This article appeared in a journal published by Elsevier. The attached
copy is furnished to the author for internal non-commercial research
and education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling or
licensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of the
article (e.g. in Word or Tex form) to their personal website or
institutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies are
encouraged to visit:
http://www.elsevier.com/copyright
Author's personal copy
Clinical Immunology (2009) 132, 420–424
a v a i l a b l e a t w w w. s c i e n c e d i r e c t . c o m
Clinical Immunology
w w w. e l s e v i e r. c o m / l o c a t e / y c l i m
Letter to the Editor
Autoreactivity to sweat and sebaceous glands and
skin homing T cells in lupus profundus
Lupus erythematosus profundus or lupus erythematosus
panniculitis (LEP) is a clinical variant of lupus erythematosus,
which involves the deep dermis and subcutaneous fat tissue.
Here we illustrate some previously undescribed findings in
LEP by direct immunofluorescence (DIF) and by immunohistochemistry (IHC). These include autoreactivity to the sweat
and sebaceous glands that were in close proximity to the
inflamed panniculus, and a strong expression to ezrin,
radixin and moesin; (ERM) with colocalization of CD44,
CD3, CD4, CD8, CD45 and HLA DP,DR,DQ. Based on our
findings, ERM seem to contribute to the polarization of the
extracellular matrix to allow T lymphocyte homecoming
locomotion within the skin, including sweat and sebaceous
glands and panniculus in LEP.
Report
A 48-year-old African American female presented with a
three-month history of multiple, asymptomatic, erythematous plaques and nodules on the leg. She denied arthralgia,
arthropathy, myalgia, fatigue, fever, Raynaud's phenomenon, gastrointestinal symptoms, and lesions occurring on
the head, trunk, and upper extremities. We found no
associated systemic symptoms. At the physical exam we
detected multiple, erythematous nodules and indurated
plaques on the lower right thigh. Lesions were skin-colored,
plaques. Laboratory data shows and erythrocyte sedimentation of 3 mm/h. A complete blood count with differential
analysis, electrolytes, blood urea nitrogen, creatinine, liver
function tests, urinalysis, and a chest radiograph were
normal. Antinuclear antibody titer was normal. Antibodies
to double-stranded DNA, SS-A, and SS-B were negative.
Anti-streptococcal antibody titers were negative. Levels of
C3 and C4 were normal. A punch biopsy of the scalp
ulceration was performed H & E stain, direct immunofluorescence (DIF) and immunohistochemistry (IHC) studies. H &
E displayed histologic features of lupus erythematosus
profundus or lupus erythematosus panniculitis (LEP). We
also observed autoreactivity to sweat and sebaceous
glands, as well as the presence of ezrin and several cells
that infiltrated including CD44, CD3, CD8, CD45 and HLA DP,
DR,DQ.
1521-6616/$ - see front matter © 2009 Elsevier Inc. All rights reserved.
doi:10.1016/j.clim.2009.05.009
DIF
In brief, 4 μm thick skin cryosections were partially fixed on
3% paraformaldehyde, and incubated with the secondary
antibodies all FITC-conjugated. The following antibodies
were raised on rabbit directed to a) anti-human IgG (γ
chain), b) anti-human IgA (α chains), c) anti-human IgM (μchain), d) anti-human fibrinogen, and e) anti-human albumin
(all at either 1:20 to 1:40 dilutions), all from Dako,
Carpenteria, California, USA. In addition to anti-ezrin
antibodies and its secondary we used Alexa Fluor® 647conjugated anti-mouse (both from Invitrogen, USA).
IHC
To study the possible correlation of the {ezrin, radixin and
moesin; (ERM)} and the homecoming immune cells to the
skin, we performed IHC by using a dual endogenous
peroxidase blockage, according to the Dako (Denmark)
insert, with the addition of Envision dual link. Furthermore,
we applied 3, 3 diaminobenzidine and counterstained with
hematoxylin. The samples were run in a Dako Autostainer
Universal Staining System. We tested for goat anti-human
CD44, CD3, CD4, CD8, CD45, HLA DP,DR,DQ and anti-human
IgM. Our tests showed positive staining by both DIF and IHC
of the sweat as well as the sebaceous by various antibodies.
