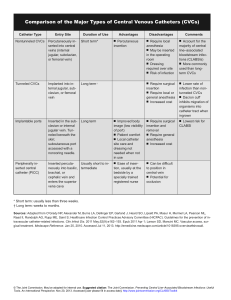
Basic Intravenous Therapy 90-95% of patients in the hospital receive some type of intravenous therapy. This presentation will enhance your knowledge of how to care for them. Previous Next Vein Anatomy and Physiology Veins are unlike arteries in that they are 1)superficial, 2) display dark red blood at skin surface and 3) have no pulsation Vein Anatomy - Tunica Adventitia - Tunica Media - Tunica Intima - Valves Previous Next Tunica Adventitia the outer layer of the vessel Connective tissue Contains the arteries and veins supplying blood to vessel wall Previous Next Tunica Media the middle layer of the vessel Contains nerve endings and muscle fibers The vasoconstrictive response occurs at this layer Previous Next Tunica Intima the inner layer of the vessel One No layer of endothelials nerve endings Surface for platelet aggregation w/trauma and recognition of foreign object at this level PHLEBITIS Previous begins here Next Valves present in MOST veins Prevent backflow and pooling More in lower extremities and longer vessels Vein dilates at valve attachment Previous Next Veins of the Upper Extremities Digital Vessels -Along lateral aspects fingers, infiltrate easily, painful, difficult to immobilize and should be your LAST RESORT Metacarpal Vessels -Located between joints and metacarpal bones (act as natural splint) Digital -Formed by union of digital veins -Geriatric patients often lack enough connective / adipose tissue and skin turgor to use this area successfully Previous Next Veins of the Upper Extremities Cephalic (Intern’s Vein) -Starts at radial aspect of wrist -Access anywhere along entire length (BEWARE of radial artery/nerve) Medial Cephalic (“On ramp” to Cephalic Vein) -Joins the Cephalic below the elbow bend -Accepts larger gauge catheters, but may be a difficult angle to hit and maintain Previous Next Veins of the Upper Extremities Basilic - Originates from the ulner side of the metacarpal veins and runs along the medial aspect of the arm. It is often overlooked becauses of its location on the “back” of the arm, but flexing the elbow/bending the arm brings this vein into view Medial Basilic - Empties into the Basilic vein running parallel to tendons, so it is not always well defined. Accepts larger gauge catheters. - BEWARE of Brachial Artery/Nerve Previous Next Purposes of IV Therapy To provide parenteral nutrition To provide avenue for dialysis/apheresis To transfuse blood products To provide avenue for hemodynamic monitoring To provide avenue for diagnostic testing To administer fluids and medications with the ability to rapidly/accurately change blood concentration levels by either continuous, intermittent or IV push method. Types of Peripheral Venous Access Devices •Butterfly (winged) or Scalp vein needles (SVN) – not recommended for non compliant patient as it can easily penetrate the vein wall causing extravasation. We use these frequently for phlebotomy •Safety Over the needle catheters (ONC) - PROTECTIV ® Previous -ACUVANCE ® Next Starting a Peripheral IV Finding a vein can be challenging - Go by “feel”, not by sight. Good veins are bouncy to the touch, but are not always visible. - Use warm compresses and allow the arm to hang dependently to fill veins. - A BP cuff inflated to 10mmHg below the known systolic pressure creates the perfect tourniquet. Arterial flow continues with maximum venous constriction. - If the patient is NOT allergic to latex, using a latex tourniquet may provide better venous congestion - Avoid areas of joint flexion - Start distally and use the shortest length/smallest gauge access device that will properly administer the prescribed therapy Previous (BE AWARE: Blood flow in the lower forearm and hand is 95ml/min) Next IV Start Pain Management One of the most frequent contributors to patient dissatisfaction is painful phlebotomy and IV starts • Use 25-27g insulin syringe to create a wheal similar to a TB skin test on top of or just to side of vein with 0.1 -0.2 ml normal saline or 1% xylocaine without epinephrine • Topical anesthesia cream (ie EMLA) may be applied to children>37 weeks gestation 1 hr. prior to stick. It might be a good idea to anesthetize a couple of sites • Have the patient close their fist (NO PUMPING) prior to stick • Make sure the skin surface cleansing agent (alcohol/chlorhexidine) is dry prior to stick. Drawing this into the vein may stimulate the vasoconstrictive action of the tunica media layer Previous Next Flushing Peripheral IV’s Use prefilled saline and heparin flush syringes located in PYXIS Heparin flush concentrations available: -100u/ml (5ml in a 10ml syringe) -10u/ml (2ml in a 3ml syringe) Flushing intervals and amounts - Peds: q 6hrs. <22ga 1ml 0.9%NS followed by 1ml heparinized (10units/ml) saline - Adults: q 8hrs w/1ml. 0.9%NS [3ml heparinized saline for OB] Previous Next Dressing/Bag Changes Physician orders are required if a peripheral catheter is left in the same site for more than 3 days. It is best to have the pharmacy add medications to the infusion bags under laminare flow to reduce contamination Previous Next Central Venous Catheters Percutaneous Tunneled PICC’s Implanted Ports Dialysis Insertion MD @ bedside w/xray confirmation MD in OR under fluoroscopy MD/trained RN @bedside w/x-ray confirmation MD in OR under fluoroscopy MD in OR under fluoroscopy Location Visible externally. Enters subclavian, ext. juglar,or int. juglar vein near clavicular area Visible ext. usually midway bet. clavicle and nipple. Tunneled under skin & threaded through subclavian or IJ Visible externally around antecubital fossa, upper arm or neck Completely internal. Titanium or plastc port is implanted in a surgically created pocket and catheter is threaded into subclavian or int. juglar vein. Access is through skin into self sealing port using special