JOURNAL OF CAFFEINE AND ADENOSINE RESEARCH
Volume 8, Number 4, 2018
ª Mary Ann Liebert, Inc.
DOI: 10.1089/caff.2018.0016
Promises of Caffeine in Attention-Deficit/Hyperactivity
Disorder: From Animal Models to Clinical Practice
Downloaded by SENCKENBERG/ZEITSCHRIFTEN from www.liebertpub.com at 12/02/18. For personal use only.
Angela Patricia França, MS,1,2 Reinaldo N. Takahashi, PhD,2
Rodrigo A. Cunha, PhD,3,4 and Rui Daniel Prediger, PhD1,2
Background: Attention-deficit/hyperactivity disorder (ADHD) is one of the most common chronic
childhood-onset psychiatric disorders. ADHD persists in many cases into adulthood, the occurrence which
is associated with attentional deficits, hyperactivity, and/or cognitive impulsiveness. A primary role of disturbances in frontocortical dopaminergic neurotransmission in ADHD is the basis for the current pharmacological treatment with psychostimulants, mainly methylphenidate. However, there is considerable evidence
that nondopaminergic alterations, including alterations in adenosinergic neuromodulation, also occur in
different brain areas. We now examine findings reported in clinical and animal studies to provide a comprehensive summary of the effects of caffeine, a nonselective adenosine receptor antagonist, in ADHD.
Additionally, we investigate the effects of caffeine and physical exercise on emotional impairments
observed in spontaneously hypertensive rats (SHRs), a validated animal model of ADHD.
Methods: Male SHRs were submitted from adolescence (30 days old) to adulthood to the association of
caffeine intake (0.3 mg/mL in drinking water) plus voluntary physical exercise in running wheels during
6 weeks. After that, depressive- and hedonic-like behaviors were evaluated in the forced swimming test
(FST) and splash test.
Findings: The clinical use of caffeine remains poorly investigated so far and the available results have been
generally positive but somewhat inconsistent, which can be largely attributed to methodological concerns.
In contrast, many studies have shown that caffeine treatment improved memory and attention deficits and
also normalized dopaminergic function in adolescent and adult SHRs. In this study, we provide a comprehensive view of the effects of caffeine in ADHD and in SHRs, and we include new findings from
our research group supporting the potential of caffeine and physical exercise in improving depressivelike behaviors of SHRs.
Conclusion: Altogether, the evidence indicates that caffeine is a promising therapeutic tool to improve cognitive and emotional symptoms in ADHD. Thus, further controlled clinical studies are necessary with a
careful adjustment of the doses of caffeine to adequately exploit this potential.
Keywords: caffeine, attention-deficit/hyperactivity disorder, SHR, review
Introduction
ity. Children with ADHD are often characterized as hyperactive, whereas adults with ADHD are more likely to
experience inner restlessness, an inability to relax, inattention, poor planning, and impulsivity.4,5 ADHD has a
significant impact on psychosocial functioning, and has
been associated with lower level of education, higher
level of unemployment, and higher rates of unsuccessful
marriages, criminality, and road traffic accidents.6,7
A
ttention-deficit/hyperactivity disorder (ADHD)
is one of the most common chronic childhood-onset
psychiatric disorders, with an estimated global prevalence
of 5.9%–7.1% among children/adolescents and 1.2%–
7.3% among adults.1–3 ADHD is characterized by three
main symptoms: hyperactivity, inattention, and impulsiv-
1
Graduate Program of Neuroscience, Center of Biological Sciences, Federal University of Santa Catarina (UFSC), Florianópolis,
Brazil.
2
Department of Pharmacology, Center of Biological Sciences, Federal University of Santa Catarina (UFSC), Florianópolis, Brazil.
3
CNC-Center for Neuroscience of Coimbra, University of Coimbra, Coimbra, Portugal.
4
Faculty of Medicine, University of Coimbra, Coimbra, Portugal.
1
Downloaded by SENCKENBERG/ZEITSCHRIFTEN from www.liebertpub.com at 12/02/18. For personal use only.
2
Regarding the pathophysiology of ADHD, several
brain regions and neural pathways have been implicated.
For instance, functional magnetic resonance imaging
studies in ADHD patients carrying out working memory, inhibitory control, and attentional tasks showed
an underactivation of frontostriatal, frontoparietal, and
ventral attention networks.8,9 Although the etiology of
ADHD is unknown, and without underscoring the importance of environmental and psychosocial factors, a
substantial genetic component has been associated with
ADHD, mostly of genes involved with dopaminergic
transmission.10
The involvement of a dopaminergic dysfunction is further heralded by the fact that stimulant medication used to
treat ADHD symptoms increase synaptic dopamine levels.11 Accordingly, treatment strategies for ADHD include
both pharmacological and psychological therapies aimed
to improve the core symptoms of ADHD and associated
functional impairments. Psychostimulants, including methylphenidate and amphetamine-based treatments, are the
most commonly prescribed pharmacological treatments
for adults and children with ADHD (for review see Ref.12).
However, in recent years, the management of ADHD
has become increasingly complex as new drugs were introduced in clinical practice: nonstimulants (e.g., atomoxetine, guanfacine, and clonidine), antidepressants
(e.g., bupropion, venlafaxine, reboxetine, desipramine,
and imipramine), antipsychotics (e.g., risperidone, aripiprazole, and thioridazine), as well as other unlicensed
drugs (e.g., modafinil and carbamazepine).12 However,
a considerable number of patients are considered nonresponders due to insufficient symptom reduction or inability to tolerate these medications.
About 40 years ago, a series of clinical studies showed
beneficial effects of caffeine to ameliorate ADHD symptoms in children (for review see Refs.13,14). These studies
were largely neglected, probably due to the large availability of psychostimulant medicines manufactured by
pharmaceutical companies in the 1970s. More recently,
there has been a new wave of scientific interest in the potential of caffeine for ADHD treatment, based on studies
in animal models that highlight a robust improvement of
cognitive and emotional impairments.
In this study, we first provide a comprehensive view of
the effects of caffeine in ADHD and in spontaneously hypertensive rats (SHRs), a validated animal model of
ADHD, and we include new findings from our research
group supporting the potential of caffeine in improving
cognitive and emotional symptoms in ADHD.
