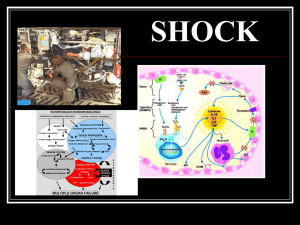
Shock in the ICU Definition: circulatory failure that results in inadequate cellular oxygen utilization. Features: Definition and Features • First: systemic arterial hypotension (systolic below 90 and mean below 70) with Tachycardia (Pulse rate above 100 • Second: signs of tissue hypoperfusion, which are apparent through the three “windows” of the body: • Cutaneous: skin is cold and clammy, with vasoconstriction and cyanosis. • Renal: urine output of <0.5 ml per kilogram of body weight per hour • Neurologic: altered mental state, which typically includes obtundation, disorientation, and confusion. • Third: hyperlactatemia indicating abnormal cellular oxygen metabolism. The normal blood lactate level 1 mmol per liter, increased (>1.5 mmol per liter) in acute circulatory failure. Four potential (Non-Exclusive), pathophysiological mechanisms: hypovolemia (from internal or external fluid loss), cardiogenic factors (e.g., acute myocardial infarction, endstage cardiomyopathy, advanced valvular heart disease, myocarditis, or cardiac arrhythmias), Classification: obstruction (e.g., pulmonary embolism, cardiac tamponade, or tension pneumothorax), or distributive factors (e.g., severe sepsis or anaphylaxis from the release of inflammatory mediators). Nonexclusive means combination: Example: Hypovolemic shock due to trauma and hemorrhage may be associated with spinal shock (distributive) or cardiac tamponade (obstructive). Septic shock (distributive) with cardiac depression (cardiogenic)…..etc Type of shock Schemic Representat ion of the four types of shock The most common in ICU is septic shock (distributive) followed by cardiogenic and hypovolemic. Obstructive is rare. Diagnosis The type and cause of shock may be obvious from: the medical history, physical examination. or clinical investigations. Point-of-care echocardiographic evaluation: Assessment for pericardial effusion. Measurement of left and right ventricular size and function. Assessment for respiratory variations in vena cava dimension. Calculation of the aortic velocity–time integral (measures of stroke volume) Initial Assessment Initial Approach: Resuscitation should be started even while investigation of the cause Iis ongoing. Identify the cause and correct rapidly examples: ◦ ◦ ◦ ◦ control of bleeding, percutaneous coronary intervention for coronary syndromes thrombolysis or embolectomy for massive pulmonary embolism, administration of antibiotics and source control for septic shock). Gadgets: ◦ arterial catheter to monitor arterial blood pressure and blood sampling. ◦ a central venous catheter for the infusion of fluids and vasoactive agents and to guide fluid therapy. Since the goal of management of shock is the same (achieve adequate tissue perfusion regardless of the case) management is similar and should be problem oriented although the exact treatments that are used to reach those goals may differ. A useful mnemonic (memory aid) to describe the important components of resuscitation is the VIP rule: V: ventilation (oxygen administration) I: infusion (fluid resuscitation) P: pump (administration of vasoactive agents). oxygen should be started immediately to increase oxygen delivery and prevent pulmonary hypertension. Pulse oximetry unreliable (Peripheral vasoconstriction) Blood gas monitoring (ABG). Ventilatory Support: • Mechanical ventilation with endotracheal intubation • patients with severe dyspnea, • hypoxemia, • or persistent or worsening acidemia (pH, <7.30). Invasive mechanical Additional benefits • of reducing the oxygen demand of respiratory muscles. • decreasing left ventricular afterload by increasing intrathoracic pressure. An abrupt decrease in arterial pressure after the initiation of invasive mechanical ventilation strongly suggests hypovolemia and a decrease in venous return. Sedative agents should be kept to a minimum to avoid further decreases in arterial pressure and cardiac output. Infusion (fluid resuscitation): Fluid challenge observe four elements in advance: ◦ First, the type of fluid: Crystalloid solutions are the first choice followed by Albumin. ◦ Second, the rate of