In addition we detected overexpression of ezrin with
colocalization of antibodies directed to CD44, CD3, CD4,
CD8, CD45 and autoreactivity with IgM. See Figures 1 and 2.
Following the diagnosis of LEP, the patient was treated with
plaquenil, 200 mg/day and the response to this therapy was
characterized by slow regression of the inflammatory
lesions.
Discussion
Only few cases in the world have described autoreactivity
to sweat and sebaceous glands in lupus panniculitis as
shown in our case. We tested for ERM and CD44 based on
the fact that these molecules have been shown to promote
T cell activation [1]. CD44 is a binding partner for the
membrane–cytoskeleton cross-linker protein ezrin. The
transmembrane receptor CD44 conveys important signals
from the extracellular microenvironment to the cytoplasm, a phenomenon known as “outside–in” signaling [1–
3]. As described for other authors, we demonstrated that
infiltrating T lymphocytes seem to be directed by a signal
from the CD44, a receptor for extracellular matrix
Author's personal copy
Letter to the Editor
proteins and glycosaminoglycans [1–3]. These findings
suggest that migratory polarity of some immune cells
including some T cell subpopulation may depend on the
recruitment of ERM proteins by the intracellular domain of
CD44 and other cells including CD3, CD4, CD8, CD45 and
HLA DP,DR, DQ. Other studies have shown other immuno-
421
logic roles of ERM based on the fact that CD44–ezrin–actin
is an important modulator of Fas-mediated apoptosis
signal pathway [4,5].
LEP is characterized by a predominately lobular, B-cell
lymphocytic and plasmacytoid infiltration in the subcutaneous adipose tissue, with progressive fibrosis and septal
.sitielu
rce
h
fotcin
a
pla
icin)A
p
il.l(csievtC
D
i54tjd
.n
u
a
o
ls(ce
h
tin
ra)C
tkso
e
lD
P
i8
n
ase
p
rn
ole
itcyp
o
e
h
fitad
izini,ld
a
n.yh
scm
oFsega
p
m
h
o
la,rce
lasm
p
cytayfo
cp
h
rltlhstiw
aie
fntsn
e
di lucrain
e
aslb
p
re
a
u
h
o
,nitlitnw
on
w
.od
isIe
h
alr)ityra
cp
e
d
o
lym
s(ird
ein
to
se
m
yd
n
satyfio
cp
h
ltih
artlih
fnstw
iitilucrain
alb
p
u
o
y)H
se
lia
t.gnm
o
d
e
(&
)r×
w
0
o
p
m
e
d
in
4w
to
)(sln
roiaEratleyd
)se(rm
sl(a
rd
eiicin
,fse
a
h
lm
osn
rw
p
e
ih
u
td
sfotle
iw
cvo
e
in
p
e
rsa
fzlistalayisp
o
lgn)h.A
w
o
r(w
o
)tselrsw
erd
ia
o
b
e
lysu
m
n
bi(m
u
th
lia-n
n
a)d
ew
sita
n
e
sgu
talsm
d
n
u
jow
rca
e
h
d
lra
T
n
e
C
h
c-tlu
p
ie
cIFrginc(iniatraslucrraiclu
gn
o
a,)ra
gB
.yFt()w
so
×D
0I4
knr)(rap
isA
d
e
(glm
rew
e
Irtd
le
n
a
rcsu
w
la
im
p
e
o,n
tb
fe
lrscveistn
sp
o
ew
d
.od
e
iIa
nr)rea(tn
ro
a
etp
aiam
tcA
n
u
grld
sea
jfo
te
h
Iap
id
/
e
m
tird
elsa
d
o
p
evsrm
u
hd
ib
oA
-n
gaid
eitn
a
Igu
tn
ajn
ocT
C
g-nFIre
ih
)D
A
stu
Io
n
fw
.o(kn
sr)m
o,n
sb
ye
tra
h
p
isw
e
m
atid
(n
e
orsltn
b
w
m
p
eiw
d
o
t.b
e
o
n
rd
liIa
n
tco
r)p
ie
rai(m
tcn
u
o
rd
ela
je
h
ta
ip
/m
tb
urd
elairtw
o
