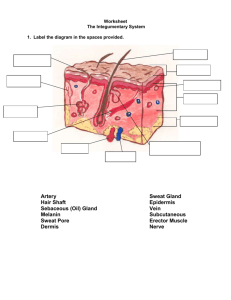
Prearrest hypothermia improved defibrillation and cardiac function in
advertisement

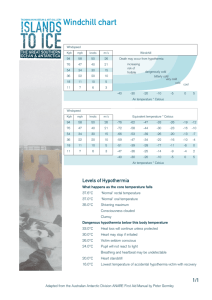
American Journal of Emergency Medicine 33 (2015) 1385–1390 Contents lists available at ScienceDirect American Journal of Emergency Medicine journal homepage: www.elsevier.com/locate/ajem Original Contribution Prearrest hypothermia improved defibrillation and cardiac function in a rabbit ventricular fibrillation model☆ Li Jiang, MM a,d,1, Chun-lin Hu, MD b,1, Zhen-Ping Wang, BMed c, Yin-Ping Li, MM d, Jian Qin, MD d,⁎ a Department of Emergency Medicine, Third Military Medical University Affiliated XinQiao Hospital, Chongqing, China Department of Emergency Medicine, the First Affiliated Hospital of Sun Yat-Sen University, Guangzhou, China Department of General Surgery, JiNan Central Hospital, JiNan, ShanDong, China d Department of Emergency Medicine, Capital Medical University Affiliated XuanWu Hospital, Beijing, China b c a r t i c l e i n f o Article history: Received 20 January 2015 Received in revised form 11 June 2015 Accepted 7 July 2015 a b s t r a c t Background: Hypothermia when cardiopulmonary resuscitation begins may help achieve defibrillation and return of spontaneous circulation (ROSC), but few data are available. Objective: The objective of this study was to determine whether prearrest hypothermia improved defibrillation and cardiac function in a rabbit ventricular fibrillation (VF) model. Results: Thirty-six New Zealand rabbits were randomized equally to receive normothermia (Norm) (~ 39°C), post-ROSC hypothermia (~33°C), or prearrest hypothermia (~33°C). Ventricular fibrillation was induced by alternating current. After 4 minutes of VF, rabbits were defibrillated and given cardiopulmonary resuscitation until ROSC or no response (≥30 minutes). Hemodynamics and electrocardiogram were monitored; N-terminal pro–brain natriuretic peptide and troponin I were determined by enzyme-linked immunosorbent assay. Myocardial histology and echocardiographic data were evaluated. First-shock achievement of perfusion rhythm was more frequent in prearrest than normothermic animals (7/12 vs 1/12; P = .027). After ROSC, dp/dtmax was higher in prearrest than normothermic animals (P b .001). Left ventricular end-systolic pressure was higher in prearrest than normothermic animals (P = .001). At 240 minutes after ROSC, troponin I and N-terminal pro–brain natriuretic peptide were lower in prearrest than normothermic animals (15.74 ± 2.26 vs 25.09 ± 1.85 ng/mL and 426 ± 23 vs 284 ± 45 pg/mL, respectively), the left ventricular ejection fraction and cardiac output were lower in the Norm group than other 2 groups (P b .01). Myocardial histology was more disturbed in normothermic than post-ROSC and prearrest animals, but was not different in the latter 2 groups. Conclusions: Induction of hypothermia before VF led to improved cardiac function in a rabbit VF model through improving achievement of perfusing rhythm by first-shock defibrillation and facilitating resuscitation. © 2015 Published by Elsevier Inc. 1. Introduction Cardiovascular disease (CVD) is the leading cause of death and disability in most industrialized nations. In China, CVD morbidity and mortality are increasing annually along with both standard of living and poor lifestyle habits. Currently in China, CVD causes about 60% of sudden cardiac deaths, making it a serious clinical and public health problem. ☆ This study was supported by funding from CPR New Theory, New Technology in Improving Cardiac Arrest Resuscitation Success Rate (xm201313). The funders had no role in the study design, data collection, analysis, decision to publish, or the preparation of the manuscript. ⁎ Corresponding author at: Department of Emergency Medicine, Capital Medical University Affiliated XuanWu Hospital, Beijing 100053, China. Tel.: +86 13910183721; fax: +86 10 83198382. E-mail address: jqin6@163.com (J. Qin). 