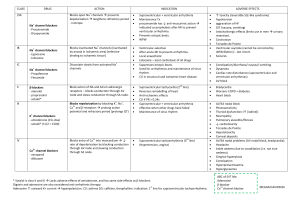
AN OVERVIEW OF CARDIOLOGY FOR THE BOARD EXAM Darcy Adin, DVM Supplemental Notes Drug therapy A. Antiarrhythmic therapy Classified according to the Vaughn-Williams scheme based on mechanism of action Class I - inhibits the fast sodium channel – further broken down into 3 subclasses Class IA examples include quinidine, procainamide. These are used to treat ventricular arrhythmias. Quinidine is used for conversion of AF in horses to sinus rhythm. Class IB – e.g. lidocaine – the treatment of choice for ventricular arrhythmias (can only be given parenterally). The main toxic effect of lidocaine is neurotoxicity. Class IC– (e.g. flecainide) these drugs are not used Class II – beta blockers – propranolol is the prototype. Used for ventricular and supraventricular arrhythmias. Low toxicity, inexpensive, effective. Anything ending in –olol is probably a beta blocker. Class III – inhibit the K channel to prolong repolarization. Examples include bretylium, amiodarone and sotalol. Class IV – calcium channel blockers. Examples include diltiazem, verapamil and nifedipine. Used for supraventricular arrhythmias. They slow conduction thru the AV node. Amlodipine is a newer calcium channel blocker with only peripheral vascular effects so it is effective for hypertension. B. Heart failure therapy 1 Diuretics - for treatment of fluid retentive states a) Loop diuretics – e.g. furosemide. These are potent diuretics that inhibit the Na/K/Cl cotransporter at the ascending loop of Henle. Side effects with high doses include electrolyte depletion and volume depletion. b) Thiazide diuretics – inhibit sodium and chloride reabsorption in the distal part of the nephron. e.g. hydrochlorthiazide. Similar side effects to loop diuretics. Less important for boards. c) K+ sparing diuretics – act on distal tubule to inihibit Na/K exchange. Example is spironolactone. Also less important for boards. Do not use osmotic diuretics (e.g. mannitol) for treatment of CHF!* 2 Angiotensin converting enzyme inhibitors Most commonly used ACE-I in veterinary medicine is enalapril. These drugs inhibit ACE to prevent the conversion of angiotensin I to angiotensin II. They have a mild vasodilating effect and inhibit Na/H2O retention by inhibiting aldosterone release. These drugs are used in conjunction with diuretics to treat CHF. Side effects can include mild hypotension and increases in BUN & creatinine in dogs that are dependent on angiotensin II for maintenance of GFR. We recommend monitoring of renal function in dogs started on an ACE-I 3 Positive Inotropes a) Digoxin – a weak positive inotrope via inhibition of the Na/K/ATPase pump. This promotes increased calcium concentration in the myocyte and enhanced contractiliity. Digoxin is also a negative chronotrope meaning it slows HR via its vagal activation. It has a long half-life (30-40 hrs) with a narrow therapeutic range. Toxic manifestations include GI signs and bradyarrhythmias (although tachyarrhythmias can also occur). Treatment usually is supportive with total discontinuation of digoxin. Atropine can be used to treat the bradyarrhythmias as it abolishes vagal tone. b) Dobutamine – a beta agonist. Used for IV treatment of low output failure c) Isoproterenol - a beta agonist d) Epinephrine / Norepinephrine 4 Vasodilators - used to reduce preload and afterload in heart failure a) Nitroprusside – arterial and venous vasodilation. IV CRI used in the acute heart failure situation. Must monitor BP. b) Hydralazine – arterial dilation only. Mainly used for hypertension or to reduce afterload in MR and thus reduce regurgitant fraction. 5 Antithrombotic agents a) Aspirin – cyclo-oxygenase inhibitor. Mainly used in an attempt to prevent thromboembolism in cats with cardiomyopathy. Although its efficacy is not great, it is well tolerated when given every 3 days. b) Warfarin – inhibits the formation of Vit K dependent clotting factors. This can also be used in cats, however clotting times need to be closely monitored and spontaneous hemorrhage is not uncommon. c) Heparin – binds to ATIII and thrombin for anticoagulation. 