The clinical use of caffeine in ADHD
There is some evidence that hyperactive children
might ingest more caffeine.15 More recent studies also
demonstrated that ADHD hyperactivity symptoms were
associated with increased frequency of coffee consump-
FRANCxA ET AL.
tion.16 Adolescents with ADHD were twice as likely to
use more caffeine than adolescents without ADHD.17
The longitudinal association between ADHD hyperactive
symptoms and later frequency of coffee consumption
could be a strategy of self-medication aiming to counteract
ADHD symptoms.16 In this context, it is important to emphasize that although caffeine is the most widely consumed psychoactive drug worldwide,18 its consumption
has not been properly controlled in several clinical trials.19
The effects of caffeine on ADHD symptoms were described for the first time in 1973, when Schnackenberg20
reported the potential of caffeine in controlling hyperkinetic behavior: 11 hyperkinetic children whose symptoms were improved after methylphenidate treatment,
but that developed many side effects, were treated with
caffeine.
The conclusion on caffeine benefits was based on the
reports by teachers and parents who were questioned
weekly during 6 weeks, first in the absence of medication
and then during the 3 weeks on coffee intake. In addition,
two cups of coffee per day (estimated 200–300 mg of caffeine daily) improved the overall measure of behavior,
including activity level, attention, impulsiveness, irritability, and explosiveness. All the children presented
lower scores on a hyperkinesia scale after methylphenidate and caffeine treatment, but caffeine did not lead to
any noticeable side effect.20 These pioneer results suggest that caffeine may be a suitable alternative as a substitute for stimulants used in hyperkinetic children.
However, for the past four decades, few clinical studies (Table 1) have further addressed the potential of caffeine for the treatment of ADHD. Harvey and Marsh,21
using a double-blind crossover method, compared the effects of regular coffee (estimated 175–200 mg of caffeine
daily) and decaffeinated coffee on a sample of children
with symptoms of hyperkinetic impulse disorder. They
observed that caffeine in regular coffee improved the children’s performance when compared with placebo or decaffeinated coffee.21 In addition, caffeine treatment at a
lower dose (158.6 mg) was superior in comparison with
placebo and to a higher dose of caffeine to mitigate behavioral impairments in ADHD.22
Another study also described significant improvement
of children with ADHD on impulsivity and general behavior measured by parents/teachers rating scales.23 Furthermore, the association of methylphenidate (10 mg)
plus caffeine (158.6 or 308.6 mg) enhanced the therapeutic effects of caffeine alone for the overall aggressiveness,
inattention, and hyperactivity score.22 Caffeine (300 mg),
both alone or associated with a low dose of amphetamines,
also decreased subjective hyperactive symptoms on the
Conner’s Abbreviated Parent Questionnaire.24 It was observed that the low dose of caffeine plus methylphenidate
was superior to all other treatments in improving total
score and hyperactivity; however, anxiety and sociability
do not seem to respond to caffeine or other stimulants.22
3
Treatment schedule
Main findings
a
Differences in nomenclature and attention-deficit/hyperactivity disorder diagnostic criteria.
Two cups of coffee per day (estimated 200–3000 mg of
Caffeine improved behavioral impairments without marked side
caffeine) during 3 weeks
effects
7 boys and 1 girl (6–11 years old) Caffeine (3 mg/kg) for the first week in a single dose, 3 mg/kg Clinical benefits of caffeine were not distinguishable from those of
with hyperactivity
(morning and afternoon) for the second week, and 6 mg/kg
placebo
for the third week
18 children (12 boys and 6 girls, Caffeine (at least 300 mg), d-amphetamine (mean: 20 mg) and Methylphenidate and d-amphetamine presented superior effects in
mean age = 8.5 years)
methylphenidate (mean: 40 mg) daily, for at least 1 week
comparison with caffeine.Caffeine effects did not differ from
placebo.Absence of marked side effects after caffeine
administration.
25 children (5–13 years)
Placebo, caffeine (50–200 mg), methylphenidate (2.5–10 mg), Caffeine (mean: 249 mg/day) had no beneficial effect.Mothers and
diagnosed as hyperkinetic
d-amphetamine (1.5–5 mg), all twice daily, and imipramine
teachers reported worsening symptoms after caffeine treatment.The
(10–25 mg) in one bedtime dose
subjects exhibited benefits after methylphenidate, d-amphetamine,
and imipramine treatment.
8 boys (6–10 years) diagnosed as Placebo (200 mg), caffeine (160 mg), or methylphenidate
Methylphenidate presented superior effects in comparison with
minimal brain dysfunction
(20 mg) once a day during 2 weeks
caffeine
8 boys (6–10 years) with minimal Placebo (100 mg), caffeine (75 mg), or methylphenidate
Methylphenidate presented superior effects in comparison with
brain dysfunction
(10 mg) twice daily during 2 weeks
caffeine on the impulsivity and hyperactivity control
5 boys and 1 girl (mean age 9.3),
Caffeine (6 mg/kg) or placebo was administered 30 min
Similar plasma caffeine levels in the hyperkinetic (163.3 mg) and
before test
control (168.3 mg) groups.Caffeine improved the attention deficits,
under treatment for hyperkinesis,
the accuracy of stimulus identification, and processing in the
but were off of the drug
hyperkinetic group.
10 boys (9–11 years) with
Caffeine (300 mg) 1 hour before test
Hyperactive children tended to make fewer omissions under caffeine
reading-disabled
treatment than under placebo.Caffeine did not improve attentional
deficits.
12 children (8 boys, 4 girls, mean Whole coffee and de-caffeinated coffee was dispensed twice Caffeine presented superior effects in comparison with placebo or
daily, during 3 weeks (estimated 175–200 mg of caffeine
decaffeinated coffee
age 7.26 years) with
daily)
hyperkinetic symptoms and
impulse disorder
20 hyperactive boys (5–12 years) Caffeine (150 mg) twice daily during 2 weeks
Caffeine improved impulsivity as measured by reaction time, as well
as general behavior measured by parents/teachers
21 hyperactive children (17 boys Placebo, caffeine (300 and 500 mg), or methylphenidate
Methylphenidate improved impulsivity and motor control.Caffeine
and 4 girls) aged 6–12 years.
(20 mg) daily during 3 weeks
did not present superior effects in comparison with placebo.
29 children (22 boys and 7 girls) One to six capsules of caffeine (80 mg), methylphenidate
Methylphenidate and d-amphetamine presented superior effects in
aged between 5 to 12 years
(10 mg), or d-amphetamine (5 mg) during 3 weeks
comparison with caffeine
17 hyperkinetic children
Acute treatment with placebo or caffeine (3 or 6 mg/kg)
The behavioral measures tended to be improved in a dose-related
(8–11 years) previously
manner but without statistical significance
treated with stimulants
6 boys (6–10 years) with
Placebo and caffeine (158.6 or 308.6 mg) during 15 days.
