Annual Report

HARYANA STATE HEALTH RESOURCE CENTRE
HSHRC-Haryana
Haryana State Health Resource Centre
Annual Report 2012-13
2013
HSHRC Annual Report 2012-13
B a y
☂ s 5 9 - 6 2 , S e c t o r - 2 , P a n c h k u l a , H a r y a n a
0
HARYANA STATE HEALTH RESOURCE CENTRE
Mrs. Navraj Sandhu, IAS
Principal Secretary Health,
Govt. of Haryana
FOREWORD
Haryana State Health Resource Centre (HSHRC) has come up very well during its first year of establishment. I wish hearty congratulations to Dr. Ashish Gupta, ED, HSHRC for successful completion of one year and on publication of its first ☜ Annual Report ☝ .
HSHRC has been technically assisting the Health Department Haryana in policy formulation, implementation, informatics, evaluation and capacity building. It has been a great asset to Health Department in areas like quality improvement of health facilities, promotion of rational use of drugs, various health related research studies, planning in health sector etc.
This report will act a source of information for Health Department and provide an insight to the activities being covered by HSHRC. I am sure that this report will be beneficial to all those persons who are indulged in carrying out similar activities in Health sector in Haryana.
I appreciate the sincere efforts made by everyone involved in the functioning of
HSHRC and in drafting of this report. I sincerely hope that HSHRC will grow and flourish even better in the years to come and will act as a valuable resource centre for the Health
Department.
Navraj Sandhu
HSHRC Annual Report 2012-13 1
HARYANA STATE HEALTH RESOURCE CENTRE
PREFACE
Dr. Ashish Gupta
Executive Director,
Haryana State Health Resource Centre
It is a matter of great pleasure and pride that Haryana State Health Resource Centre
(HSHRC) has flourished well during its first year and is making sincere efforts to address the Health related issues of the State of Haryana.
HSHRC got established in May 2012. It has a Governing Body and Executive
Committee, both of which are chaired by Principal Secretary Health, Govt. of Haryana, details of which are available on the inner pages.
HSHRC has two sets of directions. One is to work on the issues entrusted by the
Principal Secretary and stakeholders (Health Department, NRHM, NHSRC etc.) and the another is self generated by identifying lacunae in Health system proactively and come out with comments and recommendations for the same.
Haryana State Health Resource Centre (HSHRC) is an autonomous body established with an aim to become a premier technical resource and research division in public health, responsive to emerging state and national needs based on value of inclusion and quality of service delivery. There are five areas where HSHRC is currently working namely Public
Health Planning, Promotion of Rational Drug Use, Quality Assurance, Monitoring &
Evaluation and Public Private Partnership.
The Public Health Planning division is involved in planning and implementation of
Health Programs. HSHRC has also formed a High Level Task Force committee and coordinated meetings to advise and recommend corrective actions on issues like maternal
& infant mortality, anemia, malnutrition and adverse sex ratio. HSHRC provides technical support for strengthening the process of medicine and consumables, procurement, development of Standard Treatment Guideline (STG) and setting up centralized drug
HSHRC Annual Report 2012-13 2
HARYANA STATE HEALTH RESOURCE CENTRE testing unit. Under Quality Assurance division, NABH accreditation is implemented in selected public health facilities to set the standards of the quality of service delivery of the institution. HSHRC is managing the whole process of selection, collaboration, gap filling and accreditation of health facilities. HSHRC is conducting issue based research studies undertaken by M& E division to gather knowledge and evidence for policy development and modification which enable effective reach of health services to the people of Haryana.
This Annual Report is an attempt to demonstrate the performance of HSHRC during the year 2012-13 in terms of research studies, Standard Treatment Guidelines, proposals, reports, workshops etc.
I would like to thank worthy Principal Secretary Health, Govt. of Haryana, Mrs.
Navraj Sandhu, for her guidance and extensive support. I also gratefully acknowledge the support we have received from Dr. Rakesh Gupta, Mission Director, NRHM and Dr. N.K.
Arora, Director General Health Services (DGHS).
I acknowledge the support provided by Dr. Rajesh Narwal, Public Health Planning
Advisor and Ms. Jhimly Barua, Consultant Public Health Planning, NHSRC. I highly appreciate the efforts and support of all the experts of various external agencies in whose collaboration we have completed our various tasks. I am really glad by the support provided by Dr. Harpreet Sandhu, Dr. Monika Narang, Mr. Vivek Sharma, Mr. V.P.Dudeja and the entire HSHRC team for successfully achieving our goals.
I am sure that in the coming time also, our efforts will be focused on the Health related problems that our state is facing.
Dr. Ashish Gupta
HSHRC Annual Report 2012-13 3
HARYANA STATE HEALTH RESOURCE CENTRE
V
ision and
M
ission of HSHRC
Vision:
To position HSHRC as a premier technical resource and research division for meeting emerging state and national public health needs through improvement of quality of service delivery and appropriate management practices and IT tools.
Mission:
HSHRC will strive to be a centre of excellence on public health and become a technical resource centre by: a) Conducting research and generating evidence for improvement of policies b) Making health delivery system responsive and accountable through quality assurance c) Capacity building of all involved in Health sector d) Collaboration and exchange of knowledge e) Technical assistance to the department and other stakeholders
HSHRC Annual Report 2012-13 4
HARYANA STATE HEALTH RESOURCE CENTRE
S. No. CONTENT
I. Annual Work Report
PAGE No.
1.
2.
D.
E.
3.
F.
2.1
A.
B.
C.
An Introduction
Divisions of HSHRC
HSHRC Team
Public Health Planning (PHP)
Human Resource for Health
Drug Unit
Quality Improvement
Monitoring & Evaluation (M&E)
Public Private Partnership (PPP)
Workshops and Meetings
4. Other Activities of HSHRC
II. Institutional Profile
6
7
32
46
54
56
8
9
19
20
60
5.
6.
About HSHRC
Governing Body and Executive Committee
61
65
HSHRC Annual Report 2012-13 5
HARYANA STATE HEALTH RESOURCE CENTRE
I
NTRODUCTION
The first Annual Report of Haryana State Health Resource Centre (HSHRC) is an attempt to take you through the first year of our existence. HSHRC was formed by Government of
Haryana in May 2012 by a Governing Body to assist the Government in strategic planning, monitoring and evaluation of policies and programs in Health sector.
This report will inform you about the establishment of HSHRC, members and role of
Governing Body and Executive Committee. It will give you a picture of HSHRC
☂ s structure, objectives and functions. The duration of this report is from May 2012 to March 2013.
This is a progress report of HSHRC which focuses on work done on various thematic areas like evidence for policy, strategy development and Health planning, development of policy documents, quality improvement system for Health facilities and Health services, evaluation of drug procurement and rational use of drugs etc.
Most of the work reported in the following pages has been done in strategic partnership with many agencies like Quality Council of India (QCI) for quality accreditation of Health facilities, NISG for computerization of hospitals, CRY, NHSRC, IIM, PHFI for public health planning and research studies etc.
We hope that this report efficiently places HSHRC in the public domain and builds an understanding of possibilities of similar activities in the Health sector.
We sincerely look forward to an active feedback from all of our well wishers and from all those who work for strengthening public health systems to achieve our goals.
HSHRC Annual Report 2012-13 6
HARYANA STATE HEALTH RESOURCE CENTRE
D
IVISIONS of HSHRC
Haryana State Health Resource Centre (HSHRC) has been set up to provide technical support and capacity building for strengthening of district health systems and to provide support to State Health systems in program planning, strategy development and innovation.
For achieving our goal, a multi-disciplinary team is available at HSHRC with skills in medical science, public health management, quality assurance, monitoring & evaluation, operation research, human resource planning etc.
HSHRC has five divisions with their respective roles and responsibilities, which are:
I.
Public Health Planning (PHP) Division
II.
Human Resource for Health Division
III.
Drug Division
IV.
Quality Improvement Division
V.
Monitoring & Evaluation (M&E) Division
VI.
Public Private Partnership (PPP) Division
HSHRC Annual Report 2012-13 7
HARYANA STATE HEALTH RESOURCE CENTRE
H
SHRC TEAM
S. No. Name of the Employee
1 Dr. Ashish Gupta
Drug Division
2 Dr. Harpreet Kaur
3
4
5
Dr. Durbha Rohini
Ms. Uma Rani
Ms. Pooja Dhiman
Quality Division
6
7
Dr. Monika Narang
Dr. Ruchi Gupta
8 Ms. Ruchika Goyal
Monitoring &Evaluation Division
9 Mr. Vivek Sharma
10 Mr. Pratyush Kumar Bishi
11 Dr. Meenakshi Gupta
Public Health Planning (PHP) Division
12
13
14
Mr. Vivek Sharma
Dr. Manpreet Kaur
Dr. Kunal Jhanji
Dr. Puneet Khanduja
15 Dr. Asif Shafie
Public Private Partnership (PPP) Division
16 Dr. Rajeev Mehta
Administrative Unit
17
18
19
20
21
22
Mr. V.P. Dudeja
Mr. Amit Kumar
Ms. Monika Vashishtha
Mr. Manoj Mandel
Mr. Mukesh Kumar
Mr. Ajay Datta
Designation
Executive Director
MO
Consultant
Analytical Assistant
Pharmacist
MO (QA)
Consultant Q. A.
Consultant Q. A.
Senior Consultant (PHP & ME)
Special Consultant (M&E)
Consultant (Research) M&E
Senior Consultant (PHP & ME)
Consultant (PHP)
Consultant (PHP)
Consultant (PHP)
Consultant (PHP)
Consultant (PPP)
ADO/AO
Account Assistant
Computer Assistant
C.A./DEO
C.A./DEO
Driver
HSHRC Annual Report 2012-13 8
HARYANA STATE HEALTH RESOURCE CENTRE
P
UBLIC HEALTH PLANNING DIVISION
Public Health Planning is the process of defining community health problems, identifying unmet needs, surveying resources to meet them, establishing priority goals that are feasible and projecting administrative actions to accomplish the purpose of proposed programs.
A.1 Study conducted under PHP Division :
A.1.1. Workflow Study of Office of Civil Surgeon:
On a desk review it was seen that a large portion of Civil Surgeons and Deputy Civil
Surgeons
☂
time goes into reporting and fire-fighting on issues that need immediate attention instead of spending time in planning, innovation, developing and sharing best practices.
This study was conducted by HSHRC with an objective to analyze the workflow of
District level officers and of Civil Surgeon
☂ s office in districts of Haryana. It was planned to carry out a workflow analysis wherein it was planned to study the priority work of the Civil Surgeon and to map out activities of the Civil Surgeon and District
Program officers.
To begin with an in-house team of Consultants (PHP) visited 2 Districts
(Yamunanagar and Karnal) and conducted in-depth interviews elaborating the aspects of the work of District Civil Surgeons and all Deputy Civil Surgeons looking after various Health Programs at District level and the time utilization against work prioritization.
It was felt that to develop the concept further there was a need for an in-depth study into the area of organizational behavior. Thereafter collaboration was done with
Department of Organizational Behaviour (OB), IIM Ahmedabad with inputs from
School of Public Health, PGI Chandigarh and it was decided to conduct a systematic study with work-flow analysis of the district officers. Sampling of Districts was done so as to cover all the regions of the State. Visits were conducted to the sampled districts by Consultants and team members of IIM Ahmedabad for data collection.
Detail interviews were conducted with District Officers to know their work processes.
Desk review of secondary data collected from Health Department was also done. After the field visits, in depth interviews, desk review of secondary data and policy drafts, it
HSHRC Annual Report 2012-13 9
HARYANA STATE HEALTH RESOURCE CENTRE was seen that there is a great variation in the working of the civil surgeons. Role clarity was also lacking in them.
Most Civil Surgeons when asked about their main role in the system could not give a precise description of the roles and responsibilities that they are meant to discharge.
There was no uniformity in understanding of the work of a district health officer and there was also lot of variance in the tasks that different Civil Surgeons give importance to. While one Civil Surgeon spends most of the day handling reporting responsibilities another prefers to spend a lot of time in the field. Yet another chooses to remain in office and use a substantial part of the day in simply dealing with the correspondence. It also appeared that some Civil Surgeons spent a lot of time on tasks that could be effectively delegated.
