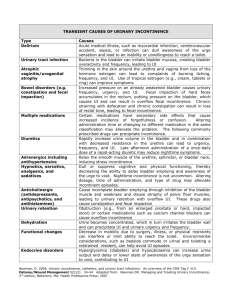
Geriatrics 03: 88-year-old female with urinary incontinence User: Daniel Amat Email: damat@med.miami.edu Date: May 26, 2020 7:04PM Learning Objectives Describe strategies for discussing personal or sensitive topics with older patients, particularly when a family member or friend is present at the visit. Identify the various types (stress, urge, mixed, and functional) of chronic urinary incontinence in the older adult. Describe both chronic and transient factors that can cause worsening urinary incontinence, including changes in bladder physiology with aging. Define the components of a through pelvic exam in a female with urinary incontinence and describe the implications of abnormal findings to explain contributors to urinary incontinence. Identify and list helpful behavioral interventions for urinary incontinence. Describe common side effects of medications used for urge urinary incontinence. Knowledge Patient Privacy When caring for an older patient with a family member or caregiver present, it is important not to make assumptions about the patient's ability to provide a history or the patient's desire for autonomy. The autonomy of a patient for whom you have no evidence of cognitive or judgmental impairment needs to be respected. If cognitive or judgmental impairment were present in a situation, you would still want to engage the patient and family member in the room together and ask permission. For some patients there may be issues that may feel too embarrassing to talk about such as bladder control or issues related to sexuality and sexual health. It is particularly important to ask the patient about their comfort level and the level of privacy the patient would prefer. It is best to ensure that, at each visit, an older adult has the opportunity to speak privately with their health care provider in the absence of family members or caregivers. Three screening questions to ask about incontinence We recommend using the "3IQ" or the 3 Incontinence Questionnaire, a self-administered 3-item questionnaire to guide this discussion and elicit the type of incontinence and assess symptom burden. A copy of the questionnaire can also be found in this article, The Sensitivity and Specificity of a Simple Test To Distinguish between Urge and Stress Urinary Incontinence. Here is a reproduction of the 3IQ: 3IQ 1: During the last 3 months, have you leaked urine (even a small amount)? □ Yes □ No 3IQ 2: During the last 3 months, did you leak urine (check all that apply): □ When you were performing some physical activity, such as coughing, lifting, or exercise? □ When you had the urge or the feeling that you needed to empty your bladder, but could not get to the toilet fast enough? □ Without physical activity and without a sense of urgency? 3IQ 3: During the last 3 months, did you leak urine most often: □ When you were performing some physical activity, such as coughing, lifting, or exercise? □ When you had the urge or the feeling that you needed to empty your bladder, but could not get to the toilet fast enough? □ Without physical activity and without a sense of urgency? □ About equally as often with physical activity as with a sense of urgency? Major Types of Urinary Incontinence Type of incontinence Answer Stress only or stress predominant Leakage with performing some physical activity, such as coughing, lifting or exercise. Urge only or urgency © 2020 Aquifer Acute onset of a strong need to urinate accompanied by bladder spasm and loss of urine. 1/4 predominant Other (not stress, not urgency) Leakage without physical activity and without a sense of urgency. Mixed (stress and urgency) Leakage occurring about equally as often with physical activity as with a sense of urgency. Other types of incontinence , besides those mentioned in the 3 IQ, have also been described. "Transient UI" and "functional UI" refer to those cases of UI caused or exacerbated by factors "outside" of the lower urinary tract such as: Comorbid conditions (e.g. stroke) Medications Impaired mobility When these factors are reversible, the UI is considered transient and may be referred to as "UI due to potentially reversible factors." Urinary incontinence may also be accompanied by other non-specific Lower Urinary Tract Symptoms (LUTS) such as: Frequency Nocturia Slow stream Hesitancy Sense of incomplete emptying Intermittent stream "Overactive bladder" is a term applied to a symptom complex of urgency due to uninhibited bladder contractions that can occur with or without urge UI and is often accompanied by frequency and nocturia. Precipitating factors to new-onset urinary incontinence Precipitating factors Mechanism Medical Conditions Urinary tract infection Cystitis with resulting urgency and frequency may precipitate urge incontinence, and should be considered even in the absence of painful urination. Urinalysis would be appropriate. Uncontrolled diabetes mellitus Diuresis associated with glycosuria can precipitate urinary incontinence and cause increased urinary frequency. Further, older adults with longstanding diabetes mellitus may develop neurogenic bladder (overflow incontinence). Mobility impairment Slowed mobility from any cause can exacerbate incontinence. An individual may postpone voiding to avoid pain related to degenerative joint disease or other pain sources; those who require assistance to toilet may not be able to move quickly enough to remain continent (also known as functional incontinence). Atrophic vaginitis Vaginal atrophy caused by decreased estrogen production and thinning of the vaginal epithelium can contribute to lower urinary tract symptoms. Vaginal atrophy has also been associated with recurrent urinary tract infections in post-menopausal women, and should be looked for during the pelvic examination. Constipation Rectal distension may cause overactive bladder, due to mass effect triggering detrusor hypercontractility. Mass effect may also cause urinary retention due to outflow obstruction. History would include a change in bowel symptoms. Diet Caffeine Caffeine is a mild diuretic and a bladder irritant. A comprehensive history would include additional questions about fluid intake and caffeinated