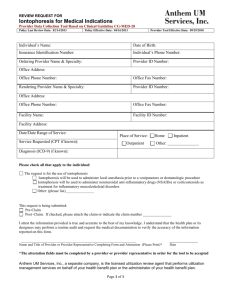
Journal of Controlled Release 284 (2018) 144–151 Contents lists available at ScienceDirect Journal of Controlled Release journal homepage: www.elsevier.com/locate/jconrel Review article Use of iontophoresis for the treatment of cancer a,⁎ James D. Byrne , Jen Jen Yeh b,c,d , Joseph M. DeSimone T b,c,e,f a Harvard Radiation Oncology Program, Boston, MA 02114, USA Lineberger Comprehensive Cancer Center, University of North Carolina at Chapel Hill, Chapel Hill, NC 27599, USA Department of Pharmacology, University of North Carolina at Chapel Hill, Chapel Hill, NC 27599, USA d Division of Surgical Oncology, Department of Surgery, University of North Carolina at Chapel Hill, Chapel Hill, NC 27599, USA e Department of Chemistry, University of North Carolina at Chapel Hill, Chapel Hill, NC 27599, USA f Department of Chemical and Biomolecular Engineering, North Carolina State University, Raleigh, NC 27695, USA b c A R T I C LE I N FO A B S T R A C T Keywords: Iontophoresis Chemotherapies Devices Drug delivery Cancer Despite major advancements in cancer treatments, there are still many limitations to therapy including off-target effects, drug resistance, and control of cancer-related symptoms. There are opportunities for local drug delivery devices to intervene at various stages of cancer to provide curative and palliative benefit. Iontophoretic devices that deliver drugs locally to a region of interest have been adapted for the treatment of cancer. These devices have shown promise in pre-clinical and clinical studies for retinoblastoma, skin, bladder, and pancreatic cancers. Herein, we review iontophoretic devices used in the management of cancer. 1. Introduction The 2018 estimate for new cancer diagnoses is 1,735,350 and cancer deaths is 609,640 [1]. Treatment of invasive cancer is largely determined by tumor histology, cancer stage, patient preference, and performance status. The primary treatment modalities include surgery, chemotherapy, and radiation therapy. For most solid tumors, surgery has remained the optimal therapy. Depending upon the cancer type, surgery may be feasible in only a small subset of patients [2–5, 7, 8]. Other modalities can be combined with surgery, including chemotherapy and radiation therapy. However, these therapies can be associated with major side effects including fatigue, diarrhea, xerostomia, and secondary malignancies [9]. As such, there is room for improvement in current cancer therapy. Local delivery of chemotherapies could provide curative or palliative benefit at various stages of cancer along with reduction of drug side effects [10]. In addition, this treatment could be an adjunct to surgery, radiation, and even systemically administered chemotherapy. An advantage to local delivery is the administration of agents that are too toxic when delivered systemically [10, 11]. Of the various methods for local chemotherapy delivery, iontophoresis has gained interest because of the control of drug delivery [12, 13]. Iontophoresis is a method of drug delivery where a mild electric current is applied around a drug reservoir to improve drug transport into the adjacent tissue. At least two electrodes, known as the anode and cathode, are required for drug delivery with one located in or in ⁎ Corresponding author at: Harvard Radiation Oncology Program, Boston, MA 02114, USA. E-mail address: jdbyrne@partners.org (J.D. Byrne). https://doi.org/10.1016/j.jconrel.2018.06.020 Received 19 April 2018; Received in revised form 14 June 2018; Accepted 14 June 2018 Available online 15 June 2018 0168-3659/ © 2018 Elsevier B.V. All rights reserved. proximity to a drug reservoir, as seen in Fig. 1. Parameters that influence iontophoretic drug delivery includes size of the electrode and quantity and time of current application [12]. These devices have been used in a variety of areas including oncology, anesthesia, sports medicine, nail fungus, and cosmetic treatments [11, 14–18]. Herein, we review the iontophoretic devices used to treat cancer. The focus is on both pre-clinical and clinical studies that showcase improvement above current therapy. In addition, we examine the barriers for iontophoretic drug delivery, challenges for clinical translation, and potential opportunities for further advancement. 2. Barriers to iontophoretic drug delivery 2.1. Physiological and biological barriers encountered by iontophoresis The tumor environment provides a significant barrier for drug transport. Tumors develop with an abundance of extracellular matrix (ECM). The large amount of ECM contributes to an abnormal tissue architecture of the tumor, and there is an abnormal growth of blood and lymphatic vessels. Tissue density, as a result of the ECM, may impede iontophoretic drug transport into and through tumors. Furthermore, abnormal vasculature may lead to deficiencies in oxygen and nutrients and the accumulation of metabolic byproducts in areas of the tumor [19, 20]. Regions of the tumor that have high accumulation of metabolic acids may have less cellular uptake of weakly basic chemotherapies, such as doxorubicin, resulting in lower drug efficacy [21]. Journal of Controlled Release 284 (2018) 144–151 J.D. Byrne et al. Fig. 1. Schematic representation of iontophoresis. The application of an electric potential generates ion flow between the anode (positive electrode) and cathode (negative electrode). Adapted with permission from reference [12]. Other barriers that influence iontophoretic drug transport include drug concentration and quantity of applied current. The quantity of drug delivered by iontophoresis is not always linearly correlated to drug concentration. This is a function of the physicochemical properties of the drug as well as formulation additives, which may complicate drug transport. As the concentration of a drug increases, additives in the formulation become competing ions that diminish the transport of the drug [12]. In addition, increasing the concentration of certain lipophilic cations, such as nafarelin, can inhibit electroosmosis through an effect from the hydrophobic surface being near to a positively charged component [27]. There seems to be a saturation effect up to a certain applied current for drugs. Tissue toxicity also limits quantity of applied current and, more importantly, current density. For example, there is a maximum tolerated current density of 0.5 mA/m2 for transdermal drug delivery due to skin irritation [28]. For cancer treated with iontophoresis, the