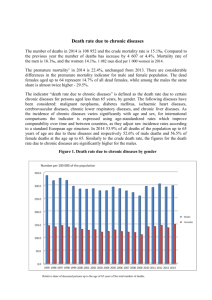
OCC3052 – ENABLING OCCUPATION II: PERFORMANCE CHALLENGES IN POPULATION HEALTH WEEK 8: CHRONIC CONDITIONS S2, 2019 LEARNING OBJECTIVES ▪ Understand and describe chronic conditions, their impact and their cost. ▪ Identify and examine the factors that influence the incidence and prevalence of chronic conditions. ▪ Explore how the Australian health systems respond to the demands created by chronic conditions. ▪ Reflect on what this means for OT practice. WHAT, HOW MANY & WHY? LIFE EXPECTANCY ▪ Australians are living longer. ▪ Life expectancy in Australia for a boy born in 2012 was 79.9 years, and for a girl, 84.3 years. ▪ Men who had survived to the age of 65 in 2012 can expect to live, on average, an additional 19.1 years (to 84.1 years), and women an additional 22.0 years (to 87.0 years). ▪ Life expectancy in Australia has risen by more than 30 years since the late 1800s. ▪ A boy born in 1890 had a life expectancy of 47.2 years; for girls it was 50.8 years. LIFE EXPECTANCY LIFE EXPECTANCY Males Females New South Wales 79.9 84.2 Victoria 80.5 84.5 Queensland 79.5 84.0 South Australia 79.8 84.2 Western Australia 80.1 84.8 Tasmania 78.7 82.6 Northern Territory 74.7 80.0 Australian Capital Territory 81.2 85.1 State or Territory In 2011, Australia was ranked 6th among OECD countries for life expectancy at birth for males, and 7th for females DEATHS IN AUSTRALIA ▪ There were 146,932 deaths in Australia in 2011. The leading underlying cause of death was coronary heart disease, accounting for 11,733 male deaths and 9,780 female deaths. ▪ For males the next most common causes of death were lung cancer (4,959 deaths) and cerebrovascular diseases (which include stroke) (4,427 deaths). ▪ For females the next most common causes of death were cerebrovascular diseases (6,824 deaths), and dementia and Alzheimer disease (6,596 deaths). CAUSES OF DEATH OVER TIME ▪ For both males and females, the five leading causes of death were the same in 2001 and 2011. The leading cause of death in both years was coronary heart disease, accounting for 20% of deaths in 2001 and 15% in 2011. ▪ For males, the largest changes in leading causes of death from 2001 to 2011 were the rise of dementia and Alzheimer disease from 13th to 6th place, and the fall of land transport accidents from 9th to 17th place. For males, two leading external causes of death (land transport accidents and suicides) fell in rank over this period while many cancer causes of death rose in rank (lung, prostate and pancreatic cancers, and cancers with unknown or ill-defined site). ▪ For females, cancer-related causes of death (breast, colorectal, pancreatic and ovarian) fell in rank over this period. Meanwhile, lung cancer deaths rose in rank, from 5th in 2001 to 4th in 2011. CAUSES OF DEATH OVER TIME ▪ For males, the largest changes in leading causes of death from 2001 to 2011 were the rise of dementia and Alzheimer disease from 13th to 6th place, and the fall of land transport accidents from 9th to 17th place. ▪ For males, two leading external causes of death (land transport accidents and suicides) fell in rank over this period while many cancer causes of death rose in rank (lung, prostate and pancreatic cancers, and cancers with unknown or ill-defined site). ▪ Although the number of new cancer cases each year is rising, largely due to population ageing, the number of new cases per 100,000 population is steady and death rates are continuing to fall. HEALTH & DEATH OVER TIME There has been a long and continuing decline in death rates in Australia. Between 1907 and 2012, the age-standardised death rate fell by more than 70%, from 2,054 to 550 deaths per 100,000 population. CHRONIC CONDITIONS AS CAUSES OF DEATH ▪ Coronary heart disease (CHD) was an associated cause of death for 51% of deaths due to diabetes, 28% of deaths due to chronic and unspecified kidney failure and 19% of deaths due to