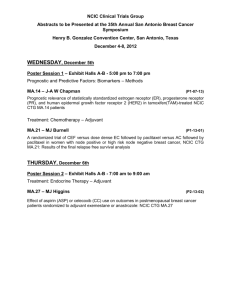
Adjuvant therapy Adjuvant therapy Survival with and without adjuvant tamoxifen in early breast cancer Mahesh K B Parmar ~1 year’s treatment 100 80 Node-negative Survival % 60 Abstract Adjuvant therapy can be defined as any treatment given after a first treatment (usually local, e.g. surgery, radiotherapy) for a primary ­tumour, when the first treatment was aimed at completely eradicating all ­visible tumour. Patients usually have no evidence of distant metastases. The basis for adjuvant therapy is the hypothesis that some patients have micrometastases that are not detected at the time of diagnosis of the primary tumour. Adjuvant therapy is given to target occult micrometastases, or to improve local tumour control. It can take the form of chemotherapy, hormonal therapy, immunotherapy or radiotherapy. Most commonly, chemotherapy is added to surgery, which is the first-choice treatment in most cancers. Over the last 10 years, adjuvant treatment of patients with disease confined to an organ (or the surrounding lymph nodes) has become possible, with benefits in common cancers (breast, colorectal) and in less common cancers such as osteosarcoma. Node-positive 40 Tamoxifen 20 Control 0 5 ~2 year’s treatment 100 80 Node-negative 60 Survival % Keywords adjuvant therapy; breast cancer; cancer; chemotherapy; colorectal cancer; ­neoadjuvant therapy; radiotherapy Node-positive 40 Breast cancer Tamoxifen Adjuvant tamoxifen: the first clear proof that adjuvant treatment has a role in the treatment of common tumours was a meta-analysis of all randomized trials comparing use of adjuvant therapy with no adjuvant therapy in women with early breast cancer treated initially by surgery. In these trials, it is clear that, in a wide range of women with oestrogen receptor-positive (or oestrogen receptor-unknown) early breast cancer, survival can be improved by the use of adjuvant tamoxifen (Figure 1). The magnitude of the improvement appears to depend largely on the duration of tamoxifen treatment and whether the disease is node positive or node negative. Although the relative reduction in risk of death appears to be similar in women with node-positive and node-negative disease, the absolute reduction is greater in nodepositive disease. There is strong indirect evidence from the meta-analysis and from randomized trials that 5 years’ tamoxifen is more effective than 2 years’ tamoxifen, which is more effective than treatment 20 0 Control 5 10 Follow-up (years) ~5 year’s treatment 100 Survival % 80 Node-negative 60 Node-positive 40 Tamoxifen 20 Mahesh K B Parmar BSc MSc Dphil is Head of the Cancer Group of the MRC Clinical Trials Unit, London, UK. He qualified in mathematics from the University of Exeter, and trained in medical statistics at the University of Nottingham and the University of Oxford. His research interests are the design and analysis of clinical trials, meta-analyses, Bayesian methods. Competing interests: none declared. MEDICINE 36:1 10 Follow-up (years) Control 0 5 10 Follow-up (years) Figure 1 38 © 2007 Published by Elsevier Ltd. Adjuvant therapy for 1 year (Figure 1). It is unknown whether more than 5 years’ tamoxifen is more or less effective than 5 years’ treatment; this is the subject of large randomized trials. The absolute difference in 10-year survival between 5 years’ and no tamoxifen is 6% in node-negative women and 11% in node-postive women. Any advantage with 10 years’ treatment over 5 years is likely to be smaller than this. Recently, a very large trial (the ATAC trial) has indicated that, for postmenopausal women with breast cancer, 5 years’ adjuvant treatment with the aromatase inhibitor, arimidex, is superior to adjuvant therapy with tamoxifen, and this is now a new standard of care.1 associated with considerable toxicity, however, and it is unclear whether such treatment is worth while in women aged 50–69 years with node-positive disease. Results suggest that combination chemotherapy including an anthracycline (e.g. doxorubicin, epirubicin) may be preferable to traditional standard combination therapy with cyclophosphamide, methotrexate and fluorouracil. This is the basis of a large, ongoing randomized trial. The effects of adjuvant combination chemotherapy seem to be additive to those of adjuvant tamoxifen. Herceptin is the first clinically available monoclonal antibody targeted against the HER-2 gene product. Recent randomized trials have shown that, in women with breast cancer whose tumours over-express HER-2, adjuvant herceptin significantly improves disease-free survival.2,3 This follows trials using heceptin in advanced disease, in which it has also been shown to improve survival. Adjuvant chemotherapy: meta-analysis has showed that adjuvant chemotherapy also improves survival in early breast cancer. The magnitude of the improvement appears to depend largely on age and nodal status (Figure 2). Adjuvant chemotherapy is Colorectal cancer Adjuvant chemotherapy has been shown to be effective in colorectal cancer. Surgery achieves macroscopic clearance of tumour in 80% of patients, but recurrence occurs in 50% of these – presumably because micrometastases were present at the time of surgery. Several randomized trials have shown that adjuvant 5-fluorouracil plus folinic acid improves survival in patients with Dukes’ C colorectal cancer (5-year survival increased from about 50% to 55%). The