maximum tolerated current density may be limited by the normal tissue adjacent to the tumors. Drug formulation plays a key role in iontophoretic drug transport. Each of the parameters must be accounted for when evaluating the preclinical and clinical utility of a drug for iontophoresis. Barriers for iontophoretic drug transport also depend upon the location of the tumor and placement of the iontophoretic device. For example, transdermal devices must deliver drug through the stratum corneum, which functions to protect the body against environmental toxins, dehydration, and infection. The stratum corneum is a major parameter that modulates transport. For this reason, methods to reduce or eliminate the stratum corneum have been investigated to improve iontophoretic drug transport [22]. For intravesical delivery, the bladder wall is relatively thin in comparison to skin; however, the major delivery challenge is the chemical environment of the bladder. As the bladder collects urine, dilution of the drug may reduce exposure and efficacy of the treatment [23, 24]. Overall, it is a matter of overcoming these barriers that will enable successful drug delivery using iontophoresis. 2.2. Drug formulation and device-related barriers for iontophoresis There are formulation and device parameters that may act as barriers to iontophoretic drug delivery, including the type of iontophoresis, pH of the drug solution, drug ionization and charge, tissue charge, drug concentration, and applied current. To understand the impact of these parameters, the two major iontophoretic transport mechanisms, including electrorepulsion and electroosmosis, must be delineated. Electrorepulsion involves charge-charge repulsion at the drug-electrode interface, and electroosmosis is a solvent flow mechanism induced by the current flow into tissue [25]. Adjusting the formulation and device parameters can result in differences in the relative importance of electrorepulsion and electroosmosis for the iontophoretic delivery of a drug. The physicochemical properties of a drug molecule and the pH of the drug solution have a direct impact on drug ionization and charge, tissue charge, and the type of iontophoresis that enables optimal drug transport. For example, increasing the pH of a weak base reduces the ionic fraction of the drug, which impacts transport in multiple ways. As the pH approaches the pKa for the weak base, the relative contribution of electrorepulsion to anodic ionotophoresis (anode-to-cathode) is reduced as there are less ions in solution. At pH values above the isoelectric point of tissue, such as skin, results in negatively charged tissue, and electroosmosis contributes more to transport of the weak base as a function of the negatively charged tissue [12]. Conversely, a higher solution pH for a weak acid, such as 5-fluorouracil, will increase the relative contribution of electrorepulsion when using cathodal (cathodeto-anode) iontophoresis [26]. The physicochemical properties of a drug molecule are critical in distinguishing the form of iontophoresis and the formulation pH most ideal for transport. 3. Approaches for iontophoretic drug delivery The iontophoretic delivery of anti-cancer agents can be categorized according to the device location. Devices have been developed for the following approaches: transdermal, transpapillary, intravesical, transscleral, and peri-pancreatic. Out of these different approaches, only devices used in transdermal and intravesical drug delivery have been tested clinically. The rest of the devices have been evaluated in preclinical studies. A summary of all routes of delivery and the drugs delivered can be found in Table 1. 3.1. Transdermal There has been a substantial quantity of work evaluating the transdermal iontophoretic delivery of drugs for skin cancers. This may be due to the ease of device delivery and testing. The broad range of agents tested for transdermal iontophoresis include small molecule chemotherapies, ALA for photodynamic therapy, vaccines and immunotherapy, and gene silencing with oligonucleotides [10, 29–50]. The versatility of agents delivered by iontophoresis is showcased in the transdermal route of delivery. Small molecule chemotherapies are among the most straight-forward drugs to deliver using iontophoresis due to size and stability. A variety of small molecule chemotherapies have been delivered in pre145 5-FU Cisplatin Cisplatin Bleomycin Vinblastine Doxorubicin Doxorubicin ALA ALA esters gp-100 peptide KVPRNQDWL CpG-ODN Miproxifen phosphate Transdermal Transdermal Transdermal Transdermal Transdermal Transdermal Transdermal Transdermal Transdermal Transdermal Transpapillary 146 * 6.0 MMC MMC δ-ALA MMC MMC MMC Carboplatin Carboplatin Gemcitabine FOLFIRINOX (Leucovorin, 5-FU, irinotecan, oxaliplatin) Intravesical Intravesical Intravesical Intravesical Intravesical Intravesical Transscleral Transscleral Peri-pancreatic Peri-pancreatic 20 mg/mL 10 mg/mL leucovorin 14.0 mg/mL 5-FU 14.4 mg/mL irinotecan 5 mg/ mL oxaliplatin 5.5–6 14.0 mg/mL 1.4–14.0 mg/mL 0.4 mg/mL 0.4 mg/mL 0.4 mg/mL 0.50% 0.8 mg/mL 0.4 mg/mL 0.1 mg/mL 0.5% (wt/wt) 0.5 mg/mL * 1–100 mM 15 mM 1.6 mg/mL * 3 mg/mL 10 mg/mL 5% (wt/wt) * 1 mg/mL Drug concentration * 5.5 5.8 * * * 6.45 MMC 6.55 * * 6.5 7.4 ~7.0 5.5 * * * 5.5 * * Drug pH Intravesical Transdermal Drug Route of delivery 10 min 20 min 2 mA 20 min 5 min 30 min 30 min 30 min 20 min 20 min 30 min 15 min 120 min 60 min 180 min 360 min 120 min 360 min 20 min 3 min 10 min 360 min 10 min 20–30 min Time 2 mA 5.0 mA/cm^2 2.57 mA/cm^2 20 mA 20 mA 20 mA 15 mA 15 mA 20 mA 5 mA 0.5 mA/cm^2 0.4 mA/cm^2 0.4 mA/cm^2 0.4 mA 0.4 mA 0.5 mA 0.5–1.5 mA 2 mA 4 mA 0.5 mA 4 mA 0.5–1.0 mA Current or current density 7 14 1 6 1 3 6–12 1 8 1 1 5 4 9 1 1 1 1–9 6 1 1 8 5 Number of treatments Pre-clinical Pre-clinical Pre-clinical Pre-clinical Clinical Clinical Clinical Clinical Clinical Pre-clinical Pre-clinical Pre-clinical Pre-clinical Pre-clinical Pre-clinical Pre-clinical Pre-clinical Clinical Clinical Clinical Pre-clinical Clinical Clinical Pre-clinical or clinical Tumor growth inhibition after iontophoretic treatment above and near tumor in mouse model of melanoma Significantly higher AUC for intrapapillary delivery compared to oral administration Iontophoresis increased MMC delivery 6-fold into viable human bladder compared to passive diffusion Iontophoresis increased MMC delivery 4–6-fold into viable human bladder at all depths compared to passive diffusion Disease free-interval was 14.5 months for