Half of Civil Surgeons interviewed admitted to a deficiency in financial and administrative knowledge especially in preparation of the NRHM PIP.
Thus, professional training be provided to officers before appointment as Civil
Surgeons to give them adequate managerial, financial and program knowledge. At the same time, a clearer understanding of roles and responsibilities be provided to Civil
Surgeons with guidelines on the amount of time to be spent on each task, how to prioritize work and effectively delegate responsibilities.
A draft report is being prepared and will be submitted shortly. Results and recommendations of the study will be distributed to the stakeholders and can be put to use for making policy decisions and taking necessary actions for improving efficient working of district health administration.
A.2 Proposals prepared under PHP Division:
A.2.1. State Urban Health Mission:
Very first task assigned to HSHRC was the preparation of policy document for launch of Urban Health in Haryana. In order to develop the concept of the Urban
Health in Haryana several rounds of consultation were held with the DGHS, Dr
Narveer Singh, MD NRHM Sh. C R Rana, officer in-charge of Urban RCH, Director FW and other headquarter officers of DGHS and NRHM. Consultations were also held with the field level officers. An elaborate review of existing documents like the
Krishnan Committee report, Urban Health Task Force recommendation, study of
Calcutta project carried out by NHSHRC, Uttarkhand Urban Health experiment by
Urban Health Centre, etc and existing urban health schemes was also done. A conceptual document was presented before the Civil Surgeon conference. The final
HSHRC Annual Report 2012-13 10
HARYANA STATE HEALTH RESOURCE CENTRE document was submitted to the Govt. after inputs from the Principal Secretary,
Health. The concept was presented by the PS, Health before the CM of Haryana in presence of several departmental Secretaries connected with the issue of urban
Areas and the Urban Health Mission was formally announced by the Government in
2011.
The UHM broadly covered the following concepts: i.
To provide primary and specialized curative Health Services to the planned urban areas through Urban dispensaries and Polyclinics. ii.
In addition it envisaged the concept of providing comprehensive health services along with 24X7 maternity services and outreach services to the underserved and slum population through a UHC (Urban Health Centre). iii.
One UHC covered population of 50000 including majority of urban slum population which would be provided all public health preventive services. iv.
It was envisaged to integrate the state urban health mission with the NUHM as and when it is launched. v.
Initially it was planned to start with 11 Polyclinics and 11 UHCs.
A.2.2. Construction Worker Scheme:
After a meeting was convened by Principal Secretary, Labour, GOH for developing a comprehensive scheme for Building and other construction workers, the task for preparation of a proposal was assigned to HSHRC. The objective was to provide health coverage to the construction workers at their residence and work site and it was stated that the Haryana Building and other Construction Worker Welfare Board would be willing to finance such a project.
Construction workers are one of the most vulnerable segments of labour force . They and their families are more prone to High incidence of accidents, diarrheal diseases, tuberculosis, vector borne diseases, occupational exposure (COPD) and NCD ☂ s like diabetes and hypertension etc.
HSHRC prepared a draft proposal after discussion with officers in the Health
Directorate and presented before the Civil Surgeon conference on 19-9-12. In the proposal it was envisaged that comprehensive Health services will be provided to building and other construction workers at place of their residence through by opening Urban Health Centres, and at workplace through Urban Mobile Medical
Units (UMMU) that will provide all services of a small PHC, ambulance services for emergency cases, treatment at district hospitals and free treatment at tertiary
HSHRC Annual Report 2012-13 11
HARYANA STATE HEALTH RESOURCE CENTRE hospitals. Funding was approved by Labor Department and HSHRC would provide technical assistance as and when needed.
A.2.3 Proposals made for the Studies to be awarded to Institutions for
Research and development scheme (Brain Storming meeting):
In the meeting of Chief Secretary it was proposed to outsource certain studies which have an impact on citizen services to professional research agencies. HSHRC coordinated the preparation of the research proposals with NRHM and Directorate and the following proposals were prepared and submitted to the Govt.
A.2.3.1
A study on household expenditure in health care, its impact on socio-economic status and health seeking behavior and expectation of citizens from health dept. in
Haryana.
A.2.3.2
A study towards attitude, quality consciousness, professional management and training needs of health facility staff to meet the needs of service seekers.
A.2.3.3
A study on access of health services for urban slum population in Haryana (Reach to the present infrastructure, cost to patient and kind of services available, public v/s private)
A.2.3.4
A knowledge, attitude and practice study on spacing contraceptive methods and emergency contraceptive pill among population of reproductive age in the state of
Haryana.
A.2.3.5
A study on epidemiology of substance abuse in youth of Haryana.
A.3 Other Activities conducted by PHP Division:
A.3.1 Project Implementation Plan (PIP) 2013-14:
Two Consultants (PHP) were full time involved in the preparation of State PIP with
NRHM for duration of 4 months. Assistance was provided to NRHM and region wise meetings of District level officers were conducted so as to orient them about GOI guidelines for the preparation of District Health Action Plans for 2013-14. Meetings were also held with State level program officers. First draft of State PIP was submitted. Changes in the PIP were made as discussed in NPCC meeting and final
State PIP for the year 2013-14 was submitted to GOI.
HSHRC Annual Report 2012-13 12
HARYANA STATE HEALTH RESOURCE CENTRE
An evidence based Need & Situation Analysis of selected Health Services in the
Districts of Haryana has been planned for the coming year. It will involve the following activities:
· Collection of evidence based information to have an actual situation at the facility level with regards of input, process and output which are affecting delivery and quality of health services.
· Sharing the lacunas with the facility and district level officers, support them for taking actions,
· Collection of information regarding needs of district level officers and their expectations from state
· Information will be useful for health managers in taking action and improvement
· It will also be useful for PIP implementation and next year planning.
A.3.2 High Level Task Force:
A high level task force was constituted by GOH and the work of coordinating the work of HLTF was assigned to HSHRC. The objectives of HLTF were to:
1. Review the trends of adverse social and health indicators of Haryana like Maternal
Mortality Rate, Under 5 Mortality Rate (U5MR), Child Mortality Rate, Infant
Mortality Rate (IMR), Neonatal Mortality Rate (NMR), Total Fertility Rate (TFR),
Couple Protection Rate (CPR), Gender Ratio, Malnutrition and Anemia.
2. Deliberate on the strategies which have been in place for the last five years.
3. Make recommendations on the strategic interventions to be made in the next five years (Plan period).
4. Assess the trends of malnutrition and anemia in the State and make recommendations to improve the nutritional status.
5. Recommend specific actions required to be taken by various departments and measures for improvement of inter sectoral coordination.
6. Take into account both rural and urban scenarios, the regional, the socio economic and cultural factors within the State while making recommendations.
The first meeting of High Level Task Force was held on 23-10-2012 at Haryana
Niwas, Sec-3, Chandigarh under the chairpersonship of Mrs. Navraj Sandhu,
Principal Secretary to Govt. of Haryana, Health & Medical Education Department. In this meeting after a general discussion about the adverse social indicators, the group was divided into three sub-groups i.e. Group A (Maternal Health + Child Health),
Group B (Anemia + Malnutrition) and Group C (Gender Equity + Family Welfare).
HSHRC Annual Report 2012-13 13
HARYANA STATE HEALTH RESOURCE CENTRE
The second and third meetings of High Level Task Force were held on 4 th - 5 th of
December 2012 and 16 th - 17 th of January, 2013 respectively.
Situational analysis, current strategies of the government was discussed and recommendations were given.
Some of the major recommendations that were made are:
A.3.2.1 Recommendations on the Maternal and Child Health sub group :
· Defining Services, Gap analysis and closure.
· Improvement of Quality of Services.
· Improvement of Referral Transport.
· Improvement of Trainings.
· Review of Maternal Mortality and Morbidity.
· Safe abortion services.
· More focus on Essential Newborn Care.
· Strengthening of Home Based Post Natal Care.
· Care of post neonatal infants and under 5 children and especially for acute respiratory infection (ARI) and acute diarrheal diseases (ADD).
· Infant Death, still birth and Child death Review (IDR)
· BCC is needed to address various issues related to maternal and child health.
· Routine Monitoring and Evaluation as well as third party evaluation of all programmes should be strengthened.
· Separate Cadre for Public Health services.
A.3.2.2 Recommendations on anemia and malnutrition sub group :
· Policy Decision
· A definite clinical and laboratory protocol to diagnose type as well as extent of anemia in individuals and population groups.
· Dietary Interventions
· Public education about disease and drugs.
· Community Involvement
A.3.2.3 Recommendations on gender equity and family welfare sub group:
· Defining Gender Issues in Health.
· Strengthening Institutional Capacities.
· Strengthening of Adolescent Health Services.
· Prevention of Sex Selection.
· Violence against women.
HSHRC Annual Report 2012-13 14
HARYANA STATE HEALTH RESOURCE CENTRE
· Improved access and information.
Final High Level Task Force Report has been submitted to Govt. of Haryana for approval and later it will be submitted to GOI.
A.3.3
Public Health Cadre:
Work of formulating a proposal for a Public Health Cadre was assigned to HSHRC.
Preparatory data collection was done by team of consultants from HSHRC. Both quantitative and qualitative data collection was done for this. Visits were made by the consultants to various health facilities to know about the workload and do situational analysis.
For preparation of this report wider consultations were held with NRHM, DGHS and other officers of the Health Directorate and NRHM and also with the office bearers of the HCMS association. Presentations were also made in the meeting of the Civil
Surgeon. It is also felt necessary to study and list the core public health functions for ensuring health promotion, health protection and health service delivery for the entire population of our State. Taking into account the wider determinants of health, need was felt to highlight linkages between various stakeholders and public health functions for better inter-sectoral coordination.
A high level task force was formulated by the Government of India to assist in the formulation of public health cadre in the state of Haryana. The chairperson of task force Dr Salunke and his team visited the state and field visits were made to interview different District and State Program Officers. Visits to the offices of the
Key personalities like Principal Secretary, Health; Managing Director, NRHM;
Executive Director, HSHRC and Director General Health Services was organized.
A workshop was also organized in collaboration with PHFI under the chairpersonship of Principal Secretary Health and various stakeholders were invites in that. Issues related to this were discussed and a draft proposal was made.
Formulation of a detailed report is under process.
A.3.4
Results Framework Document (RFD):
GOH decided to implement the Performance Monitoring & Evaluation System
(PMES) in the Department of Health vide which each department was asked to prepare a Results Framework Document (RFD ) which provides the summary of trends in previous years, achievements of current financial year and targets for the next three years. Objectives were defined for various divisions of Health
HSHRC Annual Report 2012-13 15
HARYANA STATE HEALTH RESOURCE CENTRE
Department like Maternal Health, Child Health, Family Planning, Referral Transport,
Community Process, IBSY, Construction, AYUSH, Drugs and Food Sampling etc.
These Objectives should be measured in terms of respective Actions and Success
Indicators. Various meetings were conducted with State Program Officers for compilation. Draft RFD was submitted. Changes were made as per suggestions by the Ministry. Final RFD Health for 2012-13 was completed and submitted. Targets versus achievements of RFD Health 2012-13 were reviewed periodically. First draft of RFD Health for the FY 2013-14 has been submitted.
Final RFD Health for 2013-14 will be completed and submitted to GOI. Review of
RFD will also be done.
A.3.5 Computerization of district hospitals:
In the state there are 54 General Hospitals 112 CHCs and 446 PHCs which provide a wide range of curative and preventive health care services. These institutions are providing treatment to 1.8 crores of patients in OPD and 1.6 Lacs indoor patients annually. Providing efficient healthcare services to patients in the state is the primary objective of the Department. Need was felt to put in place a suitable
Hospital Information System (HIS) to act as decision support system for hospital authorities/management for developing comprehensive healthcare policies for the benefit of citizen at large. In absence of computerization it becomes difficult to manage the patient load efficiently.