1 These 2 authors contributed equally to this work. http://dx.doi.org/10.1016/j.ajem.2015.07.017 0735-6757/© 2015 Published by Elsevier Inc. Therapeutic hypothermia has been used for treatment of critical illnesses, including traumatic brain injury [1], refractory arrhythmias [2], cardiogenic shock syndrome [3], and decrease of infarct size in patients undergoing percutaneous coronary intervention for acute myocardial infarction [4] for more than 50 years. Systemic hypothermia initiated after cardiac arrest and resuscitation can improve survival and long-term neurologic outcome [5,6], but there are few data on the heart effects. The American Heart Association 2010 guidelines for cardiopulmonary resuscitation (CPR) recommend that comatose adult patients with out-of-hospital ventricular fibrillation (VF) and cardiac arrest be cooled to 32°C to 34°C for 12 to 24 hours after return of spontaneous circulation (ROSC). However, many unanswered questions remain, including the optimal timing for hypothermia [7]. Animal studies that induced intra-arrest or prearrest hypothermia with cooling at approximately the same time as defibrillation and CPR reported improved defibrillation or ROSC [8–14]. However, only a few studies have reported the effects of preexisting hypothermia on resuscitation and myocardial function. Additional data are needed to find ways to optimize the effectiveness of CPR. 1386 L. Jiang et al. / American Journal of Emergency Medicine 33 (2015) 1385–1390 In this study, prearrest and post-ROSC systemic hypothermia were induced in a rabbit VF model to determine whether prearrest hypothermia has a cardiac function benefit. Hemodynamic function, troponin I, and Nterminal pro–brain natriuretic peptide (NT-proBNP) levels, echocardiography, and cardiac tissue histology of the animals were monitored. 2. Materials and methods 2.1. Animal preparation Thirty-six male New Zealand rabbits weighing 2.8 to 3.5 kg were maintained under standard laboratory conditions. Anesthesia was induced with 30.0 mg/kg pentobarbital (Sigma, St Louise, MI); supplemental pentobarbital was given as required to maintain sedation. The animals were intubated and ventilated (45 breaths/min, 15 mL/kg). Arterial blood gases were monitored; physiological arterial blood pH and PO2 N 100 mm Hg were maintained by ventilation adjustments. Catheters were inserted into the femoral artery and ear marginal vein to monitor arterial blood pressure and administer medications. A pressure catheter (Kombidyn Monitoring Set, Braun, Melsungen, Germany) introduced into the left ventricle through the right carotid artery measured end diastolic and systolic pressures and the rates of positive (dp/dtmax) and negative (dp/dtmin) development. Hemodynamics and electrocardiogram (ECG) were monitored with an MP150 data acquisition system (version 3.8.1; Biopac, Goleta, CA). 2.2. Induction of hypothermia Animals were randomized to 3 treatment groups of equal size: normothermia (~39°C, Norm), cooling to ~33°C after ROSC (post-ROSC), or cooling to ~ 33°C before VF with maintenance of hypothermia after achieving ROSC (prearrest). Rabbits were cooled by placing ice bags around the head, thorax, and abdomen. The bags were removed when body temperature fell to within 0.4°C or 0.5°C above target because it continued to fall for a brief time afterward. Cooling to 34°C required 28.3 ± 3.5 minutes, ice and electric heating pads were used to maintain animals at target temperature, and rectal temperature was monitored using probes supplied with the MP150 system (Biopac). All procedures described above were completed in less than 1 hour. 2.3. Ventricular fibrillation and resuscitation Fine acupuncture needles were placed in the ventricular apex of the myocardium and the right thoracic subcutis. A 6-V, 50-Hz alternating current, was applied to the acupuncture needles until VF was confirmed by surface ECG accompanied by a fall in arterial blood pressure to near zero. After 4 minutes of VF arrest without chest compression or ventilation, rabbits were defibrillated with a commercially available biphasic waveform defibrillator (HP-1723B; Hewlett Packard, Palo Alto, CA). The first shocks were given at 10 J. Cardiopulmonary resuscitation, with chest compressions at ~ 200/min and mechanical ventilation at 45 breaths/min, was then begun. Chest compression was interrupted for no more than 5 seconds every 30 seconds to observe the ECG and measure arterial pressure. After 30 seconds, additional shocks were delivered at 30 J if needed. Epinephrine 20 μg/kg was given intravenously every 3 minutes after the first shocks as needed for continuing hypotension (arterial pressure b50 mm Hg). Cardiopulmonary resuscitation was continued until achieving ROSC, mean arterial pressure (MAP) greater than 60 mm Hg without drug infusion or continued chest compressions for 5 minutes, or no response after at least 30 minutes. No drugs were given after ROSC. MAP, dp/dtmax, dp/dtmin, left ventricular enddiastolic pressure (LVEDP), and left ventricular end-systolic pressure (LVESP) were measured using the MP150 system. Hypothermia was maintained and hemodynamics were monitored continuously for 4 hours after ROSC. No liquids were given during the study. A flow diagram of the study procedures is shown in Fig. 1. 2.4. Blood samples Blood was collected from the left ventricle at 4 hours after ROSC and centrifuged (B160A medical centrifuge, Baiyang, China) to separate the plasma. Plasma NT-proBNP and troponin I levels were determined by enzyme-linked immunosorbent assay (R&D, Minneapolis, MN). Surviving animals were euthanized with 5 mL intravenous 10% KCl. 2.5. Cardiac function study by echocardiography Echocardiography was performed with the aid of the M-Turbo Ultrasound System with a 5- to 10-MHz transthoracic echocardiographic transducer (SonoSite, Bothell, WA) on all animals at baseline and 4 hours after the ROSC. Longitudinal and transverse parasternal and 4- and 2-chamber apical views were obtained. The M-mode, 2-dimensional, and Doppler imaging were examined, and the internal dimensions were recorded. Left ventricular end-systolic (ESV) and end-diastolic volumes (EDV) were calculated by the method of Simpson, and the left ventricular ejection fraction (EF) and cardiac output (CO) were estimated. 2.6. Myocardial histology Hearts were excised immediately after the 4-hour observation period. Tissue blocks were prepared from the free left ventricular subendocardium. Briefly, tissue samples were fixed in cold 2.5% glutaraldehyde in 0.1 mol/L cacodylate buffer (pH 7.4), postfixed in 1% osmium tetroxide, dehydrated, and embedded in Epon. Random 60to 80-nm ultrathin sections were cut following stereological sampling methods without consideration of the sectioning orientation, mounted on copper grids, and stained with lead citrate and uranyl acetate. The myocardial ultrastructure was examined using an FEI Tecnai G2 transmission electron microscope equipped with a CCD camera (Gatan 832, Pleasanton, CA) at magnifications from 500 to 135 000. Eight electron micrographs were obtained randomly and sequentially from 1 section cut from a block of tissue from each animal [15]. 2.7. Calculation Descriptive data were reported as proportions and means ± SD, and statistical analysis was performed with SPSS 16.0 (SSPS Inc, Chicago, IL). The hemodynamic and echocardiographic variables were found to be normally distributed; therefore, no transformation of data was needed prior to analysis. For variables that were not normally distributed, Fig. 1. A flowchart of the experimental protocol. L. Jiang et al. / American Journal of Emergency Medicine 33 (2015) 1385–1390 nonparametric methods were used. A linear mixed-model repeatedmeasures analysis was used to compare heart rate (HR), MAP, dp/ dtmax, dp/dtmin, LVESP, and LVEDP at 30, 60, 120, 180, and 240 minutes after ROSC. Dichotomous variables were compared with 2-tailed Fisher exact and t tests. Continuous variables were compared by analysis of variance. Defibrillation and resuscitation data were tested for significance by Fisher exact test. The total number of shocks and epinephrine dosage delivered within each of the 3 groups were compared using the Kruskal-Wallis test. For all statistical analyses, a P value less than .05 was considered significant. 