iontophoresis of MMC compared to 10.5 months for MMC instillation only 5 of 6 patients were disease free at 10–16 months, 1 of 6 patients recurred after 10 months 58% patients with CR at 6 months and median time to recurrence was 35 months Patients treated with sequential BCG and iontophoresis of MMC had higher disease-free interval, lower recurrence, progression, overall mortality, and disease-specific mortality compared to BCG alone Intravesical iontophoresis of MMC before TURBT reduced recurrence rates and enhanced the disease-free interval compared to intravesical passive diffusion of MMC after TURBT and TURBT alone 50% of treated eyes exhibited control at carboplatin concentration 7.0 mg/mL Iontophoresis increased carboplatin in retina, choroid, and optic nerve compared to IV therapy Iontophoresis of gemcitabine resulted in tumor shrinkage compared to only tumor growth inhibition for IV delivery Iontophoresis of FOLFIRINOX induced more tumor shrinkage compared to only IV delivery CR in 96.2% of patients CR in 26.7% of lesions, PR in 46.7% of lesions, and minimal response in 26.7% of lesions PR in 100% of patients CR in 100% of patients CR in 29.0% of lesions, PR in 71.0% of lesions Doxorubicin formulated in chitosan gels improved diffusion to deeper skin layers Iontophoresis of DOX-SLNs delivered 56% of total drug into viable epidermis Increasing ALA concentration at pH 7.4 improves drug delivery Delivery of methyl-ALA resulted in 7-fold increase in SC and 18fold increase in viable skin compared to ALA Tumor growth inhibition in mouse model of melanoma Outcomes 70 10 67 66 60 59 58 56 55 54 53 51 47 46 40 42 38 36 33 34 37 29 31 Ref. Table 1 Summary of all the routes of delivery and the different anti-cancer agents tested. Abbreviations: 5-FU – 5-fluorouracil, ALA – aminolevulinic acid, AUC – area under the curve, BCG - Bacillus Calmette-Guerin, CpG-ODN – CpG-oligodeoxynucleotides, CR – complete response, DOX-SLN – doxorubicin-loaded solid lipid nanoparticles, MMC – mitomycin C, PR – partial response, TURBT – transurethral resection of bladder tumor. J.D. Byrne et al. Journal of Controlled Release 284 (2018) 144–151 Journal of Controlled Release 284 (2018) 144–151 J.D. Byrne et al. delivery of bleomycin and vincristine [34, 35]. In one such example, the iontophoretic delivery of bleomycin was pursued for the treatment of a patient with an extensive verrucous carcinoma of the face. The treatment was performed where the anode was a hollow plastic tip containing cotton soaked with bleomycin solution and placed over the region of interest; the cathode placed on the ipsilateral upper arm. Discrete treatments were performed every other day for a total of 6 treatments. The region of interest was biopsied 3 months after treatment and revealed only moderate fibrosis and minimal chronic inflammation but no malignant cells. Findings from a physical exam within 6 months of treatment demonstrated no residual disease [34]. Kaposi sarcoma lesions in patients with human immunodeficiency virus were treated using the iontophoretic delivery of vinblastine. Thirty-one lesions in 6 patients resolved after treatment [35]. The iontophoretic delivery of doxorubicin-filled matrices and nanoparticles has been investigated. Doxorubicin strongly interacts with the stratum corneum, which causes transdermally delivered drug to remain in the skin's superficial layer making this form of delivery challenging. Various formulations of doxorubicin, including water and gel formulations, were evaluated for transdermal delivery. It was found that the iontophoretic delivery of doxorubicin in water showed slightly better delivery compared to drug formulated in hydroxyethylcellulose or chitosan gels. However, the majority of drug delivered in the water formulation was delivered to the stratum corneum. Doxorubicin formulated in chitosan gels enabled deeper transport into the skin, likely due to the chitosan interacting with negative charges of the skin [38]. In addition, the same group evaluated the iontophoresis of ~175 nm doxorubicin-loaded solid lipid nanoparticles (DOX-SLNs) through the skin. They hypothesized that encapsulating doxorubicin in SLNs would enable deeper transport into the skin. Fifteen times less doxorubicin was found in the stratum corneum using DOX-SLNs compared to the water formulation of doxorubicin; however, there was a two-fold improvement in transport of doxorubicin to deeper parts of the skin using DOX-SLNs compared to the water formulation of doxorubicin [39]. The antitumor potential was evaluated in a mouse model of SCC. The iontophoretic delivery of DOX-SLNs showed significantly improved tumor growth inhibition over 21 days compared to the water formulation of doxorubicin and no treatment [40]. Photodynamic therapy involves the transdermal administration of 5-aminolevulinic acid (ALA), an amino acid necessary in the porphyrin synthesis pathway that leads to the accumulation of Protoporphyrin IX and, ultimately, tumor cell death. Transport of ALA significantly affects the efficacy of this therapy. Iontophoresis was tested to improve penetration depth and quantity of ALA delivered, and it was found that ALA was delivered at significantly higher concentrations using iontophoresis compared to passive diffusion [41]. The impact of ALA formulation composition, ionic strength, and ALA esters on iontophoresis were subsequently tested. It was found that reducing the concentration of sodium chloride in the ALA formulation improved ALA transport [42]. Among the ALA esters, the methyl ester significantly improved (~50-fold) ALA delivery compared to the ethyl, butyl, hexyl, and octyl esters. Size and lipophilicity were directly related to transport [43]. ALA and the methyl ester formulated in a gel were also evaluated for drug transport [44]. The quantity of ALA delivery by iontophoresis over 10 min was the same as passive diffusion over 6.5 h [45]. Lastly, permeation enhancers, including YAG laser, were evaluated in combination with the iontophoretic delivery of ALA. It was found that the use of a YAG laser significantly enhanced the iontophoretic delivery of ALA by up to 246-fold compared to skin permeation across intact skin [46]. In addition to chemotherapies and ALA, the iontophoresis of cancer vaccines and immunotherapies have been explored. The iontophoresis of nanogels containing gp-100 peptide KVPRNQDWL have been evaluated for potential use as a component of anti-cancer vaccines and were found to improve transport of the nanogels