")
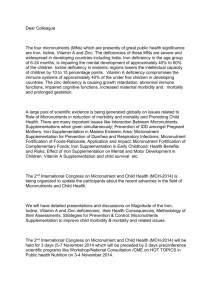
MODULE 5 STUDY GUIDE Micronutrient Deficiencies – Vitamin A, Iron and Iodine 1. Introduction 2 2. The nature of vitamin A, iodine and iron deficiency 6 3. Public health nutrition approaches to micronutrient deficiencies 10 4. Supplementation programs 11 5. Food fortification 12 5.1 Home based fortification 15 5.2 Biotechnology and the prevention of micronutrient deficiency diseases 16 6. Indirectly addressing malnutrition: Nutrition-Sensitive Interventions and Water, Sanitation and Hygiene (WASH) 17 7. Summary of key points 19 8. Conclusion 19 References 21 © Deakin University 2019 1 Essential Task 5.1: Career preparation Throughout this unit there have been tasks related to career preparation, to help you for entry into the workforce. Take a moment now to stop and reflect upon what you have gained, learnt and prepared from these tasks so far. If you haven’t done so already, make sure you have undertaken the following activities as a minimum: 1) Researched potential career pathways, job titles and job opportunities of interest (for example, using SEEK) 2) Written some statements to include in your CV about skills/knowledge you have gained/improved during this unit (and other units this trimester) 3) Collated a list of some resources / tools / sources / websites / twitter feeds etc. that you have accessed during the unit and could use again in future Remember that all these don’t have to be nutrition specific. For example, skills in critical analysis, writing proposals, taking on board feedback, working with disadvantaged groups, understanding indigenous health, considering environmental sustainability, systems thinking, etc. are likely to be relevant to many jobs. 1. Introduction Micronutrient deficiencies (defined as deficiency in one or more micronutrients) affect over two billion people world-wide in both developing and developed countries. Vitamin A, iron and iodine are key micronutrients listed in the Copenhagen Consensus (2008)1 as priority global health challenges. Deficiencies in these nutrients create enormous costs for communities in terms of health, lives lost and reduced economic productivity, and rectifying micronutrient deficiencies is considered as one of the top three international development priorities (Horton, 2009). Micronutrient deficiencies in developing countries are frequently associated with poverty, lack of adequate access to health care, low levels of maternal education and a poor quality diet. For developed countries, micronutrient deficiencies such as iron deficiency are primarily found in socioeconomically disadvantaged population groups while sub clinical deficiency states exist in populations where the deficiency has previously been eradicated. The borderline iodine status seen in parts of the Australian population provides one example of this. Copenhagen Consensus Centre is a ‘Think Tank’ based in Denmark that uses sound economic science to advise governments on the best ways to spend aid and development money. 1 © Deakin University 2019 2 In this module, the three most prevalent micronutrient deficiencies (Vitamin A, Iodine and Iron) will be discussed in terms of the complex determinants of causation; the population groups affected; and the global public health nutrition strategies established to address these deficiencies. Some areas of current debate will also be noted, together with recommendations for future program directions. 1.1 Module 5 Learning Objectives When you have completed this module you should be able to: Identify the extent of the global prevalence of vitamin A, iron and iodine deficiencies and describe the determinants of each; Discuss the historical perspectives of nutrition science and the development of public health nutrition practice in addressing micronutrient deficiencies; Compare and contrast key strengths and limitations of existing public health nutrition strategies seeking to address micronutrient deficiencies; Identify and explain the most suitable ways to prevent or ameliorate micronutrient deficiencies in the future. 1.2 Module 5 Key Dates In 2019, the following dates are the most important to be aware of, linked to Module 5 and end of the Trimester: • • • Final Seminar (attend one online seminar only through BB Collaborate): Monday 16 Sept. 7:30pm AEST; Tuesday 17 Sept, 9am AEST; Wednesday 18 Sept noon AEST. NB: If attendance is poor a seminar may be cancelled so check the news item and also ensure you RSVP in the appropriate Discussion Board thread. The presentations (in 2 parts) for module 5 can be watched at any time throughout weeks 9 to 11 of trimester The HSN302 exam will be scheduled in exam period – check your Deakin Sync for details © Deakin University 2019 3 Essential Task 5.2: Online Visit: http://www.un.org/sustainabledevelopment/ The UN’s Sustainable Development Goals (SDGs) officially came into being on January 1, 2016 (they build on the previous Millennium Development Goals www.un.org/millenniumgoals). The 17 SDGs aim to end all forms of poverty and are extremely ambitious. Have a look through the goals (go to the GOALS tab) and in particular read Goal 2: End hunger, achieve food security and improved nutrition and promote sustainable agriculture. Once you have progressed in the module, revisit the SDGs and consider which of the micronutrients has a relationship to other goals in addition to goal #2. For more information; refer to the WHO website and the United Nations Decade of Action on Nutrition - 12 of the 17 SDGs require good nutrition to be met. This website also gives a snap shot of the prevalence of stunting and the double burden of malnutrition. Background The scientific understanding of the nature of micronutrient deficiency developed over the course of the 19th and 20th centuries and many of the micronutrient deficiencies identified were eliminated or reduced during this time in industrialised countries. Historically, food fortification programs in the United States and other industrialised countries were fundamental to reducing the level of micronutrient deficiency diseases such as scurvy, (vitamin C), anaemia (iron), and pellagra (niacin deficiency). For example, the introduction of iodised table salt in Switzerland and some states in the USA reduced the level of iodine deficiency diseases in the majority of populations affected with goitre. The fortification of foods in these developed countries, which followed on the footsteps of this emerging nutrition science, was successful in eliminating most of these deficiencies. This was due to a well-developed food production system, appropriate packaging and labelling, the establishment of monitoring and surveillance systems and reasonably high levels of consumer awareness. The international public health nutrition community then turned its attention to the developing world, in an effort to address the high prevalence of micronutrient deficiencies particularly © Deakin University 2019 4 Vitamin A, Iron and Iodine. Semba (2012) refers to this approach as the iterative nutritional paradigm (see Figure 1). Figure 1. The Iterative Nutrition Paradigm: Figure source: Semba R. (2012) For developing countries, the science and technological platforms of delivery (e.g. food fortification, nutritional science and agricultural reforms) are largely already been established. How to deliver effective and sustainable programs, given the economic and socio-political constraints occurring in many countries, provide some of the nutritional challenges for the 21st century. Essential Task 5.3: Watch Please watch the video interview with Sonia Brockington, a past staff member of Deakin’s School of Exercise and Nutrition Sciences, about her experience working in international nutrition and with nutrient deficiencies (14 mins). Supplementary Task: Read If you are interested in further information about undernutrition and possibly future work in this area, Sonia has recommended reading the 2008 series in The Lancet: Maternal and Child Undernutrition. Also, see this more recent comment on the Sustainable Development Goals and children’s nutrition by Bhutta in a 2017 edition of The Lancet. © Deakin University 2019 5 2. The nature of vitamin A, iodine and iron deficiency The manifestation of a micronutrient deficiency is usually linked to the function of the nutrient in the body. The role of these three micronutrients in the body with regard to the impact on health will only be briefly discussed in this section because detailed information regarding the nutritional biochemistry of vitamins has been discussed in other units (HSN201/HSN211). For more details on this please refer to nutritional biochemistry text books, for example see Whitney, Rolfe, Crowe et al. (2011). Figure 2 (page 8) provides a brief overview of the key symptoms and risk factors of deficiency for these nutrients. Vitamin A Vitamin A deficiency is estimated to affect around 190 million children and 19 million pregnant women worldwide (WHO). Vitamin A is required for vision, cell differentiation and maturation, immunity and reproduction. Vitamin A deficiency is the leading cause of paediatric blindness in the developing world, in adolescents and adults it causes Xeropthalmia (a drying of the epithelial lining of the eyes), night blindness and affects maternal reproductive outcomes (e.g. increased maternal deaths occurring in pregnant women who have night blindness due to the associated risk of infection). Given the association between Vitamin A and immune function, Vitamin A deficiency is also an underlying cause of early childhood deaths due to measles, malaria and other infections. Poor dietary quality (in particular limited meat and animal product consumption) and lack of food diversity is a significant causative contributor to the development of this deficiency. Globally, Vitamin A deficiency appears mostly as a public health problem in countries where the food supply lacks preformed Vitamin A (meat and dairy products) and precursor carotenoids (fruit and vegetables) and is often associated with those causal factors contributing to Protein Energy Malnutrition, infections and other micronutrient deficiencies. Vitamin A deficiency is wide spread in South and South East Asia and vast regions of Africa (Sahel2 and sub-Saharan regions). Vitamin A deficiency has been virtually eliminated in developed countries (see global data base, http://www.who.int/vmnis/database/en/). Iron Iron is involved in the oxygen carrying function of haemoglobin in blood and myoglobin in muscle as well as other important metabolic processes in the body. When an individual has insufficient iron to maintain normal physiologic functions, they are considered iron deficient (Baker, 2010). Iron deficiency affects populations in both developing and