chronic obstructive pulmonary disease (COPD). ▪ Hypertensive disease was an associated cause of death for 35% of deaths due to diabetes, 28% of deaths due to cerebrovascular diseases (which include stroke) and 21% of deaths due to CHD. ▪ Kidney failure was an associated cause of death for 26% of deaths due to diabetes. ▪ Influenza and pneumonia was also a common associated cause of death – more specifically, for 31% of deaths due to asthma, 30% of deaths due to COPD and 29% of deaths due to dementia and Alzheimer disease. CHRONIC CONDITIONS AS CAUSES OF DEATH Selected chronic diseases as underlying and associated causes of death, 2011 (per cent) CHRONIC CONDITIONS & DEATH OVER TIME DEATH ▪ Currently, 9 in 10 deaths have chronic condition as an underlying cause. ▪ Cardiovascular diseases (coronary heart disease and stroke), dementia and Alzheimer disease, lung cancer and chronic lower respiratory disease including COPD are the most common underlying causes, together being responsible for 40% of all deaths. CANCER CANCER ▪ In 2010, 116,580 new cases of cancer were diagnosed in Australia (excluding basal and squamous cell carcinoma of the skin – the most common types of non-melanoma skin cancer). More than half (57%) of these cases were diagnosed in males. ▪ The risk of being diagnosed with any cancer before the age of 85 was 1 in 2 for males and 1 in 3 for females. ▪ The most commonly diagnosed cancers in 2010 were prostate in males (19,821), bowel (14,860), breast cancer in females (14,181), melanoma of the skin (11,405) and lung (10,296). CANCER ▪ The number and rate of new cases of cancer have increased over time. Between 1990 and 2010, the age-standardised incidence rate for total cancers rose by 16%, from 422 new cases per 100,000 people to 488 per 100,000. This was driven by rises in the incidence of prostate, breast and bowel cancers, due largely to improved detection and diagnosis of these cancers. ▪ The number of new cases of cancer diagnosed in Australia is projected to continue to rise over the next decade and is expected to reach 150,000 in 2020. This increase in the number of new cases, due primarily to population growth and ageing, is expected to be most evident among older populations. ARTHRITIS & MUSCULOSKELETAL CONDITIONS ▪ In 2011-12, an estimated 6.1 million people (28% of all Australians) had arthritis and/or another musculoskeletal condition. ▪ Arthritis was the most common condition, affecting 3.3 million people (15% of the population), including 8% with osteoarthritis and 2% with rheumatoid arthritis. Prevalence is higher in females than males (18% compared with 12%) and increases with age (affecting 52% of people aged 75 or over). ▪ Back problems and disc disorders affect about 2.8 million people (13% of the population). The rates are highest among people aged 65-74. ▪ An estimated 725,500 people (3% of the population) reported that they had been diagnosed with osteoporosis or low bone density (osteopenia). Most cases were reported by women (82%) and people aged 55 and over (83%). As these conditions have no overt symptoms, the figures may be underestimated. ▪ An estimated 64,200 children aged 0-14 had arthritis or another musculoskeletal condition. Juvenile arthritis affected less than 1% of Australian children. ARTHRITIS & MUSCULOSKELETAL CONDITIONS People with arthritis and other musculoskeletal conditions were more likely to report: ▪ Limitations in performing core activities (particularly self-care and mobility) than the overall population (44% compared with 15%). ▪ High or very high psychological distress (17%) than people without these conditions (9%). ▪ Experiencing mental disorders than those without these conditions (1.5 times as high). CORONARY HEART DISEASE ▪ In 2011-12, an estimated 585,900 Australians had CHD, with the condition being more common in men (3.3%) than women (2.0%) and among those aged 70 and over (15% compared with 2.2% for