into the superficial layer of the skin, as well as accumulation of Langerhans cells. Efficacy of the treatment was tested in immunocompetent mice with melanoma. After Fig. 2. Patient with BCC of the face treated with cisplatin delivered iontophoretically. (A) Pre-treatment image of a 2.9 × 2.0 cm facial lesion. (B) Lesion after 3 treatments. (C) Resolved lesion 10 months after completion of treatment. Used with permission from references [32]. clinical and clinical studies for basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) [10, 29–35]. The iontophoretic delivery of 5-FU has been evaluated for the treatment of SCC in situ in 26 patients. Eight discrete treatments were performed over 4 weeks, with 25 of 26 patients having no clinical or histologic evidence of residual SCC in situ 3 months after the last treatment [30]. The use of transdermal iontophoresis of cisplatin was evaluated in patients with BCC and SCC; these patients experienced improvement in pain and onset of healing. Fig. 2 shows the treatment response of BCC on the face of a patient after cisplatin iontophoresis [32]. Another group used local iontophoretic delivery of cisplatin for residual lesions on the eyelid and periorbital region after systemic doxorubicin therapy, which resulted in partial remission of the lesions [36, 37]. Additional clinical reports that showcase the effectiveness of transdermal iontophoresis involve 147 Journal of Controlled Release 284 (2018) 144–151 J.D. Byrne et al. 3 treatments every 3 days, mice treated with the iontophoresis of the nanogels experienced significant tumor growth inhibition compared to no treatment [47]. The iontophoresis of CpG-oligodeoxynucleotides (CpG-ODN) was tested in a mouse model of melanoma and was found to result in significant tumor growth inhibition [48]. Others have evaluated the delivery of antisense oligonucleotide-dendrimer complexes and oligonucleotides for gene silencing of skin cancers [49, 50]. 3.2. Transpapillary The concept of transpapillary administration of cancer therapeutics was developed to treat ductal carcinoma in situ (DCIS) while limiting systemic drug exposure [51]. Iontophoretic devices were generated for the transpapillary delivery of the antiestrogen drug, miproxifen phosphate (TAT-59), and the dephosphorylated metabolite miproxifen (DPTAT-59). TAT-59 concentrations delivered by iontophoresis were found to be significantly higher than passive diffusion in rat in vitro skin studies. In a canine in vivo study, TAT-59 tissue concentrations were compared after 5 daily iontophoretic treatments and 14 days after oral delivery. Drug exposure as a function of area under the curve was found to be 3-fold larger for iontophoresis compared to oral administration [52]. Iontophoretic devices offer non-invasive routes for transpapillary drug delivery that can lead to higher drug concentrations in the mammary ducts for treatment of DCIS. 3.3. Intravesical Fig. 3. Depiction of the iontophoretic foley catheter for intravesical delivery. Used with permission from reference [63]. Non-muscle invasive bladder cancer (NMIBC) is primarily treated with transurethral resection of the bladder tumor (TURBT). For patients treated with a TURBT, the 2-year recurrence risk is slightly over 50%. To reduce recurrences, patients may also undergo intravesical instillation of drugs, including mitomycin C (MMC), after TURBT. Unfortunately, the penetration of MMC into the bladder mucosa is somewhat limited. The iontophoretic delivery of MMC into the bladder wall has been tested as a potential adjunct treatment to reduce recurrences [53–64]. The initial study using this technology evaluated the iontophoretic delivery of methylene blue dye into canine bladder wall compared to passive diffusion. A Foley catheter was designed with an electrode (anode) distal to the balloon. Two skin electrodes (cathodes) were placed on the abdomen of the dogs. The bladders were filled with methylene blue solution, and current was applied (pulsed) for a total of 40 min. After treatment, the bladders were immediately removed and frozen. Methylene blue was found deeper in the submucosa and the muscularis after the application of a current compared to passive diffusion. This study established the potential for iontophoresis as a treatment of bladder disorders [53]. Iontophoresis of MMC was subsequently compared to passive diffusion in ex vivo human bladder tissue. Using a diffusion cell, the iontophoretic transport of MMC was evaluated in human bladder tissue and compared to passive diffusion over a treatment period of 15 min. MMC delivered by iontophoresis was found to be 21.5 μg/g (mean), which was significantly greater than passive diffusion (3.4 μg/g, mean) [54]. Further studies by the same group evaluated duration of current applied and depth of MMC transport compared to passive diffusion. The concentration of drug delivered into bladder wall plateaued at 15 min of applied current and was similar in quantity to 30, 45, and 60 min. When current was applied at 30 min, there was at least 4-fold greater concentration of drug transported into the different layers of bladder wall compared to passive diffusion [55]. These studies showcased the ability to deliver MMC deep into the bladder wall, which was an improvement above the standard drug instillation. The utility of iontophoresis of MMC for NMIBC was next evaluated in clinical trials [56–58]. Twenty-eight patients were administered 8 weekly treatments of either iontophoretically delivered mitomycin C for 20 min or intravesical mitomycin C (passive diffusion) instilled for approximately 2 h [56]. Fig. 3 demonstrates the device and device setup used in clinical practice [63]. Of the patients treated with iontophoresis, 6 of 15 patients (40%) experienced a pathologic complete response (pCR), which was similar to passive diffusion with 5 of 12 patients (41.6%) demonstrating a pCR. Among patients that had a pCR, patients treated with iontophoresis recurred at a rate of 33% versus 60% in patients who received passive diffusion after 6 and 7.6 months, respectively [56]. In another study, patients with recurrent bladder carcinoma in situ were treated with photodynamic therapy after ALA was driven into the bladder wall by iontophoresis. After administration of the ALA, the bladder was treated with a laser at a wavelength of 632 nm. In follow-up, 5 of the 6 patients were disease-free at 10 months, and 1 patient developed a recurrence at 10 months [57]. Although the sample sizes of these