Comparison of Gene Delivery Techniques for Therapeutic

Journal of the American College of Cardiology
© 2009 by the American College of Cardiology Foundation
Published by Elsevier Inc.
PRE-CLINICAL RESEARCH
Vol. 54, No. 18, 2009
ISSN 0735-1097/09/$36.00
doi:10.1016/j.jacc.2009.07.023
Comparison of Gene Delivery
Techniques for Therapeutic Angiogenesis
Ultrasound-Mediated Destruction of Carrier
Microbubbles Versus Direct Intramuscular Injection
Jeremy Kobulnik, MD,* Michael A. Kuliszewski, BS
C
,* Duncan J. Stewart, MD,*
Jonathan R. Lindner, MD,† Howard Leong-Poi, MD*
Toronto, Ontario, Canada; and Portland, Oregon
Objectives
Background
Methods
Results
Conclusions
This study was designed to compare the efficacy of angiogenic gene delivery by ultrasound-mediated (UM) destruction of intravenous carrier microbubbles to direct intramuscular (IM) injections.
Current trials of gene therapy for angiogenesis remain limited by suboptimal, invasive delivery techniques.
Hind-limb ischemia was produced by iliac artery ligation in 99 rats. In 32 rats, UM delivery of green fluorescent protein (GFP)/vascular endothelial growth factor-165 (VEGF
165
) plasmid deoxyribonucleic acid was performed.
Thirty-five animals received IM injections of VEGF
165
/GFP plasmid. Remaining rats received no treatment. Before delivery (day 14 after ligation) and at days 17, 21, and 28 and week 8 after ligation, microvascular blood volume and microvascular blood flow to the proximal hind limbs were assessed by contrast-enhanced ultrasound
(n
⫽
8 per group). Total transfection was assessed by reverse transcriptase–polymerase chain reaction, and localization of transfection was determined by immunohistochemistry.
By day 28, both IM and UM delivery of VEGF
165 produced significant increases in microvascular blood volume and microvascular blood flow. Whereas increases in microvascular blood volume were similar between treatment groups, microvascular blood flow was greater (p
⬍
0.005) in UM-treated animals as compared with IMtreated animals, persisting to week 8. The VEGF
165
/GFP messenger ribonucleic acid expression was greater
(p
⬍
0.05) for IM-treated animals. A strong GFP signal was detected for both groups and was localized to focal perivascular regions and myocytes around injection sites for IM and to the vascular endothelium of arterioles/ capillaries in a wider distribution for UM delivery.
Despite lower transfection levels, UM delivery of VEGF
165 is as effective as IM injections. The UM delivery results in directed vascular transfection over a wider distribution, which may account for the more efficient angiogenesis.
(J Am Coll Cardiol 2009;54:1735–42) © 2009 by the American College of Cardiology Foundation
Over the past 2 decades, there have been numerous clinical trials designed to promote new vessel growth by proangiogenic gene delivery in patients with refractory symptomatic coronary artery disease and peripheral arterial dis-
From the *Division of Cardiology, Keenan Research Centre in the Li Ka Shing
Knowledge Institute, St. Michael’s Hospital, Toronto, Ontario, Canada; and the
†Cardiovascular Division, Oregon Health & Science University, Portland, Oregon.
Supported by an operating grant (FRN 62763) from the Canadian Institutes of Health
Research, Ottawa, Ontario, Canada, and an equipment grant from the Canadian
Foundation for Innovation, Ottawa, Ontario, Canada. Dr. Lindner is supported by grants (R01-HL-074443, R01-HL-078610, R01-DK-063508) from the National
Institutes of Health, Bethesda, Maryland, and has served on the scientific advisory board for Visual Sonics. Dr. Leong-Poi is supported by a New Investigator Award from the Canadian Institutes of Health Research, Ottawa, Ontario, Canada, and an Early
Researcher Award from the Ministry of Research and Innovation, Ontario, Canada.
Manuscript received May 10, 2009; revised manuscript received July 6, 2009, accepted July 6, 2009.
ease ( 1 ). Whereas initial small open-labeled trials yielded
promising results, subsequent larger double-blind, randomized, placebo-controlled, clinical trials have failed to show
significant clinical benefits ( 2,3 ). The largely disappointing
results of clinical trials of therapeutic angiogenesis may in
part be explained by suboptimal delivery techniques ( 4,5 ),
involving either intra-arterial or direct intramuscular injection.