Earlier in 2009, an initiative in the regard was taken when, Expression of Interest
(EOI) in this regard was floated and 33 quotes were received in 2009. But the process could not be successfully completed.
In order to successfully accomplish computerization of hospitals HSHRC was directed to prepare scope of work, select a consultant for preparation of RFP by involving Directorate, NRHM and IT department in June 2012. It was decided to go through a consultative phase with the help of a competent consultant so as to draw up an effective overall solution blueprint and a roadmap for implementation. NISG &
NIC/NICSI were invited to give presentations regarding providing project consultation. Simultaneously a multidisciplinary committee was constituted to look at the presentations and evaluate. NIC expressed its inability to undertake the consulting engagement. NISG made a detailed presentation before the committee on
13-08-2012 and they were requested to submit a Techno Commercial proposal. The
NISG submitted a techno Commercial on which the committee in its meeting on 14-
09-2012 considered the proposal and recommended that advice of the Department of information Technology (IT) should be taken in this regard. IT PRISM approved the NISG for Engagement of National Institute of Smart Governance (NISG) on
HSHRC Annual Report 2012-13 16
HARYANA STATE HEALTH RESOURCE CENTRE
03-01-2013. A contract draft was prepared in consultation with NISG and vetted by the representative of the IT department, Haryana on 14-02-2013.The same proposal was sent to be vetted by the Legal Remembrance to Govt of Haryana and was approved by the same on 27-02-2013. Finally the MOU was signed between NISG and Govt. of Haryana on 03-04-2013.
As per MOU NISG has been asked to Prepare of scope of work, high level requirements, limited assessment of ready to use products available in the market including its feasibility for use, preparation and floating of RFP, evaluation of tender, selection of vendor and award of contract NISG presented its report on As Is process, Best Practices and To Be process in a meeting held on May 31, 2013. Based on the observations of the stakeholders NISG has been asked to submit Updated report on To Be report as part of Detailed Project Report. NISG has been asked to prepare detailed project (DPR) report by Second week of June and also to present
Solution Architecture on July 1, 2013.
A.3.6
Urban Slum Mapping:
HSHRC was given the task of conducting mapping of urban slums in order to plan the Urban Health Mission in Haryana. After making inquiries about the process from other states like Orissa it was decided to do the process by means of GIS mapping.
For this work it was decided to involve HARSAC (Haryana Remote Sensing
Organization) under the Department of Science and Technology (DST) for which meeting was held with the Principal Secretary of the DST.
A proposal was invited from HARSAC for preparation of City Maps. After discussion it was felt that since HARSAC have already prepared digital maps on village boundaries they can also map the political boundaries of each health centre.
In the mapping exercise of city maps there was a need to conduct a detail mapping of spatial distribution of urban population. There is lack of detailed information at the state level about the existing urban slums (notified and non-notified) and vulnerable, deprived and excluded populations along with health delivery infrastructure at city/town level.
Objectives of Urban Slum Mapping :
1) Listing, Identification and plotting of listed & unlisted slums on administrative
/political level, along with spatial extension.
2) Plotting population distribution in space on GIS maps.
HSHRC Annual Report 2012-13 17
HARYANA STATE HEALTH RESOURCE CENTRE
3) To identify the geographical location of the health facilities from Sub-centre level to
District Hospital along with the area being served and transport network for access to particular facility.
4) The mapping process will include the mapping of slums (notified and non-notified), the under-served urban pockets and urban colonies. There are large number of existing health centers, started at different times by different agencies like HUDA dispensaries, RCH centers under NRHM, Post Partum centre
☂ s for Family Planning services and ESI dispensaries. These will be put on the digital map to aid in planning and resource allocation for optimum results.
Deliverables of this activity: a. District wise Geo-referenced Digital Maps of Slums and Government Health Facilities and a state level integrated map. b. All maps will contain the following thematic layers in addition to the above: i. Latest available settlements map layer ii. Latest available Transport Network map layer. iii. Latest political boundary layer of health centres. iv. Integration of health Data on the GIS maps.
This activity will be completed by October 2013.
HSHRC Annual Report 2012-13 18
HARYANA STATE HEALTH RESOURCE CENTRE
H
UMAN RESOURCE FOR HEALTH
HSHRC was established to provide technical support, capacity building of health staff and to provide State specific Human Resource Development policies to address critical constraints of health staff. Following activities are being conducted to meet these objectives:-
B.1 Workforce Study: A study has been planned by HSHRC on Organization, Workforce and their Management, Educational and Training Institutes for various cadres of
Medical and Paramedical personnel (Medical Officers, Specialists, Nurses &
Midwifery, Lab Technicians, Pharmacists, Radiographers and OT Technicians) in the state of Haryana.
Proposal has been approved for Workforce study of three Paramedical cadres
(Nurses & Midwifery, Lab Technicians, Pharmacists).
The study will give status of staff (sanctioned, recruited and vacancies), recommendations for better working environment of the staff, factors responsible for individual performances. It will also provide capacity and gaps of quality and quantity of education and training institutions. It will also enable policy makers/managers to provide information for policy modification & development as needed. Work allotted to permanent & contractual staff and any discrepancy in it, in salary structure and other benefits given to both the cadres will also be found out.
B.2
Technical Support was provided to NRHM for preparation and submission of State
PIP, conducting Supportive Supervision to district etc.
B.3
State Institute of Family Welfare (SIHFW) conducted a study to evaluate ANM/GNM schools in various districts of the State. Technical Support was provided for the same to SIHFW.
B.4
Capacity Building of Medical and paramedical Health staff about quality improvement of health care service delivery.
B.5
Human Resource provided for planning and implementation of National Urban
Health Mission.
B.6
Capacity Building of Medical Officers and other Health staff about Rational Drug Use.
HSHRC Annual Report 2012-13 19
HARYANA STATE HEALTH RESOURCE CENTRE
D
RUG DIVISION
Introduction
The Drug Division of HSHRC has been formed in the year 2012 with the objective to provide required essential technical inputs in the field of policy reform and to strengthen the process of rational use of medicines in Haryana. Since, the inception of drug policy of Haryana a great need had been felt to develop continuous monitoring and evaluation processes to streamline the standards for drug procurement, testing of drugs for their quality assurance, drug supply and distribution, inventory management of drugs, drug prescribing practices, storage of drugs and their timely availability to the end user.
Drug Division is involved in all these areas since last one year by undertaking prescription audits and store audits, conducting trainings and workshops, adequate documentation etc. to find the gaps in implementation of drug policy in the state and finally to come up with suggestions to fill the gaps.
Drug division has worked in following broad areas during the financial year 2012-
2013:
1.
Evaluation of procurement programme & Policy reform
2.
Promotion of Rational use of Medicines
Activities proposed are- a.
Prescription audits b.
Trainings and workshops on rational drug use c.
Publication of material on rational drug use
3.
Audit of drug stores
4.
Setting up Centralized Medicine Testing Unit
HSHRC Annual Report 2012-13 20
HARYANA STATE HEALTH RESOURCE CENTRE
C.1 Evaluation of procurement programme & Policy reform
HSHRC was given the responsibility to formulate new drug policy for the state to streamline the procurement processes. In this regard a workshop was held on
4/10/2012 involving Civil Surgeons, Deputy Civil Surgeons (procurement), chief pharmacist from various districts in the chairmanship of Principle Secretary, Health.
A detailed presentation showing the present procurement process, its problem areas and suggestions was given by Dr. Ashish Gupta, ED (HSHRC).
Two districts were visited in this regard and many meetings were conducted involving doctors from General Hospitals to get their views and suggestions regarding purchase procedures including local purchase. Drug policies of other states were reviewed especially the policy related to Tamil Nadu Medical System
Corporation (TNMSC). As a result of above all efforts the new medicine purchase policy for Haryana was framed on the TNMSC model.
The new medicine purchase policy includes central procurement wing responsible for centralized purchase order and ware houses with online inventory system to improve storage conditions and maintain supply chain. Policy for local purchase of drugs and consumables has also been raised with increase of financial payments.
HSHRC Annual Report 2012-13 21
HARYANA STATE HEALTH RESOURCE CENTRE
C.2 Promotion of Rational Use of Medicine
Rational medicine use reduces cost of care, results in better clinical outcome & prevents antibiotic resistance. WHO in 2011 has declared that antibiotic resistance is one of the biggest public health problem.. Some reforms have already been done to promote rational drug use in Haryana like drawing up Essential Medicine List
(EML) in which irrational combinations were eliminated. For promoting rational use of drugs this purpose, HSHRC has carried out the following activities:
C.2.1 Prescription audit
The main objective of the prescription audits was to find out the irrationality in the prescriptions in terms of poor prescribing practices. Prescription audit of 7 districts
Kurukshetra, Palwal, Panchkula, Ambala, Hisar, Panipat and Rewari were carried out. Districts were selected randomly. Prescriptions were collected as 10% of the
OPD load in the facility. All the prescriptions were checked and verified for various parameters of the ideal prescription like mentioning of investigations, diagnosis, drug name (Generic or Branded), drug formulation, dosage, drug strength, number of drugs prescribed, and availability of prescribed drug in the hospital pharmacy.
The prescription audit report of district Kurukshetra and Palwal has been prepared and sent to the respective districts for appropriate corrective actions to be taken.
Draft report of other 5 districts (Panchkula, Ambala, Hisar, Panipat, and Rewari) is ready and will be sent to the respective districts to improve the prescribing quality.
Findings of the prescription audit of Kurukshetra and Palwal suggested the following-
C.2.1.1 Incomplete format of PrescriptionsThis affects the outcome of treatment in terms of inadequacies and adverse effects. Not even single prescription was found complete in the standard format. Components like standard pattern of history taking, general physical examinations, diagnosis and routine investigations were missing. Treatment was incomplete in respect of dosage form, strength, frequency and duration of the treatment. In 58% prescriptions all drugs were written in generic names. In 27% of prescriptions a mix of generic and brand naming of drugs were used.
C.2.1.2 PolypharmacyIt was found that the number of drugs prescribed per encounter in hospital was 3.4 and higher than the WHO recommended values of 1.6-1.8 (WHO:
Geneva, WHO/DAP/93.1, 1993)
HSHRC Annual Report 2012-13 22
HARYANA STATE HEALTH RESOURCE CENTRE
C.2.1.3 No mention of drug strengthIn 84 % of the drugs, Strength of the drugs was not mentioned. In 71% prescriptions, none of the drugs that were prescribed mentioned the strength while in 29% of the prescriptions strength was mentioned with some of the drugs only. Strength of all the drugs prescribed was mentioned in only 16% of the prescriptions
C.2.1.4 Non availability of prescribed drugs in hospital pharmacyIn 51% of prescriptions all drugs prescribed were available in the pharmacy, in 44 % of prescriptions some of the prescribed medicines were not available in pharmacy, and in 4% of prescriptions, none of the drug prescribed was available in the pharmacy.
This shows that our inventory is not complete in respect of OPD prescriptions.
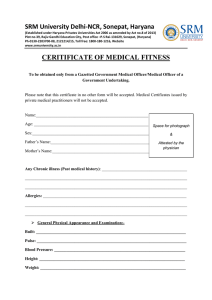
C.2.1.5 Overuse of analgesics and antibioticsFrom the present audit it was found that antibiotics and analgesics are prescribed unnecessarily and drugs required to be given for prolonged period like for Hypertension, Diabetes, Epilepsy and Anemia are not prescribed for the required time period. 54 % prescriptions were having antibiotics as compared to the WHO standard of 15-25%. While, 57% of the prescriptions were having analgesics. Fixed Dose Combinations which were not included in EML of Haryana but are present in CPSU medicine list are being used.
This is evident that we are wasting our resources on purchase of antibiotics and are not able to provide relatively cheap medicines used for chronic illnesses.