The lower caffeine dose presented superior effects in comparison with
hyperactivity, attentional
Methylphenidate (10 mg) was administered in combination
placebo and to the higher caffeine dose.The association of
deficit, and impulsivity
with caffeine during the past 5 days.
methylphenidate enhanced the beneficial effects of the two caffeine
doses.
15 boys (6–10 years) with
Amphetamine (1.6 or 5 mg) and caffeine (300 mg) administered Caffeine improved hyperactive symptoms but induced a number of
hyperactivity
alone or in combination with amphetamine (1.6 mg) twice a
side effects, including insomnia
day during 2 weeks
11 hyperkinetic children
Subjects and diagnosisa
Table 1. Summary of Clinical Studies Addressing the Effects of Caffeine in Attention-Deficit/Hyperactivity Disorder Patients
Downloaded by SENCKENBERG/ZEITSCHRIFTEN from www.liebertpub.com at 12/02/18. For personal use only.
24
22
29
28
33
23
21
32
31
26
25
34
27
30
20
Reference
Downloaded by SENCKENBERG/ZEITSCHRIFTEN from www.liebertpub.com at 12/02/18. For personal use only.
4
It is important to mention that not all studies reported unequivocal benefits upon caffeine administration to ADHD
children. Garfinkel et al.25,26 showed that caffeine intake
for a short period of time (10 days) induced beneficial effects in children diagnosed with minimal brain dysfunction
(Table 1), although the response to methylphenidate was
superior to that of caffeine in attenuating hyperactive, impulsivity, and aggressive behavior. Huestis et al.,27 using
the same caffeine dose (200–300 mg/day) previously
used by Schnackenberg,20 observed a slight improvement
that did not differ significantly from placebo and was significantly inferior in comparison with methylphenidate or
d-amphetamine.27 A posterior double-blind crossover
comparison of methylphenidate, d-amphetamine, placebo,
and caffeine corroborated these findings.28
The acute effects of caffeine (from 75 to 180 mg) were
investigated in a double-blind study on measures of visual evoked response, alpha-time, vigilance, and activity
level in hyperkinetic children. Children (8–11 years) previously treated with stimulants were withdrawn from
their medications for at least 1 week before starting caffeine treatment. Acute caffeine treatment caused a
marked central effect (on cortical evoked potentials response), but only marginal behavioral improvements
were observed on attention and activity level tasks.29
Some studies reported that individuals with ADHD respond differently to specific pharmacological treatments.21,28 For instance, in a sample of 26 subjects, 12
responded better to d-amphetamine, 10 to methylphenidate, and 1 to caffeine.28 Thus, despite the limited number of subjects in these studies, the available data indicate
that some children are more responsive to the effects
of caffeine or other psychostimulants.30 In a sample
of six hyperactive children, caffeine increased the accuracy of stimulus identification and processing and
improved attentional deficits.31 In contrast, in another
study with 10 boys with reading disability, caffeine
failed to improve attentional deficits, but hyperactive
children tended to make fewer omissions under caffeine
treatment.32
There is no consensus in the literature about the optimal caffeine dose to elicit benefits on ADHD symptoms.
Some researchers reported that low caffeine doses are
more effective in attenuating the behavioral impairments
in ADHD, contrasting with the earliest description by
Schnackenberg20 proposing that the benefits of caffeine
were observed in doses >200 mg daily. For instance, Garfinkel et al.22 reported that the treatment during 15 days
with the lower caffeine dose (158.6 mg daily) presented
superior effects in comparison with placebo and to a
higher caffeine dose (308.6 mg daily).
In contrast, Schechter and Timmons24 observed that a
high caffeine dose (600 mg daily) improved the vigilance
performance in hyperactive children. However, high caffeine doses (300 or 500 mg daily) during 3 weeks failed to
FRANCxA ET AL.
relieve the hyperactivity, inattention, impulsivity, inability
to delay gratification, and opposition behavior in more severely impaired children.33 Another study reported that
caffeine, at an average dose of 249 mg per day, alleviated
ADHD symptoms as judged by their mothers and teachers.
In this study, the caffeine dose ranged from 100 to 400 mg
daily during 1 week and the behavior was measured
weekly.34
Although many studies report that caffeine administration is well tolerated by the children and is devoid of
marked side effects,20,27 this inconsistency and lack of
agreement on the ‘‘optimal’’ dose of caffeine probably result from the general inability to monitor the polymorphisms of A2A receptors that seem to format the intake
of coffee and caffeine.35,36
In this respect, it is interesting to note that the exploitation of the Child and Adolescent Twin Study in Sweden
suggested a nominal association between ADHD traits and
three gene single nucleotide polymorphisms (rs3761422,
rs5751876, and rs35320474) of ADORA2A adenosine
A2A receptor gene.37 Although A2A receptor antagonists
are safe drugs already tested in >3000 volunteers and patients, their safety and tolerability will have to be
assessed in children before considering testing their therapeutic potential in ADHD children.
Effects of caffeine on cognitive and emotional
impairments in animal models of ADHD
Although the clinical use of caffeine in ADHD remains poorly explored (Table 1), the effects of caffeine
have been investigated in different animal models of
ADHD38–41 (Table 2). Given that the only established
molecular mechanism of action of caffeine at nontoxic
doses is the antagonism of adenosine receptors,18 some
studies also explored the effects of selective adenosine receptor antagonists, mainly focusing on antagonists of adenosine A2A receptors that exhibit robust neuroprotective
actions42 and prevent memory and emotional dysfunction
in a variety of animal models of brain disorders.42–45
In adult SHRs, previous studies showed that an acute
treatment with caffeine (3 and 10 mg/kg, i.p.) was able
to reverse the social memory impairment and spatial
learning deficit exhibited by adult SHRs.41,46 An improvement in short-term social memory was also
achieved after an acute administration of the selective
adenosine A2A receptor antagonist ZM241385 (0.5 and
1 mg/kg, i.p.). Interestingly, the acute administration of
the selective adenosine A1 receptor antagonist DPCPX
(1 and 3 mg/kg, i.p.) did not improve the SHR performance on this task. This suggests a selective involvement
of adenosine A2A receptors on social memory in SHRs.46
In contrast, the blockade of both A1 and A2A receptors
improved discriminative learning impairments of SHRs
in the object recognition task.40 This involvement of
adenosine A1 and mainly A2A receptors in the beneficial
5
Caffeine in the drinking water (0.3 g/L) during childhood
(PN15–28) and childhood to adolescence (PN15–54)
Childhood (PN15–28) and
adolescent (PN15–54) male
and female SHRs
SHRs were hyperactive and had poorer performance in the
attentional set-shifting and Y-maze paradigms and also
displayed increased dopamine transporter (DAT) density
and increased dopamine uptake in frontocortical and
striatal terminals compared with WKY rats.Caffeine
improved behavioral impairments and normalized
dopaminergic function in SHRs.