Intra-arterial delivery of genes is largely ineffective and
the inability to target specific cell types, the localized nature of transfection in proximity to injection sites, and the impracticality for repeated delivery into tissues such as the heart. The ability to noninvasively deliver genetic material to specific target tissues, such as the vascular endothelium,
Downloaded From: https://content.onlinejacc.org/ on 10/02/2016
1736 Kobulnik et al.
Ultrasound-Mediated Versus IM Gene Delivery for Angiogenesis
JACC Vol. 54, No. 18, 2009
October 27, 2009:1735– 42
Abbreviations and Acronyms
CEU ⴝ contrast-enhanced ultrasound
DNA ⴝ deoxyribonucleic acid
GFP ⴝ green fluorescent protein
FMA ⴝ fluorescent microangiography
IM ⴝ intramuscular
MBF ⴝ microvascular blood flow
MBV ⴝ microvascular blood volume
PBS ⴝ phosphate buffered saline
RNA ⴝ ribonucleic acid in a controlled manner would be an important step toward a safe and effective pro-angiogenic gene therapy.
Ultrasound-mediated (UM) destruction of intravenously administered deoxyribonucleic acid
(DNA)-bearing carrier microbubbles during their microcirculatory transit has been used to amplify transfection of reporter
plasmid DNA to skeletal ( 7 ) and cardiac muscle ( 8 ). We have pre-
viously demonstrated that UM destruction of microbubbles bearing vascular endothelial growth factor-165 (VEGF
165
) plasmid
DNA results in enhanced trans-
UM ⴝ ultrasound-mediated
VEGF ⴝ vascular endothelial growth factor fection of the vascular endothelium and improved tissue perfusion in chronically ischemic
skeletal muscle ( 9 ). The aim of our
present study was to compare gene delivery by ultrasonic destruction of intravenous VEGF
165 plasmid-bearing microbubbles to direct intramuscular (IM) injections, for therapeutic angiogenesis. The study was designed to test whether in the context of reduced limb blood flow, this vascular-based strategy would be superior to standard, but more invasive, direct IM injections, and whether the neovascularization response could be explained by the differences in the localization of gene transfection between delivery methods.
Methods
Microbubble and DNA preparation.
Plasmid DNA was charge-coupled to cationic lipid microbubbles as previously
described ( 7,9 ). For perfusion imaging, lipid-shelled deca-
fluorobutane microbubbles were used. Microbubble concentrations were determined using a Coulter Multisizer IIe
(Beckman Coulter, Fullerton, California). A bicistronic plasmid vector was constructed for the cotransfection of both enhanced green fluorescent protein (GFP) and human
VEGF
165
Animal preparation.
The study protocol was approved by the Animal Care and Use Committee at St. Michael’s
Hospital Research Centre, University of Toronto. Proximal hind-limb ischemia was produced in 99 Sprague-Dawley rats. Rats were anesthetized with intraperitoneal injection of ketamine hydrochloride (10 mg·kg mg·kg
⫺ 1
⫺ 1 ) and xylazine (8
). Under sterile conditions, the left common iliac artery and small proximal branches were exposed and ligated with 4-0 sutures. The incision was closed in layers and animals were recovered.
Perfusion imaging.
Contrast-enhanced ultrasound (CEU) imaging of the proximal hind-limb adductor muscles was
performed as previously described ( 9 ), to obtain perfusion
data on microvascular blood volume (MBV), velocity, and
microvascular blood flow (MBF) ( 9 ).
Gene delivery.
For ultrasound-mediated (UM) gene delivery, cationic microbubbles (1 ⫻ 10 9 ) coupled with 500 g of complementary DNA were infused intravenously during ultrasound transmission (Sonos 5500, Philips Healthcare,
Andover, Massachusetts) at 1.3 MHz and a transmit power
of 0.9 W, using a pulsing interval of 5 s ( 9 ). At these
settings, peak negative acoustic pressure by needle hydrophone (PVDF-Z44, Specialty Engineering Associates,
Sunnyvale, California) was calculated to be –2,100 kPa
(assuming a tissue attenuation coefficient of 0.3 dB/cm/
MHz, at tissue depth of 1 cm). For IM gene delivery, 500
g of VEGF
165
/GFP plasmid DNA was injected directly into the ischemic hind-limb adductor muscle at 5 evenly spaced sites spanning the length and width of the proximal adductor muscle, using a 24-gauge needle. This resulted in a mean distance between injection sites of 5 mm. In a subset of animals (n ⫽ 3), plasmid DNA was admixed with 10 m red fluorescent beads (100,000 beads/injection) before IM delivery, to allow for localization of transfection in relation to site of IM injection.