6 Oxygen Common Arrhythmias 1 Ventricular tachyarrhythmias With a few exceptions (not important for the boards), ventricular arrhythmias can be identified by their wide, bizarre complexes that are very dissimilar to sinus beats. They may be in singles (PVCs), couplets, triplets or as VT. Determination to treat depends on rate, polymorphism, underlying cardiac disease and hemodynamics of the patient. As stated above, lidocaine is the treatment of choice ( IV only). Some common oral therapies include procainamide, sotalol and propranolol. 2 Supraventricular tachyarrhythmias - usually appear approx 90% like the sinus beats since they take the same conduction through the ventricles. Supraventricular rhythms include sinus, atrial and AV junctional rhythms. Examples include SVT and AF. The usual therapeutic goal is to slow conduction through the AV node via digoxin, beta blockers or calcium channel blockers. Two determinations for susceptibility to atrial fibrillation are vagal tone and atrial mass. Therefore, it is not uncommon for normal horses to go into AF and thus conversion with quinidine is reasonable and possible. Most dogs and certainly cats that go into AF have serious underlying heart disease and thus the goal is to slow the ventricular response rate – 1st try digoxin and then add a beta blocker or calcium blocker if necessary. KNOW WHAT AF LOOKS LIKE – a rapid irregularly irregular supraventricular rhythm with no p waves. 3 Bradyarrhythmias a) sinus bradycardia b) 1st degree AV block – prolonged PR interval c) 2nd degree AV block – Mobitz I (PR prolongs and then drops a beat) – usually vagally mediated. Mobitz II (constant PR, then drops) – usually not vagally mediated. d) 3rd degree AV block – there is no association between the P waves and the QRS complexes. The supporting rhythm may be a junctional or ventricular escape rhythm. It is usually not responsive to atropine and usually requires permanent pacemaker implantation. e) Sick sinus syndrome – esp minature schnauzers. An intrinsic conduction disorder of the sinus node. Subsidiery pacemakers are also abnormal. Often requires pacemaker implantation. Hyperkalemia classically produces first, tall spiked T waves, then bradycardia, loss of P waves and a sinoventricular rhythm as it becomes more severe. Wandering pacemaker (changes in p wave morphology) and respiratory sinus arrhythmia are normal findings in dogs due to changes in vagal tone. Second degree AV block can be normal in athletic horses. Basic ECG Analysis The ECG is the test of choice for rhythm disturbances but is not very sensitive for chamber enlargement detection whereas echocardiography is quite sensitive. tall p waves – RAE wide p waves – LAE prolonged PR interval – 1st degree AV block wide QRS – LVE tall QRS – LVE T waves can be + or – and can vary greatly in dogs ST segment elevation or depression – myocardial ischemia/hypoxia Rt axis shift (deep s waves in I, II, III and aVF) – right heart enlargement or RBBB (RBBB is when the QRS complex is >80 ms duration) Small complexes can signify pericardial effusion Electrical alternans can signify pericardial effusion Feline Cardiac Disease 1 HCM – most common. LV hypertrophy can be due to hyperthyroidism, hypertension or primary HCM. The classic breed is the Maine coon, however it is seen in many other breeds and DSHs. Treatment involves heart failure therapy if appropriate and slowing of the HR to decrease systolic anterior motion (SAM) of the mitral valve with beta blockers or calcium channel blockers. Diltiazem is commonly used. Arterial thromboembolism is a common complication. 2 Restrictive / Unclassified Cardiomyopathy – normal wall thicknesses with large atria. Treatment and clinical outcome is similar to HCM 3 Dilated cardiomyopathy – uncommon today as most cases were caused by taurine deficiency. 4 Heartworm disease – uncommon in cats. Signs include respiratory (can look like asthma), GI (vomiting), and neurologic signs. Sudden death is common. Don't treat unless symptomatic. Canine Acquired Cardiac Diseases 1 Valvular disease - By far the most common cardiac disease seen by thegeneral practicioner in dogs. Older small breed dogs mostly. Uncommon in cats. The mitral valve is most often affected, sometimes the tricuspid as well. Due to myxomatous degeneration of the valve with age. Also called endocardiosis by some. 2 Dilated cardiomyopathy - a primary myocardial disease characterized by systolic dysfunction. Poor contractility is the primary abnormality followed by compensatory dilation. Doberman pinschers are the classic breed. Atrial fibrillation is a common arrhythmia with this disease. Can also occur in other large breed dogs. Boxers also get DCM but may present with ventricular arrhythmias and collapse only or initially. 