57%
Figure V-A: Pattern of drug groups being prescribed (No. of prescriptions=94)
54%
28%
26%
16%
Analgesics Antibiotics Antihistaminics Antacid Multivitmains
C.2.1.6 Inadequate treatmentAnemia, a major public health problem was found inadequately treated even at the district hospital level. A severely anemic baby was given iron which was inadequate in doses and duration. Even delivery cases and post natal cases are not being treated adequately. Iron and Calcium are given in once a day doses even at Hb 9.0 gm and duration of the drugs prescribed is not mentioned. If mentioned, it is not adhered to by the dispensing pharmacist. One post
HSHRC Annual Report 2012-13 23
HARYANA STATE HEALTH RESOURCE CENTRE natal case complaining of giddiness while getting up was not investigated for Hb even when her antenatal Hb was 8.5 gm/dl.
C.2.1.7 Non specific treatmentMany instances of non specific treatment were there.
Analgesic, antihistaminic, antacid and antipyretic were given simultaneously leading to polypharmacy. A large number of prescriptions were having same drugs without any provisional diagnosis.
Future Plan- A workshop will be held at the state level to share the findings so that appropriate corrective actions can be taken at the earliest in all districts. This activity will be continued and prescription audit of other districts will be conducted to see the level of improvement.
C.2.2 Training on Rational Drug Use
HSHRC has started a training session on a topic of
☜
Rational use of drugs and
Medication safety
☝
in induction training to newly recruit medical officers and dental surgeons. The trainings were organized in SIHFW, Sector-6 Panchkula. Total 5 such training sessions were held in the year 2012-2013.
C.2.3 Workshops
C.2.3.1 Workshop on
☜
Rational Use of Drugs and Standard Treatment Guidelines
☝
was conducted on 11th July 2012 under the chairmanship of Principle Secretary, Health.
A total of 32 doctors from all district hospitals of Haryana attended the workshop.
As per programme, 4 interactive sessions were conducted by Dr. Usha Gupta and
Dr. Sangeeta Sharma from Delhi Society for Promotion of Rational Use of Drugs
(DSPRUD). The discussion was on Global and national scenario of Rational Drug Use
(RDU), STG was advocated as an important tool for promoting RDU. It was concluded in the meeting that there is need to develop STG for Haryana with involvement of specialist doctors from district hospitals. It was decided that there will be a STG core committee at the state level headed by DGHS, Haryana. For each specialty a subcommittee was made comprising of up to 10 doctors per specialty with senior doctor as mentor for the group.
Future Plan- Along with doctors the paramedical staff and patients play major role in rational use of medicines. To educate paramedical staff, HSHRC would conduct trainings and workshops to promote rational use of medicines.
HSHRC Annual Report 2012-13 24
HARYANA STATE HEALTH RESOURCE CENTRE
C.2.3.2 Workshop regarding
☜ setting up of Haryana Medical Service Corporation
☝
was conducted on 21st March 2013 at SIHFW in the presence of Shri Poornalingam,
Former Principle Secretary to Tamil Nadu Government who set up the TNMSC. The workshop was attended by Principle Secretary, DGHS, MD NRHM, ED HSHRC, Civil
Surgeons, PMOs and Chief Pharmacists. The main objective of the workshop was to overview the success story behind setting up of Tamil Nadu Medical Service
Corporation (TNMSC) subsequently followed with the discussion on setting up of
Haryana Medical Service Corporation (HMSC) to streamline the process of procurement of drugs, consumables and equipments at the State Level.
C.2.4 Publication of material on rational drug use
To achieve the goal of uninterrupted free supply of good quality medicines to all patients attending public health facilities in the state, rational use needs to be focused. Rational use of medicines helps in providing standardized level of care to patients avoiding adverse outcomes. Standard Treatment Guideline, Essential List of
Medicines, Rational prescribing, Prescription Audit and Patient Education are some of the important tools for the success of rational use. Standard Treatment Guidelines
(STG) are systematically developed evidence based guiding principles for optimal patient care. It is an important document to guide the prescribers (doctors), dispensers (pharmacists) and those who plan the medicine purchase. It saves Govt. funds spent on procurement of irrational combination.
Therefore, with the aim to promote the rational use of medicines the drug unit has successfully completed the content planning process of
Haryana Standard Treatment
Guidelines (STG) for the rational prescribing by
Government practitioners of the State. The process initiated with the formation of STG
☁ Core Committee ☂ under the
Workshop on STG in progress chairmanship of DGHS,
Haryana. Subsequently,
☁
Specialty Sub-committees
☂
from each clinical specialty were formed. Content planning from each specialty sub-committee was monitored and coordinated by a
☁
Principle Coordinator
☂
. Member from
☁
Delhi Society for Promotion
HSHRC Annual Report 2012-13 25
HARYANA STATE HEALTH RESOURCE CENTRE of Rational Use of Drugs ☂ (DSPRUD) was also involved in the process to obtain overall guidance. Many workshops and meeting were called during the process to decide the format of book and priority diseases for Haryana state to be included.
The draft book has taken its final shape and soon will be physically in the hands of the government prescribers.
Future Plan A state level inauguration function will be organized to launch the STG and prescribers will be sensitized to use it. Then training programs will be formulated to ensure proper implementation of STG.
Modification of Essential Drug List (EDL) of Haryana will be done as per the drugs mentioned in Haryana STG.
It is also proposed that more reading material like Drug Formulary having the detailed information of the drugs listed in the EDL will be published to enhance knowledge of doctors and paramedical staff like.
HSHRC Annual Report 2012-13 26
HARYANA STATE HEALTH RESOURCE CENTRE
C.3 Audit of Drug Stores
Drug Division has conducted drug store audits of six districts, namely Kurukshetra,
Panchkula, Ambala, Hisar, Panipat, and Rewari. Selection of the districts was done on the random basis. During the audit visit was made to the Central stores of the district, main store of the General Hospital and store of one Primary Health Center.
Main objective of the store audit was to assess the process of drug procurement and drug inventory management to identifying the gaps/weaknesses in the existing system at various levels of its implementation; to produce evidence on the actual availability and stock-outs of drugs at the frontline service provider level. During the audit various documentations like Stock registers, Indent books, Procurement Plan of the district, Quarterly demand documents from the facilities, Invoices/bills of drug purchases, Inspection notes, Supply orders and Sanctions obtained were checked and verified to get relevant data. Physical verification of the drugs was conducted. Stock position of the drugs, their Stock out duration was also verified with the stock register.
Report of districts Kurukshetra and Panchkula highlighting the findings along with suggestions for improvement have been compiled as a report and shared with the district. The draft report of rest of the districts (Ambala, Hisar, Panipat and Rewari) has been compiled.
Findings from Drug store audit of district Kurukshetra and Panchkula suggested following-
C.3.1 Inadequate storage conditions
- Ventilation in stores is poor. Racks are there but number is not adequate and are arranged in such a way that these block the air flow to all medicines. Drug cartoons are kept directly on the floor. Anti-snake venom was kept in Almirah which should be in ILR. There was no room thermometer and hygrometer available to measure room temperature & humidity in both the stores.
Erupted walls in the store Erupted walls and congested space within the store
HSHRC Annual Report 2012-13 27
HARYANA STATE HEALTH RESOURCE CENTRE
Walls inside the store are erupted and broken at many places which results in pest infestation inside the store.
C.3.2 Non availability of medicines
Many important essential medicines were out of stock. These included drugs like Injection Pentazocine (an opioid analgesic and also used as pre-anesthetic medication), Tablet Amlodipine (an antihypertensive agent), Tablet Dicylomine (an antispasmodic agent), and Tablet and Syrup
Cotrimoxazole (a sulphonamide antibiotic recommended in IMNCI manual). Tablet
Phenobarbitone, Tablet Methyldopa, Tablet Ranitidine, Tablet Atenolol,
Tablet Frusemide.
In Panchkula 16 items were checked randomly for the stock position at the time of supply order out of which 3 items were nil/out of stock and for 4 items stock was very low and in other 9 items some stock was present. In Kurukshetra , Syrup
Paracetamol was out of stock for more than 6 months time.
From the above information it can be easily interpreted that no concept is in place for calculation of the buffer Stock, reorder level and Working stock.
C.3.3 Improper procurement procedure
Quarter wise procurement plan was prepared for the district but there is discrepancy between demand received from field and amount of medicines ordered by central store. The re-order level of each medicine had not been calculated to avoid stock outs and overstocking. This shows that demand generation from field i.e. Quantification of medicines for making supply orders is poor which a crucial step is in drug management system. Therefore, the district is not able to provide uninterrupted supply to all patients. There have been instances of cancelling the orders given earlier mainly because of the non supply of the orders placed. No risk purchase was done in case of non supply and no penalty was deducted in case of delayed supply or part supply. No in house test report was found with some of the bills. There is no prescribed performa of inspection report so that there is no scope of missing any point.
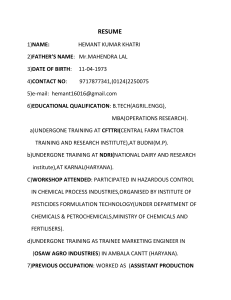
C.3.4 Group wise consumption
Analysis of yearly consumption of all medicines in both the districts randomly selecting 7 medicine groups namely Antibiotic,
Analgesic, Antihistaminic, Bronchodilator, Antihypertensive, Antidiabetics and
Antiepileptic clearly shows that there is over consumption of analgesic and antibiotic group of medicines and underuse of antihypertensives, antiepileptics, antidiabetics and medicines for bronchial asthma despite of the fact that antibiotics are required for a short period of time while the medicines for other mentioned groups need prolonged treatment.
HSHRC Annual Report 2012-13 28
HARYANA STATE HEALTH RESOURCE CENTRE
Figure IV-A : Relative Percentage of medicines available in each group (District Kurukshetra)
Antibiotics
50%
Analgesic
14% Anti Histaminic
7%
Anti
Hypertensive
9%
Anti Diabetic
4%
Anti Epileptic
5%
Bronchodilator
11%
Figure IV-B: Relative Percentage of budget consumed on groups (District Kurukshetra)
Antibiotics
74%
Analgesic
14%
Anti
Histaminic
5%
Anti Epileptic
Anti
Hypertensive
0%
1%
Bronchodilator
5%
Anti Diabetic
1%
HSHRC Annual Report 2012-13 29
HARYANA STATE HEALTH RESOURCE CENTRE
Figure IV-C : Relative Percentage of medicines available in
Anti
Epileptic
10% Anti Diabeties
3%
each group (District Panchkula)
Anti Hyper Tensive
11%
Anti Biotics
46%
Bronchodilator
7%
Anti Histaminic
9%
Analgesic
14%
Figure IV-D : Relative percentage of the consumed budget for each group
Anti Hyper Tensive
Bronchodilator
1%
1%
Anti Diabeties
0%
Anti Epileptic
4%
Anti Histaminic
12%
Analgesic
12%
Anti Biotics
70%
Future Plan Dissemination Workshop will be held at the state level to share the findings so that appropriate corrective actions can be taken. Drug unit would provide the technical help regarding any corrective actions.
HSHRC Annual Report 2012-13 30
HARYANA STATE HEALTH RESOURCE CENTRE
C.4 Centralized Medicine Testing Unit
Under the centralized medicine testing unit some labs would be empanelled at the
State level to perform the drug testing in their laboratories which would in turn help the government to monitor the quality of drugs being procured from various firms.
In the context of the above, HSHRC proposed to set up a Centralized Drug Testing
Unit at the State level. For this purpose, it was planned to empanel private drug testing laboratories. In the process, a tender document was prepared and floated.
Bids of 14 labs were received. These were reviewed by the designated committee comprising of members form HSHRC, NRHM, State Drug Controller and State
Analytical Labs. 7 labs have been approved for the empanelment on L1 rates.
For the first time in Haryana, it is now possible to test and check the quality of total
677 items including drugs, consumables, surgical and suture items before they are distributed to the peripheral facilities.
Future Plan The overall process with its documentation will be handed over to the centralized drug procurement wing which has been set up under NRHM Haryana.
Further activities will be taken up by the procurement wing.
HSHRC Annual Report 2012-13 31
HARYANA STATE HEALTH RESOURCE CENTRE
Q
UALITY DIVISION
QUALITY ASSURANCE INITIATIVES IN GOVERNMENT HEALTH FACILITIES IN HARYANA
D.1 Objectives of Quality Assurance Division:
· To provide support for developing quality management systems at hospital level leading to improvement of services quality and quality certification.