developed countries and is the biggest contributor to nutritional anaemia. Anaemia is a condition defined by the level of haemoglobin (Hb) 2 standard deviations below the average for a normal population of the same age and gender (Baker, 2010). More simply, WHO defines anaemia as a state where the number of red blood cells or their oxygen-carrying capacity is insufficient to meet physiologic needs (WHO, nd). Note that 2 Sahel is the semi arid mid section running from the west to east coast of Africa (see a map). Most articles etc. discussing regions don’t state every country other than if for a specific reason. © Deakin University 2019 6 age, sex, altitude, smoking, and pregnancy status will influence Hb levels (WHO, nd). Anaemia affects 1.62 billion people world-wide with menstruating women most at risk (WHO). Globally, severe iron deficiency anaemia is linked to morbidity and mortality in women and children as well as increasing the mortality associated with infections such as malaria. See maps on global prevalence here. Birth outcomes such as premature and low birth weight babies are also linked to iron deficiency anaemia. Poor quality diet, rapid growth, pregnancy and menstruation are some risk factors for iron deficiency anaemia with the higher risk of infections in developing countries adding to the picture. Studies on Iron status in Australia reflect similar figures to other developed countries (10.6 % in female population< 50 years of age) (Ahmed et al, 2008). Iodine The World Health Organization (WHO) estimates that 31% of the world’s population (including Australians) have insufficient intakes of iodine and are at risk of developing a spectrum of disorders call Iodine Deficiency Disorders (IDD) (WHO). Iodine is required for the synthesis of thyroid hormones which are involved in the regulation of gene expression; thus cellular development and differentiation, metabolism, bone growth and development and most importantly brain development. Iodine deficiency is the leading cause of preventable mental retardation globally. Notably, it is seen as the most significant contributor to preventable brain damage during early stages of life. Reductions in cognitive development can affect children’s learning potential, which on a population scale can affect the educational and economic capacities of communities in iodine deficient areas. Goitre, an enlargement of the thyroid gland, can also affect adult’s health and work capacity in endemic iodine deficient areas. Iodine Deficiency Disorder is a nutritional disorder primarily caused by low levels of iodine in soil and water. Prevalence rates for iodine deficiency are moderate to high in European and Mediterranean countries and the Middle East, with some regions of China also included. Australia, New Zealand and the USA were once iodine replete, however changes in food production technology (removal of iodophores previously used in food production) have been attributed to the changes in the iodine status of these populations. © Deakin University 2019 7 Essential Task 5.4: Read and Think For a quick summary regarding the progress made against iodine deficiency, watch this short video http://www.ign.org/p142002491.html Then please read this paper on Iodine deficiency: Zimmerman, M.,(2010). ‘Geographical and geological influences on nutrition’, Iodine deficiency in industrialized countries. Conference article. Proceedings of the Nutrition Society. 69,137-143 It is not necessary for you to remember every detail of prevalence and policies for each country, but this reading is useful to consider the broader similarities and differences between countries. For any of you who wrote an assignment on Iodine in HSN202, you may be able to skip some of the early sections, but everyone should read the sections on treatment and prevention and examples from different countries (page 136 onwards). 1. Summarise the reasons why populations in Europe still have high prevalence of iodine deficiency. 2. Consider if these constraints are applicable to developing countries, or are they specific to Europe and other developed countries? Figure 2: Summary of symptoms and risk factors associated with Vitamin A, Iron and Iodine deficiencies Nutrient Vitamin A Iron Iodine Symptoms of deficiency Risk factors Xerophtalmia, night blindness, skin rashes, impair immunity Inadequate intake of Vitamin A, fat malabsorption, or liver disorders Anaemia Inadequate dietary intake of iron, blood loss, increased needs, exercise, abnormal iron absorption Hyperthyrodism or hypothyrodism, mental retardation in children and intellectual disability, hair loss, fatgiue and slow reflexes Low iodine soil content, reduced use of salt or use of uniodised salt, consuming large amounts of processed foods (generally iodised salt not used) © Deakin University 2019 8 Module 5 Milestone Well done on completing half of the micronutrients module. This is an opportunity to summarise your main learnings so far and get ready for the exam. I want you to consider if you have understood the concepts presented above and go back re-read or re-watch anything that remains confusing and/or post a question on the discussion board. Speaking of the discussion board – this the time to check - what are other students saying about iodine or the other readings and activities? Read their thoughts and share your own. This is also a good time to take a