studies were very small, the data justified additional prospective study in superficial bladder cancer. There were multiple prospective trials testing the iontophoresis of MMC after a TURBT. In one of the initial prospective trials, the iontophoresis of MMC was compared to passive diffusion of MMC and BCG therapy. The treatment regimen involved 6 weekly doses of intravesical MMC therapy and then monthly maintenance doses up to 1 year. At 6 months, the percentage of patients with pCR was 58%, 31%, and 64% for iontophoresis of MMC, passive diffusion of MMC, and BCG, respectively. The median time to recurrence was 35, 19.5, and 26 months for iontophoresis of MMC, passive diffusion of MMC, and BCG, respectively [59]. Results of this study suggested that the iontophoresis of MMC was a reasonable alternative in patients unable to receive BCG. In a different prospective trial, an alternating regimen of iontophoresis of MMC and intravesical BCG (3 cycles of 2 weekly treatments of BCG followed by 1 treatment of the iontophoretic delivery of MMC) was compared to BCG alone (6 weekly treatments). Both treatment groups were given maintenance therapy for up to 1 year. In patients treated with alternating iontophoresis of MMC and BCG experienced a diseasefree survival of 69 months compared to 21 months for BCG alone. In addition, patients treated with alternating iontophoresis of MMC and BCG had lower recurrence rates (41.9% versus 57.9%) and diseasespecific mortality (5.6% versus 16.2%) compared to BCG alone [60]. 148 Journal of Controlled Release 284 (2018) 144–151 J.D. Byrne et al. multiple agents simultaneously using a single device. Multiple groups have evaluated the co-iontophoresis of drugs to improve management of pancreatic cancer, chemotherapy-induced nausea, and head and neck cancer [70, 71, 73, 74]. Taking advantage of the implanted device for pancreatic cancer, the iontophoresis of the FOLFIRINOX regimen was tested in the orthotopic PDX model as mentioned previously [70, 71]. The effect of drug formulation on the electro-transport of the FOLFIRINOX regimen was tested prior to the evaluation of efficacy. Three different formulations were tested with varying number of drugs per solution, and it was found that a 2-drug cocktail enabled better delivery of the drugs compared to a 4-drug cocktail or individual drugs [70]. It was concluded that electrolyte concentration in the formulation directly impacts drug transport. Chemotherapy-induced nausea is a significant problem encountered during administration of chemotherapy. The transdermal iontophoretic delivery of multiple anti-emetics (granisetron, metoclopramide, and dexamethasone) were tested to reduce chemotherapy-induced nausea. They demonstrated that high concentrations of drug could be achieved with delivery rates of 0.5, 3.3, and 2.0 μg*cm−2*min−1 for granisetron, metoclopramide, and dexamethasone respectively, through the skin of rats [73]. The co-iontophoresis of 5-FU and leucovorin was also evaluated for head and neck cancers. Iontophoresis was tested in bovine mucosa and was found to increase the delivery of 5-FU (8-fold increase) and leucovorin (3-fold increase) compared to passive diffusion [74]. In conclusion, co-iontophoresis can be successfully used to deliver multiple drug simultaneously. The utility of the iontophoresis of MMC has also been investigated before TURBT. Patients treated with iontophoresis of MMC compared to passive diffusion had lower recurrence rates (38% versus 59%) and disease-free survival (52 months versus 16 months) [61]. Despite these results, the adoption of the iontophoresis of MMC has been slow. 3.4. Transscleral Systemic chemotherapy is one of the primary treatments for bilateral retinoblastoma. However, it is often not sufficient to induce a complete response and is used in combination with cryoablation or laser ablation if vision cannot be preserved [65]. There also exists the concern for an increased risk of secondary tumors caused by chemotherapy in patients with RB1 mutations [66]. To reduce these effects, multiple groups have compared local iontophoretic administration of carboplatin to the eye to systemic administration in pre-clinical animal models [65–67]. The transscleral iontophoresis of carboplatin was tested in mouse models of retinoblastoma. Dose escalation of carboplatin concentration, including 1.4, 7.0, 10.0, or 14.0 mg/mL, was evaluated using twice weekly treatments over 3 weeks. These studies were compared to a no current control, and inhibition of the tumor was found after multiple iontophoretic treatments. There was minimal to no ocular toxicity up to 10 mg/mL carboplatin [67]. Furthermore, their team studied the pharmacokinetics of the iontophoretic administration of carboplatin after a single treatment in rabbits. Iontophoretic delivery of carboplatin resulted in higher concentrations in ocular tissue and optic nerve compared to IV delivery. Again, there was no evidence of ocular toxicity after iontophoretic delivery [68]. Additional evaluation of carboplatin delivery via a hydrogel-iontophoresis system did not result in improved delivery compared to passive diffusion [69]. 5. Challenges for clinical translation There are many different challenges to the successful translation of iontophoretic devices, including depth of drug transport, toxicity, location of tumor, and transport of large molecules. From our own data, gemcitabine was found up to 1 cm away from the electrode in canine pancreatic tissue. However, the quantity of drug at that distance away may be subtherapeutic [11]. In addition, another group demonstrated the distance of mitomycin C transport was greater than 4 mm into the bladder wall [54]. Passive diffusion plays an additional role in drug transport away from the device. Drug delivery in large, bulky tumors may be a significant challenge that will need to be investigated. Additional barriers to successful translation include toxicity to normal tissue and location of tumor. Iontophoretic devices are able to administer large concentrations of drugs to the local area around the device and, thus, normal tissue nearby may be impacted. Toxicity profiles will need to be evaluated, especially in sensitive or vital areas. For example, the delivery of drugs directly into the pancreas raises the concern for pancreatitis [75]. In addition, the location of the tumor plays a role in accessibility. If the device is unable to be positioned for optimal delivery, the full utility of the device may not be realized. Lastly, the list of drug candidates for iontophoresis is limited by size and potency. Antibodies, large molecules, and nanoparticles are particularly challenging to deliver [76]. The voltage required for delivery of these agents is limited by normal tissue toxicity. In addition, compounds that require very high concentrations to be effective may not be useful. Other strategies to increase drug concentration may be needed to enhance efficacy [13]. 