The animals socially isolated for 1 week or more exhibited
spatial attention deficit in the water-finding test and
impaired contextual and conditional fear memory in the
fear-conditioning test.Caffeine and methylphenidate
improved SI-induced latent learning deficits.
PN15–28: caffeine improved spatial working memory
impairments of female SHRs in the Y-maze test.PN15–
55: caffeine increased locomotor activity of female SHRs
and improved the short-term memory of male and female
SHRs in the object recognition task.SHRs from both
sexes presented increases in the BDNF, truncated and
phospho-TrkB receptors, and also phospho-CREB levels
in the hippocampus. Caffeine normalized BDNF in males
and truncated TrkB receptor in both sexes.
Caffeine and methylphenidate improved the objectrecognition deficits of adult SHRs
Caffeine intake improved the attention deficits of 6-OHDAlesioned rats
All tested drugs (caffeine, methylphenidate, and the
selective adenosine receptor antagonists) improved shortterm object-recognition ability of SHRs
46
Caffeine and the selective adenosine A2A receptor antagonist
ZM241385, but not the selective adenosine A1 receptor
antagonist DPCPX, improved short-term social
recognition memory deficits of SHRs
Pretraining administration of caffeine improved spatial
learning deficit of SHRs
52
38
51
39
50
40
41
Reference
Main findings
6-OHDA, 6-hydroxydopamine; BDNF, brain-derived neurotrophic factor; DPCPX, 8-cyclopentyl-1,3-dipropylxanthine; ICR, Institute of Cancer Research; PN, postnatal; SHRs, spontaneously
hypertensive rats; SI, social isolation; TrkB, tropomyosin kinase receptor kinase B; ZM241385, 4-(2-[7-amino-2-{2-furyl}{1,2,4}triazolo-{2,3-a}{1,3,5}triazin-5-yl-amino]ethyl) phenol.
Acute i.p. administration of caffeine (0.5–1 mg/kg) or
methylphenidate (1–10 mg/kg) 30 min before the
behavioral tasks (water-finding, fear-conditioning, Ymaze and object recognition)
Chronic i.p. administration of caffeine (2 mg/kg) twice a day
during 21 days
Acute i.p. administration of caffeine (3–10 mg/kg),
ZM241385 (0.5–1 mg/kg), or DPCPX (1–3 mg/kg) 30 min
before the first presentation of the juvenile rat in the
social recognition task
Acute i.p. administration of caffeine (1–10 mg/kg) 30 min
before training, immediately after training, or 30 min
before the test session of the spatial version of Morris
water maze
Acute i.p. administration of caffeine (1–10 mg/kg),
methylphenidate (2 mg/kg), DPCPX (1–5 mg/kg),
ZM241385 (0.1– 1mg/kg), or the association of
DPCPX+ZM241385 (3 + 0.5 mg/kg) 30 min before the
first trial of the object recognition task
Chronic i.p. administration of caffeine (3 mg/kg) or
methylphenidate (2 mg/kg) during 14 days
Caffeine in the drinking water (1 mg/ml) for 2 weeks
(PN25–38)
Treatment schedule
Adolescent male ICR mice
(30 days old) under SI
Adolescent female SHRs
(25 days old)
Sprague–Dawley neonatal
6-OHDA-lesioned rat at
PN7
Adolescent male SHRs
(24 days old)
Adult male and female SHRs
(3 months old)
Adult female SHRs (3 months
old)
Adult male SHRs (3 months
old)
Animals
Table 2. Summary of the Effects of Caffeine in Nonclinical Studies Using Animal Models of Attention-Deficit/Hyperactivity Disorder
Downloaded by SENCKENBERG/ZEITSCHRIFTEN from www.liebertpub.com at 12/02/18. For personal use only.
Downloaded by SENCKENBERG/ZEITSCHRIFTEN from www.liebertpub.com at 12/02/18. For personal use only.
6
effects of caffeine is probably associated with the ability of these receptors to control synaptic plasticity processes in the prefrontal cortex47 and hippocampus.48,49
Acute treatment with caffeine also improved, in a
dose-dependent manner, learning deficits in a socialisolation-induced model of ADHD.38
Of high interest, chronic caffeine treatment seems to
provide long-term cognitive benefits in SHRs. Chronic
caffeine administration during adolescence was able to
improve short-term recognition ability in adult SHRs,50
improve memory and attention deficits,39,51 and also normalize dopaminergic function by reducing dopamine
reuptake in the striatum and frontal cortex of SHRs.51
More recently, Nunes et al.52 studied the effects of free
caffeine intake (0.3 g/L) from childhood to adolescence
in behavior and in brain-derived neurotrophic factor
(BDNF) signaling pathway in male and female SHRs.
The authors observed hyperlocomotion, recognition,
and spatial memory disturbances in adolescent SHRs
from both sexes. However, females showed a lack of habituation and worsened spatial memory.
Caffeine intake hampered recognition memory impairments in both sexes; however, spatial memory was recovered only in female SHRs. Female SHRs displayed
exacerbated hyperlocomotion after caffeine treatment.
SHRs from both sexes presented increase in the levels
of BDNF, truncated and phospho-TrkB receptors and
also phospho-CREB in the hippocampus. Caffeine normalized BDNF in males and truncated TrkB receptor in
both sexes.52 These findings reinforce and extend the previous data obtained in male SHRs, showing the potential
of caffeine for the treatment of cognitive impairments in
ADHD, regardless of gender.
FRANCxA ET AL.
The effects of caffeine have been also investigated in
the emotional alterations observed in ADHD models.
According to epidemiological and clinical studies, the
majority of patients with ADHD present multiple psychiatric and nonpsychiatric comorbid disorders.53–55
Overall, ADHD-afflicted males display an increased
risk of neuropsychiatric disorders, whereas females appear to have associated more frequently with internalizing disorders.55 Among the most frequently observed
comorbidities are anxiety and affective disorders, such
as depression,56,57 resulting in a serious impairment
of daily life with several functional and psychosocial
problems.56
In addition to the pharmacological strategy, lifestyle
changes, such as physical exercise practice, have been
researched due to their effects on improving brain health.