· To help the State develop and adopt standard protocols for providing quality health care services.
· To undertake assessments and monitoring of quality protocols adopted by the
State and suggest changes and improvements.
· To provide technical and managerial guidance for implementing quality protocols.
D.2
Adoption of Standards
For QA at facility level, Quality standards of NABH were adopted in the state.
National Accreditation Board for Hospital and Health Care facilities (NABH accreditation) was selected because:
1) NABH accreditation provided an optimum benchmarking standard for healthcare facilities
2) NABH standards are comprehensive.
3) NABH is nationally and internationally recognized
D.3 NABH Standards
There are different set of standards for hospitals and for CHC/PHCs which are as below:
D.3.1 Standards for Hospitals are:
D.3.1.1 Patient Centered Standards
1) Access Assessment and Continuity of Care (AAC)
2) Care of Patients (COP)
3) Management of Medication (MOM)
4) Patients Right and Education (PRE)
HSHRC Annual Report 2012-13 32
HARYANA STATE HEALTH RESOURCE CENTRE
5) Hospital Infection Control (HIC)
D.3.1.2 Organization Centered Standards
6) Continuous Quality Improvement (CQI)
7) Responsibilities of Management (ROM)
8) Facility Management and Safety (FMS)
9) Human Resource Management (HRM)
10) Information Management System (IMS)
D.3.2 Standards for CHCs and PHCs has been divided into 4 sections which relate to
1) Infrastructure Standards
2) Process Standards
3) Governance Standards
4) Outcome Standards
D.4 Methodology of Implementation:
HSHRC has initiated the Quality Improvement program in Haryana vide two approaches one of which is by engaging external agency and is being co-ordinated and monitored by in-house team and another which is solely being implemented by in-House team.
D.5 Process of NABH accreditation in Haryana:
D.5.1 Sensitization Workshop: A Sensitization workshop was organized on 3 rd May
2012, by HSHRC which was attended by worthy Principal Secretary Health and
DGHS along with Civil Surgeons and Medical Superintendents of 10 districts. In this workshop representatives from Quality Council of India (QCI) sensitized various stake holders about QCI and NABH.
D.5.2
Signing of MoU with QCI : The process of Quality Improvement was initiated by signing an MOU with QCI dated 7 th August 2012. QCI is the external agency providing technical support and various trainings in selected facilities.
D.5.3 Building of in-house Quality team : The in-house Quality Assurance team of
Haryana State Health Resource Centre was built. The process of team building involved selection of a regular HCMS doctor of commitment, sufficient seniority and experience as a team leader. The team leader was sent on exposure visits and various trainings like NABH internal counselor training, NABH assessor course,
HSHRC Annual Report 2012-13 33
HARYANA STATE HEALTH RESOURCE CENTRE
NABL training and ISO trainings. A QA team was selected at state level from candidates with qualification and experience of accrediting hospitals and Labs for
NABH accreditation. The team became the coordinating body for the process of
NABH Accreditation.
D.5.4 Selection of facilities for NABH accreditation : a) Selection of District Hospitals :
Under this process, in the 1 st phase two District Hospital i.e. District Hospital
Gurgaon and Faridabad have been selected and in the 2 nd Phase, three District
Hospitals at Panchkula, Rohtak and Hisar have been selected. b) Selection of PHCs and CHCs:
Two CHCs viz Kalka and Dabwali & two PHCs viz Pinjore and Keharwala of
Districts Panchkula and Sirsa respectively have been selected.
D.5.5 Technical Assistance:
The technical assistance agencies/ external consultants appointed by QCI for facilitating the NABH process in these facilities are:
· Astron Hospital and Healthcare Consultants- DH-Gurgaon, CHC Kalka, PHC
Pinjore (Dist. Panchkula)
· Academy of Hospital Administrators (AHA), NOIDA - DH Faridabad, CHC
Dabwali, PHC Keharwala (Dist. Sirsa)
· Medica Synergie Pvt. Ltd., Kolkata - DH-Panchkula, DH-Rohtak and DH-Hisar
D.5.6
Sensitization programme in nine facilities:
Sensitization meetings (with facility heads, respective civil surgeons from districts and state quality assurance team from headquarter level) have been conducted at various facilities. The sensitization involved information and knowledge sharing related to NABH standards and objective elements.
These meetings have been co-ordinated by QA team of HSHRC. Schedule of various meeting is as follows:-
· DH-Gurgaon on 12/09/2012,
· DH-Faridabad on 13/09/2012,
· DH-Panchkula on 30/01/2013,
· DH- Rohtak on 11/02/2013,
· DH- Hisar on 12/02/13, and
· CHC Kalka and PHC- Pinjore on 24/09/2012
· CHC-Dabwali and PHC Keharwala on 12/12/12
HSHRC Annual Report 2012-13 34
HARYANA STATE HEALTH RESOURCE CENTRE
D.5.7 Gap Analysis:
Gap Analysis has been conducted in terms of Infrastructure, Equipment, regulatory compliances, manpower and adherence to NABH process standards at DH-Gurgaon, Faridabad, Rohtak, Hisar, Panchkula and at CHCs ♠ Kalka and
Dabwali and PHCs- Pinjore and Keharwala.
D.6 Training Programme for Internal Councilors (POI):
Nine facilities have undergone three-day Training Programme for Internal
Councilors (POI) at:
· DH-Gurgaon from 7-9 th December,
· DH-Faridabad from 28 th -30 th Dec 2013,
· DH-Rohtak from 12 th -14 th April 2013,
· DH- Hisar 17-19 th May 2013,
· DH-Panchkula from 24 th -26 th May 2013
· CHCs ♠ Kalka and PHCs- Pinjore from 15 th to 17 th March 2013 and
· CHC Dabwali and PHC Keharwala from 5 th -7 th May 2013
In total 271 staff members of hospitals, CHCs and PHCs have been trained in POI
HSHRC Annual Report 2012-13 35
HARYANA STATE HEALTH RESOURCE CENTRE
These trainings have been co-ordinated and attended by State QA Team members
D.7 Capacity Building:
In addition to POI training hospital staff is also undergoing specialized trainings to build capacity at various facilities. List of trainings include:
D.7.1 Training on Documentation:
· Trainings on how to develop various manuals like Quality Manual, Infection
Control Manual, Hospital Safety Manual, Disaster and Emergency Preparedness
Manual, Laboratory Safety Manual, Radiology Safety Manual are being conducted.
· Following this training hospitals selected in 1 st phase are already developing policies and standard operating procedures related to NABH standards.
D.7.2 Trainings of hospital staff on Committee formation:
· Trainings have been conducted about formation of various committees, their composition and Terms of References (TORs). The committees are multidisciplinary and there is involvement of all levels of staff.
· Following this training various committees have been constituted in the hospitals selected in first phase.
Consultants from HSHRC regularly visit these facilities in order to guide the hospital level quality co-ordinators. Assistance is also being provided in developing documentation.
D.8 Formation of Committees:
The following committees have been constituted at DH-Gurgaon, Faridabad and
Panchkula whose meetings are being held regularly (monthly) as per schedule and being mentored by HSHRC QA team. Following is the list of committees formed along with their TORs:
D.8.1 Quality Assurance Committee : Quality Assurance committee or Steering committee creates a continuous quality improvement program for the hospital embracing all departments.
HSHRC Annual Report 2012-13 36
HARYANA STATE HEALTH RESOURCE CENTRE
D.8.2 Hospital Safety Committee (Disaster Management / Emergency Preparedness
Committee): Major functions include identification and elimination of the potential safety and security risks to staff, patients, and visitor in the hospital.
D.8.3 Infection Control Committee and Infection Control Team: Major functions include: Continued surveillance of hospital acquired infections, Development and formulation of preventive and corrective programmes in view of infectious hazards,
Develop a hospital antibiotic policy, develop a system of identifying, reporting, investigating and controlling the hospital acquired infections .
D.8.4 Code Blue Team : Major functions involve resuscitating a patient requiring CPR, to document the policies and procedures that guide the use of cardiac resuscitation throughout the organization, to record , analyse and evaluate all episodes of Cardiac
Arrest in the hospital by a multi disciplinary committee and to formulate preventive measures based upon this analysis.
D.8.5 Hospital Ethics Committee: Hospital Ethics committee discusses and offer judgment upon complex ethical issues as and when these are referred to the committee about organ donation, clinical trials etc.
D.8.6 OT & Blood Bank Committee: Major functions involve analysing blood transfusion reactions and turnaround times for blood bank. For OT analysing rescheduling of procedures, utilisation indices and taking corrective and preventive actions etc.
D.8.7 Pharmaco-therapeutic Committee: An Advisory role on the pharmaco-economic evaluations of drugs, to co-ordinate the introduction of new drugs/extended use of existing medicines.
D.8.8 Medical Audit & Mortality-Morbidity Committee : Major functions involve audit of medical records and feedback to clinicians on the same.
D.8.9 Grievance Redressal Committee: Major functions involve to issue a policy on grievance redressal, develop a mechanism of handling employee grievances, take action on all employee grievances.
D.8.10 Credentialing and Privileging Committee: Major functions involve verification of the qualifications and trainings of the medical personnel
D.9 Technical Support from HSHRC:
Consultants from HSHRC regularly visit these facilities and provide technical inputs.
Review meetings are regularly held to assess the progress of process of NABH accreditation.
HSHRC Annual Report 2012-13 37
HARYANA STATE HEALTH RESOURCE CENTRE
D.10 Review:
D.10.1 Review at Level of Principal Secretary and DGHS:
Two meetings have been held at DH Gurgaon and DH Faridabad respectively under the chairpersonship of worthy Principal Secretary Health. Various decisions have been taken for closure of gaps as far as infrastructure, equipment and manpower is concerned. These decisions are being implemented along with o/o DGHS in order to facilitate the process of NABH accreditation.
D.10.2 Meetings of State Quality Assurance committee:
One meeting of State Quality Assurance committee has been held under the chairpersonship of worthy Principal Secretary Health on 20/12/12. Various decision points included.
· Optimization of manpower in various health care facilities. The issue is being followed up with O/o DGHS. Revised staffing norms are being developed. Also some revisions are being done in the norms for manpower to be hired through outsourcing.
· Formulation of a Core Committee: A core committee was formulated for the design framework to be adopted for construction of new hospitals as per NABH.
As regards to construction and up gradation of OT
☂ s and CSSD etc HSHRC is coordinating the process as per NABH standards.
· Infrastructure modifications specifically in operation theatres as per NABH standards like separate air handling units (AHU), ventilation system, laminar flow,
HEPA filters. HSHRC is in the process of implementing various changes required in
OT as per NABH standards. Extensive study on the subject has been done by QA team of HSHRC. Tender document for OT up-gradation and installation of HVAC is being prepared by HSHRC.
D.11 Plan for next Phase:
In the next phase the following steps would be taken:
· Implementation of processes and development of systems is an ongoing process which would continue.
· Documentation and closure of Gaps identified as per NABH standards would continue.
· Specialized certificate trainings on Disaster management, clinical Audit, Surgical site infection, medication safety would be conducted.
HSHRC Annual Report 2012-13 38
HARYANA STATE HEALTH RESOURCE CENTRE
· Internal Audit of the concerned facilities would be conducted and reassessments would also be done this year.
· The facilities taken up in the first phase for accreditation would apply for Pre-
Assessment in the current year 2013-14
D.12 Quality Improvement focused study for 3 departments
Haryana state health Resource Centre
☂ s in-house Quality Assurance team had initiated the process of Quality Improvement in sixteen District Hospital of Haryana which aimed at improving the quality of services in three departments ☂ viz. Accident,
Emergency and Trauma Department, Maternity units and laboratories.
