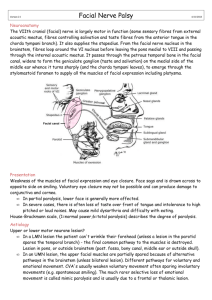
Chapter 1 INTRODUCTION Facial nerve enters temporal bone at the internal acoustic meatus then continues through the fallopian canal and exits via the stylomastoid foramen. Temporal branch of facial nerve lies within the parotid gland to cross the zygomatic arch. Zygomatic, buccal, and marginal mandibular branches of the facial nerve innervate the muscles of the facial expression. Facial nerve is a mixed nerve having motor, sensory and parasympathetic fibres. Nerve supplies motor innervations to the facial muscles, stapedius, stylohyoid muscle and posterior belly of digastric muscles. Parasympathetic fibers of nerve supply lacrimal and submandibular glands via the greater superficial petrosal nerve and chorda tympani respectively. Parasympathetic innervation controls flow and amount of saliva and tear production from glands. Sensory and parasympathetic function of nerve is carried by Intermediate nerve via chorda tympani which carry sensations from gustatory receptors, floor of the mouth and palate towards the solitary nucleus in medulla. Greater petrosal nerve provides cutaneous innervation from external auditory canal, concha, mucous membranes of the nasopharynx and palate (De Seta et al., 2014). Facial palsy is a dysfunction in VII cranial nerve. It can be due to any cause. This umbrella term covers all related terminologies of central facial palsy, idiopathic facial palsy and peripheral palsy. Facial palsy is divided into two types: supranuclear and infranuclear lesion. Neurons supplying the lower face quadrant receive upper motor neurones (UMN) from the opposite side of motor cortex. On contrary to this, neurons supplying the upper face quadrant receive UMN innervations from both sides. Thus, an UMN lesion causes one-sided facial palsy sparing some portion of frontalis and orbicularis oculi muscles because of the bilateral cortical innervation. Volitional facial movements are lost but facial movements can occur with emotional responses. In supranuclear lesion or central facial palsy, ipsilateral monoparesis, hemiparesis or dysphasia may be presented due to vast cerebrocortical damage. Infra nuclear or Lower motor neuron (LMN) facial palsy is known as one-sided paralysis of all facial expression muscles in both voluntary and emotional conditions. Forehead wrinkles are absent and eye closure is absent on affected side. Angle of the mouth droops and drooling may occur. Other defects such as aguesia, hyperacusis may also occur depending upon location of lesion (Newadkar, Chaudhari and Khalekar, 2016). Central facial palsy can be distinguished from Peripheral facial palsy by the involvement of periocular muscles in the latter one. In peripheral palsy, forehead wrinkles are absent, brow movements are lost and affected eye is unable to close properly called as Bell’s phenomenon. This occurs due to impairment of frontal branches of seventh cranial nerve. Although, in central facial palsy forehead area is spared due to dual innervation. There is no loss of forehead wrinkles, brow movements are normal and Bell’s Phenomenon is negative (Pereira et al., 2011). Central facial palsy or laqwah is referred to a neurological condition in which facial paralysis of lower contralateral side of face occurs due to some brain damage between the level of cerebral cortex to brainstem nuclei. In this condition, half side of face undergoes flaccid paralysis, thus this paralyzed side becomes weak and the face shifts towards the opposite side. This condition doesn’t involve eye and forehead region muscles (Shoja et al., 2009). Maas and Safdieh (2009) conducted a study on pathophysiology and principles of localization of stroke in which they stated that MCA infarction can cause some stroke with some typical symptoms specific for each artery. MCA strokes usually cause central facial palsy and upper limb paralysis. In case when superior division of MCA is affected, these symptoms may present: contralateral hemiplegia and hemisensory loss, Broca’s aphasia and visual perceptual disorders. Prevalence of facial palsy of grade III or more in the House Brackmann Scale was found more prevalent in women. Prevalence rate of disease increases with age. Other associated factors of facial palsy include positive history of cardiovascular disease and hypercholesterolemia. Facial palsy patients have higher rates of depression and have restricted social participation (Chang et al., 2016). Lower motor neuron lesion (LMNL) or peripheral facial palsy affects all muscles of the same side. In contrary, Upper motor neuron lesion (UMNL) or central facial palsy affects the lower quadrant of face at opposite side. Central facial palsy doesn’t affect frontalis muscle thus sparing the forehead movements (Reich, 2017). Bell's palsy is a type of peripheral paralysis of Facial Nerve (CN VII) which causes sudden unilateral facial weakness in facial expression muscles supplied by facial nerve. Associated symptoms may include changes in taste and hearing sensations, changes in facial sensations and ear pain. Facial nerve may be damaged by