h
serd
se
and
ib
oa
d
ieitagu
tln
aM
gjn
G
og,cd
n
a
T
A
C
,Ig-n
e
sp
u
rvoth
C
ld
,n
I3
b
F
a
cifsw
e
lla
tih
n
d
e
)u
oe
h
sA
filF
ro
a
d
e
t.n
w
vH
C
lD
s(p
o
t8)a
e
rIsld
.w
io
h
ge
(cta
sguajT
n
iC
e
oIgcsp
oIFim
u
h
nb
r-e
n
h
ra
ifo
sw
d
vt.iw
o
gn
ftsT
a
e
h
w
o
)ln
a
igd
etlrsikn
aw
so
ru
h
ale
dyi)sgn(sp
oind
yb
io
a
en
otrw
insd
e
(ia
ltn
o
m
e
a
su
tid
n
gw
arw
d
le
itsa
zcv0
n
o
u
5
w
lie
h
grfn
-cs:a1
e
d
itb
so
n
a
eivtn
asiti,n
ospitnd
).d
iIa()×04w
o
)d
e(rs)rga
n(inseiw
a
e
nd
ib
e
o
trgsu
n
ego
i(tn
aim
u
hb
r-n
aid
eitfae
gu
n
tad
sgw
n
h
jo
w
ie
ch
tsalw
T
in
e
C
h
grt-cm
)vo
iT
e
w
.h
Io
iF
a
s(m
w
io
se
d
)tD
lta
srIo
n
ua
w
r)ignh
(sp
oiniae
utgnb
ld
se
nD
ia
p
(n
isu
a.t,Icsd
,)×0
ie
w
g4
h
r,o
)d
ert(n
u
lsocr)n
e
ra(rgse(d
ib
od
eitagu
tn
ajn
ocT
C
-IFG
h
g-,te
nw
sgn
d
Iaie
th
sa
fo
in
lgrte
m
cveiam
it,tb
)so
w
n
u
.B
d
yF(ve
e
i)×
w
0
ore
D
1sw
I)b
o
p
so
(lre
n
rale
w
yd
sn
aiu
to
e
s(d
n
u
a
o
recltb
a
gyecosFigure
itse
ym
gn
d
sa
tyfo
lcp
h
m
ih
tsoein
taso
ycrm
std
n
i}R
a
E
M
e
xhn
t;rd
on
)t(ie
h
P
E
m
xd
so
n
Lalw
itp
,eirtsm
o
a
e
n
p
h
li)gan
o
.A
e
fn
r(zefio{sn
oseop
re
h
xit1
tn
e
rvo
c,tH
tailcf&
h
in,csp
e
tH
gn
w
fC
,e
o
isP
h
E
rLaiIu
d
n
tgld
n
a
cF
sin
FD
ifh
I)aIt(
Author's personal copy
422
scarring. LEP is an unusual presentation of lupus erythematosus, characterized by deep subcutaneous nodules, most
commonly localized to the upper limbs and face [6,7]. The
clinical and histologic diagnoses of LEP may be difficult in
cases in which involvement of subcutaneous fat tissue is the
only manifestation of the disease. LEP has also been
reported to associate with discoid lupus erythematosus
(DLE) [7]. In our case, in addition to positive classic lupus
band test, we detected autoreactivity to sweat and
sebaceous glands by DIF as well as a strong autoreactivity
directed to ERM, both at the inflamed glands as well as the
epidermis above the panniculitis and under the panniculitis.
In a related case of lupus erythematosus treated with
cyclophosphamide, other authors have reported that DIF
showed not only positive lupus band test but also a
autoreactivity two eccrine sweat glands also occurred as
described in our case [8]. Other authors have described a
novel autoantibody reactive with carbonic anhydrase,
which is present in sera from patients with systemic lupus
erythematosus (SLE) [9]. This autoantibody is directed
against sweat glands, as well as kidney [9]. In a further
large study, the skin biopsies from 62 lupus erythematosus
patients were examined by DIF to determine the presence
of IgG, IgM, IgA and C3 among different structures of the
skin [10,12]. In addition to positive lupus band test,
autoreactivity was observed to some collagen fibers,
dermal capillaries, the basement membrane zone of
selected hair follicles, sweat glands and arrector pili
muscles [5].