The focus was laid majorly on three departments of Emergency & Trauma
Department, Maternity & Labour Room and Laboratory because:
· They are considered to be the backbone of Hospital services
· Maximum patient volumes in public hospitals are in these departments
· These three departments Cater to critical patients
· Handling of medico-legal cases is responsibility of these three departments
· There are specific training requirements
· Functional 365*24*7, so there are more chances of errors & litigations, patient safety is a major concern
· These are largely responsible for the public image of the hospital
Aim of the project was to initiate Quality Improvement Process for district hospitals other than those selected for NABH accreditation and to improve the quality of healthcare delivery services.
Objectives of the project included: a. To assess the existing service delivery standards of the district hospitals to identify the baseline level of Health care delivery of services. b. To assess the existing infrastructure, equipment, manpower, process flow c. To suggest alterations in structural designs of the facilities to meet the requirement. d. To initiate documentation for various activities. e. To reinforce training requirements for the clinical and non clinical staff.
HSHRC Annual Report 2012-13 39
HARYANA STATE HEALTH RESOURCE CENTRE
Consultants from QA team of HSHRC visited these facilities and conducted gap analysis with the help of staff interviews and by observing the process is being followed.
☜
As Is
☝ gap audits were conducted in DH- Ambala on 26 th November 2012, DH- Sirsa on
13 th and 14 th December 2012, DH-Kurukshetra on 4 th January 2013. In these gap audits: v Existing infrastructure of 3 departments was studied in detail. v Manpower for the hospitals was compared against sanctioned strength as well as manpower actually required as per workload. v Equipment gaps were assessed using the work load of specialty and advancement of technology. v State of Regulatory compliances was assessed.
As a result of the gap audits it was concluded that standardization of these departments with respect to infrastructure, manpower and process flow needs to be done, this lead to a thought that development of standards for the Emergency Department and Maternity units needs to be done. For labs it was decided to use NABL standards as benchmark.
D.12.1 Development of standards for Maternity Units:
HSHRC Annual Report 2012-13 40
HARYANA STATE HEALTH RESOURCE CENTRE
In order to standardize maternity/ labour rooms ☂ steps were taken to develop standards for maternity/ labour rooms. A proposed draft having the following was developed:
· Basis for calculating beds for antenatal ward, number of delivery tables required against district wise workload was calculated. Number of ante-natal beds, number of pre-natal beds, and number of post-natal beds required against district wise workloads was also worked upon.
· Infrastructure of rooms with proposed layout of a maternity unit was developed having the following essential area demarcations:
1) Waiting area and Lobby
2) Antenatal Room with designated Eclampsia Beds
3) MTP Room
4) Examination and Preparation Room
5) Pre-Delivery Room
6) Delivery Room
7) Post Natal Room
· Equipment required was separately incorporated along with the essential medications.
The draft developed was not finalized due to duplication of activity. Later on
GOI has come up with the MNH standards and these can be adopted by the state as it is.
D.12.2 QUALITY IMPROVEMENT FOR LABORATORIES AS PER NABL (ISO-15189)
Introduction
Laboratory services form the
☜ back bone of a hospital
☝
. Lab services must be consistent and dependable to correctly access and manage patients with various illnesses. Without accurate lab services, test results may be wrong, and if they are not accurate, consistent, and dependable, every effort is essential to raise them to acceptable standards.
HSHRC Annual Report 2012-13 41
HARYANA STATE HEALTH RESOURCE CENTRE
Laboratories in district hospitals handle a huge amount of workload, increased service delivery at district hospitals lead to a compromise in the quality of reporting of laboratory results. Quality Management Systems for laboratory is vital for standardisation of laboratories as per Pre-Analytical systems (Sample collection/ Phlebotomy and transportation of samples), Analytical systems (Analysis of patient samples) and Post ♠ analytical systems (result reporting and monitoring patient turnaround times)
The NABL standards (ISO- 15189) include the following parameters which are related to
MANAGEMENT REQUIREMENTS
Organization & Management Quality Management Systems, Document Control, Review of
Contracts, Examination by referral laboratories, External Services and Supplies, Advisory
Services, Resolution of Complaints, Identification & controls of Non-conformities,
Corrective Action, Preventive Action, Continual Improvement, Quality and Technical
Records, Internal Audits, Management Reviews
TECHNICAL REQUIREMENTS
Personnel Accommodation and Environmental Conditions, Laboratory Equipment, Preexamination Procedures, Examination Procedures, Assuring the Quality of Examination procedures, Post -examination Procedures, Reporting of Results
HSHRC has initiated the NABL (National Accreditation Board for Testing and Calibration
Laboratories) of the laboratory of district hospital Panchkula as a pilot project.
The following activities have been conducted in the laboratory:
Gap analysis of the laboratory has been completed as per NABL (ISO-15189 standards), the gap analysis report has been shared with the DGHS and MD (NRHM). Gap Analysis of
Laboratory of DH- Panchkula was submitted to the hospital in November 2012.
A detailed action plan has been prepared based on Gap analysis report. Six meetings have already been held with the hospital authorities. Three staff including one pathologist, one microbiologist and one senior lab technician from the laboratory has been sent for specific training on ISO 15189 (NABL)
The laboratory is in the preparation stage of various documents like Quality manual,
Standard Operating Procedures for Haematology and Biochemistry, Sample Collection
Manual and Directory of Services. Templates for documentation are being provided by
HSHRC. Also technical inputs are being provided by in house quality assurance team of
HSHRC.
Quality Management Systems for laboratory have initiated the Critical result documentation and timely convey to the physician in-charge of the patient in case of any
HSHRC Annual Report 2012-13 42
HARYANA STATE HEALTH RESOURCE CENTRE high alert values. Usage of Internal controls for Haematology and Biochemistry have been initiated for various equipments. External Quality Assurance Scheme (EQAS) have been initiated from January 2013 for Haematology from All India Institute of Medical Sciences-
(EQAP) and for Biochemistry and Immunology from CMC Vellore (EQAS) as well. Results are being quarterly received; corrective and preventive actions are being taken.
Consultants from HSHRC regularly visit the laboratory and hold weekly meetings to review the progress.
Laboratory will apply for Pre-Assessment in the current year 2013-14
D.12.3 QUALITY IMPROVEMENT OF EMERGENCY DEPARTMENT AT DISTRICT LEVEL
Introduction and Objective
At present the Accident & Emergency department (A & ED) of District Hospitals is stretched beyond capacity. There are a total of 21 districts in Haryana. During the year
2011-12, a total of 7,04,384 patients were treated in A & ED. On an average about approx
5,00,000 patients are treated in A &ED on OPD basis out of which about 70,000 are admitted ,with about 2000 MLCs and 300 Post mortems being done.
Keeping in view of the above statistics it was felt that there is a need to evolve standards for infrastructure, equipment and manpower in the Accident & Emergency Department for
District level hospitals in Haryana. For this purpose the strategy decided is as follows:
Step 1 Formation of Manual
Step 2 Gap Analysis : After finalising the manual, gap analysis of various health facilities
( district hospitals) would be conducted by quality assurance team of HSHRC in terms of infrastructure, manpower, equipment and processes followed by the gap closure of the gaps.
HSHRC Annual Report 2012-13 43
HARYANA STATE HEALTH RESOURCE CENTRE
Step 3 Gap Closure: The gaps identified would be analysed at state level and a responsibility matrix would be developed and the process of gap closure would be initiated.
D.13 Educational Visits and Trainings conducted for capacity buildings
1) Educational visit was made to District hospital Ernakulum, Kochi, Kerela
2) Thirteen MOs have been sponsored for PG Certificate course in QM & AHO (Quality
Management and Accreditation in Healthcare Organization) by Academy of Hospital
Administration (AHA) as a capacity building exercise out of which 4 have already cleared the examination and have received certificates.
3) Three doctors and one lab technician sponsored for training in ISO 15189 (NABL) standards.
4) ACLS trainings already provided to 2 Anesthetists at GH-Gurgaon.
5) Two doctors have been trained as NABH assessors at State level.
In the current year more doctors will be trained in PG Certificate course in QM & AHO
(Quality Management and Accreditation in Healthcare Organization) for orientation.
ACLS Provider Trainings to be provided to Anesthetists in DH-Rohtak, DH-Hisar, DH-
Panchkula DH- Faridabad, CHC-Kalka and CHC-Dabwali.
HSHRC Annual Report 2012-13 44
HARYANA STATE HEALTH RESOURCE CENTRE
They will then act as master trainers and train the rest of the staff in BLS. Various specialized trainings would be provided by QCI like training on disaster management, medication safety etc. at facilities selected for NABH accreditation.
HSHRC Annual Report 2012-13 45
HARYANA STATE HEALTH RESOURCE CENTRE
M
ONITORING & EVALUATION DIVISION
Monitoring and Evaluation is an essential management tool which helps to ensure that health activities are implemented as planned and to assess whether desired results are being achieved or not. It provides concurrent feedback on the progress of activities and helps to identify the problems in their implementation and suggests corrective actions for the same.
E.1 STUDY ON FUNCTIONALITY AND UTILIZATION OF HEALTH
SERVICES IN CHCs OF HARYANA
The population coverage by CHC is one among the important factors that influence the accessibility of health care services. The prescribed guideline as per the central government to establish a CHC is 80,000 to 1, 20,000 populations. Furthermore every CHC envisaged as primary and secondary care provider to rural and semi urban population. The Indian Public Health Standards are the benchmarks which have set a standards for minimum infrastructure, service availability, human resource and quality standards for CHC in India.
A study was designed with an aim to assess CHCs according to the population served and to the status of availability of services, accessibility, human resource and service utilization at CHCs. The tool for data collection was developed using Indian
Public Health Standard (IPHS, revised 2012) for CHCs and regular HMIS formats
(GoI) for service utilized at CHCs. Total of 109 CHCs were covered in the study.
Population covered by CHCs in Haryana
(in Lakhs)
2-3 lakhs
13%
3 lakhs
5%
1.2-2 lakhs
46%
Data NA
3%
0.5 lakh
14%
0.5-0.8 lakh
6%
0.8-1.2 lakh
13%
The study revealed that only 13% of the CHCs fitted in the norms of catering
80,000 to 1,20,000 population.
· 20% CHCs were covering less than 80,000 population, out of which
14% CHCs were covering even less than 50,000 population.
· 18% CHCs of the state were covering more than 2,00,000 population. Certainly these CHCs may face difficulties in providing services to its beneficiaries compromising the
HSHRC Annual Report 2012-13 46
HARYANA STATE HEALTH RESOURCE CENTRE quality of services being provided.
· Hence, 38% CHCs require attention of Policy makers and managers to rationalise as per coverage and CHC norms.
· Most CHCs of Jhajjar (67% CHCs (4 out of 6)) and Bhiwani (44% CHCs (4 out of 9)) districts had less than 50,000 population covered under it
· Most of the CHCs in Mewat (3 out of 3), Panipat (2 out of 3), Karnal (3 out of 6) and
Fatehabad (4 out of 4) districts serve more than 2 lakhs population.
E.1.1 Status of availability of services, accessibility, human resource and service utilization at CHCs:
E.1.1.1 Status of availability of services :
· 8% of the CHCs were not providing even basic services like 24-hour delivery services (normal and assisted) and ante natal & post natal clinics.
· Emergency obstetric care including surgical interventions like caesarean sections and other medical interventions were available only in 9% of the total CHCs.
· Blood storage facility was available only in 4% CHCs.
· RTI/STI services are available at 79% CHCs and ICTC services in 47% CHCs.
· X-rays were available in 47% CHCs and ECG was in only 22% CHCs.
· MTP services were available at 33% CHCs. Permanent Family planning methods were not done at 62% CHCs.
· 25% CHCs were not providing RTI/STI services at all.
E.1.1.2 Status of Human resource at CHCs:
· There were filled positions of only 39 specialists in all CHCs added together instead of 665 as per IPHS norms, indicating a gap of 94%.
· Not even half number of Medical officers and AYUSH officers (47%) were available at CHCs as per IPHS norms.
· Availability of Lab technicians in CHCs was slightly better (i.e. 87%) as compared to other health staff.
· Medical officers of AYUSH were in position in 49% CHCs.
· 32%, 41% and 52% positions of the Nursing staff, Pharmacists and Radiographers respectively were found vacant in CHCs.