3.5. Peri-pancreatic Systemic chemotherapy has been minimally successful in controlling pancreatic tumor growth as a result of poor drug transport into pancreatic tumors. Implantable iontophoretic devices were developed for implantation directly onto pancreatic tumors. Initial device studies involved single treatments performed in ex vivo patient-derived xenograft (PDX) tumors, showing a dose-dependent relationship between concentration of gemcitabine in the device and gemcitabine delivered. The efficacy of the iontophoretic devices was tested in an orthotopic PDX mouse model. Devices were implanted directly on orthotopic tumors and resided on the tumors for up to 2 months, as seen in Fig. 4A and B. Biweekly device treatments for 7 weeks with iontophoresis of gemcitabine demonstrated significant tumor shrinkage (mean log2-fold change in tumor volume of −0.8) compared to tumor growth in IV gemcitabine, IV saline, and device saline groups (mean log2-fold change in tumor volume of 1.1, 3.0, and 2.6, respectively) (Fig. 4C). The iontophoretic delivery of gemcitabine was subsequently tested in dogs demonstrating a significantly higher local concentration of drug delivered (7-fold difference) and lower systemic drug level compared to drug delivered by IV [11]. Furthermore, delivery of the drug regimen known as FOLFIRINOX (folinic acid, fluorouracil, irinotecan, and oxaliplatin) was evaluated in the same orthotopic PDX model [70, 71]. It was found that the iontophoresis of FOLFIRINOX resulted in tumor regression in 50% of the mice treatment compared to 0% of mice treated with IV FOLFIRINOX after 7 weeks of weekly treatment [71]. This iontophoretic device made possible the local delivery of multiple agents to pancreatic tumors. 6. Conclusion Iontophoresis can potentially offer a local drug delivery approach resulting in high concentrations of anti-cancer drugs in the areas of greatest need. Simultaneous delivery of multiple different drugs is also feasible using iontophoresis. It may become a treatment option for certain cancers, including retinoblastoma, skin, bladder, and pancreatic cancers. The translation of iontophoretic devices is contingent on 4. Co-iontophoresis of chemotherapies Current cancer therapy relies heavily on the delivery of multiple agents for synergistic benefit to improve efficacy and reduce drug resistance [72]. Iontophoresis provides an opportunity for delivery of 149 Journal of Controlled Release 284 (2018) 144–151 J.D. Byrne et al. Fig. 4. Iontophoretic delivery of gemcitabine through devices implanted on orthotopic pancreatic tumors. (A) Images of the device. (B) The setup for device delivery where the device (anode) and the counter electrode (cathode) were connected to an external power supply. (C) The efficacy of the iontophoretic device treatments were tested in orthotopic PDX mice. Data are fold change in tumor volume (log2). Adapted with permission from reference [11]. finding the right situation where the device can add benefit over current therapies. [11] J.D. Byrne, M.R. Jajja, A.T. O'Neill, L.R. Bickford, A.W. Keeler, N. Hyder, K. Wagner, A. Deal, R.E. Little, R.A. Moffitt, C. Stack, M. Nelson, C.R. Brooks, W. Lee, J.C. Luft, M.E. Napier, D. Darr, C.K. Anders, R. Stack, J.E. Tepper, A.Z. Wang, W.C. Zamboni, J.J. Yeh, J.M. Desimone, Local iontophoretic administration of cytotoxic therapies to solid tumors, Sci. Trans. Med. 7 (2015) 273ra14. [12] Y.N. Kalia, A. Naik, J. Garrison, R.H. Guy, Iontophoretic drug delivery, Adv. Drug Deliv. Rev. 27 (2004) 619–658. [13] R.H. Guy, Interview with Richard H guy by Hannah Coaker, Ther. Deliv. 5 (2014) 123–128. [14] A. Fanelli, M.C. Sorella, J.E. Chelly, Iontophoretic transdermal fentanyl for the management of acute perioperative pain in hospitalized patients, Expert. Opin. Pharmacother. 17 (2016) 571–577. [15] M.C. Edmondson, R. Day, D. Wood, Vancomycin iontophoresis of allograft bone, Bone Joint Res. 3 (2014) 101–107. [16] L. Runeson, E. Haker, Iontophoresis with cortisone in the treatment of lateral epicondylalgia (tennis elbow)–a double-blind study, Scand. J. Med. Sci. Sports 12 (2002) 136–142. [17] S. Baswan, G.B. Kasting, S.K. Li, R. Wickett, B. Adams, S. Eurich, R. Schamper, Understanding the formidable nail barrier: a review of the nail microstructure, composition and diseases, Mycoses 60 (2017) 284–295. [18] J.A. Scott, A.K. Banga, Cosmetic devices based on active transdermal technologies, Ther. Deliv. 6 (2015) 1089–1099. [19] M. Yu, I.F. Tannock, Targeting tumor architecture to favor drug penetration: a new weapon to combat chemoresistance in pancreatic cancer? Cancer Cell 21 (2012) 327–329. [20] V.P. Chauhan, T. Stylianopoulos, Y. Boucher, R.K. Jain, Delivery of molecular and nanoscale medicine to tumors: transport barriers and strategies, Annu. Rev. Chem. Biomol. Eng. 2 (2011) 281–298. [21] J.K. Saggar, M. Yu, Q. Tan, I.F. Tannock, The tumor microenvironment and strategies to improve drug distribution, Front. Oncol. 3 (2013) 154. [22] J.Y. Fang, W.R. Lee, S.C. Shen, Y.P. Fang, C.H. Hu, Enhancement of topical 5-aminolaevulinic acid delivery by erbium:YAG laser and microdermabrasion: a comparison with iontophoresis and electroporation, Br. J. Dermatol. 151 (2004) 132–140. [23] M.S. Highley, A.T. van Oosterom, R.A. Maes, E.A. De Bruijn, Intravesical drug delivery. Pharmacokinetic and clinical considerations, Clin. Pharmacokinet. 