As related in our case, other authors reported of a
53-year-old woman suffering with SLE with vasculitis and
overexpression of ezrin in her renal biopsy, and the
presence of a significant number of T cells in the renal
interstitial [11]. The T cells in the kidney were found to
express CD44 and phosphorylated ezrin thus accounting
for their renal homing [10]. In addition, the authors
reported that T lymphocytes in SLE display increased
levels of CD44; ERM-phosphorylation; actin polymeriza-
Letter to the Editor
tion, and chemotactic migration, when compared with T
cells in patients with rheumatoid arthritis and normal
individuals. The significance of our findings in DIF and
IHC in regards of the presence of ERM in proximity with
the affected lesions and colocalization with CD3, CD4,
and CD8, CD45, CD44 and HLA DP,DR,DQ antibodies in
addition to autoreactivity detected when using IgM
against sweat and sebaceous glands maybe indicatives
that CD44–ERM CD4, CD8, CD45 HLA DP,DR,DQ signaling
pathway may be involved in the homing of T cells to the
skin in LEP.
Conflicts of interest
None.
Acknowledgments
We would like to thank Mr. Jonathan Jones for the great
technical support at Georgia Dermatopathology Associates.
Funding sources: this work was supported by Georgia
Dermatopathology Associates, Atlanta, GA, USA.
References
[1] Y. Li, T. Harada, Y.T. Juang, V.C. Kyttaris, Y. Wang, M. Zidanic,
K. Tung, G.C. Tsokos, Phosphorylated ERM is responsible for
increased T cell polarization, adhesion, and migration in
patients with systemic lupus erythematosus, J. Immunol. 178
(2007) 1938–1947.
[2] P. Mangeat, C. Roy, M. Martin, ERM proteins in cell adhesion and
membrane dynamics, Trends Cell. Biol. 9 (1999) 187–192.
[3] S. Tsukita, S. Yonemura, S. Tsukita, ERM (ezrin/radixin/moesin)
family: from cytoskeleton to signal transduction, Curr. Biol. 9
(1997) 70–75.
[4] M.H. Shaffer, R.S. Dupree, P. Zhu, I. Saotome, R.F. Schmidt, A.I.
McClatchey, B.D. Freedman, BurkhardtJ.K. , Ezrin and moesin
function together to promote T cell activation, J. Immunol. 182
(2) (2009 Jan 15) 1021–1032.
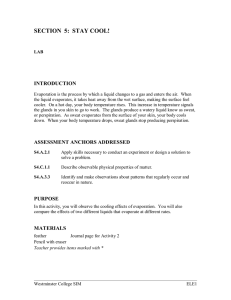
Figure 1 (a) In this Figure, are the clinical, H & E, IHC and DIF findings of LEP, with specific attention to the overexpression of {ezrin,
radixin and moesin; (ERM)} on epidermis and in the sweat glands in proximity to the LEP phenomenon. (a) An infiltrate consisting
mostly of lymphocytes and histiocytes around eccrine sweat and sebaceous glands (yellow arrows) (100×). (b) By DIF, we observed
positive immunostaining of the eccrine sweat glands, with IgG-FITC-conjugated antibodies (green) (red arrows) (400×). In c, d, g, h,
the nuclei were counterstained using Dapi (blue staining) (white arrows). (c) The DIF also showed a positive immunostaining with the
eccrine sweat glands when FITC-conjugated anti-human fibrinogen antibodies were used (green staining) (red arrows) (400×). (d) In
addition, positive staining was observed around the inflamed eccrine sweat glands when an anti-ezrin monoclonal antibody was used
at a 1:50 dilution (red staining) (dark yellow arrows). The red arrow shows positive stain of the sweat glands when using the antiserum
anti-human fibrinogen FITCI conjugated. (e) IHC shows a positive stain of CD8 cells around the sweat gland. (f) A DIF revealed the
positive lupus band test for IgA, IgG, IgM, and C3, in which all FITC-conjugated antibodies showed a linear distribution at the dermal/
epidermal junction (red arrow). In addition, some deposits by the same antibodies were seen between epidermal cells (pink arrow). (f)
Another DIF using FITC-conjugated anti-human IgA antibodies revealed deposits of IgA at the dermal/epidermal junction in a linear
pattern (red arrow). In addition, some deposits of clustered IgA were seen between several epidermal cells (pink arrow) (400×). (g) By
DIF, a strong granular circular staining (circular around the epidermal cells) was seen when FITC-conjugated anti-human-albumin
antibodies were used (yellow arrows). (h) A strongly positive ezrin was seen at all levels of the epidermis, as well as in some foci within
the superficial dermis (red) (yellow arrows) (400×). (i) H & E staining demonstrates a predominately lobular panniculitis with
infiltration of lymphocytes and histiocytes in the deep dermis (yellow arrow). In addition, there is a lobular panniculitis with a dense
infiltrate of lymphocytes, plasma cells, and macrophages. Focal hyalinization of the adipocytes is present. (j and k) Positive CD45 and
CD8 cells around the panniculitis. (l) A clinical picture of the panniculitis.