Fluorescent microangiography.
Immediately before sacrifice, the distal hind-limbs were flushed with heparinized saline via an abdominal aortic cannula. A 10% solution of fluorescent microspheres (0.2
m) (Sigma-Aldrich, St.
Louis, Missouri) mixed with a 1% solution of low melting point agarose at 45 o C was injected at constant rate into the aortic cannula until seen on venous return. The animal was euthanized and placed in an ice bath to facilitate cooling and solidification of the casting agent. Hind-limb tissue was placed in 10% buffered formalin, sectioned (200 m) using a vibratome and visualized under confocal microscopy. A series of stacked images (4 m slices) were taken and the middle 25 slices (100 m total thickness) were projected to quantify the vessel density using automated software (IPTK analysis soft-
ware, Reindeer Graphics Inc., Asheville, North Carolina) ( 9 ).
Immunohistochemistry.
In vivo transfection efficacy and spatial localization was determined using immunohistochemistry. Explanted tissue was cryoembedded in optical cutting temperature compound (Sakura Finetek Japan, Tokyo, Japan) and stored at – 80 o C. Cryo-blocks were sectioned (15 m thick) every 25 m and rehydrated in phosphate buffered saline (PBS), fixed in 2% paraformaldehyde (Sigma-Aldrich) in PBS, and washed with PBS. Cell surface antigens were identified using mouse antihuman
CD31 (Alpha Diagnostics Inc., San Antonio, Texas), mouse antihuman Tie-2 (Clone Ab33, Upstate Biotechnology, Milford, Massachusetts), and mouse antihuman
Alpha-actin (Sigma-Aldrich). The presence of antibody was confirmed by exposure to a phycoerythrin conjugated secondary antibody. TO-PRO-3 (Invitrogen, Burlington, Ontario, Canada) was used as a nuclear marker.
To better assess regional distribution, tissue was prepared and sectioned as described earlier and visualized under
Downloaded From: https://content.onlinejacc.org/ on 10/02/2016
JACC Vol. 54, No. 18, 2009
October 27, 2009:1735– 42
Kobulnik et al.
Ultrasound-Mediated Versus IM Gene Delivery for Angiogenesis
1737 fluorescent microscopy for VEGF/GFP signal. Hind-limb skeletal muscle was divided into a 10 ⫻ 10 grid (using 20 ⫻ high power fields) and every other field was scored for the presence of GFP signal (checkerboard grid with a total of 25 scored fields). Fields were deemed positive if clear GFP signal was detectable, and the number of positive fields (out of 25) was recorded.
To assess spatial localization in relation to site of IM injection, tissue was prepared and sectioned as described previously. Sections were visualized under low-magnification confocal microscopy and injection sites were identified by the presence of 10 m red fluorescent beads, which remained adjacent to the site of IM injection. Four adjacent low power fields were taken with the same confocal settings and recompiled to illustrate one contiguous image of GFP transfection in relation to the red fluorescent beads that mark the injection site.
Reverse transcriptase–polymerase chain reaction.
Semiquantitative real-time reverse transcriptase–polymerase chain reaction for exogenous VEGF
165
/GFP transcript was
performed on hind-limb tissue, as previously described ( 9 ).
Briefly, tissue samples were harvested, flash frozen in liquid nitrogen, and stored at –80 o C until processing. Messenger ribonucleic acid (RNA) was isolated using the Aurum total
RNA kit (Bio-Rad Laboratories, Mississauga, Ontario), which utilizes deoxyribonuclease to ensure no plasmid DNA contamination in the final product. Because, a bicistronic vector was used to deliver VEGF
165
/GFP, the following primers were used to assay for exogenous transgene expression: forward
5 = -ACGTAAACGGCCACAAGTTC-3 = and reverse 5 = -
AAGTCGTGCTGCTTCATGTG-3 = .
Experimental protocol.