37 (1999) 59–73. [24] H. Zargar, J. Aning, J. Ischia, A. So, P. Black, Optimizing intravesical mitomycin C therapy in non-muscle-invasive bladder cancer, Nat. Rev. Urol. 11 (2014) 220–230. [25] R.H. Guy, Y.N. Kalia, M.B. Delgado-Charro, V. Merino, A. Lopez, D. Marro, Iontophoresis: electrorepulsion and electroosmosis, J. Control. Release 64 (2000) 129–132. [26] V. Merino, A. Lopez, Y.N. Kalia, R.H. Guy, Electrorepulsion versus electroosmosis: effect of pH on the iontophoretic flux of 5-fluorouracil, Pharm. Res. 16 (1999) 758–761. Acknowledgements and funding information J.D.B. was supported by the UNC Medical Scientists Training ProgramNIGMS-2-T32-GM008719, and PhRMA Foundation Fellowship. Conflicts of interest J.D.B., J.J.Y., and J.M.D. hold equity in the start-up company, Advanced Chemotherapy Technologies L.L.C. References [1] R.L. Siegel, K.D. Miller, A. Jemal, Cancer statistics, 2018, CA-A Cancer J. Clin. 68 (2018) 7–30. [2] C.R. Ferrone, M.F. Brennan, M. Gonen, D.G. Coit, Y. Fong, S. Chung, L. Tang, D. Klimstra, P.J. Allen, Pancreatic adenocarcinoma: the actual 5-year survivors, J. Gastrointest. Surg. 12 (2008) 701–706. [3] S. Gillen, T. Schuster, C. Meyer Zum Büschenfelde, H. Friess, J. Kleeff, Preoperative/neoadjuvant therapy in pancreatic cancer: A systematic review and meta-analysis of response and resection percentages, PLOS Med. 7 (2010) e1000267. [4] M.F. Berry, Esophageal cancer: staging system and guidelines for staging and treatment, J. Thorac. Dis. 6 (2014) S289–S297. [5] S. Lin, K. Hoffmann, P. Schemmer, Treatment of hepatocellular carcinoma: A systematic Review, Liver Cancer 1 (2012) 144–158. [7] C. Laroche, F. Wells, R. Coulden, S. Stewart, M. Goddard, E. Lowry, A. Price, D. Gilligan, Improving surgical resection rate in lung cancer, Thorax 53 (1998) 445–449. [8] S. Msika, M.A. Tazi, A.M. Benhamiche, C. Couillault, M. Harb, J. Faivre, Population-based study of diagnosis, treatment and prognosis of gastric cancer, Br. J. Surg. 84 (1997) 1474–1478. [9] H. Suit, S. Goldberg, A. Niemierko, M. Ancukiewicz, E. Hall, M. Goitein, W. Wong, H. Paganetti, Secondary carcinogenesis in patients treated with radiation: a review of data on radiation induced cancers in human, non-human primate, canine and rodent subjects, Radiat. Res. 167 (2007) 12–42. [10] J.B. Wolinsky, Y.L. Colson, M.W. Grinstaff, Local drug delivery strategies for cancer treatment: gels, nanoparticles, polymeric films, rods, and wafers, J. Control. Release 159 (2012) 14–26. 150 Journal of Controlled Release 284 (2018) 144–151 J.D. Byrne et al. (1996) 1496–1501. [54] S.M. Di Stasi, G. Vespasiani, A. Giannantoni, R. Massoud, S. Dolci, F. Micali, Electromotive delivery of mitomycin C into human bladder wall, Cancer Res. 57 (1997) 875–880. [55] S.M. Di Stasi, A. Giannantoni, R. Massoud, S. Dolci, P. Navarra, G. Vespasiani, R.L., Stephen, electromotive versus passive diffusion of mitomycin C into human bladder wall: concentration-depth profiles studies, Cancer Res. 59 (1999) 4912–4918. [56] M. Brausi, B. Campo, G. Pizzocaro, P. Rigatti, A. Parma, G. Mazza, A. Vicini, R.L. Stephen, Intravesical electromotive administration of drugs for treatment of superficial bladder cancer: a comparative phase II study, Urology 51 (1998) 506–509. [57] A. Stenzl, I. Eder, H. Kostron, H. Klocker, G. Bartsch, Electromotive diffusion (EMD) and photodynamic therapy with delta-aminolaevulinic acid (delta-ALA) for superficial bladder cancer, J. Photochem. Photobiol. B 36 (1996) 233–236. [58] C.R. Riedl, M. Knoll, E. Plas, H. Pfluger, Intravesical electromotive drug administration technique: preliminary results and side effects, J. Urol. 159 (1998) 1851–1856. [59] S.M. Di Stasi, A. Giannantoni, R.L. Stephen, G. Capelli, P. Navarra, R. Massoud, G. Vespasiani, Intravesical electromotive mitomycin C versus passive transport mitomycin C for high-risk superficial bladder cancer: a prospective randomized study, J. Urol. 170 (2003) 777–782. [60] S.M. Di Stasi, A. Giannantoni, G. Arcangelo, M. Valenti, G. Zampa, L. Storti, F. Attisani, A. De Carolis, G. Capelli, G. Vespasiani, R.L. Stephen, Sequential BCG and electromotive mitomycin versus BCG alone for high-risk superficial bladder cancer: a randomized controlled trial, Lancet Oncol. 7 (2006) 43–51. [61] S.M. Di Stasi, M. Valenti, C. Verri, E. Liberati, A. Giurioli, G. Leprini, F. Masedu, A.R. Ricci, F. Micali, G. Vespasiani, Electromotive instillation of mitomycin immediately before transurethral resection for patients with primary urothelial nonmuscle invasive bladder cancer: a randomised controlled trial, Lancet Oncol. 12 (2011) 871–879. [62] S.M. Di Stasi, L. Storti, A. Giurioli, G. Zampa, E. Liberati, M. Sciarra, B. Iorio, R.L. Stephen, Carcinoma in situ of the bladder: long-term results of a randomized prospective study comparing intravesical electromotive mitomycin-C, passive diffusion mitomycin-C and Bacillus Calmette-Guerin, Eur. Urol. Suppl. 7 (2008) 180. [63] S.M. Di Stasi, C. Riedl, Updates in intravesical electromotive drug administration of mitomycin-C for non-muscle invasive bladder cancer, World J. Urol. 27 (2009) 325–330. [64] C. Gan, S. Amery, K. Chatterton, M.S. Khan, K. Thomas, T. O'Brien, Sequential bacillus Calmette-Guérin/electromotive drug Administration of Mitomycin C as the standard Intravesical regimen in high risk nonmuscle invasive bladder cancer: 2year outcomes, J. Urol. 195 (2016) 1697–1703. [65] Y.A. Yousef, S.E. Soliman, P.P. Astudillo, P. Durairaj, H. Dimaras, H.S. Chan, E. Héon, B.L. Gallie, F. Shaikh, Intra-arterial chemotherapy for retinoblastoma: a systematic review, JAMA Ophthalmol. 134 (2016) 584–591. [66] P. Temming, M. Arendt, A. Viehmann, L. Eisele, C.H. Le Guin, M.M. Schündeln, E. Biewald, K. Astrahantseff, R. Wieland, N. Bornfeld, W. Sauerwein, A. Eggert, K.H. Jöckel, D.R. Lohmann, Incidence of second cancers after radiotherapy and systemic chemotherapy in heritable retinoblastoma survivors: a report from the German reference center, Pediatr. Blood Cancer 64 (2017) 71–80. [67] B. Hayden, M.E. Jockovich, T.G. Murray, M.T. Kralinger, M. Voigt, E. Hernandez, W. Feuer, J.M. Parel, Iontophoretic delivery of carboplatin in a murine model of retinoblastoma, Invest. Ophthalmol. Vis. Sci. 47 (2006) 3717–3721. [68] B.C. Hayden, M.E. Jockovich, T.G. Murray, M. Voigt, P. Milne, M. Kralinger, W.J. Feuer, E. Hernandez, J.M. Parel, Pharmacokinetics of systemic versus focal carboplatin chemotherapy in the rabbit eye: possible implication in the treatment of retinoblastoma, Invest. Ophthalmol. Vis. Sci. 45 (2004) 3644–3649. [69] E. Eljarrat-Binstock, A.J. Domb, F. Orucov, A. Dagan, J. Frucht-Pery, J. Pe'Er, In vitro and in vivo evaluation of carboplatin delivery to the eye using hydrogeliontophoresis, Curr. Eye Res. 33 (2008) 269–275. [70] J.D. Byrne, M.R. Jajja, A.T. O'Neill, A.N. Schorzman, A.W. Keeler, J.C. Luft, W.C. Zamboni, J.M. Desimone, J.J. Yeh, Impact of formulation on the iontophoretic delivery of the FOLFIRINOX regimen for the treatment of pancreatic cancer, Cancer Chemo. Pharm. 