Author's personal copy
Letter to the Editor
423
Figure 2 IHC of the skin. The red arrows show positivity as following: (a) Positive IgM around the sweat glands. (b) Positive CD44
around the sweat glands (colocalizing with the ezrin overexpression), as well as in some superficial vessels. (c) CD45 positive cells were
seen around the superficial vessels. (e) H & E lymphohistocityc infiltrated around the sweat glands (blue arrow) and under them (white
arrow). (f) Positive IHC staining of the same lymphohistocityc inflammatory using anti-human IgM antibody. (g and h) CD8 and CD4,
respectively positive in the deep panniculus surrounding the sweat glands and their ductus. (i) HLA DP,DR,DQ positive in the
lymphohistocityc infiltrated above the panniculitis. (j) Positive staining around the sweat (white arrow) and the sebaceous glands (red
arrows) with IgM by IHC. (k and l) IgM positive around the pilosebaceous complex. and on the panniculitis respectively.
Author's personal copy
424
[5] P. Mrass, I. Kinjyo, L.G. Ng, S.L. Reiner, E. Puré, W. Weninger,
CD44 mediates successful interstitial navigation by killer T cells
and enables efficient antitumor immunity, Immunity 29 (6)
(2008 Dec) 971–985.
[6] C. Massone, K. Kodama, W. Salmhofer, R. Abe, H. Shimizu,
A. Parodi, H. Kerl, L. Cerroni, Lupus erythematosus
panniculitis (lupus profundus): clinical, histopathological, and
molecular analysis of nine cases, J. Cutan. Pathol. 6 (2005)
396–404.
[7] M.B. Wimmershoff, U. Hohenleutner, M. Landthaler, Discoid
lupus erythematosus and lupus profundus in childhood: a report
of two cases, Pediatr. Dermatol. 2 (2003) 140–145.
[8] D.W. Lienesch, D.F. Mutasim, R.R. Singh, Neutrophilic eccrine
hidradenitis mimicking cutaneous vasculitis in a lupus patient:
a complication of cyclophosphamide, Lupus 9 (2003) 707–709.
[9] Y. Inagaki, Y. Jinno-Yoshida, Y. Hamasaki, H. Ueki, A novel
autoantibody reactive with carbonic anhydrase in sera from
patients with systemic lupus erythematosus and Sjögren's
syndrome, J. Dermatol. Sci. 3 (1991) 147–154.
[10] J.F. Honeyman Mauro, A. Robles Velasco, Direct immunofluorescence in cutaneous lupus erythematosus, Med. Cutan.
Ibero. Lat. Am. 1 (1976) 41–44.
[11] R.A. Cohen, G. Bayliss, J.C. Crispin, G.F. Kane-Wanger, C.A. Van
Beek, V.C. Kyttaris, I. Avalos, C.Y. Yu, G.C. Tsokos, I.E. Stillman,
Letter to the Editor
T cells and in situ cryoglobulin deposition in the pathogenesis of
lupus nephritis, Clin. Immunol. 1 (2008) 1–7.
[12] V. Riccieri, A.S. Scavalli, A. Spadaro, E. Taccari, A. Zoppini,
Lupus erythematosus panniculitis: an immunohistochemical
study, Clin. Rheumatol. 13 (1994) 641–644.
Ana Maria Abreu-Velez*
Michael S.Howard
Georgia Dermatopathology Associates, 1534 North
Decatur Rd. NE; Suite 206, Atlanta,
GA 30307-1000, USA
⁎ Corresponding author. Fax: +1 404 8764897.
E-mail address: abreuvelez@yahoo.com.
Anne M. Loebl
Department of Dermatolology,
Medical College of Georgia, Augusta, GA and
Dermatology Centre of Augusta, Augusta, GA, USA
4 May 2009