SBIRT Training
Pam Pietruszewski
The National Council for Behavioral Health
April 2016
What is SBIRT?
• Screening to identify patients at-risk for developing
substance use disorders.
• Brief Intervention to raise awareness of risks, elicit
internal motivation for change, and help set healthy
goals.
• Referral to Treatment to facilitate access to
specialized services and coordinate care between
systems for patients with highest risk.
2
Recommended by the American
Academy of Pediatrics
• Regards substance abuse as a pediatric
disorder
• First published a policy statement in 2011
• Published a paper in July 2016 updating its
statement
• Advocates the use of SBIRT in the varied
settings in which youth receive healthcare.
SBIRT Paradigm Shift
• Not looking for addiction
• Looking for individuals with unhealthy substance
use patterns
• Looking for opportunities for intervention
• Meeting people where they are
4
Video: Anti-SBIRT
Video: Effective SBIRT
SBIRT Work Flow
Screening
No Use
Low Risk
Reinforce
healthy
choices
CRAFFT Score 1 or >
Moderate Risk
High Risk
Brief Intervention
1-4 sessions
Brief Intervention AND
Referral to Treatment
Follow-up
Screening
A systematic way of identifying potential
for problems using a standardized,
reliable and valid tool
8
Brief Screen (Pre-Screen)
During the past 12 months, did you:
1. Drink any alcohol (more than a few sips)?
2. Smoke any marijuana or hashish?
3. Use anything else to get high?
If any “YES” ask full CRAFFT questions
If all “NO” just ask CAR question
9
“Healthy Lifestyle” Screening
Another Brief Screen (S2BI)
In the past year how many times have you used…
1.
2.
3.
4.
5.
6.
7.
8.
Tobacco products (including e-cigarettes or vaping)
Alcohol
Marijuana
Illegal drugs (such as cocaine or Ecstasy)
Prescription drugs not prescribed for you (such as pain medication or Adderall)
OTC medications (such as cough medicine) for non-medical reasons
Inhalants (such as nitrous oxide)
Herbs or synthetic drugs (such as salvia, K2 or bath salts)
If any “YES” ask full CRAFFT questions
If all “NO” just ask CAR question
No history of use History past year use History monthly use
History daily use
No Risk
Severe Risk
Mild Risk
Moderate Risk
Levy et al. JAMA Pediatr. 2014
Full Screen: CRAFFT
1. Have you ever ridden in a car driven by someone (including yourself)
who was “high” or had been using alcohol or drugs?
2. Do you ever use alcohol or drugs to relax, feel better about yourself, or
fit in?
3. Do you ever use alcohol or drugs while you are by yourself, or alone?
4. Do you ever forget things you did while using alcohol or drugs?
5. Do your family or friends ever tell you that you should cut down on your
drinking or drug use?
6. Have you ever gotten into trouble while you were using alcohol or
drugs?
12
CRAFFT Scoring
Low Risk
Moderate Risk
High Risk
Abstinence
CRAFFT Score 1
CRAFFT Score 2+
If 1+ provide brief intervention
If 2+ also consider referral to treatment.
Source: American Academy of Pediatrics, 2011
CRAFFT IS IN AWARDS
Screening is an Ongoing Process
ATTC Adolescent SBIRT Learner's Guide
Optional:
• Alcohol is the most commonly used drug among
youth in the United States. Excessive drinking is
responsible for more than 4,300 deaths among
underage youth each year and cost the U.S. $24
billion annually. In addition to the thousands of
deaths each year that result from underage
drinking, approximately 200,000 young people
visit an emergency room for alcohol related
injuries. Despite these staggering numbers, 2015
marked the lowest levels for alcohol use
recorded by government data among high school
youth. This strongly contradicts the common
refrains often heard that “all teenagers drink,” or
“it is a harmless rite of passage.”
National Institute on Alcohol Abuse and Alcoholism. Alcohol Screening
and Brief Intervention for Youth; A Practitioner's Guide. Rockville, MD:
National Institute on Alcohol Abuse and Alcoholism;2011.
Brief Intervention
15-30 minutes
Help clients to be aware
of their patterns of use,
understand the associated
risks and make their own
decisions.
Help patients to
accept more
intensive treatment
for those who might
benefit.
http://www.integration.samhsa.gov/clinical-practice/sbirt/brief-interventions
22
Brief Intervention
The Brief Negotiated Interview Format
1.
2.
3.
4.
Raise the subject
Provide feedback
Enhance motivation
Develop a plan
Brief Intervention
1.
2.
3.
4.
Raise the subject
Provide feedback
Enhance motivation
Develop a plan
National Survey on Drug Use and Health, SAMHSA
https://www.healthypeople.gov
https://www.healthypeople.gov
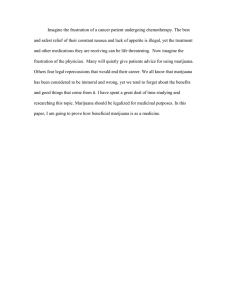
THC is at a historic high
(paranoia, hallucinations, anxiety)
< 4% in 1995
12% in 2014
Disapproval is at historic low
32% (lowest since 1975)
Addressing Marijuana Myths
SBIRT Colorado: www.healthteamworks.org
Marijuana is all natural
Marijuana may also contain harmful contaminants. Many natural
substances are known to harm human health.
Marijuana helps with stress and anxiety
It is important to identify underlying causes of stress and anxiety.
Explore alternatives to marijuana. Heavier users of marijuana may
experience improved mental clarity and motivation when they stop
using.
It’s legal. So why quit, or how could it be a problem?
Other legal substances such as tobacco, alcohol, and prescription
narcotics cause significant harm. Marijuana is associated with
serious, long-term negative health effects.