81 (2018) 991–998. [71] J.D. Byrne, M.R. Jajja, A.N. Schorzman, A.W. Keeler, J.C. Luft, W.C. Zamboni, J.M. DeSimone, J.J. Yeh, Iontophoretic device delivery for the localized treatment of pancreatic ductal adenocarcinoma, Proc. Natl. Acad. Sci. U. S. A. 113 (2016) 2200–2205. [72] J. Wheler, J.J. Lee, R. Kurzrock, Unique molecular landscapes in cancer: implications for individualized, curated drug combinations, Cancer Res. 74 (2014) 7181–7184. [73] J. Cázares-Delgadillo, A. Ganem-Rondero, V. Merino, Y.N. Kalia, Controlled transdermal iontophoresis for poly-pharmacotherapy: simultaneous delivery of granisetron, metoclopramide and dexamethasone sodium phosphate in vitro and in vivo, Eur. J. Pharm. Sci. 85 (2016) 31–38. [74] T. Gratieri, Y.N. Kalia, Targeted local simultaneous iontophoresis of chemotherapeutics for topical therapy of head and neck cancers, Int. J. Pharm. 460 (2014) 24–27. [75] M. Manohar, A.K. Verma, S.U. Venkateshaiah, N.L. Sanders, A. Mishra, Pathogenic mechanisms of pancreatitis, World J Gastrointest Pharmacol Ther. 8 (2017) 10–25. [76] R.H. Guy, Y.N. Kalia, M.B. Delgado-Charro, V. Merino, A. Lopez, D. Marro, Iontophoresis: electrorepulsion and electroosmosis, J. Control. Release 64 (2000) 129–132. [27] J. Hirvonen, Y.N. Kalia, R.H. Guy, Transdermal delivery of peptides by iontophoresis: structure, mechanism and feasibility, Nat. Biotechnol. 14 (1996) 1710–1713. [28] M. Roustit, S. Blaise, J.L. Cracowski, Trials and tribulations of skin iontophoresis in therapeutics, Br. J. Clin. Pharmacol. 77 (2014) 63–71. [29] J.Y. Fang, C.F. Hung, Y.P. Fang, T.F. Chan, Transdermal iontophoresis of 5-fluorouracil combined with electroporation and laser treatment, Int. J. Pharm. 270 (2004) 241–249. [30] M.L. Welch, W.J. Grabski, M.L. McCollough, H.G. Skelton, K.J. Smith, P.A. Menon, L.L. Anderson, 5-fluorouracil iontophoretic therapy for Bowen's disease, J. Am. Acad. Dermatol. 36 (1997) 956–958. [31] N.S. Chandrashekar, R.H. Shobha Rani, Microprocessor-controlled iontophoretic drug delivery of 5-fluorouracil: pharmacodynamic and pharmacokinetic study, J. BUON 12 (2007) 529–534. [32] B.K. Chang, T.H. Guthrie Jr., K. Hayakawa, L.P. Gangarosa Sr., A pilot study of iontophoretic cisplatin chemotherapy of basal and squamous cell carcinomas of the skin, Arch. Dermatol. 129 (1993) 425–427. [33] T.R. Bacro, E.B. Holladay, M.J. Stith, J.C. Maize, C.M. Smith, Iontophoresis treatment of basal cell carcinoma with cisplatin: a case report, Cancer Detect. Prev. 24 (2000) 610–619. [34] T. Tsuji, Bleomycin iontophoresis therapy for verrucous carcinoma, Arch. Dermatol. 127 (1991) 973–975. [35] K.J. Smith, J.L. Konzelman, F.A. Lombardo, H.G. Skelton 3rd, T.T. Holland, J. Yeager, K.F. Wagner, C.N. Oster, R. Chung, Iontophoresis of vinblastine into normal skin and for treatment of Kaposi's sarcoma in human immunodeficiency virus-positive patients. The Military Medical Consortium for Applied Retroviral Research, Arch. Dermatol. 128 (1992) 1365–1370. [36] M.N. Luxenberg, T.H. Guthrie Jr., Chemotherapy of eyelid and peritorbital tumors, Trans. Am. Ophthalmol. Soc. 83 (1985) 162–180. [37] M.N. Luxenberg, T.H. Guthrie Jr., Chemotherapy of basal cell and squamous cell carcinoma of the eyelids and periorbital tissues, Ophthalmology 93 (1986) 504–510. [38] S.F. Taveira, A. Nomizo, R.F. Lopez, Effect of the iontophoresis of a chitosan gel on doxorubicin skin penetration and cytotoxicity, J. Control. Release 134 (2009) 35–40. [39] S.F. Taveira, D.C. De Santana, L.M. Araújo, F. Marquele-Oliveira, A. Nomizo, R.F. Lopez, Effect of iontophoresis on topical delivery of doxorubicin-loaded solid lipid nanoparticles, J. Biomed. Nanotechnol. 10 (2014) 1382–1390. [40] L.A. Huber, T.A. Pereira, D.N. Ramos, L.C. Rezende, F.S. Emery, L.M. Sobral, A.M. Leopoldino, R.F. Lopez, Topical skin cancer therapy using doxorubicin-loaded cationic lipid nanoparticles and iontophoresis, J. Biomed. Nanotechnol. 11 (2015) 1975–1988. [41] R.F. Lopez, M.V. Bentley, M.B. Delgado-Charro, R.H. Guy, Iontophoretic delivery of 5-aminolevulinic acid (ALA): effect of pH, Pharm. Res. 18 (2001) 311–315. [42] R.F. Lopez, M.V. Bentley, M. Begoña Delgado-Charro, R.H. Guy, Optimization of aminolevulinic acid delivery by iontophoresis, J. Control. Release 88 (2003) 65–70. [43] R.F. Lopez, M.V. Bentley, M.B. Delgado-Charro, D. Salomon, H. van den Bergh, N. Lange, R.H. Guy, Enhanced delivery of 5-aminolevulinic acid esters by iontophoresis in vitro, Photochem. Photobiol. 77 (2003) 304–308. [44] N. Merclin, T. Bramer, K. Edsman, Iontophoretic delivery of 5-aminolevulinic acid and its methyl ester using a carbopol gel as vehicle, J. Control. Release 98 (2004) 57–65. [45] H.E. Bodde, P.E.H. Roemele, W.M. Star, Quantification of topically delivered 5aminolevulinic acid by iontophoresis across ex vivo human stratum corneum, Photochem. Photobiol. 75 (2002) 418–423. [46] J.Y. Fang, W.R. Lee, S.C. Shen, Y.P. Fang, C.H. Hu, Enhancement of topical 5aminolaevulinic acid delivery by erbium:YAG laser and microdermabrasion: a comparison with iontophoresis and electroporation, Br. J. Dermatol. 151 (2004) 132–140. [47] M. Toyoda, S. Hama, Y. Ikeda, Y. Nagasaki, K. Kogure, Anti-cancer vaccination by transdermal delivery of antigen peptide-loaded nanogels via iontophoresis, Int. J. Pharm. 483 (2015) 110–114. [48] K. Kigasawa, K. Kajimoto, T. Nakamura, S. Hama, K. Kanamura, H. Harashima, K. Kogure, Noninvasive and efficient transdermal delivery of CpG-oligodeoxynucleotide for cancer immunotherapy, J. Control. Release 150 (2011) 256–265. [49] V.V. Vlassov, M.V. Nechaeva, V.N. Karamyshev, L.A. Yakubov, Iontophoretic delivery of oligonucleotide derivatives into mouse tumor, Antisense Res. Dev. 4 (1994) 291–293. [50] V.V. Venuganti, M. Saraswathy, C. Dwivedi, R.S. Kaushik, O.P. Perumal, Topical gene silencing by iontophoretic delivery of an antisense oligonucleotide-dendrimer nanocomplex: the proof of concept in a skin cancer mouse model, Nano 7 (2015) 3903–3914. [51] V. Stearns, T. Mori, L.K. Jacobs, N.F. Khouri, E. Gabrielson, T. Yoshida, S.L. Kominsky, D.L. Huso, S. Jeter, P. Powers, K. Tarpinian, R.J. Brown, J.R. Lange, M.A. Rudek, Z. Zhang, T.N. Tsangaris, S. Sukumar, Preclinical and clinical evaluation of intraductally administered agents in early breast cancer, Sci Transl. Med. 26 (2011) 106ra108. [52] M. Komuro, K. Suzuki, M. Kanebako, T. Kawahara, T. Otoi, K. Kitazato, T. Inagi, K. Makino, M. Toi, H. Terada, Novel iontophoretic administration method for local therapy of breast cancer, J. Control. Release 168 (2013) 298–306. [53] T. Gürpinar, L.D. Truong, H.Y. Wong, D.P. Griffith, Electromotive drug administration to the urinary bladder: an animal model and preliminary results, J. Urol. 156 151