Contrast-enhanced ultrasound perfusion imaging of the ischemic and contralateral control hind-limb adductor muscles was performed 14 days after ligation. Gene delivery was then performed, according to assigned treatment groups: group 1—intramuscular injection of VEGF
165
/GFP plasmid (IM); group 2— ultrasound mediated VEGF
165
/GFP plasmid microbubble delivery
(UM); and group 3—control group, no treatment (n ⫽ 32 per group). Then, CEU imaging was performed at days 17, 21, and 28 and 8 weeks after ligation (n ⫽ 8 per group). In 4 rats per group (days 28 and week 8), FMA was performed before sacrifice. An additional 3 rats underwent intramuscular injections of VEGF
165
/GFP plasmid mixed with red fluorescent beads and sacrificed 3 days later for determination of localization of GFP transfection in relation to the site of IM injections.
Tissue for immunohistochemistry and reverse transcriptase– polymerase chain reaction was obtained from the remaining rats’ ischemic and nonischemic hind limbs.
Statistical methods.
All data are expressed as mean ⫾ SD.
Comparisons between groups at multiple stages were performed by 2-way analysis of variance; if significant, Bonferroni correction for multiple comparisons was applied when post-hoc analysis between different time points or between different groups at the same time point was performed
(GraphPad Prism version 5.0a, GraphPad Software Inc., La
6000
4000
2000
0 day 17 day 21 day 28 week 8
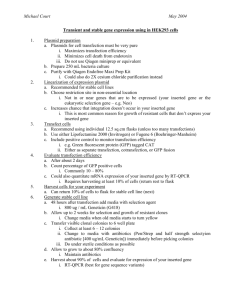
Figure 1
Exogenous VEGF
165
/GFP mRNA Transcript Following Ligation
Real-time reverse transcriptase–polymerase chain reaction data showing exogenous vascular endothelial growth factor-165 (VEGF
165
)/green fluorescent protein (GFP) messenger ribonucleic acid (mRNA) transcript at days 17, 21, and
28 and week 8 after ligation (intramuscular [IM] gene therapy in solid bars , ultrasound-mediated [UM] therapy in open bars ). Relative VEGF
165
/GFP mRNA expression was significantly lower for UM delivery compared with IM delivery at all time points after delivery. *p ⬍ 0.05 compared with IM gene therapy.
Jolla, California). Statistical significance between 2 groups was determined by 2-tailed unpaired t tests. Differences were considered significant at p ⬍ 0.05 (2-sided).
Results
Comparison of transgene expression.
Real-time reverse transcriptase–polymerase chain reaction data for exogenous
VEGF
165
/GFP messenger RNA at various time points after delivery are shown in
Figure 1 . Using specific primers,
robust exogenous transgene expression (normalized to the contralateral nonischemic muscle) was detected in both IMand UM-treated ischemic muscles and was undetectable in control untreated animals. For both treatment groups, transfection was greatest at day 3 following delivery (day 17 after ligation), decreasing over time. The IM delivery resulted in significantly greater transfection compared with the UM delivery at all early time points, with transgene expression diminishing in both treatment groups by week 8
Muscle perfusion and vascular density.
At 2 weeks after iliac artery ligation, immediately before gene delivery, mean
MBV and MBF in the ischemic leg was reduced to ⬃ 35%
of the normal leg in all 3 groups ( Fig. 2 ). In the control
group, there was no change in normalized MBV and MBF
over time ( Fig. 2 ). With IM therapy, there was a significant
increase in normalized MBV that began at day 17 following ligation, reaching a plateau at days 21 and 28, and waning by week 8. Whereas MBV increased early in IM-treated ischemic muscle, significant increases in MBF were not seen until day 28. In comparison, the improvement in perfusion with UM therapy was more delayed, with normalized MBV and MBF peaking at 28 days after ligation (14 days following gene delivery), and persisting to 8 weeks after
ligation ( Fig. 2 ). When compared with IM therapy, UM
Downloaded From: https://content.onlinejacc.org/ on 10/02/2016
1738 Kobulnik et al.
Ultrasound-Mediated Versus IM Gene Delivery for Angiogenesis
JACC Vol. 54, No. 18, 2009
October 27, 2009:1735– 42 therapy yielded a significantly greater improvement in normalized MBF than with IM therapy. This superior therapeutic effect of UM gene delivery was seen at 28 days after
ligation and persisted out to week 8 ( Fig. 2 ). Fluorescent
microangiography analysis revealed reduced vessel density in the control group’s ischemic muscle 4 weeks after iliac artery ligation. Consistent with CEU perfusion data, at 14 days after gene delivery, there were increases in vessel density both in the IM and UM groups that mirrored changes in
MBV. Whereas changes in MBF at day 28 were significantly greater for UM, as compared with IM, therapy, changes in both MBV and vessel density by FMA at day 28 between UM- and IM-treated animals were not signifi-
and
Localization of gene transfection.
