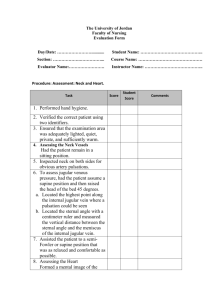
Head to Toe Assessment 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. Introduce self, explain procedure, obtain consent, environment, and ID check. Notice LOC, upright and relaxed, no distress/comfort, no cyanosis or pallor in face. PQRSTU Vital signs a. Normal ranges: BP: 40/50-140/90, HR: 60-100, R: 12-20, T: 36-38, O2%: >95% room air. Oriented to person, place and time (name, location date), alert and aware. Eyes a. Check pupils with pen light; round & symmetrical, constrict to light b. Accommodating & symmetrical movement Anterior Chest a. Inspect: no lumps, bumps or masses, no cyanosis or pallor, skin intact, ribs sloping downward, costal angle less than 90, elliptical shaped thorax. AP ½ of transverse diameter, breathing w/ no accessory muscle, no chest retraction, trachea midline, no dressings, or tubes. b. Palpate: tenderness or pain? No masses, lumps, or bumps, no pulsation. c. Auscultate: Anterior & lateral; good air entry from apex to base of lung bilaterally, no wheezes or crackles. Heart sounds: start at 2nd ICS R of sternal border; aortic valve S2 louder than S1, 2nd ICS L of sternal border; pulmonic valve, S2 louder than S1, Erb’s point; 3rd ICS on sternal border, equal sounds. 4th or 5th ICS L of sternal border; tricuspid valve, S1 louder than S2, 5th ICS on midclavicular line on L; mitral valve, S1 louder then S2, also point of maximum impulse, listen for full minute to obtain pulse and rhythm. Same locations but use bell if any murmurs were heard or place patient on L side. Anterior Abdomen a. Any nausea, vomiting, diarrhea, or pain? Change in diet or appetite? b. Inspect: share, no bules, pulsations, no dressings, no bags, no cyanosis, or pallor c. Auscultate: each quadrant, 5-30 BS, listen for full 5 mins to confirm no sounds, check for bruits by listening to vascular areas (aortic, iliac, renal, and femoral) d. Palpate: light palpation approx. 1 cm, any pain or tenderness? No lumps or masses. Deep palpation 5-8 cm, pain, or tenderness? Locate organs Upper Extremities a. Look symmetrical even muscle tone b. Even muscle strength c. Skin intact, warm, and dry d. No cyanosis or pallor e. Capillary refill, blanches and colour returns in less than 3 seconds f. Radial and bronchial pulses, equal and strong Lower Extremities a. Inspect: even hair distribution, same colour, no cyanosis, or pallor. No dressing and skin intact. b. Palpate: skin warm and dry, no edema, or swelling. Popliteal, posterior tibias and dorsal pedis pulses equal and strong. Capillary refill on toes. Posterior Chest a. Inspect: no lumps, bumps, masses, cyanosis, or pallor. Skin intact, spine straight. b. Palpate: no lumps, bumps, masses, or tenderness. Symmetrical chest expansion. c. Auscultate: z pattern, good air entry from apex to base of lung bilaterally, no crackles, wheeze, or adventitious breath sounds. The Interview Subjective data, informed by patient Objective data, hard facts, lab results, body language Gather complete accurate details, establish rapport and trust, use open and closed questions Health history: biographical data, source of data, reason for seeking care, current and history of health, family history, function assessment and ADL’s Review systems: general overall health state, skin hair and nails, head, eyes, ears, nose and sinus, mouth and throat, neck, breasts, axilla, respiratory, cardiovascular, peripheral vascular, gastrointestinal, urinary, genitals, sex, musculoskeletal, neuro, endocrine, hematological. Pain/Mental Health/ General Survey General Survey: weight and height, vital signs, inspect, palpate, percussion (resonance is lungs, tympany is abdomen, dull is organ, flat is bone, muscle, or tumor), auscultation. Pain: duration; acute or persistent, source; nociceptive (tissue injury) somatic or visceral, neuropathic, or referred, PQRSTU Metal Health: A Appearance, B Behaviour, C Cognition, T Thinking. Assessment; observation, interview, exam, physical assessment, collaboration w/ others. Mental health abnormal findings: LOC; alert, lethargic, obtunded, stupor/semi coma, coma, delirium. Mood and affect; flat/blunted, depression, depersonalization, elation, euphoria, anxiety, fear, irritability, ambivalence, lability, inappropriate affect. Respiratory/ Breast Order of assessment: inspect, palpate, percussion, auscultation Anterior thoracic landmarks: suprasternal notch; u shape depression just above sternus (breastbone). Manubriosternal angle; “angle of Luis” sternal angle. Costal angle less than 90 (where ribs meet) Posterior thoracic Landmarks: vertebra prominesis; bon vertebrae at bottom of neck C7. Inferior border or scapula marks 7th or 8th ICS. 12th rib: palpate between spine and side to identify free tip. Inspection: shape of thorax, AP diameter, symmetry of chest wall, presence of superficial veins, angle of ribs, ICS, muscle of respiration. Rate: Eupnea: 12-20 bpm, Tachypnea: >20 bpm, Bradypnea: <12 bpm, Apnea: no respirations for 10 s. Depth: shallow, hypernea, air trapping, kussmauls (deep rapid breathing), sighing, symmetry, audibility, patient position (upright, supine, or orthopnea) Sputum: “Phlegm”, colour, odor, amount, consistency. Palpation: anterior, posterior, lateral, pulsations, masses, thoracic tenderness, thoracis expansion, crepitus (popping or crackling). Tactile fremitus: “99”, flat palm to feel vibrations. Symmetrical expansion. Percussion: resonance normal, usually on posterior Auscultation: anterior; bronchial- over throat & trachea, bronchovesicular- 2nd & 3rd ICS, vesicular sounds over lungs. Posterior- bronchovesicular C7-T2, vesicular sounds over lungs. Vesicular sounds; 4 ICS- MAL (RUL), 6 ICS AAL (RML), 8 ISC PAL (RLL), 4 ICD MAL (LUL), 6 ICS MAL (LLL). Substance use/Nutrition/Interpersonal Violence Nutritional status: degree of balance between nutrient intake and requirements. Objective data: weight, measure BMI, waist to hip ratio. Interpersonal Violence: including intimate partner, sexual assault, child, and elder abuse Dependence: physiological in nature, normal response to repeated doses, characterized by both tolerance and withdrawal. Skin/Heat, Neck/Peripheral Vascular Inspect: colour, Jugular venous pressure, capillary refill, visible pulsations, even hair distribution, edema, ulcers, skin temp and colour. Palpation- note pulsations, thrills, heaves (should be none). Aortic, pulmonic, erb’s point, tricuspid, mitral Auscultation- first, start at 2nd ICS R of sternal border; aortic valve S2 louder than S1, 2nd ICS L of sternal border; pulmonic valve, S2 louder than S1, Erb’s point; 3rd ICS on sternal border, equal sounds. 4th or 5th ICS L of sternal border; tricuspid valve, S1 louder than S2, 5th ICS on midclavicular line on L; mitral valve, S1 louder then S2, also point of maximum impulse, listen for full minute to obtain pulse and rhythm. Same locations but use bell if any murmurs were heard or place patient on L side. Venous system- pallor, Allen’s test (pressure on artery in wrist, ensure blood flow), arterial assessment. Inspection of JVP and Periphery- position 45 degrees, right side of neck; check internal jugular impulse @ base od sternal notch, is not visualized measure external jugular vein (use 2 ruler method and tangential light to see impulse) maybe indication of tricuspid regurgitation or insufficiency, right side CHF. Assessment of Arterial Pulses: equal, one @ a time, radial, brachial, carotids, aortic, femoral, popliteal, posterior tibial, dorsalis pedis. Characteristics are rate, rhythm, amplitudes, and symmetry. Auscultation: carotids, bilaterally, client hold breath to listen for bruits. Abdomen and Musculoskeletal Organs: RUQ kidney, liver, gallbladder, duodenum, head of pancreas, ascending, and transverse colon. RLQ appendix, cecum, ovary, ureter, spermatic cord. LUQ stomach, spleen, pancreas, liver, kidney, adrenal, splenic flexure of colon. LLQ descending colon, sigmois colon, ovary, ureter, spermatic cord. Midline-> aorta, uterus, and bladder. Landmarks: Spleen behind and parallel to 10th rib on left side, extends from 9th to 11th rib about 7 cm, normally not palpable. 4 layers of muscle form ventral abdomen wall, joined by linea alba, one set (rectus abdominis) forms strip extending length of midline, palpable edged. Solid viscera: those that maintain characteristic shape. Hollow viscera: stomach, gallbladder, small intestine, colon, and bladder. Subjective data: dysphagia, change in appetite, nausea/vomiting, history, prescriptions, alcohol, and drug use. Objective data: contour, symmetry, skin, pulsations, movement, or demeanor. Hepatomegaly; enlarged liver, grater then 7 cm Dullness in front of midaxillary line may indicate splenomegaly. Auscultate bowel sounds & vascular sounds Percussion Palpation- watch for guarding. Rebound should be done @ end as it can be painful. Tenderness of CVA is common sign of