break. When you are ready, move on to the next part of the module. © Deakin University 2019 9 3. Public health nutrition approaches to micronutrient deficiencies The WHO/CDC logic model for micronutrient interventions in public health maps out the programme theory and plausible relationships between inputs and expected SDGs. The advantage of this logic model is that it can be adapted to different contexts and used for purposes such as planning, performance measurement or evaluation (WHO, 2016). The main global strategies to directly address micronutrient deficiencies can be broadly categorised as supplementation, food fortification, home based approaches and biotechnological approaches. Each of these potential strategies is discussed below. Additionally, there is increasing recognition recently of the importance of other related factors which contribute indirectly to undernutrition and nutrient deficiencies, and therefore increasing focus of interventions on more than just providing the deficient micronutrients. The role of Nutrition Sensitive Interventions and Water, Sanitation and Hygiene (WASH) are also discussed below. Essential Task 5.5: Online Each of the organisations listed below play roles in addressing the micronutrient deficiencies discussed in this module. Spend a few minutes exploring each website and take particular notice of the type of organisation and service/programs offered. Visit Micronutrient Initiative (MNI): www.micronutrient.org Visit the Global Alliance for Improved Nutrition (GAIN): www.gainhealth.org Visit The Iodine Global Network website: http://www.ign.org/ You might like to discuss your responses on the CloudDeakin discussion board. Activity: Compare the roles and actions of the organisations above to that of UNICEF. Visit http://www.unicef.org/nutrition/index_iodine.html Careers question: Does working with any of these organisations interest you? Why or why not? © Deakin University 2019 10 4. Supplementation programs Vitamin A As a public health nutrition strategy, Vitamin A supplementation has been deemed to be the most effective way to prevent vitamin A deficiency. The supplementation of children is the primary focus of programs with some programs also supplementing postpartum women. Supplementation involves the delivery of twice yearly doses of retinol capsules to children between 6 and 59 months of age. Dr Alfred Sommer (1986) in his seminal trial on Vitamin A supplementation, showed a 34% reduction in child mortality rates in children in Indonesia with high dose vitamin A capsules. This study and other similar trials are regarded as the evidence base for Vitamin A policy development, which has been adopted by UNICEF and implemented on a global basis. Supplementary Task: Read and view You may be interested to read Dr Sommer’s original study Sommer. A., Tarwotjo. I., Djunaedi. E,.et al(1986). Impact of Vitamin A supplementation on childhood mortality. A randomized controlled community trial. Lancet.327; 8491:1169-1173. If you are interested you can view also Dr Alfred Sommer’s presentation at Harvard School of Public Health on Vitamin A supplementation in the following clip (skip the first 6:30 minutes of introduction, need to install Silverlight in order to view). http://webapps.sph.harvard.edu/accordentG2/ddl20121212/main.htm?layout=default&type=ms&archived=visible&bandwidth=high&audioon ly=no# Vitamin A supplementation programs are delivered in a number of ways; through designated Child Health Days, through existing health services and/or combined with national or regional broad based programs such as national immunization programs. At other times, programs are instigated as a ‘vertical’ stand-alone program, particularly in high risk regions. Let’s discuss responses to this task in the Module 5 online seminar in week 10 Essential Task 5.6: Read and think Please read this report and answer the following study questions: Thapa S.(2010) Nepal’s Vitamin A supplementation program 15 years on. Sustained growth in coverage and equity and children still missed. Global Public Health. Vol 5, Number 4:325-334. 1) There were a number of key elements for program success listed in this article. Identify the main ones and consider how these could be applied to other micronutrient supplementation programs e.g. iron. 2) Another important aspect of this article is the investigation and discussion of those who did not receive Vitamin A supplementation. Why is this consideration an important part of a public health nutrition approach? © Deakin University 2019 11 Iodine Iodine supplementation in the form of oral doses of iodised oil usually occurs in regions of the world where Universal Salt Iodisation (discussed further below) has not occurred. Children are given a single dose of iodised oil annually and a one off dose for adults. This is not a very cost effective strategy and still may not reach populations groups that need it the most. Iron In countries where the prevalence of iron deficiency anaemia is relatively low, iron supplementation, after screening, is usually provided by the primary health care providers, as occurs in developed countries. In contrast when a large proportion of the population is affected by iron deficiency, universal iron supplementation is the approach used in most developing countries. As one example, the prevention of iron deficiency has now been included in the Thailand National