There was no discernable GFP signal detected in the ischemic muscle of the untreated control group. In comparison, a robust GFP signal was detected in both IM- and UM-treated groups by fluorescent confocal microscopy. Whereas IM gene delivery resulted in focal regions of bright GFP signal predominantly within regions adjacent to IM injection sites, UM-treated muscle showed a more diffuse signal with a significantly
greater number of microscopic fields expressing GFP ( Fig. 4 ).
For IM delivery, immunohistochemical staining revealed focal
Figure 2 MBV and MBF in the Ischemic Muscle for 3 Treatment Groups
(A) Normalized microvascular blood volume (MBV) in the ischemic muscle for the 3 treatment groups at baseline (pre-treatment) and days 17, 21, and 28 and week 8 after ligation. *p
⬍
0.005 compared with corresponding data in control untreated animals, †p
⬍
0.05 compared with corresponding data in IM-treated animals, ‡p
⬍
0.001 compared with corresponding baseline (pre-delivery) data.
(B) Normalized microvascular blood flow (MBF) in the ischemic muscle for the 3 treatment groups at baseline (pre-treatment) and at days 17, 21, and 28 and week 8 after ligation. *p
⬍
0.01 compared with corresponding data in control untreated animals; †p
⬍
0.005
compared with corresponding data in IM-treated animals; ‡p
⬍
0.05 compared with corresponding baseline (pre-delivery) data. Abbreviations as in
Downloaded From: https://content.onlinejacc.org/ on 10/02/2016
JACC Vol. 54, No. 18, 2009
October 27, 2009:1735– 42
Kobulnik et al.
Ultrasound-Mediated Versus IM Gene Delivery for Angiogenesis
1739 areas of colocalization of GFP predominantly within myocytes, with some signal from surrounding capillaries and interstitial
cells of the ischemic adductor muscle ( Fig. 5 ) and little to no
signal from arterioles or venules. In UM-treated muscle, the
GFP signal was predominantly associated with the vascular endothelium of small- and medium-sized arterioles within the ischemic adductor muscle, with signal also detected within
capillaries and extending to surrounding myocytes ( Fig. 5 ).
Discussion
Currently, the most effective strategy for delivering angiogenic genes to induce clinically important therapeutic neovascularization within ischemic muscle is unknown. We have previously demonstrated the potential of UM destruction of VEGF
165 plasmid-bearing microbubbles for improving tissue perfusion in the setting of severe chronic hindlimb ischemia (9). The aim of our present study was to directly compare this noninvasive technique for gene delivery to the current standard delivery method of direct IM injection. We have now demonstrated that despite lower total transfection, the strategy of UM gene delivery produces a pattern of gene expression that may be more efficacious compared with direct intramuscular injections for the induction of therapeutic angiogenesis in ischemic skeletal muscle. This finding could potentially lead to the development of newer, more effective and noninvasive methods of gene delivery for therapeutic angiogenesis in patients, one that could be used to test multiple and repetitive gene therapies in clinical trials.
Gene delivery strategies for angiogenesis.
Initial strategies for transcatheter delivery of angiogenic genes have used an intracoronary route, which is limited by imprecise localization of genes and the potential for systemic delivery to noncardiac tissue. In addition, transfection efficiency is poor
( 10 ), in part due to poor retention and rapid clearance by
circulating deoxyribonucleases. For this reason, catheterbased techniques for transendocardial injections have been
nique. Whereas IM delivery has advantages including the
A B C
D E F
G
Figure 3 Microvessel Density by FMA in 3 Groups
(A to F) Representative stacked images of microvessels in ischemic hind-limb muscle after no treatment and IM and UM delivery of VEGF
165
/GFP plasmid deoxyribonucleic acid, using fluorescent microangiography (FMA). Scale bar
⫽
50
m.