The study suggests that Blood storage and Emergency Obstetric care services should be improved at the CHCs, so that the FRUs can be declared fully functional.
Minimum staff provision for 24 delivery service and other required facilities should be provisioned. There is need of rationalization of staff availability, improvement in infrastructure to improve OPD/IPD services at CHCs.
HSHRC Annual Report 2012-13 47
HARYANA STATE HEALTH RESOURCE CENTRE
The CHCs, formed below the prescribed norm of population may have less workload and hence underutilized. The human resource deployed in these CHCs need to be rationalized as per its utilization of the services.
The CHCs which are covering less than prescribed population norm may be recategorized into Level II and II and declared as different level of CHCs which will have slightly more staff position than PHCs but less than that of CHCs.
On the other hand, the CHC which were covering population more than the prescribed norm is bound to be overloaded may be categorized as Level I Plus .
More human resource may be deployed in these CHCs to improve service delivery.
Immediate attention needed to the CHCs (6) which were serving more than 3 lakh population. Additional CHCs should be planned in the area where the population coverage is more than the prescribed norm. These CHCs may also be taken as FRUs.
The detailed report is in final submission phase.
HSHRC Annual Report 2012-13 48
HARYANA STATE HEALTH RESOURCE CENTRE
E.2 STUDY ON INFANT AND MATERNAL DEATH AUDIT IN
HARYANA
This study was conceptualized with an aim to identify gaps in the present infant and maternal death audit system of Haryana for further reduction in IMR and MMR of the state. MMR of state although is less than average MMR for India and IMR is just the same for both, but there is a long way to go for achieving better health indicators for the state. These can be achieved by answering few questions like whether
Haryana health department is able to find out the exact cause of death of a mother or infant. Are there any gaps in present verbal autopsy process by health functionaries? Therefore, a third party evaluation was done by CRY organization and HSHRC. Funds for the study were provided by CRY while HSHRC provided technical and logistic support.
Objectives of the study were:
1. To assess the present process of Infant and Maternal Death audit in Haryana
2. To check the efficacy of existing data on maternal and infant deaths by back checking of selected sample.
3. To identify gaps in the audit process of Infant and Maternal Deaths and recommend corrective measures
Four critical districts were selected from all the four regional divisions of Haryana state. All the maternal deaths and 5% of the reviewed infant deaths was the selected sample for this study. Teams from HSHRC co-ordinated CRY at various issues. A one day workshop was organized for the district level stakeholders to make them aware of the study and to take their inputs for betterment and making data collection process easy and successful.
HSHRC Annual Report 2012-13 49
HARYANA STATE HEALTH RESOURCE CENTRE
Various tools were developed to collect data for finding the answers of objectives.
Verbal autopsy forms in local language and interview questionnaires for health functionaries and a check list to assess the autopsy process was developed. A team from CRY constituted by data enumerators and supervisors visited the households of the deceased person and verbal autopsies were done. In-depth interviews of concerned medical staff and district level officers were also done.
This Study is still going on as final findings and report is in progress. Valuable recommendations for improving the audit process will be extracted from the findings.
HSHRC Annual Report 2012-13 50
HARYANA STATE HEALTH RESOURCE CENTRE
E.3 STUDY ON ASSESSMENT OF IDLE MEDICAL EQUIPMENTS IN
CHCS OF HARYANA
Equipment is the essential infrastructure element and major contributor along with drugs, facilities, manpower and other devices for the delivery of various diagnostic and therapeutic services to the people. Health care technology management cycle includes various activities for the equipment under management.
Out of nine steps of the cycle, three important steps after procurement and installation are (a) training and skill development, (b) operation and safety and (c) maintenance and repair. In spite of its obvious importance, equipment often does not receive proper attention in terms of planning, incorporation and management.
A study was planned by Monitoring & Evaluation division of HSHRC with an aim to strengthen the ongoing system of planning, acquisition and maintenance of the medical equipments for a comprehensive and more effective management at CHCs of
Haryana.
Haryana state is having 21 districts and there are 110 Community Health Centers.
CHCs, sub-divisional hospitals and General hospitals are all meant to provide secondary level of care to the patients.
Moreover, CHCs compared to SDH and GH is more accessible to people in terms of distance and time need to travel. CHCs are
Figure-1
Management Cycle getting less attention of health managers in terms of improvements in infrastructure mainly medical equipments and their proper utilization than DH and SDH. Hence health care services are providing through
CHCs are not up to the mark or adequate in quantity and quality.
Therefore CHCs are chosen as the area for this study. Assessment of the availability, shortage, working order and utilization of various medical equipments along with various possible reasons for idleness of the equipments in community health centers were its main objectives. All the CHCs were covered in this study and list of 47 major equipments in CHCs was considered by short listing the equipments from IPHS list.
Biomedical engineering division of NRHM collaborated with HSHRC for data
HSHRC Annual Report 2012-13 51
HARYANA STATE HEALTH RESOURCE CENTRE collection procedure. Biomedical engineers at districts visited CHCs for collecting required information for the study.
Key findings of the study are as follows:
· There is a shortage of 26% for all these 47 equipments at CHCs and 21% equipments lie idle due to one or more reasons.
· There is no CHC in Haryana where all these equipments were present and no district with CHCs having medical equipments more than 75%.
· Two districts were found to be having idle equipments by more than 30%.
· Equipment wise idleness showed that there were 14 equipments which were idle by more than 30% in the CHCs. These equipments are shown in following graph.
· The Blood storing refrigerators were idle by 72% followed by Halothane
Vaporizer with 64% and colorimeter by 30%
· These 14 equipments were from labour, surgical, radiology, laboratory and neonatal care departments.
Health services hampered due to medical equipment idleness:
· Specialty services to the patients like complicated deliveries, major operations and operations under general anesthesia.
Major reason for idleness :
Ø Non availability of professionals and technical staff to operate that equipment
(15%)
Ø 12% equipments received without demand/indent
Ø 12% awaited condemnation of non-working equipments
Ø Repairing, training of the staff and under utilization of CHCs with no load of patients were the other major contributors of equipment idleness.
Final report and recommendations are in progress.
HSHRC Annual Report 2012-13 52
HARYANA STATE HEALTH RESOURCE CENTRE
E.4 DATA INFORMATION CENTRE
HSHRC has planned to establish data resource centre in the division of M&E. Health program progress data is being collected from various division of health department and analyzed by using advance mathematical methods and statistical test to make aware whether programs are making significant change. These findings are to be shared with key stakeholders like state and district level health officers.
Analysis of Key Indicators (from HMIS Haryana)
HMIS data has been used from the month of April 2012 to March 2013 for all the districts of Haryana and analysis has been done on yearly basis. The analysis has been done for some selected indicators of health which are as follows:
A. ANC services Index (composite index for ANC registration, TT-2/Booster, ANC-3, and distribution of 100 IFA tablet)
B. Eclampsia cases managed during delivery
C. Place of delivery
D. MTP cases
E. Sex ratio at birth
F. Immunization index (composite index including BCG, DPT-3, Polio-3, and measles)
G. Vit. A dose
H. Load of OPD at the Govt. health facilities
I. RTI/STI cases treated
For advance analysis of the above indicators various demographic estimations has been used.
HSHRC Annual Report 2012-13 53
HARYANA STATE HEALTH RESOURCE CENTRE
P
UBLIC PRIVATE PARTNERSHIP (PPP) DIVISION
F.1 Proposed Common Biomedical Waste Treatment & Disposal
Facilities
Keeping in view of the problems faced by various Government and private hospitals in handling biomedical waste, Government of Haryana proposes to set up Common
Biomedical Waste Treatment and Disposal facility on PPP basis.
Following activities were undertaken in this regard: o Preparation of Draft RFP Documents consisting of Instruction to Bidders, Draft
Concession Agreement and Schedules o Organized Investment Meet of prospective Private Sector Players to understand their viewpoints on the proposed development
F.2 Setting up of Diagnostic Facilities in various District Hospitals in
Haryana
The Health Department, Government of Haryana, is engaged in the development and provision of Health Care Delivery System in Haryana and as part of this continuing endeavor, the Department has decided to undertake development, operation and maintenance of the radiological services at selected District Hospitals of Haryana through Public Private Partnership on Design, Build, Finance, Operate and Maintain basis, and has decided to carry out the bidding process for selection of a private entity as the Bidder to whom the Project may be awarded.
Assistance was provided to Department of Health in preparation of the RFP documents in terms of providing suggestions on viability gap funding and key performance indicators for these facilities.
F.3 Draft Monitoring Mechanism for various outsourcing services in
Hospitals in Haryana
In order to improve the quality of health care services and to allow hospital doctors to concentrate on patient care, various Government hospitals have contracted ancillary
HSHRC Annual Report 2012-13 54
HARYANA STATE HEALTH RESOURCE CENTRE services such as laundry, housekeeping, security, etc. to private sector players. Now, in order to ensure the performance by these outsourcing agencies, it was felt that a robust monitoring mechanism with inbuilt review system has to be prepared in order to monitor these services on regular basis.
A draft institutional mechanism was prepared for establishing a system for monitoring & reviewing various outsourcing services in Government Hospitals.
HSHRC Annual Report 2012-13 55
HARYANA STATE HEALTH RESOURCE CENTRE
W
ORKSHOPS and MEETINGS CONDUCTED BY
HSHRC DURING 2012-13
S.
No.
Workshop Conducted Venue Date
Drug Division
1 Rational Use of drugs and Standard
Treatment Guideline
2
☁
Rational Use of drugs and medication safety ☂ induction training of newly recruited medical officers and dental surgeons
Red Bishop,
Panchkula
SIHFW,
Panchkula
11 th July 2012
15 th Sept 2012,
05 th Oct 2012,
16 th Oct 2012,
29 th Nov 2012 &
30 th Jan 2013
3 Consultation on New drug policy
4 Setting up of
☁
Haryana Medical
Service Corporation
☂
SIHFW,
Panchkula
SIHFW,
Panchkula
Quality Division
5 Workshop on sensitization
♠ by
Quality Council of India (QCI)
Red Bishop,
Panchkula
04 th October 2012
20th March 2013
3 rd May 2012
S.
No.
Meetings Conducted Venue
Public Health Planning Division
1. First High level Task Force Meeting Haryana Niwas, sector-
3, Chandigarh.
2. Second High level Task Force
Meeting
Red Bishop, sector-1,
Panchkula.
3. Third High level Task Force
Meeting
Red Bishop, sector-1,
Panchkula.
Date
23 rd Oct 2012
4 th and 5 th Feb 2012
16 th and 17 th Jan 2013
Drug Division
Meetings regarding setting up of Centralized medicine testing unit
HSHRC Annual Report 2012-13 56
HARYANA STATE HEALTH RESOURCE CENTRE
4.
5.
6.
Pre bid meeting NRHM, Panchkula 17 th Aug 2012
Technical bid evaluation
Financial bid evaluation
NRHM, Panchkula
NRHM, Panchkula
07 th Sept 2012
&
22 nd Feb 2013
14 th March 2013,
23 rd April 2013 &
03 rd May 2013
Meetings regarding development of Standard Treatment Guideline (STG)
7. STG Core committee meeting to finalize the members of specialty sub-committee
8. First meeting of all sub-committee members
DGHS, Haryana
SIHFW
Panchkula
04 th & 8 th Aug 2012
9. Final meeting for STG
&
Proof reading of draft
Red Bishop, Panchkula
&
SIHFW, Panchkula
21 st Aug 2012,
12 th Sept 2012
&
27 th Sept 2012
22 nd Jan 2013
&
29 th March 2013
10. Sensitization of GH-Gurgaon
Quality Division
GH- Gurgaon
11. Sensitization of GH-Faridabad GH-Faridabad
CHC-Kalka
12 th Sept 2012
13 th Sept 2012
24 th Sept 2012 12. Sensitization of CHC- Kalka, PHC-
Pinjore
13. Sensitisation of CHC- Dabwali PHC-
Keherwala
14. State Quality Assurance Meeting
CHC-Dabwali
O/o PSH
12 th Dec 2012
15. Meeting related to NABH accreditation
16. Sensitization of GH-Rohtak
17. Sensitization of GH- Hisar
Conference Room, GH
Gurgaon
GH- Rohtak
GH-Hisar
20 th Dec 2012
21 st Jan 2013
11 th Feb 2013
12 th Feb 2013
HSHRC Annual Report 2012-13 57
HARYANA STATE HEALTH RESOURCE CENTRE
Meetings/Workshops Attended by the members of HSHRC in
2012-13
S.
