus—can increase risk of perforation Cleansing Enemas Preoperative—prevent involuntary escape of fecal material during surgical procedures Diagnostic procedures—promote visualization of intestinal tract by radiographic or instrument examination Constipation—used to relieve constipation or fecal impaction Help establish regular bowel function during a bowel-training program Most common types of solutions: tap water, normal saline solution, soap solution, and hypertonic solution o Hypotonic (tap water) & isotonic (normal saline solution)—large volume enemas that result in rapid colonic emptying May be dangerous for patients with weakened intestinal walls o Hypertonic salutations—available commercially & are administered in smaller volumes Draw water into the colon which stimulates defecation reflex May be contraindicated in patients for whom sodium retention is a problem May be contraindicated for patients with renal impairment or reduced renal clearance—compromised ability to excrete phosphate adequately hyperphosphatemia Hypertonic Solution Enema—fleets enema (saline) o Administer 70-139 mL o Stimulates peristalsis Hypotonic Solution—tap water o Administer 500-1000mL o Cleanses colon rapidly o Administer cautiously—assess or signs of circulatory overload Retention Enema—oil based o 150-200mL solution o Lubricates/softens o Retained in bowel for prolonged period o Lubricate stool & intestinal mucosa making defecation easier o Carminative enemas—help expel flatus from rectum and provide relief from gaseous distension o Common solutions: milk and molasses, magnesium-sulfate—glycerin—water (MGW) enema o Medicated enemas—provide medications that are absorbed through rectal mucosa o Anthelmintic enemas—destroy intestinal parasites High Enemas—cleans as much of the colon as possible Low Enemas—clean the rectum & sigmoid colon Administering an Enema 1. Left lateral position 2. Hold container no higher than 12-18 inches 3. Administer no more than 1000cc 4. Solution temp between 105-110 degrees 5. Don’t instill air 6. Insert tube slowly—between 3-4 inches 7. C/O pain—STOP—restart slower rate Retaining the Enema Cleansing Enema—retain 5-10 minutes Retention Enema—retain 30 minutes Document 1. Type of solution 2. Amount of solution 3. Length of time solution retained 4. Describe returns Meeting the Needs of Patients with Bowel Diversions Ostomy—surgically formed opening from the inside of an organ to the outside o Intestinal mucosa is brought out to the abdominal wall & a stoma—part of ostomy attached to the skin—is formed by suturing the mucosa to the skin Ileostomy—allows liquid fecal content from the ileum of the small intestine to be eliminated through the stoma Colostomy—permits formed feces in the colon to exit through the stoma Bowel Diversion Ostomies Ostomy—opening into the abdominal wall Ileostomy—opening into the ileum Colostomy—opening into the colon May be either temporary or permanent o Temporary ostomies—performed to allow the intestine to repair itself after inflammatory disease, some types of intestinal surgery, or injury Patient returns for a second surgery in several weeks & intestine is reconnected o Permanent ostomies—performed for debilitating intestinal or cancer of colon or rectum Restorative proctocolectomy ileal pouch—anal anastomosis (IPAA)—surgical intervention that does not involve an external stoma o o o Also called J pouch or internal pouch Commonly considered for use in those patients with inflammatory bowel disease, (ulcerative colitis) Involves removal of colon and rectum, but leaves anus intact small intestine is sutured directly to the anus—creates a colonlike pouch o Patient is able to control expulsion of feces through the intact internal & external anal sphincter Care for patient: o Remove and change non-drainable pouches when they are half full o Inspect stoma regularly—should be dark pink to red and moist Pale stoma—may indicate anemia Dark purple/blue—may reflect compromised circulation or ischemia Bleeding around the stoma & its stem should be minimal Most protrude ½-1 inch from abdominal surface & appear swollen & edematous initially Check dressing frequently Yeast infections can occur around stoma if not kept dry o Record intake and output every 4 hours for the first few days after surgery Bowel Classification Temporary—allows the affected portion to rest & heal Permanent—provides a means for elimination Colostomy Sites Ostomy should protect the skin, collect fecal discharge, and control odor Normally does not produce drainage until normal peristalsis returns o Ileostomy drains within 24-48 hours because of liquid contents in small intestine For 1st few days, most patients wear an open-ended appliance that allows for drainage of fecal material without removing the appliance Ileostomy & ascending colostomy—produce liquid stools Transverse colostomy—produce foul odors Descending colostomy—produce semi-solid stools Colostomy Irrigation—used to promote regular evacuation of distal colostomies Ileostomies—not irrigated because the fecal content of ileum is liquid and cannot be controlled Water is inserted into the colostomy & water/feces are expelled into irrigation sleeve Patient can wear stoma caps that soak up discharge and a flatus filter Living with an Ostomy Liquid medications If rectum is removed, no enemas or suppositories & no rectal temperature Patients experience a loss of independence and body image disturbances Patient education—essential for independence in self-care Ileostomies—ensure adequate daily fluid intake to avoid dehydration and fluid electrolyte imbalances due to large fluid output o Output is high in potassium & sodium—important that electrolytes are monitored closely o Tendency to develop food blockages & fiber blockages Lecture 7: Teaching & Learning Patient Education Seen in a variety of healthcare settings Patients & their families have a right to healthcare education A well-designed teaching plan that fits the patient’s learning needs can: o Help reduce healthcare costs o Improve quality of care o Help the patient gain more independence Joint Commission on Accreditation of Healthcare Organizations Throughout the patient’s stay, the patient & their family receive education specific to the patient’s healthcare needs. This includes information regarding proper administration of medications, proper use of hospital equipment, and instructions on how to obtain followup care after discharge. This standard is accomplished by nurse’s ability to: o Accurately assess the patient’s educational needs o Include the patient/family in the teaching plan o Evaluate the learning Comprehensive Patient Education 1. Health promotion o Promoting healthy behaviors through education may assist the patient with changing/maintaining better health habits o If patients are more health conscious, they may be more likely to seek early diagnoses for health problems o Developmental o Normal child bearing, hygiene, nutrition, exercise, mental health, spiritual health 2. Illness prevention o First aid, safety, immunizations, screening, identification and management of risk factors 3. Restoration of health o Injured or ill patients need information to regain or improve their level of health (self-medicating) o Orientation to treatment center & staff, patient’s and nurses’ expectations of each other o Illness and physical condition o Medical & nursing regiments and how the patient can participate in care 4. Coping with impaired functioning o New knowledge or skills may be necessary for some patients to continue with their ADL o Education should begin when needs are identified and/or when patient/family demonstrate willingness to learn o COPE Model Creativity—generate alternatives Optimism—help patient view illness with confidence Planning—plan for future problems to reduce uncertainty Expect Information—help family get expert information from health care provider to develop a plan 5. Promoting outcomes o High level wellness and self-care practices o Disease prevention and early detection o Quick recovery with minimal or no complications o Ability to adjust to acute or chronic and terminal illness o Patient & family acceptance of lifestyle changes associated with illness or disability Teaching—deliberate set of actions that helps individual to learn Learning—change in behavior when they acquire knowledge Steps of Teaching-Learning Process 1. Assess learning needs and learning readiness—knowledge, attitude, or skills needed 2. Diagnose the patient’s learning needs—be realistic 3. Development outcomes—STO & LTO 4. Develop a teaching plan—select content, teaching strategies, or activities 5. Implement teaching plan and strategies—prepare environment, be flexible, keep teaching sessions short 6. Evaluate learning—if outcomes met, reinforce, evaluate yourself Culturally Competent Patient Teaching Understand patient culture Multicultural team Be aware of personal biases Core cultural values Written materials Health Literacy—ability to obtain, read, understand, and act on health information Internet searches, reading pamphlets, medication doses Effects all races, age, education & income groups Understood at 5th grade level Confirm the learner understands This empowers patients Identify patients at risk Effective Teachers Determine preexisting knowledge Determine learning needs Determine appropriate time to teach Maintain effective interpersonal communication o Organize information in a logical sequence o Lessons should progress from simple to complex o Clear and concise Evaluation o Have the patient demonstrate a newly learned skill. (behavior) o Have the patient repeat newly acquired knowledge. (cognitive) o Provide feedback to the learner regarding his successes and deficiencies Domains of Learning 1. Cognitive domain—understanding 2. Affective domain—attitude 3. Psychomotor domain—motor skills 1. Cognitive Learning—storage and recalling new information Knowledge: recall facts and basic concepts to recall new knowledge Comprehension: ability to understand what is learned Application: use information in a new situation, acquired information in concrete situations Analysis: draw connections among ideas, compare, contrast Synthesis: assimilating parts of information as a whole; what