(G) Quantitative microvessel density by FMA of ischemic hind-limb muscle at day 28 and week
8 following ligation, in all groups. At day 28 after ligation, FMA revealed a significant increase in the density of microvessels in the ischemic leg of both IM- and
UM-treated animals, as compared with control untreated animals, with a trend for greater vessel density in UM-treated ischemic muscle. *p
⬍
0.05 compared with corresponding data from control ischemic muscle. Abbreviations as in
Downloaded From: https://content.onlinejacc.org/ on 10/02/2016
1740 Kobulnik et al.
Ultrasound-Mediated Versus IM Gene Delivery for Angiogenesis
A B
JACC Vol. 54, No. 18, 2009
October 27, 2009:1735– 42
C
Figure 4 Transgene Expression After IM Delivery
Focality of transgene expression after IM delivery. The IM injection sites were marked with fluorescent microspheres (A, single white arrow) and GFP expression assessed in adjacent fields at day 3 following injection. Strong GFP signal is seen in close proximity to injection sites (A, double white arrows) , declining with increasing distance from the needle tract. Remote hind-limb muscle is shown in B where there is minimal GFP expression.
C shows the number of high power (20
⫻
) fields (out of
25) positive for GFP signal in IM- and UM-treated ischemic skeletal muscle. *p
⬍
0.05 compared with corresponding data from IM-treated muscle. IV
⫽ intravenous; U/S
⫽ ultrasound; other abbreviations as in
delivery of most of the genetic material directly into target tissue with minimal systemic effects, this method is invasive, especially as it pertains to cardiac delivery. Even though the
risk of serious complications is relatively low ( 11 ), repeated
deliveries have not been studied in clinical trials and will remain a limitation of this technique.
A noninvasive strategy for gene delivery by the ultrasonic destruction of plasmid-bearing microbubbles has been developed that results in targeted transfection and therapeutic effects in many tissues, including skeletal and cardiac muscle, without delivery to remote nontargeted organs. If effective and safe, such a strategy could become the technique of choice for repeated gene deliveries to any organ accessible to ultrasound. Only a few studies have compared the efficacy of UM gene delivery to standard direct IM
injection. Christiansen et al. ( 7 ) compared the efficacy of
ultrasonic destruction of intravenous or intra-arterial injections of luciferase-reporter plasmid DNA-bound microbubbles to direct IM injections into normal skeletal muscle.
Whereas luciferase activity was similar between animals treated with IM and intra-arterial microbubble delivery, they found 100-fold greater luciferase activity in skeletal muscle with IM delivery, as compared with intravenous UM
delivery. Similarly Pislaru et al. ( 13 ) demonstrated similar
luciferase activity in rat skeletal muscle treated with IM plasmid compared with intra-arterial UM delivery; however, they did not assess intravenous UM delivery.
Our study is the first to directly compare IM delivery to
UM destruction of plasmid DNA-bearing microbubbles, using a “functional” gene, namely VEGF
165
. At first glance, it does not seem a fair comparison, with transfection efficiency by real-time polymerase chain reaction demonstrating an 8- to 10-fold greater messenger RNA expression for IM delivery as compared with intravenous UM delivery.
The magnitude of the difference is similar to that published with reporter genes. This is not surprising given the large discrepancy in total DNA dose delivered, with nearly 100% delivered for IM injection compared with a much lesser fraction for UM delivery. Ultrasound-mediated delivery is a method of targeted intravascular gene delivery that is reliant entirely on local tissue perfusion, whereby transfection is targeted to the vascular endothelium and adjacent perivascular tissues by external ultrasound application. Whereas
100% of the DNA is administered intravenously, due to low blood flow in noncontracting skeletal muscle coupled with marked flow reduction due to iliac artery ligation, only a small fraction, ⬃ 10%, will enter the ischemic hind limb where it can be delivered. To maximize delivery, we used longer pulsing intervals to allow microbubble replenishment into tissue between destructive ultrasound pulses, a high
Downloaded From: https://content.onlinejacc.org/ on 10/02/2016
JACC Vol. 54, No. 18, 2009
October 27, 2009:1735– 42
A
B
C
Kobulnik et al.
Ultrasound-Mediated Versus IM Gene Delivery for Angiogenesis
1741
D
E
F
Figure 5 Immunofluorescent Staining of IM- and UM-Treated Ischemic Muscle
Examples of immunofluorescent staining of IM-treated (A to C) and UM-treated (D to F) ischemic muscle, at day 17 after ligation.