Physical exercise can exert protective effects against cognitive decline,58,59 increase cognitive performance,60 and
also improve emotional impairment, as depression, anxiety, stress responsivity, and mood state.61 Recently, a
meta-analysis has shown that, in addition to significantly
improving depressive symptoms in patients with cognitive
impairment, physical exercise ameliorates neuropsychiatric symptoms, quality of life, and activities of daily
living.62
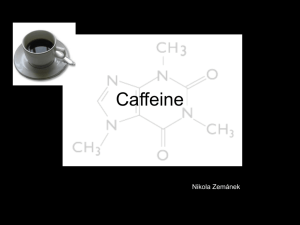
Therefore, we investigated the effects of chronic caffeine intake and physical exercise on the emotional impairments observed in SHRs. Male SHRs were submitted from
adolescence (30 days old) to adulthood to the association
of caffeine intake (0.3 mg/mL in drinking water) plus voluntary physical exercise in running wheels during 6 weeks.
After that, depressive- and hedonic-like behaviors were
evaluated in the forced swimming test (FST) and splash
FIG. 1. Schematic representation of the experimental design. Caffeine intake (3 mg/mL in drinking water) associated
with voluntary physical exercise was applied from adolescence (1 month old) to adulthood during 6 weeks and after
that the behavioral analysis was performed. SHRs, spontaneously hypertensive rats.
EFFECTS OF CAFFEINE IN ADHD
Downloaded by SENCKENBERG/ZEITSCHRIFTEN from www.liebertpub.com at 12/02/18. For personal use only.
test. The schematic representation of the experimental design is detailed in Figure 1.
The FST is widely used for the identification of pharmacological and nonpharmacological agents with potential antidepressant actions, as indicated by a significant
reduction of the immobility time of rodents during this
test.63 The animal is considered immobile when it is
only floating or performing the minimum of movements
necessary to keep its head out of the water.64 In addi-
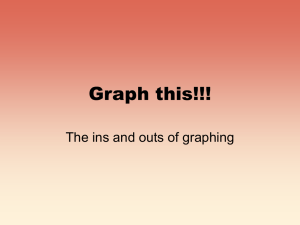
FIG. 2. Effects of chronic caffeine intake (0.3 mg/mL in
the drinking water) and voluntary physical exercise (running
wheels) from adolescence to adulthood on depressive-like
behavior of male SHRs evaluated in the FST. The bars represent (A) the immobility time (seconds), (B) swimming time
(seconds), and (C) climbing time (seconds) of SHRs in the
FST. Data are expressed as means – SEM (n = 10 animals
per group). *p < 0.05 compared with SHR control group (vehicle treated). Two-way ANOVA followed by Dunnett’s
post hoc test. ANOVA, analysis of variance; FST, forced
swimming test; SEM, standard error of the mean.
7
tion, the duration of swimming time and climbing
time were recorded during a 5-minute test session, as
described previously.64
Two-way analysis of variance (ANOVA) (caffeine intake vs. physical exercise) revealed a significant effect of
caffeine intake [F(1,36) = 27.785; p < 0.05] and of physical
exercise [F(1,36) = 53.703; p < 0.05], but not of their interaction [F(1,36) = 2.2498; p = 0.142] on immobility time in
the FST. Dunnett’s post hoc comparisons revealed a significant reduction in the immobility time in male SHRs
from the caffeine, exercise, and caffeine plus exercise
groups in comparison with the control group (vehicle treated), indicative of an antidepressant effect (Fig. 2A).
Chronic caffeine intake [F(1,36) = 19.723; p < 0.05] and
physical exercise [F(1,36) = 27.663, p < 0.05], but not their
interaction [F(1,36) = 3.0331; p = 0.090], also present significant effects on swimming time: when compared with
the control group (vehicle treated), caffeine, exercise,
and caffeine plus exercise groups showed an increase in
the swimming time (Fig. 2B). Moreover, there was a significant main effect of physical exercise [F(1,36) = 33.787;
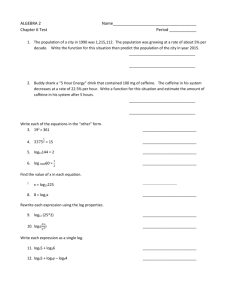
FIG. 3. Effects of chronic caffeine intake (0.3 mg/mL
in the drinking water) and voluntary physical exercise
(running wheels) from adolescence to adulthood on
hedonic-like behaviors of male SHRs evaluated in the
splash test. The bars represent (A) the latency (seconds)
for the first grooming behavior and (B) total grooming
time (seconds) of SHRs in the splash test. Data are
expressed as means – SEM (n = 10 animals per group).
Two-way ANOVA. There were no significant differences.
FRANCxA ET AL.
Downloaded by SENCKENBERG/ZEITSCHRIFTEN from www.liebertpub.com at 12/02/18. For personal use only.
8
p < 0.05] in the climbing time. A subsequent Dunnett’s
post hoc test indicated that caffeine plus exercise group increased significantly the climbing time of SHRs (Fig. 2C).
In addition, the splash test was carried out to evaluate
hedonic- and self-care behavior, after spraying a 10% sucrose solution on the dorsal coat of rat, as previously described.65 As the sucrose solution is viscous, the hair of
the animal becomes sticky and wet and it initiates the
grooming behavior.66 The evaluation of grooming behavior (an index of self-care phenotype) included nose/
face grooming, head washing (semicircular movements
over the head and behind the ears), body grooming (fur
licking and scratching the body with the hind paws),
leg/paw licking and tail/genitals cleaning.67
Deficits in the hedonic response to rewards (‘‘consummatory anhedonia’’) and a decreased motivation to
pursue them (‘‘motivational anhedonia’’) have been described as anhedonic symptom.68 In animal models, distinct conditions seem to lead to anhedonic-like behavior,
such as environmental stress69 and exposure to toxins.66,70 Two-way ANOVA (caffeine intake vs. physical
exercise) revealed that there were no significant effects
of caffeine intake and/or physical exercise in the latency
to grooming (Fig. 3A) and total grooming time (Fig. 3B)
in the splash test.
These results indicate that, in a significant and independent way, chronic caffeine intake and physical exercise
exhibit antidepressant-like effects in SHRs, without alterations on hedonic-like behaviors. These findings provide
the first evidence of beneficial effects of chronic caffeine
intake and physical exercise on emotional impairments
observed in an animal model of ADHD. Since the effects
of caffeine on mood have been shown to be mediated by
adenosine A2A receptors,71 which interact with dopamine
transporters and dopamine D2 receptors,72 namely, in the
prefrontal cortex51,73 to control effort-based decisionmaking,74 working memory, and reversal learning,75 it is
expected that future work should explore the ability of selective A2A receptor antagonists to control emotional alterations in ADHD models.