Nutrition policy. While this has resulted in declining rates of anaemia in women and school-age children, a number of barriers to program implementation exist, reflecting global barriers to iron supplementation. These barriers include lack of a regular supply of iron tablets and women and health workers not understanding the impact of anaemia on health. Other barriers include unpleasant side effects of the medication (e.g. constipation) and irregular attendance at antenatal clinics where supplementation usually takes place. School based supplementation for children shows better outcomes for anaemia reduction, as a number of different strategies can be employed at the school site. The relationship of iron to other nutrients associated with anaemia, folate and vitamin A, makes the approach of supplementation with iron alone, questionable. Supplementary Task: Read and view You may be interested to read some of this paper: Winichagoon P, 2002, Prevention and control of anaemia: Thailand experiences, Journal of Nutrition, vol. 132, no. 4, pp. 862S-866S Current debate and discussion for program planners concerns the relative advantages and disadvantages of single versus multiple nutrient supplementation. Poor diet, lack of dietary diversity and infections impact on a number of different nutrients and it may be most practical to supplement a number of nutrients at one time. For example, iron and folate supplementation for pregnant women and women of child bearing age has been more effective in reducing anaemia than iron alone. 5. Food fortification Food fortification involves the addition of vitamins and minerals to food products to restore nutrients lost during processing or to incorporate nutrients that are low or absent in the population’s © Deakin University 2019 12 food supply. Food fortification is considered a public health nutrition strategy to prevent micronutrient deficiency states from occurring. It’s important to be aware that considerable controversy remains regarding fortification of the whole of a community for the benefit of a few. Controversies are broad reaching, but often relate to our poor understandings of the potential for harm. Supplementary task: read Read: Lawrence M, 2013, Food Fortification: The evidence, ethics, and politics of adding nutrients to food, Chapter 2: Food fortification evidence and ethics, Chapter 3: Food fortification politics: the actors, activities, and agendas. (Access via Oxford Scholarship Online link – use Internet Explorer as your browser). Food fortification for micronutrient deficiency requires using foods that are readily available and consumed by the population at an affordable price. Usual carriers for the nutrients are flour, maize, salt and sugar and oils. Universal salt iodisation is seen as the most successful example of a globally significant food fortification strategy, reaching over 70% of households worldwide. Food fortification programs can be implemented on a national scale, aiming for high population coverage and programs that are targeted at particular populations sub groups using specially formulated foods (complementary weaning foods for infants and fortified supplements for school age children and pregnant women). Vitamin A As an example of food fortification, mandatory fortification of sugar with Vitamin A has been implemented in Guatemala for over three decades. Evaluation studies have shown that the fortification program reduced the prevalence of Vitamin A deficiency significantly. Fortification of oils and condiments with Vitamin A used in cooking in Asian and middle east countries, and palm oil in West Africa, India and Malaysia, have also been linked to improvements in Vitamin A deficiency prevalence rates. However, even when estimates of coverage rates seem to be high as in some of the Latin American countries, some sub population groups such as infants do not consume the amounts of sugar (or oils) required to sustain serum retinol levels. This underscores the need for fortified weaning/complementary foods. Large scale programs require commitments from the private sector, particularly the food industry and government, good infrastructure and food distribution systems. The foods need not only adequate levels of the Vitamin A but also for sufficient amounts to be consumed. Regular monitoring of the food item to ensure that Vitamin A levels are maintained is necessary at both regional and central production sites. © Deakin University 2019 13 Iron Iron fortification of commonly consumed foods such as wheat flour can be a cost effective way of meeting a large population requirement for additional iron. Iron fortification of wheat flour and wheat products such as weaning/complementary foods, breakfast cereals, biscuits and cakes occurs in many developed countries. However, despite fortification, when these foods are included as part of a varied diet, they may not be consumed in sufficient quantities to influence the nutritional intakes of all population sub groups. At-risk sub groups are primarily those with high requirements (e.g. due to growth) or small intakes, including infants, young children, adolescents, pregnant women, and the elderly. Nutrition education on the importance of selecting and including iron fortified foods as part of the diet is an important adjunct with any fortification program. Supplementary Task: Read You may be interested in