Red
⫽
CD31 staining; blue
⫽ nuclear staining (TO-PRO-3); yellow ⫽ colocalization of GFP and red CD31 staining. Within IM-treated muscle, there were areas without discernable GFP signal (A, yellow arrows) , interspersed with regions of strong GFP signal localized predominantly within myocytes (B, white arrows) and surrounding capillaries, with little GFP signal within arterioles (C, red arrows) . In comparison, within UM-treated muscle, a more diffuse GFP signal was seen, localized to the vascular endothelium of both capillaries
(D, yellow arrows) , their surrounding myocytes (E, white arrows) , and within small- to medium-sized arterioles (F, red arrows) . Scale bar
⫽
50
m. Abbreviations as in
acoustic power and low frequency ( 14 ), and prolonged the
ultrasound delivery time. Using a continuous infusion of
DNA-bearing microbubbles, a steady local concentration within the vascular bed is maintained, and repeated application of intermittent high-power ultrasound during the infusion allows for continuous gene delivery as the microbubbles recirculate through the systemic circulation. By scanning along the length of the hind-limb adductor muscles, we were able to deliver plasmid DNA to the entire proximal ischemic bed, resulting in a wider field of delivery.
Finally, by continuing ultrasonic destruction for 10 min after completion of microbubble-DNA infusion, we allowed additional delivery of any remaining circulating DNAbearing microbubbles that had not been delivered.
Localization of gene transfection: importance for angiogenesis.
Despite substantially lower transgene expression,
UM delivery resulted in a similar angiogenic effect, by both
CEU perfusion imaging and by fluorescent microangiography. Changes in microvascular blood volume were noted earlier with IM gene therapy, suggesting a more rapid onset of angiogenesis in keeping with substantially greater VEGF transgene expression. However, although maximal changes in vessel density by FMA and MBV by CEU were similar in both IM- and UM-treated ischemic muscle, the increase in MBF, arguably a more functional end point, was greater for UM gene therapy. The discordance between marked increases in MBV and more modest changes in MBF in
IM-treated ischemic muscle bears similarity to the neovasculature within highly vascularized tumors, whereby CEU blood volume is greater than surrounding normal tissue; however, due to immature and tortuous vessels, blood velocity is low leading to proportionately lower MBF
( 15,16 ). This novel observation suggests that UM delivery
may have a greater “biologic” response than IM delivery, resulting in a more functional neovasculature despite lower transfection rates. The use of a bicistronic vector encoding for VEGF
165 and a marker gene, enhanced GFP, allowed us to compare the localization of gene transfection by both
UM and IM delivery. Ultrasound-mediated gene therapy produced a more diffuse pattern of transfection and was localized to the vascular endothelium of medium to small arterioles and capillaries, with adjacent myocyte transfection
Downloaded From: https://content.onlinejacc.org/ on 10/02/2016
1742 Kobulnik et al.
Ultrasound-Mediated Versus IM Gene Delivery for Angiogenesis
JACC Vol. 54, No. 18, 2009
October 27, 2009:1735– 42 likely via the surrounding microvasculature. In contrast, IM delivery resulted in more focal pockets of transfection, interspersed with areas of no transfection. Areas of highest transfection were localized to IM injection sites, with a decreasing gradient of transfection with distance from the needle track.
The GFP/VEGF transfection was localized predominantly to myocytes, along with adjacent capillaries, with minimal to no arteriolar transfection. The latter finding is in keeping with
data from Gal et al. ( 17 ), who used in situ hybridization to
show that myocytes represented the site of luciferase expression after IM injections of firefly luciferase-reporter gene into skeletal muscle in rabbits. Thus, our study demonstrates that a strategy of intravascular gene therapy that enhances transfection to the vascular endothelium of arterioles and capillaries in a wider, more diffuse pattern is more effective than one that predominantly targets myocytes, along with adjacent capillaries, in a more focal distribution.
Study limitations.
For controls, we only studied animals that received no treatment. Ideally, controls should also include groups with: 1) ultrasound alone at the same dosimetry; 2) microbubbles bearing VEGF
165 plasmid
DNA alone; and 3) ultrasound and microbubbles bearing control plasmid DNA. We have previously demonstrated that
UM delivery of microbubbles bearing GFP plasmid DNA as a microbubble-control plasmid DNA treated group yielded no significant improvement in MBF over time and was similar to
control animals that received no treatment ( 9 ).
Conclusions
In summary, despite lower transgene expression, UM microbubble destruction of VEGF
165 may be more effective than direct IM delivery. Ultrasound-mediated delivery results in directed vascular transfection over a wider distribution as compared with IM delivery, which predominantly transfects myocytes and surrounding capillaries. This difference in the localization of gene transfection likely accounts for the more efficient angiogenesis seen with UM delivery of
DNA-bearing microbubbles and highlights the importance of the site of transfection in optimizing gene delivery strategies for therapeutic angiogenesis.