autoimmunological reactions, infection, ischemia, tumor or any other structure compressing the nerve. It exhibits lower motor neuron lesion symptoms. Usually, unilateral facial nerve is affected but rarely both facial nerves can be affected (Eviston et al., 2015). Bell’s palsy is one of the most frequent forms of facial palsy affecting 75% of cases. The peak incidence found between ages 14-45 years. Median age of onset being 40 years.2 Annually 11 and 40 or 9 and 240 cases per 100,000 subjects are reported with Bell Palsy. This epidemiological data can be influenced by the climate, race, genetic predisposition, co-morbid diseases of subjects and demographic characteristics of different areas. All these factors can cause variation in incidence and prevalence of Bell’s Palsy (DiegoSastre, Prim-Espada, and Fernández-García, 2005). These cases are predominantly reported in winter (31.38%) and autumn (30.13%) season. The seasonal incidence of Bell’s palsy is because of increased rate of viral upper respiratory tract infection during cold months. It supports the infectious cause of Bell’s palsy. Male and female, both are equally affected by Bell’s palsy. The prevalence increases in women during pregnancy i.e. 43 cases per 100,000 subjects. Unilateral facial paralysis is more common either left or right side. Bilateral facial paralysis at both sides of face is very rare with prevalence of 0.3-2% (Bašić-Kes et al., 2013). Amongst the four theories proposed for explaining the etiology of Bell's palsy: vascular, viral, immunological and compressive. Viral theory has remained the most popular one to explain the etiology. It is postulated that reactivation of dormant Herpes Virus can lead to Bell’s palsy. Association of herpes virus infection with Bell’s palsy has been supported by serological studies i.e. by measuring amount of IgM and IgG in Bell’s palsy patients (Musani et al., 2009). Bell's palsy occurs due to compression of the facial nerve at geniculate ganglion. Labyrinthine segment, first portion of facial canal has the narrowest diameter. It is most common site of compression in majority of Bell’s palsy patients. Inflammation of nerve in narrow portion causes compression and ischemia (Warner, 2005). Bell’s palsy is diagnosed by ruling out other diseases. Basic assessment involves a comprehensive history and physical examination. Bell’s palsy can be labeled as acute onset of one-sided, LMNL weakness of the facial nerve in the absence of a known cause. Comprehensive assessment aims to exclude organic causes of facial weakness such as neurological, otologic, infectious, inflammatory, neoplastic, cerebellopontine angle pathology and vascular insufficiency. Onset and timing of symptoms should be inquired in history (Phan, Panizza and Wallwork, 2016). Bell’s palsy comprise of 4 phases. Progress phase continues from 1-7 days of onset till complete progression when muscles go in flaccidity and facial asymmetry develops. Plateau phase lasts from peak of disease until recovery starts in 2-3 weeks. Prognosis of disease is predicted on basis of this phase. This phase passes through 2 different periods. At first, muscle strength is weak (in House Brackmann scale grade 5 or 6) just like the progress phase. In second period, muscles start gaining strength and they lie in less than 5 grade of House Brackmann scale. In the recovery phase, muscles have acquired enough strength and try to make facial expressions in a natural manner. HBGS is less than Grade 4. Sequelae phase will occur in the absence of treatment during first 3 phases. In case of incomplete recovery, the muscle strength will go on decreasing, length will be shortened and elasticity will also decrease. Complete paralysis will occur in severe cases. Adhesion of muscle and nerve, entrapment of facial nerve and lack of nerve excitability can be the other possible events occurring. So, patient complains of synkinesis, spasm, contractures, crocodile tears syndrome, deafness and tinnitus in the sequelae phase (Park et al., 2019). Synkinesis is a sequelae of Bell’s palsy which is aesthetically very disturbing for the patient. It affects the quality of life due to hesitation in social participations. Synkinesis is an abnormal facial movement performed involuntarily during voluntary movement of other muscles e.g smiling, blinking, eating or speaking. It occurs due to improper regeneration of facial nerve. Onset of synkinesis starts 3 to 4 months after Bell’s palsy and can continue for a period of 2 years. There are 2 common forms of synkinesis: ocular-oral and oral-ocular. Ocular synkinesis comprises of voluntary ocular movement combined with involuntary oral movement. Whereas, oral synkinesis comprise of voluntary oral movement combined with involuntary ocular movement (Pourmomeny, and Asadi, 2014). Patients with facial palsy show common attributes. In comparison to the unaffected side of the face, the side influenced by palsy has less wrinkles (as a result of muscular traction on the dermis), a less obvious nasolabial fold and a deviation of the side of the mouth and brow. The non-affected