checking out further information in different countries regarding iron fortification: http://www.ffinetwork.org/global_progress/ Food fortification programs addressing iron deficiency anaemia in developing countries are complicated and have some of the limitations expressed above, but in addition, other constraints may influence anaemia prevention outcomes. Iron fortification technologically is more difficult compared to other nutrient fortifications and can alter the taste and appeal of the food. Developing countries may not have standardised technologies to enable this to happen or a formalised delivery system. Various iron food fortification options have been extensively studied in many countries including Thailand, Brazil and the Philippines. In Brazil, the addition of iron to wheat flour is now considered a mandatory and cost effective practice having the most significant large scale effects on anaemia prevalence rates in at risk population groups. Other fortification strategies such as the fortification of milk and drinking water with iron have also been tested in smaller populations groups but these strategies are yet to be adopted and scaled up to the national level. Through the employment of a range of strategies Thailand has also been successful in reducing anaemia levels in women and children. Food fortification has included a wider range of foods, including the fortification of condiments such as soy and fish sauces and noodles all of which are affordable to the poorer sections of communities. Globally, school based programs are seen as a most effective platform in providing children with a regular supply of fortified foods in the form of biscuits, milk or porridge blends. Iodine Given salt intakes globally are high; the addition of iodine to salt (salt iodisation) is seen as a very effective method to address deficiencies in both the developing and developed countries. © Deakin University 2019 14 Progress on improving iodine consumption is measured, on a population level, by the number of households consuming iodised salt and the levels of urinary iodine in population sub groups. Some countries have achieved quite significant household coverage such as China (95%) and Nigeria (98%). Denmark has virtually eliminated iodine deficiency through mandatory salt iodisation and the mandatory iodisation of salt used in the manufacture of bread has been introduced in Australia (and other countries) after the re-emergence of sub optimal iodine status in certain segments of the population. In many developed countries, given the high salt intakes mentioned previously, there are public health moves to reduce the level of salt in foods, due to the adverse effects of high salt intakes on cardiovascular health. This may suggest a need to consider increasing iodine levels in other foods to meet recommended population intakes 5.1 Home based fortification Other types of fortification program used to increase intakes of these macronutrients, particularly iron, are the home fortification strategies such as ‘Sprinkles’. This is a powder containing iron alone or with other vitamins and minerals, which can be used in homes or schools. Sprinkles are added to existing foods and drinks and are very cost effective, however, achieving distribution and use remains a challenge in some communities. Another product is called Nutributter which has a slightly longer shelf life than a powder though is more expensive. These products are particularly good to increase the micronutrient intake of women and children in areas where deficiency prevalence’s are quite high and fortified foods are not readily available. For more information on these types of products see the Home Fortification Technical Advisory Group's Evidence pages. Essential Task 5.7: Read and think Access the report ‘The Early Nutrition and Anaemia Prevention Project’, June 2013, which discusses the assessment of remote Indigenous Australian infants’ iron status, and actions to address the issue. Read the introductory section on page 5-9, then section 4.5 (pages 19-21) “Multimicronutrient ‘sprinkles’ “, which discusses some of the practicalities of this homebased fortification strategy. 1. What were some of the benefits of this approach? 2. What were some of the challenges/limitations of this approach? Share your thoughts on the discussion board Homestead food production programs and dietary diversification The main objective of Homestead Food Production Programs is to increase and ensure year-round availability and intake of micronutrient-rich foods in poor households, particularly by women and © Deakin University 2019 15 children. These programs should be used in combination with both supplementary and food fortification programs. The aim is to increase the variety of foods eaten particularly those rich in vitamin A and iron, through nutrition education, social marketing, and the use of small loans to enable purchasing of seeds, tools and fertilisers. Supplementary Task: Online Read the following article and consider whether there is merit in reviewing some of the micronutrient deficiency strategies used in vertical programs toward more food based approaches. List your reasons for and against. Wallace. S., (2012) Understanding opposition to vitamin A supplementation in India. American Journal of Public Health. 102:1286-1297. 