Reprint requests and correspondence: Dr. Howard Leong-Poi,
7-052 Bond Wing, St. Michael’s Hospital, 30 Bond Street,
Toronto, Ontario M5B 1W8, Canada. E-mail: leong-poih@smh.
toronto.on.ca
.
REFERENCES
1. Vincent KA, Jiang C, Boltje I, Kelly RA. Gene therapy progress and prospects: therapeutic angiogenesis for ischemic cardiovascular disease.
Gene Ther 2007;14:781–9.
2. Grines CL, Watkins MW, Helmer G, et al. Angiogenic Gene
Therapy (AGENT) trial in patients with stable angina pectoris.
Circulation 2002;105:1291–7.
3. Henry TD, Annex BH, McKendall GR, et al., on behalf of VIVA
Investigators. The VIVA trial: Vascular endothelial growth factor in
Ischemia for Vascular Angiogenesis. Circulation 2003;107:1359 – 65.
4. Simons M, Bonow RO, Chronos NA, et al. Clinical trials in coronary angiogenesis: issues, problems, consensus: an expert panel summary.
Circulation 2000;102:E73– 86.
5. Simons M. Angiogenesis: where do we stand now? Circulation
2005;111:1556 – 66.
6. Kornowski R, Fuchs S, Leon MB, Epstein SE. Delivery strategies to achieve therapeutic myocardial angiogenesis. Circulation 2000;101:
454 – 8.
7. Christiansen JP, French BA, Klibanov AL, Kaul S, Lindner JR. Targeted tissue transfection with ultrasound destruction of plasmid-bearing cationic microbubbles. Ultrasound Med Biol 2003;29:1759–67.
8. Shohet RV, Chen S, Zhou YT, et al. Echocardiographic destruction of albumin microbubbles directs gene delivery to the myocardium.
Circulation 2000;101:2554 – 6.
9. Leong-Poi H, Kuliszewski MA, Lekas M, et al. Therapeutic arteriogenesis by ultrasound-mediated VEGF165 plasmid gene delivery to chronically ischemic skeletal muscle. Circ Res 2007;101:295–303.
10. Wright MJ, Wightman LM, Latchman DS, Marber MS. In vivo myocardial gene transfer: optimization and evaluation of intracoronary gene delivery in vivo. Gene Ther 2001;8:1833–9.
11. Kastrup J, Jorgensen E, Ruck A, et al., on behalf of Euroinject One
Group. Direct intramyocardial plasmid vascular endothelial growth factor-A165 gene therapy in patients with stable severe angina pectoris. A randomized double-blind placebo-controlled study: the Euroinject One trial. J Am Coll Cardiol 2005;45:982– 8.
12. Stewart DJ, Hilton JD, Arnold JM, et al. Angiogenic gene therapy in patients with nonrevascularizable ischemic heart disease: a phase 2 randomized, controlled trial of AdVEGF(121) (AdVEGF121) versus maximum medical treatment. Gene Ther 2006;13:1503–11.
13. Pislaru SV, Pislaru C, Kinnick RR, et al. Optimization of ultrasoundmediated gene transfer: comparison of contrast agents and ultrasound modalities. Eur Heart J 2003;24:1690 – 8.
14. Chen S, Shohet RV, Bekeredjian R, Frenkel P, Grayburn PA.
Optimization of ultrasound parameters for cardiac gene delivery of adenoviral or plasmid deoxyribonucleic acid by ultrasound-targeted microbubble destruction. J Am Coll Cardiol 2003;42:301– 8.
15. Chomas JE, Pollard RE, Sadlowski AR, Griffey SM, Wisner ER,
Ferrara KW. Contrast-enhanced US of microcirculation of superficially implanted tumors in rats. Radiology 2003;229:439 – 46.
16. Ellegala DB, Leong-Poi H, Carpenter JE, et al. Imaging tumor angiogenesis with contrast ultrasound and microbubbles targeted to alpha(v)beta3. Circulation 2003;108:336 – 41.
17. Gal D, Weir L, Leclerc G, Pickering JG, Hogan J, Isner JM. Direct myocardial transfection in two animal models. Evaluation of parameters affecting gene expression and percutaneous gene delivery. Lab
Invest 1993;68:18 –25.
Key Words: angiogenesis y gene therapy y chronic ischemia.
Downloaded From: https://content.onlinejacc.org/ on 10/02/2016