Moreover, physical exercise is a nonpharmacological
approach that confers long-term benefits and directly
implies the quality of life and brain health. Exercise
plays an important role in the molecular events related
to the management of energy metabolism and synaptic
plasticity,76 and its beneficial effects on brain plasticity
continue to develop even after the end of exercise.60
Therefore, the independent effects promoted by physical
exercise in improving the emotional alterations in SHRs,
encourage new studies to investigate their role in ADHD
symptoms.
Conclusion
The preclinical results reviewed in this study provide convergent evidence that different schedules of caffeine administration (acute vs. chronic, route, doses, etc.)
improved cognitive and emotional impairments and
also normalized dopaminergic function in adolescent
and adult SHRs (Table 2; Fig. 2). In contrast, the results
from previous clinical studies on the efficacy of caffeine
have been inconsistent, with some authors demonstrating an improvement of ADHD symptoms, whereas others have not found convincing positive caffeine effects
(Table 1). For this reason, the general view in the field is
that adjunctive caffeine is not contraindicated for the
treatment of ADHD, but it might not be a viable replacement for the first-line treatment for ADHD such
as methylphenidate.
In a meta-analysis study, Leon77 reported that the
small number of studies, the small sample size (14.4 subjects/study), and the great variation in caffeine doses are
the main limiting factors and should be considered with
caution. Since the effects of caffeine in ADHD and in
SHRs appear to be mediated by adenosine A2A receptors,
this review points to the need to investigate clinically and
preclinically a therapeutic role of available A2A receptor
antagonists. In addition, physical exercise is a simple intervention that promotes known benefits in cognition and
emotional state, which could contribute to the therapeutic
approach in ADHD symptoms. Therefore, additional
controlled clinical studies with a careful adjustment of
the dose of caffeine to the particular A2A receptor polymorphism of each subject are necessary to better address
the effects of caffeine in ADHD therapy.
Acknowledgments
Some of the research reviewed in this article was supported by the Conselho Nacional de Desenvolvimento
Cientı́fico e Tecnológico (CNPq, Universal 408676/
2016-7), Coordenação de Aperfeiçoamento de Pessoal
de Nı́vel Superior (CAPES-FCT), Programa de Apoio
aos Núcleos de Excelência (PRONEX—Project NENASC),
Fundação de Apoio à Pesquisa do Estado de Santa
Catarina (FAPESC), LaCaixa, Centro 2020 (projects
CENTRO-01-0145-FEDER-000008:BrainHealth 2020 and
CENTRO-01-0246-FEDER-000010), and through FCT
(POCI-01-0145-FEDER-031274). A.P.F. received scholarships from CAPES. R.D.P. is supported by research fellowship from CNPq and is a scientific consultant of
Brazilian Coffee Industry Association.
Author Disclosure Statement
The authors have no financial or personal conflicts of
interest related to this work.
References
1. Faraone SV, Antshel KM. Diagnosing and treating
attention-deficit/hyperactivity disorder in adults. World
Psychiatry. 2008;7:131–136.
2. Polanczyk GV, Willcutt EG, Salum GA, Kieling C,
Rohde LA. ADHD prevalence estimates across three
EFFECTS OF CAFFEINE IN ADHD
3.
4.
Downloaded by SENCKENBERG/ZEITSCHRIFTEN from www.liebertpub.com at 12/02/18. For personal use only.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
decades: An updated systematic review and metaregression analysis. Int J Epidemiol. 2014;43:434–442.
Moffitt TE, Houts R, Asherson P, et al. Is adult ADHD a
childhood-onset neurodevelopmental disorder? Evidence
from a four-decade longitudinal cohort study. Am J Psychiatry. 2015;172:967–977.
European Medicines Agency. Guideline on the clinical
investigation of medicinal products for the treatment
of attention deficit hyperactivity disorder (ADHD).
2008. Available at: http://www.ema europa.eu/docs/
en_GB/document_library/Scientific_guideline/2010/08/
WC500095686.pdf. Accessed August 2018.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed., DSM-5.
2012. Available at: http://www.dsm5.org. Accessed
August 2018.
Biederman J, Faraone SV, Spencer TJ, Mick E, Monuteaux MC, Aleardi M. Functional impairments in adults
with self-reports of diagnosed ADHD: A controlled
study of 1001 adults in the community. J Clin Psychiatry.
2006;67:524–540.
Goodman DW. The consequences of attention-deficit/
hyperactivity disorder in adults. J Psychiatr Pract. 2007;
13:318–327.
Cortese S, Kelly C, Chabernaud C, et al. Toward systems
neuroscience of ADHD: A meta-analysis of 55 fMRI
studies. Am J Psychiatry. 2012;169:1038–1055.
Thapar A, Cooper M. Attention deficit hyperactivity disorder. Lancet. 2016;387:1240–1250.
Faraone SV, Perlis RH, Doyle AE, et al. Molecular genetics of attention-deficit/hyperactivity disorder. Biol
Psychiatry. 2005;57:1313–1323.
Swanson JM, Kinsbourne M, Nigg J, et al. Etiologic
subtypes of attention-deficit/hyperactivity disorder:
Brain imaging, molecular genetic and environmental
factors and the dopamine hypothesis. Neuropsychol
Rev. 2007;17:39–59.
Catala-Lopez F, Hutton B, Nunez-Beltran A, et al. The
pharmacological and non-pharmacological treatment of
attention deficit hyperactivity disorder in children and
adolescents: A systematic review with network metaanalyses of randomised trials. PLoS One. 2017;12:
e0180355.
Ioannidis K, Chamberlain SR, Muller U. Ostracising caffeine from the pharmacological arsenal for attentiondeficit hyperactivity disorder—was this a correct decision? A literature review. J Psychopharmacol. 2014;28:
830–836.
Takahashi RN, Pamplona FA, Prediger RD. Adenosine
receptor antagonists for cognitive dysfunction: A review of animal studies. Front Biosci. 2008;13:2614–
2632.
Rapoport JL. Diet and hyperactivity. Nutr Rev. 1986;
44(Suppl):158–162.
Marmorstein NR. Energy drink and coffee consumption
and psychopathology symptoms among early adolescents: Cross-sectional and longitudinal associations. J
Caffeine Res. 2016;6:64–72.
Walker LR, Abraham AA, Tercyak KP. Adolescent caffeine use, ADHD, and cigarette smoking. Childrens
Health Care. 2010;39:73–90.
Fredholm BB, Battig K, Holmen J, Nehlig A, Zvartau
EE. Actions of caffeine in the brain with special refer-
9
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
ence to factors that contribute to its widespread use.
Pharmacol Rev. 1999;51:83–133.