fluid administration Fluids should be infused rapidly to induce a quick response typically, an infusion of 300 to 500 ml of fluid during a period of 20 to 30 minutes. ◦ Third, the objective of the fluid challenge must be defined. In shock, the objective is usually an increase in systemic arterial pressure, ◦ Fourth the safety limits must be defined. Pulmonary edema is the most serious complication of fluid infusion. Central venous pressure of a few millimeters of mercury above the baseline value is usually set to prevent fluid overload (not always accurate). Fluid challenges can be repeated as required but must be stopped rapidly in case of nonresponse in order to avoid fluid overload. Adrenergic agents (adrenergic agonists): Pump (administration of vasoactive agents): β-adrenergic: increase blood flow but also increases the risk of myocardial ischemia as a result of increased heart rate and contractility e.g. isoproterenol (only in bradycardia). α-adrenergic increase vascular tone and blood pressure but can also decrease cardiac output and impair tissue blood flow, especially in the hepatosplanchnic region for this reason, phenylephrine, an almost pure α-adrenergic agent, is rarely indicated. Norepinephrine to be the vasopressor of first choice; it has predominantlyαadrenergic properties, but its modest β-adrenergic effects help to maintain cardiac output. Administration generally results in a clinically significant increase in mean arterial pressure, with little change in heart rate or cardiac output. The usual dose is 0.1 to 2.0 μg per kilogram of body weight per minute. 01 02 03 04 Dopamine has predominantly βadrenergic effects at lower doses and α-adrenergic effects at higher doses: very low doses (<3 μg perkilogram per minute, given intravenously) may selectively dilate the hepatosplanchnic and renal circulations, but controlled trials have not shown a protective effect on renal function,14 and its routine use for this purpose is no longer recommended. undesired endocrine effects on the hypothalamic–pituitary system, resulting in immunosuppression, primarily through a reduction inthe release of prolactin. In a recent randomized, controlled, double blind trial, dopamine had no advantage over norepinephrineas the first-line vasopressor agent; moreover, it induced more arrhythmias and was associated with an increased 28-day rate of death among patients with cardiogenic shock.. / Dopamine: Others: Epinephrine, which is a stronger agent, has predominantly βadrenergic effects at low doses, with α-adrenergic effects becoming more clinically significant at higher doses. However, epinephrine administration can be associated with an increased rate of Arrhythmia. Reserve for refractory cases. Vasopressin: deficiency can develop in patients with very hyperkinetic forms of distributive shock, low-dose vasopressin may result in substantial increases in arterial pressure. Dobutamine: predominantly β-adrenergic properties. Inotropic cardiac support. Increase cardiac output. Arterial blood pressure: Mean arterial pressure of 65 to 70 to achieve adequate tissue perfusion (skin, metal status, urine output). Oxygen Delivery, SvO2 and ScvO2. Goals and Monitoring of Hemodynamic support: Lactate to Guide Treatment of Shock: • Lactate is produced during tissue hypoxemia and hypoperfusion. • In cardiogenic and hypovolemic shock, lactate rises as tissue hypoxemia results in increased anaerobic metabolism. • In distributive (usually septic) shock, mechanisms other than pure tissue ischemia (anaerobic metabolism) may contribute to elevated lactate levels. • Impaired liver function (either pre-existing or due to shock) may reduce lactate clearance in any patient with shock, resulting in persistently high lactate values even after perfusion is restored and lactate production normalizes. Microcirculatory Variables. Side stream Dark-Field Image of Sublingual Microcirculation in Healthy Volunteer and Patient with Septic Shock handheld devices for orthogonal polarization spectral (OPS) imaging and its successor, sidestream dark-field (SDF) The four phase of shock treatment: First (salvage) phase, ◦ the goal of therapy