those aged 25-69). ▪ In 2011, an estimated 69,900 people aged 25 and over had a heart attack. There has been a 20% fall in heart attack rates over the last 5 years (age-standardised rate of 427 per 100,000 people in 2011 compared with 534 in 2007). STROKE ▪ In 2009, an estimated 375,800 Australians (205,800 males and 170,000 females) had had a stroke at some time in their lives. Most (70%) were aged 65 or over. ▪ The rate of stroke events has fallen by 25% over the last decade (from an age-standardised rate of 186 to 140 per 100,000 population between 1997 and 2009). But the total number of Australians experiencing a stroke rose by 6% over the same period, reflecting the ageing of the population. ▪ In 2009, over one-third (35%) of Australians who experienced a stroke had a resulting disability; this was an improvement from 1998 when the rate was 45%. STROKE Over the last 3 decades, stroke death rates have fallen by almost 70% (from an agestandardised rate of 103 to 33 deaths per 100,000 population between 1979 and 2011). MENTAL HEALTH ▪ 2007 data suggests that of the Australian adult population, an estimated that 45% of Australians aged 16-85 had experienced a mental disorder sometime in their lifetime (equating to 7.3 million people), and that an estimated 1 in 5 (20%) of the population aged 16-85 (equating to 3.2 million people) had experienced a common mental disorder in the previous 12 months. ▪ Of these, anxiety disorders (such as social phobia) were the most common, afflicting 14.4% of the population, followed by affective disorders (such as depression, 6.2%) and substance-use disorders (such as alcohol dependence, 5.1%). These 3 groups of common mental disorders were most prevalent in people aged 16–24 and decreased as age increased. Prevalence was higher for females than males in all age groups. MENTAL HEALTH ▪ From the child and adolescent survey conducted in 1998, 14% of children and adolescents aged 4-17 (an estimated 321,181 people in 2013) had a clinically significant mental health problem. ▪ In terms of less common but more severe mental disorders, estimates from the 2010 National Survey of People Living with Psychotic Illness indicated that 0.45% of the population aged 18-64 (almost 64,000 people) were treated annually by public sector mental health services for a psychotic disorder, with schizophrenia being the most common disorder. MENTAL HEALTH Prevalence of common mental disorders in the Australian population, 1997/1998 and 2007 CHRONIC RESPIRATORY CONDITIONS ▪ In 2011-12, about 3 in 10 Australians (29%) suffered from 1 or more chronic respiratory conditions (6.3 million people). ▪ Hay fever and asthma were the 2 most common conditions, affecting an estimated 3.7 million (17%) and 2.3 million Australians (10%). ▪ Asthma was one of the most common chronic health conditions among children, (i.e. estimated 393,000 children aged 0-14 (9%) in 2011-12). ▪ COPD was comparatively rarer (i.e. estimated at 529,000 Australians (2%)). ▪ Both COPD and asthma were more common in areas of lowest socioeconomic status than in areas with the highest status (4% compared with 2% for COPD, and 12% compared with 9% for asthma). ▪ Small fall in the age-standardised prevalence of asthma and COPD from 2001 to 2011-12, from 12% to 10% for asthma and from 4% to 2% for COPD. CHRONIC RESPIRATORY CONDITIONS & DEATH DIABETES ▪ There are an estimated 1 million people aged 2 or over with diagnosed diabetes in Australia. However, this is likely to be an underestimate – as for every 4 adults with diagnosed diabetes, there is estimated to be 1 with undiagnosed diabetes. ▪ Of all people with diabetes, around 85% have type 2 diabetes and 12% have type 1 diabetes. In addition, gestational diabetes affects about 1 in 20 pregnancies each year. ▪ Diabetes is becoming more common – the rate of self-reported diabetes more than doubled, from 1.5% to 4.2% of Australians, between 1989-90 and 