Chen JF, Eltzschig HK, Fredholm BB. Adenosine receptors as drug targets—What are the challenges? Nat Rev
Drug Discov. 2013;12:265–286.
Schnackenberg RC. Caffeine as a substitute for Schedule
II stimulants in hyperkinetic children. Am J Psychiatry.
1973;130:796–798.
Harvey DH, Marsh RW. The effects of de-caffeinated
coffee versus whole coffee on hyperactive children.
Dev Med Child Neurol. 1978;20:81–86.
Garfinkel BD, Webster CD, Sloman L. Responses to
methylphenidate and varied doses of caffeine in children
with attention deficit disorder. Can J Psychiatry. 1981;
26:395–401.
Firestone P, Poitras-Wright H, Douglas V. The effects of
caffeine on hyperactive children. J Learn Disabil. 1978;
11:133–141.
Schechter MD, Timmons GD. Objectively measured hyperactivity—II. Caffeine and amphetamine effects. J
Clin Pharmacol. 1985;25:276–280.
Garfinkel BD, Webster CD, Sloman L. Individual responses to methylphenidate and caffeine in children
with minimal brain dysfunction. Can Med Assoc J.
1975;113:729–732.
Garfinkel BD, Webster CD, Sloman L. Methylphenidate and caffeine in the treatment of children with minimal brain dysfunction. Am J Psychiatry. 1975;132:
723–728.
Huestis RD, Arnold LE, Smeltzer DJ. Caffeine versus
methylphenidate and d-amphetamine in minimal brain
dysfunction: A double-blind comparison. Am J Psychiatry. 1975;132:868–870.
Arnold LE, Christopher J, Huestis R, Smeltzer DJ.
Methylphenidate vs dextroamphetamine vs caffeine in
minimal brain dysfunction: Controlled comparison by
placebo washout design with Bayes’ analysis. Arch
Gen Psychiatry. 1978;35:463–473.
Conners CK. The acute effects of caffeine on evoked response, vigilance, and activity level in hyperkinetic children. J Abnorm Child Psychol. 1979;7:145–151.
Conners CK. A Placebo-crossover study of caffeine
treatment of hyperkinetic children. Int J Ment Health.
1975;4:132–143.
Reichard CC, Elder ST. The effects of caffeine on reaction time in hyperkinetic and normal children. Am J Psychiatry. 1977;134:144–148.
Kupietz SS, Winsberg BG. Caffeine and inattentiveness
in reading-disabled children. Percept Mot Skills. 1977;
44(3 Pt 2):1238.
Firestone P, Davey J, Goodman JT, Peters S. The effects
of caffeine and methylphenidate on hyperactive children.
J Am Acad Child Psychiatry. 1978;17:445–456.
Gross MD. Caffeine in the treatment of children with
minimal brain dysfunction or hyperkinetic syndrome.
Psychosomatics. 1975;16:26–27.
Cornelis MC, El-Sohemy A, Campos H. Genetic polymorphism of the adenosine A2A receptor is associated
with habitual caffeine consumption. Am J Clin Nutr.
2007;86:240–244.
Cornelis MC, Kacprowski T, Menni C, et al. Genomewide association study of caffeine metabolites provides new insights to caffeine metabolism and dietary
FRANCxA ET AL.
10
37.
38.
39.
Downloaded by SENCKENBERG/ZEITSCHRIFTEN from www.liebertpub.com at 12/02/18. For personal use only.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
caffeine-consumption behavior. Hum Mol Genet.
2016;25:5472–5482.
Molero Y, Gumpert C, Serlachius E, et al. A study of
the possible association between adenosine A2A receptor gene polymorphisms and attention-deficit hyperactivity disorder traits. Genes Brain Behav. 2013;12:
305–310.
Ouchi H, Ono K, Murakami Y, Matsumoto K. Social isolation induces deficit of latent learning performance in
mice: A putative animal model of attention deficit/hyperactivity disorder. Behav Brain Res. 2013;238:146–153.
Caballero M, Nunez F, Ahern S, et al. Caffeine improves
attention deficit in neonatal 6-OHDA lesioned rats, an
animal model of attention deficit hyperactivity disorder
(ADHD). Neurosci Lett. 2011;494:44–48.
Pires VA, Pamplona FA, Pandolfo P, Fernandes D, Prediger RD, Takahashi RN. Adenosine receptor antagonists improve short-term object-recognition ability of
spontaneously hypertensive rats: A rodent model of
attention-deficit hyperactivity disorder. Behav Pharmacol. 2009;20:134–145.
Prediger RD, Pamplona FA, Fernandes D, Takahashi
RN. Caffeine improves spatial learning deficits in an animal model of attention deficit hyperactivity disorder
(ADHD)—The spontaneously hypertensive rat (SHR).
Int J Neuropsychopharmacol. 2005;8:583–594.
Cunha RA. How does adenosine control neuronal dysfunction and neurodegeneration? J Neurochem. 2016;
139:1019–1055.
Cunha RA, Ferre S, Vaugeois JM, Chen JF. Potential
therapeutic interest of adenosine A2A receptors in psychiatric disorders. Curr Pharm Des. 2008;14:1512–1524.
Cunha RA, Agostinho PM. Chronic caffeine consumption prevents memory disturbance in different animal
models of memory decline. J Alzheimers Dis. 2010;
20(Suppl 1):S95–S116.
Chen JF. Adenosine receptor control of cognition in normal and disease. Int Rev Neurobiol. 2014;119:257–307.
Prediger RD, Fernandes D, Takahashi RN. Blockade of
adenosine A2A receptors reverses short-term social memory impairments in spontaneously hypertensive rats.
Behav Brain Res. 2005;159:197–205.
Kerkhofs A, Canas PM, Timmerman AJ, et al. Adenosine A2A receptors control glutamatergic synaptic plasticity in fast spiking interneurons of the prefrontal
cortex. Front Pharmacol. 2018;9:133.
Rebola N, Lujan R, Cunha RA, Mulle C. Adenosine A2A
receptors are essential for long-term potentiation of
NMDA-EPSCs at hippocampal mossy fiber synapses.
Neuron. 2008;57:121–134.
Temido-Ferreira M, Ferreira DG, Batalha VL, et al. Agerelated shift in LTD is dependent on neuronal adenosine
A2A receptors interplay with mGluR5 and NMDA receptors. Mol Psychiatry. 2018 [Epub ahead of print]; DOI:
10.1038/s41380-018-0110-9.
