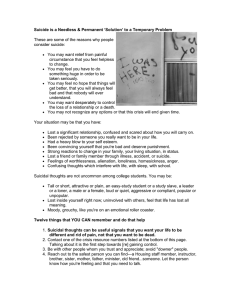
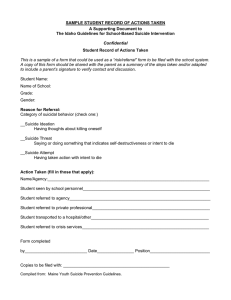
Student Name: Bryan LaPeer Course: NGR6102 – Care of the Adult I Assignment: History & Physical 2 Date: 11/20/20 Mr. A is a pleasant, 17-year-old, white, male. Referral: none Source and Reliability: Self and mother, both reliable sources. Chief complaint: “Medication change for depression.” HPI: Patient states that he has not been feeling the same over the past few weeks. He has no desire to complete daily activities and does not want to get up out of bed. Patient stays that he is always tired. He can not think of any life changes that occurred prior to this change in behavior. Nothing increases his energy levels or makes him feel better. The patient complains of no pain. His mother believes that he needs to have his medication switched to Celexa because that is what she takes for her depression. Allergies: NKA Current Mediation: Effexor 50mg BID. Childhood Illnesses – Medical & Surgical: Broken right tibia as a child. Psychiatric: Depression Health Maintenance. Immunizations: Immunizations up to date. Health maintenance not addressed. Family History: Mother – Depression. Father – Heart disease. Only child. Social History: Patient lives with his mother and his aunt and uncle. The patient’s father does not live with the patient or have much communication with him. They share one car between the four of them. The patient does not drink alcohol or use drugs. Exercise & Diet: not assessed. Safety Measures: Wears seat belt. No guns in the household. ROS: Denies headache, weight gain or loss sleep disturbances, guilt, change in memory, change in speech, no delirium, psychomotor retardation or agitation. Patient complains of fatigue, loss of appetite, interest deficit, concentration deficit, and worthless. Mother reports that the patient has become increasingly short tempered. Patient has not attempted suicide previously but has a plan to cut his wrists. He states that he as not tried it before because he does not like blood. Patient does not have any homicidal thoughts. O (Objective)/Physical Exam VS – BP: 118/68, HR: 86, RR: 16, Temp 98.6, weight: 151, height: 64 inches, Height- 5’7” Weight- 165 BMI- 25.9 General Appearance: Appears healthy and calm. Skin: Warm and moist. No lesions or rashes. HEENT: Oral mucosa is moist and without lesions, oropharynx pink with tonsils present. Fundoscopic exam shows a sharp disc with normal appearing vessels and no lesions. Neck: No JVD, no thyroidmegaly or thyroid masses. Cardiovascular: S1S2, RRR, no murmurs, no gallops. DP and radial pulses equal bilaterally. No lower extremity edema. Capillary refill less than 2 seconds. Lungs: CTA bilaterally, no wheezes, rhonchi, or crackles. Abdomen: soft, non-tender, non-distended, no bruits or pulsatile masses, bowel sounds are active, no organomegaly. Lower extremities: No tenderness or edema. Calves are equal in size bilaterally. ECG- normal sinus rhythm. No QRS, ST, or T wave abnormalities. Mr. A is alert, awake, oriented x 3. Patient is clean and dressed appropriate for age. Flat affect, anxious, depressed, withdrawn, and responses to questions are extremely short. Patient thought processes and content are abnormal with suicidal thoughts and a plan. Patient insight into mental status changes in intact, accepts judgment. Speech and language clear and understandable. No flight of ideas, obsessions, compulsions, delusions, illusions, or hallucinations. A (Assessment) Problem #1 – Change in mental status (F09) Most Likely Diagnosis #1 – Depression w/ suicidal ideations. This diagnosis was chosen because the patient has multiple risk factors including current suicidal plan, availability of lethal means, and male gender. Plan (P): Testing: none. Therapy/Treatment: Immediate referral to the local health department psychiatric department that takes walk in emergencies. Patient and mother agree that they will go tomorrow. Mother agrees that she will remove all knives from the house when they return home. The patient made a verbal contract that he will not harm himself. Education: Suicide is the 13th leading cause of death worldwide, with about 1 million deaths every year due to self-inflicted violence. In people ages 14-44 years, self-inflicted injury is the fourth leading cause of death and the sixth leading cause of ill health and disability worldwide, making suicide a significant public health concern. Suicide is more common among males, resulting from a constellation of psychological, biologic, genetic, social, and environmental factors. The two most prevalent mental disorders associate with suicide are major depressive disorder and substance abuse. Suicide defined refers to any thoughts or actions associated with an implicit or explicit intent to die. There are five components to suicide: ideation, intent, plan, access to lethal means, and history of past suicide attempts. Effective treatment of the patient’s mental disorder plays important role in suicide prevention. Follow-up: Patient and mother informed that if symptoms worsened this evening or prior to going to the psychiatrist that they are go to the closest emergency room for treatment. Patient and local health department will be contacted tomorrow by the referral specialist and a nurse to ensure that the patient followed through with the psychiatric consult. Conclusion There weren’t any labs drawn for this case, so none actually guided the provider’s choices on the patient’s care. But if there’s one that could have been relevant to the patient’s depression, standard thyroid tests could have been run, to determine if his condition might be related to an endocrinological lethargy (Bickley, 2019). But since this was a follow-up visit concerning a medication regimen he’d already started, it was decided not to. For this patient, pharmaceuticals are going to be the primary treatment for his psychological condition (Arcangelo & Peterson, 2016). However, he was educated on good practice for maintaining a level emotional state and state-of-mind, including seeking counseling and engaging in worthwhile social activities. With this patient, the key difficulty was getting him to express himself sufficiently to understand his feeling and his needs, so a course of action could be taken. As providers, it’s good practice to hone conversation skills so as to elicit the most desired information in as little time as we can take, so as not to delay the patient’s care (Domino, 2020). My key takeaway from this encounter would be the way you talk with a patient with this complaint, making an effort to be empathetic and understanding, to let them know their concerns are very much yours, too. I suppose the only thing different I might have done could have been to try him on a trial of the medication his mom suggested. But because the condition is so sensitive, it was decided not to change anything without the backing opinion of a psychiatric professional. For my future practice, I’d like to develop greater skills for addressing psychological needs, and I think it’d be beneficial to my future patients if I made a serious effort to do so. References Arcangelo, V.P. & Peterson, A.M. (2016). Pharmacotherapeutics for advanced practice: A practical approach (2nd ed.). Philadelphia: Lippincott Williams & Wilkins. 221-222. Bickley, L. S. (2019). Bates’ pocket guide to physical examination and history taking (6th ed.). Philadelphia: Lippincott Williams & Wilkins. 14-16. Domino, F. J. (Eds.). (2020). The 5-minute clinical consult. Philadelphia: Lippincott Williams & Wilkins. 21.