5.2 Biotechnology and the prevention of micronutrient deficiency diseases Biotechnology, or biofortification, primarily involves increasing nutrient-density of crops. It involves a number of key research areas, including developing new varieties of plants and crops through conventional farming practices (e.g. orange flesh sweet potato), development of drought and pest resistant seeds and/or genetic modification of foods to increase micronutrient levels. The use of biotechnologies for food production is an interesting and challenging issue to consider. There is much debate about the hazard and ethics of genetic manipulation of seeds, the ‘ownership’ of seed, and the ethics of not progressing with such technological approaches in the face of deficiencies. Essential Task 5.8: Online Read this brief information at the WHO website about biofortification. Scroll down the page and click on Current and ongoing clinical trials relating to biofortification of crops, to see examples of current research in this area and the different crops targeted (note there are a number of pages). Visit at least one of the following additional websites discussing biofortification: Watch this short video clip (3 mins) is one of series showing how in Uganda there are moves to increase Vitamin A adequacy by encouraging the biofortification, growing and consumption of orange Sweet Potato crops. Visit Golden Rice Project, to understand more about the rationale, development and distribution of Golden Rice. International Union of Nutritional Sciences Statement on Benefits and Risks of Genetically Modified Foods for Human Health and Nutrition Do you think biofortified crops are a good solution to Vitamin deficiency diseases? In answering this question, consider the following: - Is genetic modification of foods appropriate? When? Why or why not? - What are some key risks and benefits of biofortification? WhoUniversity stands to2019 benefit from biofortification (are there any potential vested interests?) ©-Deakin 16 6. Indirectly addressing malnutrition: Nutrition-Sensitive Interventions and Water, Sanitation and Hygiene (WASH) Finally, for this module, let us consider some broader approaches to this population nutrition challenge. Ruel and Alderman (2013) suggest that addressing maternal and child nutrition in at risk groups should not just focus on nutrient specific interventions but that there needs to be more research on the potential benefits of nutrition sensitive interventions and programs, for example in agriculture, social safety nets, early child development and education: Nutrition sensitive interventions are (those which) address the underlying determinants of fetal and child nutrition and development— food security; adequate caregiving resources at the maternal, household and community levels; and access to health services and a safe and hygienic environment—and incorporate specific nutrition goals and actions (Ruel and Alderman 2013, p536). Essential Task 5.9: Read & think Read the first two pages of Ruel & Alderman, Nutrition-sensitive interventions and programmes: how can they help to accelerate progress in improving maternal and child nutrition? The Lancet, 2013: 382; 536-551 and Multi-sectorial approaches to nutrition (page 19 is essential, however feel free to read more!) Summarise in your own words: 1) What are Nutrition Sensitive interventions? (How do they differ from Nutrition Specific Interventions?) 2) What are some examples of types of interventions which are Nutrition Sensitive? © Deakin University 2019 17 An example of a Nutrition Sensitive Intervention is action to improve Water Sanitation and Hygiene (WASH). Interventions focussed on WASH have been proposed as key strategies is addressing undernutrition. Essential Task 5.10: Read & think Access this 2014 briefing paper by Action Contre La Faim: Greater investment in Water, Sanitation and Hygiene is key to the fight against undernutrition. Read the Introduction & Part 1 (pages 3-6). Write yourself a summary of why addressing WASH in developing countries has been linked to improving nutrition outcomes, i.e: 1) What are the key links between WASH and nutritional status? 2) Why do WASH interventions improve nutritional status? 3) Could interventions to address WASH be cheaper and more sustainable than Nutrient Specific Interventions? Why? Have a look at the abstract in the following systematic review by Davesh et al (2017) Water, sanitation, and hygiene interventions for acute childhood diarrhea: a systematic review to provide estimates for the Lives Saved Tool. This paper reveals the outcomes of several WASH interventions on the risk of diarrhea. Final Essential Task 5.11: Think In summarising your readings from throughout this module, compare and contrast key strengths and limitations of existing public health nutrition strategies seeking to address micronutrient deficiencies. Revisit the Sustainable Development Goals (SDGs) and, based on your knowledge from this module about factors associated with micronutrient deficiencies, identify which of the goals are related in some way to micronutrient deficiencies and malnutrition. For a summary of some of the links, visit the synopsis of The Global Nutrition Report 2016, which discusses on page 2 how nutrition is central to the SDGs. © Deakin University 2019 18 7. Summary of key points Micronutrient deficiencies are defined as deficiency in one or more micronutrients, and affect over two billion