non coring needle Visible externally. Arm or leg placement Polyurethane $200-$400 Silicone $3500-$5000 Silicone / polyurethane $350-$500 Silicone catheter. Port is titanium or plastic w/self sealing diaphragm $3500-$5000 Various materials Lumen 2-3 2-3 1-2 1-2 2-3 Sutured Yes/entire life Yes, until internal Dacron cuff healed No Yes Yes Duration Short term 4-10 days Long term Long term Long term Mid term Flushes 5-10ml NaCl after use and daily 5-10ml NaCl after use and daily 5-10ml NaCl after use and daily 10ml NaCl followed by 4.5ml heparinized saline (adults-100units/ml; peds-10units/ml) after ea. use or monthly if not accessed Done ONLY by IV team or dialysis nurses Brands/ Names Arrow Howe, Triple Lumen, Subclavian, IJ Hickman, Broviac PICC, PIC, EDPC, Arrow Howe, Gesco, PASV Bard, Accces Port-A-Cath Bard, Tesio, Vescath, Quinton MD or speically trained RN @ bedside MD in OR Specially trained RN @ bedside MD in OR MD in OR Material/Cost Discontinue Previous Next Central Venous Catheter Sites Percutaneous(Subclavian) PICC (Peripherally inserted Central Catheter) Implanted Port (single or double lumen) Tunnelled (Hickman) Previous Percutaneous (IJ-Int. Jugular) Next CVC Care/Maintenance Percutaneous Tunneled Flush after each access or daily for catheters>21ga, q 6 hrs <21 ga -adults: 10ml saline - peds/neonates: 5ml saline (preservative free for infants <1yr) PICC Transparent dressing change q 7 days & prn Previous Next CVC Care/Maintenance Flush after each use and weekly while accessed; monthly when not acessed - 10ml saline (preservative free for pts. <1yr) Implanted Port - followed by 4.5ml-5ml heparinized saline 100units/ml for adults 10units/ml for peds Transparent dressing/ access needle change q 7days Previous Next Monitor and document site condition: Site Care • Hourly for peds •Q 2 hr for adult * Indicates complication: •Infiltration •Phlebitis •Thrombosis •Cellulitis •Septicemia Previous Next Infiltration/Extravasation The most common cause is damage to the wall during insertion or angle of placement. STOP INFUSION and treat as indicated by Pharmacy, Medication package insert or drug reference book. Notify MD and document Previous Next Phlebitis/Thrombophlebitis Chemical - Infusate chemically erodes internal layers. Warm compresses may help while the infusate is stopped/changed. Anti-inflammatory and analgesic medications are often used no matter what the cause Mechanical Bacterial - Caused by irritation to internal lumen of vein during insertion of vascular access device and usually appears shortly after insertion. The device may need to be removed and warm compresses applied - Caused by introduction of bacteria into the vein. Remove the device immediately and treat w/antibiotics. The arm will be painful, red and warm; edema may accompany Previous Next Cellulitis Inflammation of loose connective tissue around insertion site. - Caused by poor insertion technique - Red swollen area spreads from insertion site outwardly in a diffuse circular pattern - Treated w/antibiotics Previous Next Septicemia/Pulmonary Edema/ Embolism Septicemia - Severe infection that occurs to a system or entire body - Most often caused by poor insertion technique or poor site care - Discontinue device immediately, culture and treat appropriately Pulmonary edema- caused by rapid infusion Pulmonary embolism - Caused by any free floating substances that require thrombolytic therapy for several months. Increased risk w/lower ext. Air embolism- caused by air injected into IV system. Keep insertion site below level of heart Previous Next Troubleshooting Vascular access device will not flush/can’t draw blood - Evaluate for kink in tubing or catheter tip against vein wall. Vascular access device (VAD) leaking when flushed - Verify that hub access cap is connected correctly Patient complains of pain while VAD being flushed - Assess for infiltration VAD broken - PICC’s may be repaired. All other devices must be replaced Call IV therapy team member for any concerns or questions. Previous Next Policy notes KVO rate: RN’s and LPN’s can start peripheral IV’s after initial training and observation by preceptor Adults - 10 ml/hr Pediatrics - 2-3 ml/hr Neonates - 0.5-1 ml/hr Only until rate order received Verification required for: •Insulin •Heparin •Potassium LPN’s CANNOT infuse blood products or high risk IV medications. Previous •Digoxin •Chemotherapy LPN’s cannot push IV medications Next IV Medication Administration Many medications require patient monitoring that cannot be done on units where the nurse/patient ratios are greater than 1:2 A patient can be moved to a unit where the ratio is appropriate for invasive/frequent monitoring or another nurse can be brought to care for the patient during the med administration Previous All Medications Cannot Be Administered on All Units General Care Units: Can give meds requiring only basic physical assessment data Stepdown Units: Can give meds that require more invasive or frequent monitoring than is available on general care units Intensive Care Units: Can give meds that require more invasive or frequent monitoring than is available on the Stepdown units. VANDERBILT URL LINK FOR IV MEDICATIONS: www.mc.vanderbilt.edu/pharmacy/ivroom/IV MedAdm061003.pdf Next IV Medication Administration Sample page from the Pharmacy med administration web site See “APPROVED FOR” section. You will find if the medication can be administered on your unit. Previous Next www.ins1.org Infusion Nurses Society (INS) Previous Professional Organization that sets the standards of care for clinicians practicing in the field of infusion therapy. Standards set by INS are reflected in our policies and procedures related to infusion therapy for health care providers. In a court of law, the standards set by the INS are used to assess the infusion clinician’s performance. Next