2011-12. ▪ In 2011-12, diabetes was more common in men (6%) than women (4%) and was more common in older age groups – affecting 15% of those aged 65-74 compared with 5% for those aged 45-54. DIABETES ▪ In 2011, there were around 2,400 new cases of type 1 diabetes, with half of these being among people aged 18 or under. ▪ Rates of type 1 diabetes remained stable over 2000-2011, with age-standardised rates of around 10 to 12 new cases per 100,000 population per year. ▪ In 2011-12, there were around 49,800 new cases of diagnosed type 2 diabetes among people 10 and over, based on preliminary findings. ▪ Despite nearly all cases (92%) occurring in those aged 40 and over, there were around 430 new cases among children and young people aged 10–24 – even though type 2 diabetes is generally regarded as a disease of adulthood. DIABETES & MEDICATION CHRONIC KIDNEY DISEASE According to the 2011-12 Australian Health Survey, 1 in 10 people (or 1.7 million Australians) aged 18 and over have biomedical signs of CKD. There were about 2,500 new cases of KRT-treated-ESKD in 2011 (equating to an age-standardised rate of 10 people per 100,000 population or 7 new treated-ESKD cases per day). Diabetes was the leading cause of KRT-treated-ESKD in 2011, accounting for 1 in 3 new cases. Over-representations are present. INJURIES ▪ Injury was recorded as a cause of 10,668 deaths in 2009-10 in Australia, or 7.6% of all deaths. ▪ One-third of male injury deaths and almost two-thirds of female cases occurred at ages 65 and older. Less than 2% of cases were at ages younger than 15. ▪ The most common causes of injury deaths in 2009-10 were falls (32.2%), intentional self-harm (20.8%) and transport accidents (13.9%). ▪ From 1999-00 to 2009-10, injury deaths comprised a fairly constant proportion of all deaths in Australia, ranging from 7.4% to 8.1%. INJURIES ▪ Adjusting for age, injury deaths decreased from 55.1 per 100,000 population in 1999-00 to 46.8 in 2004-05, with little change in more recent years. ▪ The injury death rate was 45.4 per 100,000 population in 200910. ▪ For most external causes, rates of injury-related deaths tended to decline from 1999-00 to 2007-08: 3.8% per year for transport injury, 3.3% for thermal injury (i.e. exposure to smoke, fire, heat and hot substances), 5.5% for drowning, 3.2% for suicide and 5.5% for homicide. Rates of poisoning deaths involving pharmaceuticals fell sharply to 2001-02, then rose by 2.2% per year to 2007-08. ▪ Rates of fall-related injury deaths have not shown a marked trend. INJURIES & HOSPITALISATIONS IN VICTORIA, THE RESULT HAS BEEN… Projected prevalence of selected chronic diseases in Victoria 2022 Demand for health services is changing 70.0% 60.0% 50.0% 40.0% 30.0% 20.0% 10.0% Planning area W es t So ut h Co as t So ut h im m er a W M al ee an d Py re ne es Ea st Ce Gi pp nt ra sla lV nd ic -W el lin gt Go on Ge ul bu el on rn g Va an lle d ya Co nd as t Lo w er Hu m e Up pe r Hu m Ce e nt ra lG ip ps la nd Ce nt ra lH igh la nd s 0.0% Ce nt ra la nd Hospital utilisation could be better managed % primary care type presentations to ED Primary care type presentations to ED CHRONIC CONDITIONS: IMPACT & COST CHRONIC CONDITIONS: AN OVERVIEW ▪ Have complex and multiple causes. ▪ Usually have a gradual onset, and are often accompanied by acute stages, and may also have a sudden onset – especially after injury. ▪ Occurs at all stages cross the life span; more prevalent in older age. ▪ Can compromise quality of life through physical (and often comorbid mental) health limitation and disability. ▪ Are generally long term and persistent, leading to a gradual deterioration of health. ▪ Not usually immediately life threatening, but are a significant cause of premature death. CHRONIC CONDITIONS: WHAT & WHY? ▪ Advances in prevention and treatment of diseases and injuries has increased prevalence and incidence. This is alongside demographic changes (people living