effect of adjuvant chemotherapy in patients with Dukes’ B disease remains unclear. Further reliable information on the role of adjuvant therapy in these patients will emerge in the next few years. Worldwide, 5-fluorouracil plus folinic acid has become a standard treatment in Dukes’ C disease. Although the increase in interest in 5-fluorouracil occurred as a consequence of trials showing a survival benefit with this drug combined with levamisole, the role of levamisole in this combination has been usurped by folinic acid, and treatment with levamisole has largely ceased. Survival with and without adjuvant polychemotherapy in early breast cancer Age 50 years 100 80 Survival % Node-negative 60 Node-positive 40 Polychemotherapy 20 Control 0 0 5 10 Follow-up (years) Age Adjuvant radiotherapy may have a role in the treatment of early rectal cancer, particularly for alleviating pain and staunching haemorrhage, and may improve survival. Both pre-operative and postoperative radiotherapy have been used widely; a recent randomized trial has indicated that a short course of pre-operative radiotherapy is superior, and this is now becoming standard practice.4 50 years 100 80 Survival % Node-negative Neoadjuvant therapy There is increasing interest in the possibility of giving adjuvant therapy as early as possible – that is, before primary therapy. Such treatment may shrink the primary tumour, making primary treatment easier and more effective, and may allow eradication of micrometastases at the first opportunity and therefore with a greater likelihood of success. This approach is sometimes termed ‘neoadjuvant’. Neoadjuvant therapy has perhaps been most successfully used in osteosarcoma, particularly of the limbs. Adjuvant combination chemotherapy both before and after primary treatment has become standard practice in this disease; limb-sparing surgery is now the rule rather than the exception, and amputation 60 Node-positive 40 Polychemotherapy 20 Control 0 0 5 10 Follow-up (years) Figure 2 MEDICINE 36:1 39 © 2007 Published by Elsevier Ltd. Adjuvant therapy is seldom used. Combination chemotherapy (often including cisplatin and doxorubicin) can achieve considerable and sometimes complete shrinkage of the primary tumour, facilitating surgical access. Neoadjuvant chemotherapy is under assessment in non-small cell lung cancer and bladder cancer. The value of modern radiotherapy in this setting needs to be assessed in large randomized trials. The future Adjuvant therapy has been shown to improve survival in many patients with cancer and during the next 10 years may be shown to have a role in the treatment of other tumours (e.g. non-small cell lung cancer, cervical cancer). Introduction of current adjuvant therapies in breast and colorectal cancer has been slow because most trials have not been large enough to establish clear benefits. Future trials must address this problem, and should sometimes include thousands of patients to reliably assess the benefits and deficits. ◆ Deleterious effects of adjuvant therapy Adjuvant therapy is not without toxicity and can theoretically cause more harm than good. This is perhaps best illustrated in a meta-analysis of all randomized trials of adjuvant radiotherapy in patients with non-small cell lung cancer in whom the primary treatment was surgery. This meta-analysis showed that survival was poorer in patients who received adjuvant radiotherapy than in those treated by surgery alone (Figure 3); the harm seemed to be greatest in patients with the earliest stages of the disease. It has been postulated that the main reason for this observation is toxicity of radiotherapy to the lungs and nearby organs in the postoperative setting. Most of these trials were undertaken many years ago, using what may now be considered outdated radiotherapy techniques. Nevertheless, the possibility remains that, even with modern techniques, postoperative adjuvant radiotherapy may be deleterious or may have a minimal positive effect. References 1Howell A, Cuzick J, Baum M, et al. Results of the ATAC (arimidex, tamoxifen, alone or in combination) trial after completion of 5 years’ adjuvant treatment for breast cancer. Lancet 2005; 365: 60–62. 2Romond EH, Perez EA, Bryant J, et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med 2005; 353: 1673–84. 3Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med 2005; 353: 1659–72. 4Quirke P, Sebag-Montefiore D, Steele R, et al. Local recurrence after rectal cancer resection is strongly related to the plane of surgical dissection and is further reduced by pre-operative short course radiotherapy. Preliminary results of the Medical Research Council (MRC) CR07 trial. J Clin Oncol 2006; 24: 3512. Survival with and without adjuvant postoperative radiotherapy in non-small cell lung cancer 1.0 Survival % 0.8 0.6 0.4 Further reading Early Breast Cancer Trialists’ Collaborative Group. Systemic treatment of early breast cancer by hormonal, cytotoxic, or immune therapy. Lancet 1992; 339: 1–15, 71–85. Midgley R, Kerr D. Colorectal cancer. Lancet 1999; 353: 391–9. PORT Meta-analysis Trialists’ Group. Postoperative radiotherapy in non-small cell lung cancer: systematic review and meta-analysis of individual patient data from nine randomised controlled trials. Lancet 1998; 352: 257–63. Postoperative radiotherapy 0.2 Control 0 0 12 24 36 48 60 Time (months) Figure 3 MEDICINE 36:1 40 © 2007 Published by Elsevier Ltd.