products. Medications Diuretics Rapid increases in bladder volume may precipitate urge incontinence. Anticholinergics, Sedation may cause cognitive impairment that interferes with the ability to sense and respond to the need to void, particularly at night, resulting in enuresis. Anticholinergics may cause incomplete bladder emptying and © 2020 Aquifer 2/4 sedatives, and hypnotics constipation and thus contribute to frequency, urgency, and urinary incontinence. An example would be TYLENOL® PM, where the diphenhydramine component has anticholinergic as well as sedative effects. Physiological Changes of Bladder Function with Aging In older adults, changes to bladder physiology can occur at multiple levels: the urothelium (muscle atrophy, tissue atrophy) the detrusor muscle (detrusor smooth muscle responsiveness decreases) vascular changes central and peripheral nervous system innervation (including sacral reflex patterns) Age-related impaired detrusor contractility is associated with lower urine flow rates and a small increase in post-voiding residual volume (PVR) (so that the upper limit of normal for PVR increases from 50 ml for younger adults to 200 ml for older adults). Guidelines on PVR volume measures Post Void Residual Interpretation in older adults Volume <100 ml Normal 100 - 200 ml Elevated, and may necessitate further evaluation/intervention, such as stopping medications with anticholinergic side-effects. >200 ml Elevated, and further interventions, such as an indwelling bladder catheter or the need to do selfcatheterization to empty the bladder may be necessary. Pelvic Examination and Clinical Rationale Evaluation Type Clinical rationale (why the evaluation is needed) Atrophic vaginitis or other vaginal pathology can be seen. Labial skin and vaginal mucosal inspection Atrophy can contribute to dryness and causes symptoms of itching. Signs of vaginal atrophy include thinning, pallor, and loss of rugae. Signs of inflammation and dermatitis can include erythema, petechiae, telangiectasias, and friability. Labial fusion can also occur in older women due to atrophy. Pelvic organ prolapse can be evaluated by using half of a disposable speculum to gently pull down on the posterior or push up on the anterior vaginal walls. Split speculum examination Pelvic organ prolapse, as well as vaginal vault prolapse, can contribute to urinary symptoms and voiding dysfunction. Inadequate pelvic support, and/or pelvic wall defects all can lead to urinary incontinence by allowing bladder pressure to exceed urethral pressure. Stress incontinence can be evaluated with this test. Supine cough stress test The supine cough stress test involves asking the patient to cough and evaluating whether urine leaks from the urethra with the cough. Because this test is best performed when the patient has a full bladder, having the patient urinate before the pelvic examination for a urinalysis or a post-void residual volume (PVR) volume may not be ideal for this portion of the exam. Strength of the external anal sphincter can be assessed with the digital rectal examination (DRE). Digital rectal examination The DRE allows you to see if there is weakness of the external anal sphincter at rest and with a voluntary squeeze. It also allows you to assess for fecal impaction which can cause urinary retention and overflow-type urinary incontinence. Sacral reflexes, specifically S2 and S3, can be evaluated by the presence of an anal wink. Anal wink © 2020 Aquifer 3/4 The presence/absence of neurologic reflexes could indicate weak pelvic floor support or a neurologic impairment. Non-Pharmacological Measures for Urinary Incontinence In general, non-pharmacologic measures are considered first-line treatment for women with UI, regardless of type of UI. Some of these measures include: Advising the patient to decrease caffeine in general, and especially at night. Remember to remind patients that caffeine is not just found in coffee, but also in many teas and soft drinks. Caffeine is also an ingredient in some over-the-counter medications such as Excedrin™and Anacin™. Advise to limit fluid intake after 5 p.m.; just drink fluids earlier in the day. Recommending a schedule of regular voiding (e.g. every two hours) to avoid an overfull bladder. Pelvic floor muscle exercises. (See Teaching Point below.) Other non-pharmacological interventions that address potential functional components include: Leave a nightlight on to make it easier to get in and out of the bathroom safely at night. Raise the toilet seat with or without grab bars. For a good summary of pharmacologic and non-pharmacological interventions, see the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK): https://www.niddk.nih.gov/health-information/health-topics/urologic-disease/urinaryincontinence-women/Pages/facts.aspx#treatment Pelvic Floor Muscle Exercises Pelvic floor muscle exercises (also known as Kegel exercises) increase the strength of pelvic floor muscles and therefore can be helpful for both stress incontinence and UI/OAB in both men and women. Instruction on pelvic floor muscle exercises could be incorporated into the pelvic examination. Isolation of the proper pelvic floor muscles is an important aspect of doing pelvic floor muscle exercises correctly. A good example to tell your patients is to try to squeeze the rectum "like you are trying not to pass gas." Squeezing the external anal sphincter muscles will also contract the other involuntary pelvic floor muscles. If available, pelvic floor physical therapy along with biofeedback can be used to help increase the effectiveness of these exercises. References Brown JS, Bradley CS, Subak LL, et al. The sensitivity and specificity of a simple test to distinguish between urge and stress urinary incontinence. Ann Intern Med. 2006; 144(10):715-723. Dubeau CE. The aging lower urinary tract. J Urol. 2006; 175(3 Pt 2):S11-15. Goode PS, Burgio KL, Richter HE, Markland AD. Incontinence in older women. JAMA. 2010; 303(21):2172-2181. Micromedex. www.micromedexsolutions.com Accessed February 13, 2019. Zimmern P, Rubin C, Oksenberg L. SAGE: Urinary Incontinence in the Elderly. 2013; http://www.gerisage.com/modules/ui/index.htm. © 2020 Aquifer 4/4