people world-wide in both developing and developed countries. Deficiencies in Vitamin A, Iron and Iodine are key concerns. Micronutrient deficiencies are frequently associated with poverty, lack of adequate access to health care, low levels of maternal education and a poor quality diet. Traditional strategies to address micronutrient deficiencies are nutrition specific, and include supplementation, food fortification, home based approaches and biotechnological approaches. There is growing evidence that nutrition sensitive interventions and programs (for example in agriculture, social safety nets, early child development and education) and Water, Sanitation and Hygiene (WASH) initiatives can also be beneficial in reducing vitamin deficiencies and improving maternal and child health in at-risk populations. 8. Conclusion Micronutrient deficiencies affect over two billion people worldwide. Food fortification and nutrient supplementation was introduced around 30 years earlier in developed countries than in the first of the developing countries to receive them. As a result the prevalence of micronutrient deficiencies is still highest in developing countries. There has been considerable research into the best way to approach micronutrient deficiencies, particularly with a view of improving maternal and child health. Multiple approaches are available including nutrition specific interventions (supplementation, food fortification, home fortification, biofortification) and nutrition sensitive interventions. Different strategies work better in different places, and it is likely that a combination are required to ultimately address deficiencies and achieve the Sustainable Development Goals. © Deakin University 2019 19 Module 5 Milestone Well done on completing the final HSN302 module. Just before you turn to focus on the preparation for your exam, please take a few minutes to check in with the unit learning outcomes (below). How do you rate your own competence against these outcomes? Is there anything you need to work on before completing trimester? What can you show case in job applications, volunteer roles or your work place moving forward? Sincere thanks for your hard work in T2 and very best wishes for the exam and your future. Rebecca and Kristy © Deakin University 2019 20 References Ahmed. F.et al .(2008). Iron status amongst Australian adults: findings of a population based study in Queensland, Australia. Asia Pacific Journal of Clinical Nutrition. 17,(1):40-47 Baker RD, Greer, FR. The Committee of Nutrition (2010). Clinical Report—Diagnosis and Prevention of Iron Deficiency and Iron-Deficiency Anemia in Infants and Young Children (0 –3 Years of Age). American Academy of Pediatrics. Vol 125, issue 5. http://pediatrics.aappublications.org/content/pediatrics/126/5/1040.full.pdf Bhutta, ZA. Global child nutrition and the sustainable development goals. The Lancet. October 16, 2017. Vol 1. http://dx.doi.org/10.1016/ S2352-4642(17)30119-0 Lamounier. J., Capanema. F., Rocha. D., (2010) Iron fortification Strategies for the control of childhood anemia in Brazil. Journal of Tropical Pediatrics. 56,6:448-452 Retrieved from http://ezproxy.deakin.edu.au/login?url=http://dx.doi.org/10.1093/tropej/fmq001 Horton et al. (2009). Micronutrient fortification (iron and salt iodization), Copenhagen Consensus Centre. Available from: http://www.copenhagenconsensus.com/research/best-practice-papers/micronutrient-fortification. Semba R. (2012) The historical evolution of thought regarding multiple micronutrient nutrition. Journal of Nutrition.14,1:143S-156Sdoi:10.3945/jn.110.137745 Accessed 06/03/13 http://jn.nutrition.org.ezproxym.deakin.edu.au/content/142/1/143S.full.pdf+html Sommer.A., Tarwotjo.I.,Djunaedi.E,.et al. (1986). Impact of Vitamin A supplementation on childhood mortality. A randomized controlled community trial.Lancet.327;Issue 8491:1169-1173: Accessed 06/03/13 http://ezproxy.deakin.edu.au/login?url=http://dx.doi.org/10.1016/S0140-6736(86)91157-8 Thapa S.(2010) Nepal’s Vitamin A supplementation program 15 years on. Sustained growth in coverage and equity and children still missed. Global Public Health. Vol 5, Number 4:325-334. Accessed 06/03/13 http://ezproxy.deakin.edu.au/login?url=http://dx.doi.org/10.1080/17441690802676352 Wallace. S., (2012) Understanding opposition to vitamin A supplementation in India. American Journal of Public Health. 102:1286-1297 Retrieved from http://ezproxy.deakin.edu.au/login?url=http://dx.doi.org/10.2105/AJPH.2012.300759 Whitney, Rolfe, Crowe, Cameron Smith, Walsh, Understanding Nutrition: Australian and New Zealand edition. Cengage Learning, 2011. Winichagoon P. (2002) Prevention and control of anaemia: Thailand experiences. Journal of Nutrition.132,4:862S866S Accessed 10/12/13 http://jn.nutrition.org.ezproxym.deakin.edu.au/content/132/4/862S.full.pdf+html World Health Organization (WHO) Vitamin and Mineral Nutrition Information System (VMNIS) Micronutrients database http://www.who.int/vmnis/database/en/ World Health Organization (WHO) Anaemia. Accessed 28/08/2018 http://www.who.int/topics/anaemia/en/ Zimmerman, M.,(2010). ‘Geographical and geological influences on nutrition’, Iodine deficiency in industrialized countries. Conference article. Proceedings of the Nutrition Society. 69,137-143. Accessed 06/03/13 http://dx.doi.org.ezproxy-m.deakin.edu.au/10.1017/S0029665109991819 © Deakin University 2019 21