side of the face reacts to the facial palsy with a hyperkinetic response of the muscle tissues owing to the absence of tone on the affected side. This unevenness of vectoral powers makes facial deviations that are seen when the patient is still or is endeavoring to grin or smile. The muscles on the affected side of the face do not move. Therefore, there is an imbalance between the sides of face. The muscles on the non-paralyzed side of face over contract, having no strong rival. The non-paralyzed side of the face presents deviation in the labial, nasal, and orbital areas in any event, when the muscles are in a normal resting state. In these cases, facial rotation happens toward the side of the face that has not been affected, making the normal side of the face shorter. Treatment of facial palsy tries to restore the evenness of the mouth in the individual's smile and to get the contraction of the palpebral and oral sphincters, which are the most significant components in the facial cosmetic sense that are lost (de Maio and Bento, 2007). Physiotherapy treatment in the different phases of facial palsy targets to restore facial expression ability of facial muscles and to regain normal trophism, strength and function of facial muscles. It seeks to lessen or prevent complications to improve the psyche of patient and to achieve societal participation. Different techniques are utilized for treatment of facial palsy: massage, thermotherapy, electrotherapy, neural facilitation techniques, facial mime exercises and neuromuscular reeducation with EMG or mirror biofeedback and many others (Teixeira, Valbuza and Prado, 2011). Objective: The importance of the current systematic review is associated with the lack of comparative efficacy of intervention protocols used in the clinical practice of physiotherapy for treating facial palsy of different causes. The primary motive of the this research is to determine the efficacy of physiotherapy interventions used for treating facial palsy between 2015 and 2020 and suggesting an effective intervention plan for managing the condition. REFERENCES Bašić-Kes, V., Dobrota, V.Đ., Cesarik, M., Matovina, L.Z., Madžar, Z., Zavoreo, I. and Demarin, V., 2013. Peripheral facial weakness (Bell's palsy). Acta Clinica Croatica, 52, pp.195-202. Chang, Y.S., Choi, J.E., Kim, S.W., Baek, S.Y. and Cho, Y.S., 2016. Prevalence and associated factors of facial palsy and lifestyle characteristics: data from the Korean National Health and Nutrition Examination Survey 2010–2012. BMJ open, 6(11), p.e012628. De Diego-Sastre, J.I., Prim-Espada, M.P. and Fernández-García, F., 2005. The epidemiology of Bell's palsy. Revista de neurologia, 41(5), p.287. de Maio, M. and Bento, R.F., 2007. Botulinum toxin in facial palsy: an effective treatment for contralateral hyperkinesis. Plastic and Reconstructive Surgery, 120(4), pp.917-927. De Seta, D., Mancini, P., Minni, A., Prosperini, L., De Seta, E., Attanasio, G., Covelli, E., De Carlo, A. and Filipo, R., 2014. Bell’s palsy: symptoms preceding and accompanying the facial paresis. The Scientific World Journal, 2014. Eviston, T.J., Croxson, G.R., Kennedy, P.G., Hadlock, T. and Krishnan, A.V., 2015. Bell's palsy: aetiology, clinical features and multidisciplinary care. Journal of Neurology, Neurosurgery & Psychiatry, 86(12), pp.1356-1361. Maas, M.B. and Safdieh, J.E., 2009. Ischemic stroke: pathophysiology and principles of localization. Neurology, 13(Part 1), pp.2-16. Musani, M.A., Farooqui, A.N., Usman, A., Atif, S., Afaq, S., Khambaty, Y. and Ahmed, L., 2009. Association of herpes simplex virus infection and Bell's palsy. J Pak Med Assoc, 59(12), pp.823-5. Newadkar, U.R., Chaudhari, L. and Khalekar, Y.K., 2016. Facial palsy, a disorder belonging to influential neurological dynasty: Review of literature. North American journal of medical sciences, 8(7), p.263. Park, Y.K., Lee, C.I., Lee, J.H., Lee, H.J., Lee, Y.K., Seo, J.C. and Kim, J.S., 2019. A Facial Chuna Manual Therapy for Peripheral Facial Nerve Palsy. Journal of Acupuncture Research, 36(4), pp.197-203. Pereira, L.M., Obara, K., Dias, J.M., Menacho, M.O., Lavado, E.L. and Cardoso, J.R., 2011. Facial exercise therapy for facial palsy: systematic review and meta-analysis. Clinical rehabilitation, 25(7), pp.649-658. Phan, N.T., Panizza, B. and Wallwork, B., 2016. A general practice approach to Bell's palsy. Australian family physician, 45(11), p.794. Pourmomeny, A.A. and Asadi, S., 2014. Management of synkinesis and asymmetry in facial nerve palsy: a review article. Iranian journal of otorhinolaryngology, 26(77), p.251. Reich, S.G., 2017. Bell’s palsy. CONTINUUM: Lifelong Learning in Neurology, 23(2), pp.447-466. Shoja, M.M., Tubbs, R.S., Loukas, M., Shokouhi, G. and Ardalan, M.R., 2009. FACIAL PALSY AND ITS MANAGEMENT IN THE KITAB AL‐HAWI OF RHAZES. Neurosurgery, 64(6), pp.1188-1191. Teixeira, L.J., Valbuza, J.S. and Prado, G.F., 2011. Physical therapy for Bell's palsy (idiopathic facial paralysis). Cochrane Database of Systematic Reviews, (12). Warner, M., 2005. Bell’s Palsy. Greenberg's Text-atlas of Emergency Medicine, p.70.