3 Pericardial disease - Pericardial effusion typically occurs in large breed dogs. Causes include benign idiopathic effusion, heart base tumor, RA hemangiosarcoma, mesothelioma and infection. Findings include ascites, jugular pulses, weak femoral pulses, pulsus paradoxus, muffled heart sounds and tachycardia, globoid cardiomegaly on radiographs and small QRS complexes and electrical alternans on ECG. Lasix is contraindicated with pericardial effusion as it decreases preload and diastolic filling is already compromised. Pericardiocentesis is performed from the right side so as to avoid puncturing the coronary arteries. Traumatic pericarditis in cows is caused by penetration of a foreign object from the reticulum to the pericardium. 4 Heartworm disease - Know the life cycle! L1 are the microfilaria and are taken up by a mosquito during a blood meal. L1 matures to L3 in the mosquito. L3 migrates through the mosquito mouthparts after a blood meal and penetrates the dogs skin. L3 matures to L5 in the SQ tissues and L5 migrates to the pulmonary arteries where they mature into adult heartworms. The whole process takes approx 6.5 mos. - Know the various classes including caval syndrome. - Caval syndrome is when the adults who normally live in the pulmonary arteries migrate into the right heart producing hemoglobinemia, hemoglobinuria, hepatic and renal dysfunction and right heart failure. Most heartworm cases do not have caval syndrome and typical signs include coughing and exercise intolerance. - Pulmonary hypertension can occur and a split S2 may be audible due to delayed closure of the pulmonic valve. - Radiographic signs include enlarged, tortuous, and truncated pulmonary arteries and possibly right heart enlargement. - Occult heartworm disease implies a positive antigen test and a negative microfilaria test. - The antigen test detects adult female worms. - Treatment against the adults is with an arsenical. Caparsalate (thiacetarsemide) used to be used most commonly. Side effects include hepatotoxicity and phlebitis if injected perivascularly. Immiticide (melarsamine) is now available and is used more now as it involves only 2 IM injections, is effective and has few side effects. - Prevention can be obtained either monthly with ivermectin or milbemycin or daily with diethylcarbamazine. 5 Infective endocarditis - usually bacterial. A predisposing cause is usually not identified, however subaortic stenosis is a known risk factor. Many bacteria have been isolated, however Strep, Staph and E. coli are the classic. Findings include the presence of new heart murmur, signs of systemic embolism, cyclic fevers and lameness. IE occurs on the mitral and aortic valves in small animals and on the pulmonic and tricuspid valves in ruminants. Congenital Heart Disease 1. Stenotic lesions Subaortic stenosis – breed predispositions include G. Ret., Boxers, G. Shep, Rott., Newfies. This is a pressure overload so concentric LV hypertrophy occurs Pulmonic stenosis – Beagles and other small breed dogs especially. Also a pressure overload 2 Dysplastic lesions – Mitral valve dysplasia (esp bull terr) & Tricuspid dysplasia (esp labs) 3 Shunts PDA – most common defect in dogs. Continuous murmur. Typically small breeds (esp poodles) but G.Sheps also. Radiographs classically show a “ductal bump” on the aorta, enlarged PA, pulmonary overcirculation, and left sided enlargement, sometimes pulmonary edema. To determine what enlarges with a shunt, simply trace where the extra blood flows. Those chambers or vessels that accommodate the shunted blood will enlarge. VSD – another common congenital defect. This is the most common congenital defect in the horse. VSDs have a right sided systolic murmur associated with them. ASD – have a soft left basilar systolic murmur due to “relative PS” from the increased volume crossing the pulmonic valve. Tetralogy of Fallot – sounds like pulmonic stenosis with clinical signs of right to left shunting. The 4 essentials are pulmonic stenosis, overriding aorta, large VSD and RV concentric hypertrophy. Toxicities Oleander – the primary toxin is a cardiac glycoside so signs will be similar to dig toxicity Adriamycin (doxorubicin) – can cause myocardial failure and arrhythmias Selenium deficiency