goes together Evaluation: justify a stand or decision; evaluate outcome 2. Affective Learning Receiving—willingness to listen Responding—active participation through listening & reacting verbally and nonverbally Valuing—attaching worth to an object Resolving conflict—acceptance of outcome 3. Psychomotor Learning Guided response—performing an act under guidance; involves imitation Mechanism—performing complex skills; higher level of behavior Adaptation—changing a motor response when unexpected problems again Basic Learning Principles 1. Willingness or motivation to learn 1. Physical readiness—is patient in pain? Does he mobilize easily? pain impairs concentration 2. Emotional readiness—is the patient in fear, depressed, experiencing anxiety? i. Mild level of anxiety may motivate an individual, a high level prevents learning from occurring 3. Cognitive readiness—what is the patient’s conscious level? Can he think clearly? o A state of readiness Active participation—becomes involved Relevance—knowledge/skills must be relevant Feedback—avoid negative feedback Nonjudgmental support—show acceptance Simple to complex—organize your material so it can be easily comprehended o Not ready patient will ignore you o Cultural Barriers Speak clearly and slowly Empathetic 2. 3. Locate someone familiar with the culture (helps with translation) Ability to learn o Cognitive Development—determine patient’s knowledge base Learning occurs more readily when new information compliments existing knowledge Age may not reflect developmental capabilities o Physical Development—evaluate patient’s physical health before beginning teaching plan To learn psychomotor skills, patient must have necessary strength and coordination Learning environment o Room lighting—makes demonstrating/reading difficult o Quiet setting—privacy o Appropriate furniture o Adequate ventilation o Good ventilation and comfortable temperature o Number of people to teach—make sure everyone can hear/see/is comfortable o Limit teaching to 15-30 minutes Integrating the Nursing & Teaching Process Nursing process—reveals patient’s health needs o While determining the pt’s health needs, may identify some educational needs o When education becomes a part of the care plan, the teaching process begins Teaching process—begins when education becomes a part of the care plan o Pt’s learning needs, willingness/motivation to learn o Be flexible with teaching plan o Repetition facilitates retention 1. Assessment Learning needs—assess level of understanding regarding treatment o Assess past medical experiences o Assess patient’s level of understanding regarding current health status, implications of illness, types of therapies, prognosis Motivation to learn o Behavior—attention span, tendency towards questions, memory o Attitudes toward healthcare providers o Physical and emotional symptoms—pain, anxiety, fear may interfere with pt’s participation in teaching plan o Sociocultural background o Learning style—brochures, videos, discussions, demonstrations o Knowledge base—what does the pt already know? Ability to learn o Physical strength—movement and coordination; extent to which they can perform skills o Reading level—have pt explain instructions he just read o Developmental level Age—older pt’s may be forgetful Teaching/learning environment o Reduce distractions o Comfort—ventilation, temperature, furniture, lighting, etc. o Equipment—necessary equipment available 2. Nursing Diagnosis After assessment, you interpret data & develop a nursing diagnosis that reflects pt’s specific learning need o Ensures that teaching is goal directed Classify ND by the 3 domains to help remain focused on subject/teaching method: o Affective Domain—knowledge deficit related to misunderstanding of prognosis o Cognitive Domain—knowledge deficit related to newly diagnosed or newly prescribed therapy o Psychomotor domain—knowledge deficit related to inexperience with skill 3. Planning After determining ND, learning goals or expectd outcomes are developed. o Learning goals or expected outcomes should be in agreement with the needs perceived by the patient Objectives help to determine expected outcomes Objectives guide the teaching plan Specific, measurable, time oriented Developing objectives o Short term—immediate learning needs Example: understanding upcoming diagnostic test o Long term—assists permanently adapting to health problems o Must: Example: learning to plan a diet with diabetic restrictions State a specific behavior USE VERBS Be observable or measurable Time oriented 4. Implementation Know patient’s needs Select appropriate time limiting length of session Know patient’s ability to comprehend Select appropriate teaching method Involve patient and family members Control the environment—conductive to learning Use repetition, feedback Remain flexible 5. Evaluation Determines what has been learned & what should be reinforced Reveals new learning needs May modify/repeat teaching plan after evaluating Evaluate own teaching strategies with the patient 6. Documentation Specific content: who/what was taught, evaluation of learning, method of teaching