is to achieve a minimum blood pressure and cardiac output compatible with immediate survival. ◦ Minimal monitoring is needed; arterial and central venous catheters. ◦ Lifesaving procedures to treat cause (e.g., surgery for trauma, pericardial drainage, revascularization for acute myocardial infarction, and antibiotics for sepsis) Second (optimization)phase: ◦ The goal is to increase cellular oxygen availability ◦ Adequate hemodynamic resuscitation. ◦ Measurements of SvO2 and lactate guide therapy and monitoring of cardiac output cardiac output should be considered. Third (stabilization) phase: ◦ the goal is to prevent organ dysfunction, ◦ Oxygen supply to the tissues is no longer the key problem, and organ support becomes more relevant. Fourth (de-scalation) phase: ◦ the goal is to wean the patient from vasoactive agents ◦ promote spontaneous polyuria or provoke fluid elimination using diuretics or ultrafiltration to achieve a negative fluid balance. Circulatory shock is associated with high morbidity and mortality. Appropriate treatment is based on a good understanding of the underlying pathophysiological mechanisms. Treatment should include correction of the cause of shock and hemodynamic stabilization, primarily through fluid infusion and administration of vasoactive agents. Conclusion: The patient’s response can be monitored by means of careful clinical evaluation and blood lactate measurements; microvascular evaluation may be feasible in the future. Hemorrhagic Shock Definition and Causes hypovolemic shock. (examples: of Hypovolemic non-Hemorrhagic) ? inadequate oxygen delivery at the cellular level. Death quickly follows if bleeding not stopped (2 million/year/globally)! Common causes: ◦ ◦ ◦ ◦ ◦ Trauma ( Death 1.5 million annually) maternal hemorrhage. gastrointestinal hemorrhage. Rupture Aortic Aneurysm. Perioperative hemorrhage Oxygen delivery is insufficient. Cells transition to anaerobic metabolism. Lactic acid, inorganic phosphates, Oxygen debt . Accumulation of lactic acid, Inorganic phosphate free radicles. Release of damageassociated molecular patterns (known as DAMPs or alarmins) leads to systemic inflammation. ATP deficiency leads to failure of homeostasis, membranes disruption Necrosis and celldeath Shock at Cellular level: Shock at Tissue level hypovolemia and vasoconstriction cause hypoperfusion. End-organ damage in the kidneys, liver, intestine, and skeletal muscle and multiorgan failure in survivors. Extreme hemorrhage (exsanguination) pulselessness results in hypoperfusion of the brain and myocardium: ◦ cerebral anoxia ◦ fatal arrhythmias within minutes. Blood vessels: ◦ Endotheliopathy systemic shedding of the protective glycocalyx barrier. ◦ Clot formation at the site of injury and fibrinolysis at distant area (plasminogen activation and glycocalyx shedding . ◦ Profound coagulopathy , plantlets dysfunction and loss. Iatrogenic factors. Management….1: Pre-hospital: ◦ Pressure, Tourniquet, hemostatic dressing. ◦ Large pore IV administration (minimal to keep palpable pulse and patient awake) ◦ Avoid dilutional coagulopathy. Rapid transport to Hospital. Dx: ◦ s/s subtle. ◦ BP low when loss of more than 30%. ◦ anxiety, tachypnea, a weak peripheral pulse, and cool extremities with pale or mottled skin. Classification of Hemorrhagic Shock Management…2: Initial Evaluation: ◦ ◦ ◦ ◦ Source…Hidden or obvious….Intracavity in trauma (chest, abdomen and pelvis) Radiograph and US (pelvis chest and abdomen) Blood gas and lactate CBC, INR and Electrolytes. Resuscitation: ◦ Find and control source of bleeding ◦ Restore intravascular volume Management…3: Transfusion: Massive-transfusion protocols mobilize universal donor blood products (e.g., packed red cells, plasma, platelets, and cryoprecipitate) to the patient’s bedside in prespecified ratios (1:1:1 (i.e., 6 units of plasma and 1 unit of apheresis platelets [equivalent to approximately 6 units of pooled platelets] for every 6 units of red cells) 1 g of intravenous calcium chloride after transfusion of the first 4 units of any blood product) limiting crystalloid infusions to 3 liters in the first 6 hours after arrival at the hospital