longer and an ageing population). ▪ Impact of lifestyle worldwide: tobacco, alcohol, physical inactivity, poor diet and nutrition, obesity, high blood pressure. ▪ WHO (2011) indicates a rapid increase in the global burden of disease due to chronic conditions. ▪ Predicts that by 2020, chronic conditions will account for approximately 75% of all deaths. ▪ In Australia, estimated that chronic conditions are responsible for over 80% of the burden of disease. CHRONIC CONDITIONS: COST & IMPACT Chronic conditions Source: Ratzen (n.d.) DALYS BY CONDITION BREAKDOWN OF DALYS BY CONDITION BURDEN OF DISEASE BY RISK FACTORS Behavioural: Smoking Behavioural: Inactivity Behavioural: Alcohol Biomedical: Diet Biomedical: Obesity Biomedical: Hypertension Biomedical: Blood fats Ischaemic heart disease Y Y N Y Y Y Y Stroke Y Y Y Y Y Y Y Type 2 diabetes Y Y N Y Y Y N Kidney disease Y Y N Y Y Y N Arthritis Y Y N N Y N N Osteoporosis Y Y Y Y N N N Lung cancer Y N N N N N N Colorectal cancer N Y Y Y Y N N COPD Y N N N N N N Asthma Y N N N N N N Depression N Y Y N Y Y N Y Y N N N N N Oral health SPENDING BY CONDITION TYPE OF SPENDING BY CONDITION CHANGE IN ADMISSIONS: 05/06 TO 09/10 CURRENT & FUTURE DIRECTIONS, Refining Australia’s Health System CHALLENGES ▪ Changed Commonwealth funding contribution – widening the fiscal gap ▪ Uncertainty and reduced transparency ▪ National prevention leadership ▪ Health workforce planning – national, public/private ▪ ACSQCHE - across public and private sectors ▪ Co-payment – pressure on primary health care and public hospitals Redefining Commonwealth – State funding arrangements Ensuring that on-going health care funding is sustainable RATIONALISING ROLES & RESPONSIBILITIES Particular emphasis on education and health care. NATIONAL HEALTH PRIORITY AREAS ▪ Arthritis and musculoskeletal conditions ▪ Asthma ▪ Cancer control ▪ Cardiovascular health ▪ Diabetes ▪ Mental health ▪ Injury prevention and control ▪ Obesity ▪ Dementia PREVENTION NATIONAL DISABILITY INSURANCE SCHEME ▪ NDIS will provide support for people with permanent and significant disabilities, their families and carers. ▪ As a group, people with disability experience significantly poorer health than those without disability. Almost half (46%) of people aged 15-64 with severe or profound disability report poor or fair health compared with 5% for those without disability. ▪ For people aged 15-64 with a specific long-term health condition or injury, a higher proportion of those with severe or profound disability than those without disability had: young onset of arthritis before age 25 (14% compared with 6%); osteoporosis before age 45 (43% compared with 31%); young onset of diabetes before age 25 (23% and 7% respectively). ▪ Progressing…sort of. QUALITY & PERFORMANCE ▪ Enhancing leadership and systems to achieve best use of people, resources, and evolving knowledge. ▪ Quality Prescribing Initiative, Polypharmacy Initiative, etc. ▪ Clinical leadership programs. ▪ Reporting and review programs – across all areas of service delivery. ▪ Various states of progress. OPPORTUNITIES ▪ PCEHR and HealtheNet ▪ Prevention – State leadership ▪ Primary Health Networks – shape agenda for integrated care ▪ Co-payments – States enter primary care ▪ ABM Portal – smart use of data ▪ Health Productivity and Performance – ensure breadth and relevance ▪ White papers on the Reform of the Federation and Tax Reform NATIONAL STRATEGIC FRAMEWORK FOR CHRONIC CONDITIONS NATIONAL STRATEGIC FRAMEWORK FOR CHRONIC CONDITIONS Objectives ▪ Focus on prevention for a healthier Australia. ▪ Provide effective and appropriate care to support people with chronic conditions and optimise quality of life. ▪ Target priority populations. Strategic Priority Areas Strategic Priority Areas have been identified under each Objective. These are the core priority areas where Partners should focus attention to achieve each of the Objectives. Partners can