MI Sandwich Approach to Feedback
Elicit: What do you know about…
Advise: That’s partially correct…in
addition…
Elicit: What do you think? Where
does that leave you?
Brief Intervention
1.
2.
3.
4.
Raise the subject
Provide feedback
Enhance motivation
Develop a plan
Motivational interviewing is a
collaborative, person-centered, guiding
method designed to elicit and strengthen
motivation for change.
Miller & Rollnick, 2012
MI Spirit
Partnership
Evocation
Acceptance
Compassion
Motivational Interviewing for Adolescent Substance
Use: A Review of the Literature
Barnett, et al. Addict Behav 2012
“MI appears to be a good fit with adolescents’
developmental need to exert their independence
and make decisions for themselves, while it
respects their heightened levels of psychological
reactance and coincides with the development of
their decision-making skills.”
Some Motivational
Interviewing Principles
1. Motivation is not static.
2. Ambivalence is normal to the
change process.
3. Pushing too hard will evoke
resistance to change.
4. Evoking patient’s own change
talk will enhance behavior
change.
Ambivalence
Change
Talk
Sustain
Talk
Developing Discrepancy
“What are the good things about pot?
“What are the not so good things about
pot?”
Pros
Cons
Decisional Balance
Good
Not so good
No change
1
2
Change
4
3
Listening to Motivate Change
•
•
•
•
Open-Ended Inquiry
Affirmations
Reflections
Summarize
Open-Ended Inquiry
Instead of:
Try:
Do you get any exercise?
What activities do you enjoy?
Can you cut back?
How have you approached
changes in the past?
Attributes of Successful Changers
Accepting
Adaptable
Alert
Ambitious
Assertive
Brave
Careful
Committed
Considerate
Creative
Determined
Eager
Faithful
Flexible
Focused
Forgiving
Hopeful
Ingenious
Mature
Open
Patient
Persistent
Reasonable
Reliable
Steady
Strong
Thorough
Trusting
Truthful
Willing
Reflections
• What you hear, what you observe
• Not problem solving or advice
• Succinct ~ momentum
41
“I like to chill with my friends. I’m not going to
quit smoking pot because it’s not a problem.”
You don’t want to quit smoking pot.
Hanging out with your friends is an
opportunity to relax.
Pot doesn’t pose any problems for
you and if it did you would do
something about it.
Being Prepared for “Resistance”
1. Everyone drinks.
2. Pot is no big deal.
3. I can quit anytime I want to.
4. There’s nothing else to do around here.
Open-Ended Inquiry
Affirmations
Reflections
What are we especially listening for?
The person’s own arguments for change!
Desire
Ability
Reasons
Need
Commitment
Action
Taking steps
Nothing
works
I can’t miss
any more
school
I’m a loser
I’ve
heard it
all before
I need to
get my
phone
back
Change Talk
The Road to Change
• What would need to happen for you to want to make
a change? (Desire)
• How would you do it if you decided? (Ability)
• What are the three best reasons? (Reason)
• What’s most important to you? (Need)
Brief Intervention
1.
2.
3.
4.
Raise the subject
Provide feedback
Enhance motivation
Develop a plan
Achievable Goals
Defining Success
Risky behaviors & associated consequences
vs
Quantity & frequency
• What could you do differently?
• What might be your next step?
• What would a shift in use look like?
Readiness Rulers
– On a scale of 0 to 10, how important is it for you to
do something different?
– On a scale of 0 to 10, how confident are you that
you can do something different?
Close on
Good Terms
Summarize the patient’s statements in
favor of change.
Emphasize the patient’s strengths.
What agreement was reached?
CDC, 2014
Video: Adolescent
Referral to
Treatment
Use the BI Structure
(even if referring to treatment)
especially if referring to treatment
1.
2.
3.
4.
Raise the subject
Provide feedback
Enhance motivation
Develop a plan
Help clients trust the process
By being part of the process
“Steven over at the treatment center is really good at…”
“I’d like to touch base to see how you’re doing…”
RT at Bill Wilson Center
1. Refer to the systems of care for clients more
open to entering treatment or who have
parent/guardian who will ensure participation.
2. Obtain a release of information from client in
order to follow up and connect with the intake
person and later the substance use treatment
provider, so that there can be on-going
communication.
Youth System of Care
(YSOC)
Adult System of Care
(ASOC) “Gateway”
408 272-6518
1-800-488-9919
https://www.sccgov.org/sites/
dads/Youth-System-ofCare/Pages/home.aspx
https://www.sccgov.org/sites/dads
/Adult%20System%20of%20Care/
Pages/Adult-System-of-Care.aspx
• Networks of providers overseen by our county’s Department
of Behavioral Health Services.
• Each have a single entry point.
• Once a referral is received, it is screened to match the client
to a provider, based on geographic location and language or
cultural considerations.
Other RT Options
Seven Challenges
• Evidence-based, harm-reduction model that focusses
on decision making.
• We have both groups and individual sessions
available.
• Particularly suitable for youth in a pre-contemplative
stage of change.
Other Resources
• Stephen Betts, Director, Behavior Health Integration
408 850-6137 sbetts@billwilsoncenter.org
Resources
RASAI Program Resources
http://www.nationalcouncildocs.net/reducing-adolescent-substanceabuse-initiative
Alcohol Screening and Brief Intervention for Youth: A
Practitioner's Guide
http://www.niaaa.nih.gov/Publications/EducationTrainingMaterials/Pa
ges/YouthGuide.aspx
Adolescent SBIRT Curriculum – NORC Univ of Chicago & Kognito
http://sbirt.webs.com/curriculum
Thank You!
pamp@thenationalcouncil.org
 0
0