Pires VA, Pamplona FA, Pandolfo P, Prediger RD,
Takahashi RN. Chronic caffeine treatment during prepubertal period confers long-term cognitive benefits in
adult spontaneously hypertensive rats (SHR), an animal
model of attention deficit hyperactivity disorder
(ADHD). Behav Brain Res. 2010;215:39–44.
Pandolfo P, Machado NJ, Kofalvi A, Takahashi RN,
Cunha RA. Caffeine regulates frontocorticostriatal dopa-
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.
mine transporter density and improves attention and cognitive deficits in an animal model of attention deficit
hyperactivity disorder. Eur Neuropsychopharmacol. 2013;
23:317–328.
Nunes F, Pochmann D, Almeida AS, Marques DM, Porciuncula LO. Differential behavioral and biochemical responses to caffeine in male and female rats from a
validated model of attention deficit and hyperactivity
disorder. Mol Neurobiol. 2018;55:8496–8498.
Bernardi S, Faraone SV, Cortese S, et al. The lifetime
impact of attention deficit hyperactivity disorder: Results
from the National Epidemiologic Survey on Alcohol and
Related Conditions (NESARC). Psychol Med. 2012;42:
875–887.
Steinhausen HC, Novik TS, Baldursson G, et al. Coexisting psychiatric problems in ADHD in the ADORE
cohort. Eur Child Adolesc Psychiatry. 2006;15(Suppl
1):I25–I29.
Jensen CM, Steinhausen HC. Comorbid mental disorders
in children and adolescents with attention-deficit/
hyperactivity disorder in a large nationwide study. Atten
Defic Hyperact Disord. 2015;7:27–38.
Taurines R, Schmitt J, Renner T, Conner AC, Warnke A,
Romanos M. Developmental comorbidity in attentiondeficit/hyperactivity disorder. Atten Defic Hyperact
Disord. 2010;2:267–289.
Spencer TJ, Biederman J, Mick E. Attention-deficit/
hyperactivity disorder: Diagnosis, lifespan, comorbidities,
and neurobiology. Ambul Pediatr. 2007;7(1 Suppl):73–81.
Laurin D, Verreault R, Lindsay J, MacPherson K, Rockwood K. Physical activity and risk of cognitive impairment and dementia in elderly persons. Arch Neurol.
2001;58:498–504.
Duzel E, van Praag H, Sendtner M. Can physical exercise in old age improve memory and hippocampal function? Brain. 2016;139(Pt 3):662–673.
Berchtold NC, Castello N, Cotman CW. Exercise and
time-dependent benefits to learning and memory. Neuroscience. 2010;167:588–597.
Blumenthal JA, Babyak MA, Moore KA, et al. Effects of
exercise training on older patients with major depression.
Arch Int Med. 1999;159:2349–2356.
Leng M, Liang B, Zhou H, et al. Effects of physical exercise on depressive symptoms in patients with cognitive
impairment: A systematic review and meta-analysis. J
Nerv Ment Dis. 2018;206:809–823.
Porsolt RD, Anton G, Blavet N, Jalfre M. Behavioural
despair in rats: A new model sensitive to antidepressant
treatments. Eur J Pharmacol. 1978;47:379–391.
Detke MJ, Rickels M, Lucki I. Active behaviors in the rat
forced swimming test differentially produced by serotonergic and noradrenergic antidepressants. Psychopharmacology. 1995;121:66–72.
Machado DG, Cunha MP, Neis VB, et al. Rosmarinus
officinalis L. hydroalcoholic extract, similar to fluoxetine, reverses depressive-like behavior without altering
learning deficit in olfactory bulbectomized mice. J Ethnopharmacol. 2012;143:158–169.
Schamne MG, Mack JM, Moretti M, et al. The genderbiased effects of intranasal MPTP administration on anhedonic- and depressive-like behaviors in C57BL/6
mice: The role of neurotrophic factors. Neurotox Res.
2018;34:808–819.
Downloaded by SENCKENBERG/ZEITSCHRIFTEN from www.liebertpub.com at 12/02/18. For personal use only.
EFFECTS OF CAFFEINE IN ADHD
67. Kalueff AV, Tuohimaa P. Grooming analysis algorithm
for neurobehavioural stress research. Brain Res Protoc.
2004;13:151–158.
68. Treadway MT, Zald DH. Reconsidering anhedonia in depression: Lessons from translational neuroscience. Neurosci Biobehav Rev. 2011;35:537–555.
69. Boulle F, Massart R, Stragier E, et al. Hippocampal and
behavioral dysfunctions in a mouse model of environmental stress: Normalization by agomelatine. Transl
Psychiatry. 2014;4:e485.
70. Matheus FC, Rial D, Real JI, et al. Temporal dissociation
of striatum and prefrontal cortex uncouples anhedonia
and defense behaviors relevant to depression in 6OHDA-Lesioned Rats. Mol Neurobiol. 2016;53:3891–
3899.
71. Kaster MP, Machado NJ, Silva HB, et al. Caffeine acts
through neuronal adenosine A2A receptors to prevent
mood and memory dysfunction triggered by chronic
stress. Proc Natl Acad Sci USA. 2015;112:7833–
7838.
72. Ferre S, Quiroz C, Woods AS, et al. An update on adenosine A2A-dopamine D2 receptor interactions: Implications
for the function of G protein-coupled receptors. Curr
Pharm Des. 2008;14:1468–1474.
73. Real JI, Simões AP, Cunha RA, Ferreira SG, Rial D.
Adenosine A2A receptors modulate the dopamine D2
receptor-mediated inhibition of synaptic transmission
11
74.
75.
76.
77.
in the mouse prefrontal cortex. Eur J Neurosci. 2018;
47:1127–1134.
Pardo M, Lopez-Cruz L, Valverde O, et al. Adenosine
A2A receptor antagonism and genetic deletion attenuate
the effects of dopamine D2 antagonism on effort-based
decision making in mice. Neuropharmacology. 2012;
62:2068–2077.
Wei CJ, Singer P, Coelho J, et al. Selective inactivation
of adenosine A2A receptors in striatal neurons enhances
working memory and reversal learning. Learn Mem.
2011;18:459–474.
Gomez-Pinilla F, Hillman C. The influence of exercise
on cognitive abilities. Compr Physiol. 2013;3:403–428.
Leon MR. Effects of caffeine on cognitive, psychomotor,
and affective performance of children with attention-deficit/hyperactivity disorder. J Atten Dis. 2000;4:27–47.
Address correspondence to:
Rui Daniel Prediger, PhD
Department of Pharmacology
Center of Biological Sciences
Federal University of Santa Catarina (UFSC)
Florianópolis, SC 88049-900
Brazil
E-mail: rui.prediger@ufsc.br or ruidsp@hotmail.com