readily identify, plan and implement their own policies, strategies, actions and services against the Strategic Priority Areas. DoH, 2016 NATIONAL STRATEGIC FRAMEWORK FOR CHRONIC CONDITIONS Objective 1: Focus on prevention for a healthier Australia Strategic Priority Area 1.1 Risk reduction Strategic Priority Area 1.2 Partnerships for health Strategic Priority Area 1.3 Critical early life stages Strategic Priority Area 1.4 Timely and appropriate detection DoH, 2016 NATIONAL STRATEGIC FRAMEWORK FOR CHRONIC CONDITIONS Objective 2: Provide effective and appropriate care to support people with chronic conditions and optimise quality of life Strategic Priority Area 2.1 Active engagement Strategic Priority Area 2.2 Continuity of care Strategic Priority Area 2.3 Accessible health services Strategic Priority Area 2.4 Information sharing Strategic Priority Area 2.5 Supportive systems DoH, 2016 NATIONAL STRATEGIC FRAMEWORK FOR CHRONIC CONDITIONS Objective 3: Target priority populations Strategic Priority Area 3.1 Community and culture Strategic Priority Area 3.2 Targeted action DoH, 2016 BUT, IT’S NOT THAT EASY! CHRONIC CONDITIONS & THEIR RISK FACTORS ▪ In Australia, as elsewhere, the prevalence of chronic disease varies across the socioeconomic gradient for a number of specific diseases, as well as for important disease risk factors ▪ However, the diseases with substantial disparities across the socioeconomic quintiles are different, for different stages in the life course. ▪ Any health interventions to address the impact of chronic disease and associated risk factors, at a population level, need to take socioeconomic inequalities into account. PREVALENCE OF TYPE 2 DIABETES Rate ratios (Most/Least disadvantaged) – 2001: 2.39, 2011-12: 2.19 SMOKING RATES Rate ratios (Most/Least disadvantaged) – 2001: 1.87, 2011-12: 2.33 OBESITY RATES Rate ratios (Most/Least disadvantaged) – 1995: 1.34, 2007-8: 1.80, 2011-12: 1.63 SO, WHAT DOES THIS ALL MEAN? IMPLICATIONS FOR OT PRACTICE OTs are able to play a key role in meeting the challenges and demands of chronic conditions – be that at the upstream, midstream or downstream levels. The skills, knowledge and advocacy that OTs are able to bring to their work makes them an invaluable resource in working with chronic conditions. “Although more research is needed, evidence indicates that occupational therapy interventions improve BADLs and IADLs, health, and quality of life for people with chronic diseases such as RA, COPD, chronic heart failure, and depression. The evidence suggests that similar occupational therapy interventions are applicable across a range of diagnoses and may be applicable to diagnoses beyond the scope of this review. The interventions commonly include goal setting, energy conservation, joint protection, exercise, assistive devices, and coping strategies. Occupational therapy practice for people with chronic diseases can be continued and built on to meet the increasing prevalence and needs of people with these conditions” Source: Hand, Law & McColl (2011) CONCLUSIONS fast ▪ Australia’s health care system is complex and changing – : with chronic conditions a key driver of demand and cost, and therefore of reform. ▪ As such, responding to health needs requires practitioners to be able to work at the up, mid and downstream levels. ▪ Good health is more than just getting a service user/client to do what you suggest. Developing self-confidence and self-agency to manage your health requires the incorporation of psychological theory and findings, adult learning principles and health promotion concepts, as well as responding to change. ▪ This in turn requires recognition of political, financial, social and environmental contexts, enabling service users/clients to address the multiple barriers to better health and well-being that they face. ▪ There is no simple solution, especially to the challenges posed by chronic health conditions.