pyelonephritis. Genitourinary/Prostate/Pregnancy Subjective data: self-care behaviours, family history, rectal conditions, medications, rectal bleeding, usual bowel routine, change in bowel habits Objective data: proper position, proper tools, and equipment. Head & Neck/Eyes/Ears/Nose, Mouth, and Throat Skull: composed of 8 cranial bones frontal R & L, ethmoid, sphenoid, temporal, occipital, and parietal R/L. Subjective data: headache, injury, dizziness, neck pain, limitation of motion, lumps, swelling, history of head, or neck surgery. Physical Exam: inspect skull, cranial nerves, neck, thyroid gland. Regional Lymphatics 10 locations o Preauricular- front of ear o Postauricular- back of eat o Occipital- base of skull o Submental- under chin o Submandibular- follows jaw line o Jugulodigastric- posterior of mandible o Superficial cervical- under ear o Deep cervical- under sternocleid o Posterior cervical- triangle/ edge or trapez o Surpa clavicular- above clavia Eyes: sensory organ of vision. Internal anatomy- spheric, sclera, choroid, retina, optic disc. Movements comes from 3 CN. Outer layer contain cornea. Middle layer- choroid, dark pigment, pupil, lens. Retinal vessels- have thin sliver of light, macula located temporally, contains fovea centralis. Light rays are refracted though transparent media (cornea, aqueous humor, lens, vitreous bodies) and strike retina. Neurological 2 parts of nervous system. CNS- central nervous system, brain, and spinal cord. Peripheral Nervous system- 12 pairs of cranial nerves, 31 pairs of spinal nerves. Function of the CNS- cerebral cortex (frontal lobe- personality, behaviours, emotions IQ, ability to write words, parietal lobe- sensation, recognize body parts L vs R, temporal lobe- primary auditory reception center, occipital lobe- primary visual centra and understanding of written material). Diencephalon thalamus- main rely station for nervous system and pain threshold. Hypothalamus- center for temp control, sleep, pituitary, and emotional regulations. Cerebellum- blend and coordinate motion of muscles involved in voluntary movement. Brain stemmidbrain contains nerve pathways between hemisphere and medulla, center for visual reflexes, postural reflex. Pons connects medulla oblongata and midbrain, ventral to cerebellum. Medulla Oblongatacontinuation of spinal cord in brain and controls quality of respirations, heart rate, swallowing, hiccups, gag, and cough reflex. Function of PNS- carries message to CNS from sensory receptors and from CNS to muscles and glands. Dermatome is an area of skin supplied with afferent nerves fibers by single posterior spinal root. Spinal nerves are mixed. Reflex Arc response below level of consciousness where sensory afferent fibers carry a message though motor efferent fibers to cause a response in innervated muscle. Autonomic Nervous system- parts of NS that governs the glands, cardiac muscles, smooth muscles (digestion) respiratory, and skin. Sympathetic and parasympathetic. Function is to maintain homeostasis. Types of neuro exams- screening-> well persons, no significant subjective findings. Complete performed when neurological concerns I/D through history. Neuro recheck-> performed after complete exam f/u. Physical Exam- assess mental status, speech, and language. Assess cranial nerve function. Asses for motor function (muscle mass, tone, movement, strength). Assess balance and coordination (finger to finger, heel to shin, arm drift test, rapid alternating movements, Romberg’s Test-balance). Asses sensory function- light touch, superficial pain sensation, temp sensitive, position sense, vibration sense, 2-point discrimination, stereognosis, graphesthesia, extinction, point location. Assess reflexes, 4+= vert brisk, hyperactive, 3+ brisker then normal, 2+ average normal, 1+ diminished, 0- no response. Bicep C5 and C6, triceps C6 and C8, patellar L2 and L4, AchillesL5 and S2, plantar reflex L4 and S2. Glascow Coma Scale- objective assessment that gives numeric value to LOC. Eye opening response; 4spontaneous, 3- to speech, 2- to pain, 1- no response. Motor Response: 6- obeys command, 5-localizes pain, 4flexion/withdrawal, 3-flexion- abnormal (decorticate rigidity), 2- extension- abnormal (decerebrate rigidity), 1no response. Best verbal response: 5- orientated x 3, 4- conversation- confused, 3- speech- inappropriate, 2sounds- incomprehensible, 1- no response. Total score of 7 or less indicates comes, fully alert should be 15.