No.
Meetings/Workshops
Attended
Venue
Public Health Planning Division
1. Health Policy and Planning NIHFW, Delhi
Date
2. Training for Public Health
Planning and Monitoring &
Evaluation Professionals
NHSRC, Delhi
15 th to 17 th Oct
2012
30 th Jan to 1 st Feb
2013
Drug Division
3. Workshop on management of medication by QCI
4. Meeting regarding study on
☜ assessment of rational use of drugs in 10 states of India
☝
by
CIPS
Fortis Hospital, Mohali 19 th May 2012
Indraprastha Apollo
Hospital, Delhi
Quality Division
10 th August 2012
5. Workshop on Clinical Audit NABH, New Delhi 1 st July 2012
AHA, Noida 18 th June 2012 onwards
6. PG Certificate course in QM & AHO
(Quality Management and
Accreditation in Healthcare
Organization)
7. 3-day Programme on Internal
Councillors
8. Workshop on CQI (Continuous
Quality Improvement)
9. Workshop on ISO 9001:2008
New Delhi
NABH, New Delhi
New Delhi
31 st Aug to 2 nd Sept
2012
25 th Aug 2012
8 th -12 th Oct 2012
10. NABL ♠ Internal Auditor training on ISO 15189
11. 3-day Programme on Internal
Councilors
12. 3-day Programme on Internal
Councilors
13. PGIMER-Laws applicable to hospitals
14. SASH Conference
New Delhi
GH-Gurgaon 7
18 th th
- 9
♠
2012 th
21 st Dec
Dec 2012
GH-Faridabad from Dec 28 th - 30 th Dec 2012
2013,
PGIMER, Chandigarh 7 th
♠
8 th Feb 2013
New Delhi 9 th Feb 2013
15. Hospiarch-Conference on Hospital
Planning and architecture
Chandigarh 16 th Feb 2013
HSHRC Annual Report 2012-13 58
HARYANA STATE HEALTH RESOURCE CENTRE
16. 3-day Programme on Internal
Councilors
CHCs
♠
Kalka and PHCs-
Pinjore
15 th - 17 th March
2013
Venue Date Division S.
No.
Cross Visits Attended
1. General Hospital-Ernakulum,
Cochin
Cochin 31 st Dec -2 nd
Jan 2013
Quality
HSHRC Annual Report 2012-13 59
HARYANA STATE HEALTH RESOURCE CENTRE
O
THER ACTIVITIES OF HSHRC
4.1 Website:
2.
3.
4.
5.
6.
Website is considered as the virtual face of the department in the cyber world and not merely as an electronic brochure. In order to disseminate the information about various health issues, achievements, research and activities of HSHRC through one common platform there is need of a website for the department.
Following are the main objectives for development of HSHRC Web site:
1. To establish identity of HSHRC in cyber world
To publicize activities and functions of HSHRC
To coordinate and interact with stakeholders
To provide quick access to knowledge based technical support/information
To provide/develop online data centre.
To publish articles, events and news related to HSHRC
4.2 Newsletter:
HSHRC has designed, prepared and printed newsletter (HSHRC Bulletin) from the month of June 2013. It will be printed on quarterly basis and share HSHRC
☂ s activities and their planning, research study findings, key results of HMIS data etc.
HSHRC Annual Report 2012-13 60
HARYANA STATE HEALTH RESOURCE CENTRE
I
NSTITUTIONAL PROFILE
ABOUT HSHRC
5.1 Introduction:
The Haryana State Health Resource Centre (HSHRC) came into existence in May
2012 with the formation of first Governing Body. HSHRC primarily acts as an autonomous and independent body to advise the Govt. of Haryana for strategic planning and development of Health & Family Welfare services in Haryana, which include Health planning, implementation, monitoring and evaluation of policies and programmes in the State. It creates expertise and information and develops capacities of organization in the State and districts for this purpose.
The goal of the organization is to contribute and strengthen all the efforts towards directed towards universal access to health care.
5.2 Structure:
At present there are five divisions working in HSHRC namely:
1.
Public Health Planning
2.
Human Resource for Health
3. Drug Unit
4. Quality Assurance
5. Monitoring & Evaluation
6. Public Private Partnership.
Each division is headed by Medical Officer/Senior Consultant who reports to
Executive Directors. Networking with various stake holders working in health sector is a key initiative in various activities in HSHRC. In research, QA, PPP (and others), HSHRC has entered into networking with various academic and professional organization for technical assistance, funding, collaborative activities etc.
HSHRC Annual Report 2012-13 61
HARYANA STATE HEALTH RESOURCE CENTRE
5.3 Objectives:
5.3.1. Governance
· To promote and support good governance in the Health sector.
· To assist the Govt. in framing a perspective Health Plan, Finance & Budget requirements and identify and suggest alternate and additional sources of finance.
· To advice the Govt. and provide necessary policy inputs for improving the efficiency, transparency and quality of supply chain management system and asset management procedures for drugs & equipments.
· To advice and facilitate the Govt. with respect to considering for adoption and framing of new legislations in the Health Sector.
· To assist the Govt. to formulate a comprehensive IT plan for the Health Sector.
· To provide policy inputs to the State Government on matters specifically referred.
5.3
.
2. Monitoring & Evaluation
· To provide evidence based insights on wider determinants of health outcomes for planning of the Health Sector at State, District and Sub-District levels.
· To develop a State of the art monitoring and evaluation system based on latest innovations and technology.
· To promote and undertake analytical work to continuously improve the planning, implementation, monitoring and review of the Health Sector.
· To develop and promote a system of community based monitoring of the health programmes and institutions.
5.3
.
3. Programme Management
· To promote, facilitate and improve programme planning management in the
State, District, Sub-District and facility levels.
· To be the focal point for knowledge management, documentation and dissemination of knowledge and experiences as well as good practices in health systems in India and across the world.
· To facilitate and design systems for improving transparency, accountability, community participation and technological innovations in the Health Sector.
· Mobilize financial and non financial resources for complementing/ supplementing the NRHM activities in the State.
HSHRC Annual Report 2012-13 62
HARYANA STATE HEALTH RESOURCE CENTRE
· To improve programme management through adoption of Information
Technology based management practices.
· To provide support for efficient implementation of programmes of National
Rural Health Mission and Health Directorate at State, District and Sub-District levels.
5.3.4. Quality Assurance
· To provide support for developing quality management systems at hospital levels leading to improvement of services quality and quality certification.
· To help the State develop and adopt standard protocols for providing quality policy care services.
· To undertake assessments and monitory of quality protocols adopted by the
State and suggest changes and improvements.
· To provide technical and management guidance for implementing quality protocols.
5.3.5.
Human Resource Development
· To facilitate professional Human Resource Management in the Health Sector.
· To provide support for Capacity Development of Govt. organizations at State,
District and Sub-District levels and non-government institutions.
· To identify/empanel a pool of institutions and individuals to provide capacity support.
· To facilitate induction and development of new professional skill in the system including contracting and management of consultants/institutions to meet the needs of the sector.
5.3.6. Public Private Partnership
· To help identify promote and facilitate public private participation in Health
Sector.
· To formulate and promote adoption of standard tender documents, evaluation processes and post tender monitoring for Public Private Partnership.
5.3.7
Others
· To collaborate with National and State Institutes of Health and Family Welfare,
Academic institutions specializing in Health Sector, National State and Regional and other State level Health Resource Centres and Programme Management
Units at different levels in mutually agreed areas.
HSHRC Annual Report 2012-13 63
HARYANA STATE HEALTH RESOURCE CENTRE
· To undertake any other functions entrusted to it by the State and Governing
Body Health Society.
For performing these functions/achieving these objectives the HSHRC shall:
· Establish and carry out the administration and management of the Society
☂ s
Secretariat, which will serve as the implementation arm of the Society.
· Create administrative, technical professional and other posts in the Secretariat of the Centre as deemed necessary.
· Employ/retain, dismiss personnel as required from time to time.
· Adopt its own package salary and related allowances package for its employees.
· Adopt own procurement procedures and employ the same for procurement of goods and services.
· Hire appropriate consultants/professionals/organizations on job work basis for specific tasks.
· To make rules and regulations for managing the affairs of the Society and to make additions, deletions and amendments in them from time to time as needed in the interest of the Society and Programme.
· To incur expenditure for managing the affairs of the Society.
HSHRC Annual Report 2012-13 64
HARYANA STATE HEALTH RESOURCE CENTRE
G
overning Body and Executive Committee
The Governing Board is made up of about 50% from the government and the rest being leading public health experts from academics and civil society. The Governing Body consists of 18 members. Total number of members of Governing Body can be increased or decreased, but they shall not exceed 25. The terms of the Governing Body will be for 5 years. It would be reconstituted after the period.
Members of Governing Body are as following:
1.
Principal Secretary, Health and Medical Education, Haryana.
2.
Vice Chancellor of Pt. B.D Sharma Postgraduate Institute of Medical Sciences, Rohtak or his nominee not below the rank of Head of Department
3.
Mission Director, National Rural Health Mission, Haryana.
4.
Director General Health Services, Haryana
5.
Director General Health Services, AYUSH, Haryana
6.
Director General Medical Education & Research(DMER), Haryana
7.
Director, National Rural Health Mission (NRHM)
8.
Director, Hospital Management Division (HMD), O/o DGHS
9.
Civil Surgeon, Panchkula
10.
Civil Surgeon, Mewat
11.
Dr. (Mrs.) Krishna Sangwan, (Retd.), Professor HOD Gynae and Obs. PGIMS, Rohtak, C/o
Vice Chancellor of Pt. B.D Sharma Postgraduate Institute of Medical Sciences, Rohtak
12.
Dr. Sardari Lal Verma, MD Paediatric C/o Verma Hospital, Rohtak
13.
Dr. S. B Siwatch (Retired) Professor and HOD Medicine, PGIMS, Rohtak
30/443, Siwach Hospital, Dev Colony, Delhi Road, Rohtak
14.
Dr. J.C. Dhall, Sr. Professor (Retd.) General Surgery, PGIMS, Rohtak
H.No. 1172, Sector -1, HUDA, Rohtak , 124001
15.
Dr. Virender Sangwan, MS Opth. L.V Parsad Eye Instt., Hyderabad
16.
Representative of Department of Community Medicine, School of Public Health, PGI,
Chandigarh
17.
Representative of National Health System Resource Centre, Ministry of Health and
Family Welfare, Govt. of India, New Delhi
Dr. Vandana Prashad, Paediatrician & Public Health Expert, National Commission for
Protection of Child Rights, Chanralok, Building (5 th Floor), 36, Janpath, New Delhi-1
18.
Dr. Ashish Gupta, Executive Director, HSHRC, Member Secretary (Ex- Officio)
HSHRC Annual Report 2012-13 65
HARYANA STATE HEALTH RESOURCE CENTRE
The Governing Body has full authority to exercise and perform all the acts for planning, establishment and running HSHRC.
EXECUTIVE COMMITTEE:
Members of the Executive Body are:
1.
Principal Secretary, Department of Health and Medical Education, Haryana.
2.
Mission Director, NRHM Haryana.
3.
Director General Health Services, Haryana.
4.
Director General Health Services, AYUSH, Haryana.
5.
Director, NRHM.
6.
Executive Director, HSHRC, Haryana.
Governing Body and Executive Committee both decide the annual work plan, budget and appraisal. They also review the achievements of previous year. Selection
Committee, byelaws and operational guidelines are approved by the Executive
Committee.
HSHRC Annual Report 2012-13 66
HARYANA STATE HEALTH RESOURCE CENTRE
HSHRC Annual Report 2012-13 67