Phramcology: many …factors VII ?? Tranexamic acid Management ….4: Achieving definitive hemostasis: ◦ ◦ ◦ ◦ ◦ ◦ ◦ Acute torso trauma… less than 10 minutes in ER. Limbs….Tourniquet…… OR Priorities the site of severe bleeding. GI bleed…. Endoscopy. Endovascular occlusion: resuscitative endovascular balloon occlusion of the aorta (REBOA). assessed for evidence of: ◦ ongoing hemorrhage, ◦ unpaid oxygendebt, ◦ anemia, coagulopathy, ◦ electrolyte derangements, ◦ other sequelae of over- or under-resuscitation Damage Control Resuscitation Septic Shock Warm and Cold Shock Definitions: Sepsis: systemic inflammatory response to infection. Severe Sepsis: when sepsis is complicated by acute organ dysfunction. Septic Shock: sepsis complicated by either hypotension that is refractory to fluid resuscitation or by hyperlactatemia. Organ dysfunction: need for supportive therapy (mechanical ventilation, dialysis….) Incidence: 2% of all hospital admissions and 10% of ICU admission, ¾ million per year in USA, 19 million per year worldwide. Mortality : 80% 30 years ago now 20-30%. Etiology: Community acquired (pneumonia) or Hospital acquired. Pneumonia, abdominal sepsis and UTI. Blood culture positive in only 1/3 of cases. In 1/3 culture from all sites are negative. Causative organism: ◦ Gram negative in 62% ◦ Gram positive in 47% ◦ Fungi in 19% Predisposing factors: Age, sex, chronic disease, immunological status and genetics Clinical features: General Variables. Fever (core temperature, >38.3°C) Hypothermia (core temperature, <36°C) Elevated heart rate (>90 beats per min or >2 SD above the upper limit of the normal range for age) Tachypnea Altered mental status Substantial edema or positive fluid balance (>20 ml/kg of body weight over a 24-hr period) Hyperglycemia (plasma glucose, >120 mg/dl [6.7 mmol/liter]) in the absence of diabetes Clinical Features: Inflammatory Variable Leukocytosis (white-cell count, >12,000/mm3) Leukopenia (white-cell count, <4000/mm3) Normal white-cell count with >10% immature forms Elevated plasma C-reactive protein (>2 SD above the upper limit of the normal range) Elevated plasma procalcitonin (>2 SD above the upper limit of the normal range) Clinical features: Organ dysfunction variables. Arterial hypoxemia (ratio of the partial pressure of arterial oxygen to the fraction of inspired oxygen, <300) Acute oliguria (urine output, <0.5 ml/kg/hr or 45 ml/hr for at least 2 hr) Paralytic ileus (absence of bowel sounds) Increase in creatinine level of >0.5 mg/dl (>44 μmol/liter) Thrombocytopenia (platelet count, <100,000/mm3) Coagulation abnormalities (international normalized ratio, >1.5; or activated partial-thromboplastin time, >60 sec) Hyperbilirubinemia (plasma total bilirubin, >4 mg/dl [68 μmol/liter]) Clinical Features: Tissue perfusion Variables. Hyperlactatemia (lactate, >1 mmol/liter) Decreased capillary refill or mottling Severe sepsis (sepsis plus organ dysfunction) Septic shock (sepsis plus either hypotension [refractory to intravenous fluids] or hyperlactatemia) Acute organ dysfunction: Respiratory: acute respiratory distress syndrome (ARDS) defined as hypoxemia with bilateral infiltrates of noncardiac origin. Cardiovascular: hypotension or an elevated serum lactate level after adequate volume expansion, requiring the use of vasopressors’ myocardial dysfunction. Brain: obtundation or delirium. Kidney: Acute kidney injury, decreasing urine output, increasing serum creatinine level , may requires treatment with renal-replacement therapy. Others: Paralytic ileus, elevated aminotransferase levels, altered glycemic control, thrombocytopenia and disseminated intravascular coagulation,adrenal dysfunction, and the euthyroid sick syndrome Guidelines are organized into two “bundles” of care: Initial management: • initial management bundle to be accomplished within 6 hours • management bundle to be accomplished in the ICU. • Resuscitation: fluid and vasoactive agents and respiratory therapy. / • Forming probable Dx, culture, drainage and Antibiotic therapy. Treatment: ICU management: • monitoring and support of organ function, • avoidance of complications, • de-escalation of care when possible.