1387 Table 2 Defibrillation and resuscitation outcomes First-shock success First-shock perfusing rhythm ROSC achieved Norm (n = 12) Post-ROSC (n = 12) Prearrest (n = 12) 5/12 1/12⁎ 9/12 5/12 0/12⁎ 8/12 8/12 7/12 11/12 ⁎ P ≤ .05 vs prearrest. 3.3. Hemodynamic data 3. Results 3.1. Baseline A total of 36 rabbits were randomized equally to the 3 treatment groups, and their baseline characteristics are presented in Table 1. There were no differences in baseline HR, MAP, dp/dtmax, dp/dtmin, LVEDP, LVESP, body temperature, or echocardiographic data. Ventricular fibrillation was induced after induction of hypothermia in the prearrest group or at an equivalent time in other 2 groups. Heart rate and dp/dtmin were significantly lower the in the prearrest group after cooling than those in the Norm and post-ROSC groups before cardiac arrest (Table 1). Differences in MAP, dp/dtmax, LVEDP, and LVESP observed after cooling were not significant. As shown in Table 3, HR was higher in the Norm group than in the post-ROSC and prearrest groups (P b .001). There were no significant differences in MAP or LVEDP among the groups. The prearrest group, but not the post-ROSC group, had a higher dp/dtmax (P b .001) than the Norm group. dp/dtmin was lower in the post-ROSC group than in the Norm group (P = .001), but the difference in dp/dtmin in the prearrest and Norm groups was not significant. Finally, LVESP was higher in the prearrest than in the Norm group (P = .001). 3.2. Resuscitation data 3.4. Troponin I and NT-proBNP Successful defibrillation was defined as termination of VF regardless of asystole, pulseless electrical activity, or sinus rhythm. Defibrillation and resuscitation outcomes are shown in Table 2. First-shock defibrillation, that is, termination of VF with the first 10-J shock, succeeded in 5 of the 12 animals in the Norm group, 8 of 12 in the prearrest group, and 5 of 12 in the post-ROSC group. These differences were not statistically significant, and there were also no differences in the total number of defibrillation shocks delivered in each group. Seven of the 12 animals in the prearrest group achieved ROSC immediately after initial 10-J shocks without CPR or drug support compared with 1 of 12 in the Norm group (P = .027) and 0 of 12 in the post-ROSC group (P = .005). Nine of 12 animals in the Norm group, 8 of 12 in the post-ROSC group, and 11 of 12 in the prearrest group achieved ROSC. The median epinephrine dose administered in the prearrest group (0 μg/kg; range, 0-680 μg/kg) was less than those in the Norm group (66 μg/kg; range, 0-680 μg/kg; P b .05). There was no significant difference in the median epinephrine doses given in the post-ROSC (69 μg/kg; range, 58-700 μg/kg) and Norm groups. Table 1 Data at baseline and after induction of hypothermia Characteristic Norm (n = 12) Post-ROSC (n = 12) Prearrest (n = 12) Baseline HR 312 ± 21 MAP (mm Hg) 100 ± 11 dp/dtmax (mm Hg/s) 3542 ± 437 dp/dtmin (mm Hg/s) 3066 ± 598 LVEDP (mm Hg) −0.1 ± 2.0 LVESP (mm Hg) 118 ± 11 Temperature (°C) 38.9 ± 0.1 Before induction of VF HR (beats/min) 291 ± 18 MAP (mm Hg) 96 ± 6 dp/dtmax (mm Hg/s) 3034 ± 422 dp/dtmin (mm Hg/s) 3129 ± 543 LVEDP (mm Hg) 1.1 ± 0.8 LVESP (mm Hg) 110 ± 13 Temperature (°C) 38.8 ± 0.2 Values are means ± SEM. ⁎ P ≤ .05 compared with Norm. ⁎⁎ P ≤ .05 compared with post-ROSC. 295 ± 26 96 ± 8 3402 ± 305 2769 ± 191 1.2 ± 3.0 119 ± 10 38.9 ± 0.1 293 ± 21 102 ± 10 3413 ± 356 2939 ± 466 1.1 ± 1.9 123 ± 12 39.0 ± 0.2 300 ± 16 97 ± 6 2932 ± 341 2909 ± 258 2.1 ± 1.6 106 ± 17 38.8 ± 0.1 211 ± 16⁎,⁎⁎ 96 ± 14 3052 ± 225 2278 ± 362⁎,⁎⁎ 1.6 ± 1.5 106 ± 12 33.3 ± 0.1⁎,⁎⁎ Prearrest cooling decreased troponin I and NT-proBNP levels after ROSC. At 240 minutes, troponin I concentration was significantly lower in the prearrest than in the Norm group (15.74 ± 2.26 vs 25.09 ± 1.85 ng/mL, P b .001), but there was no significant difference in concentration between the Norm and post-ROSC groups (25.09 ± 1.85 vs 23.48 ± 2.66 ng/mL, P N .05). The NT-proBNP concentration was 426 ± 23 pg/mL in the Norm group at 240 minutes after ROSC, which was significantly higher than the concentrations of 360 ± 69 pg/mL observed in the post-ROSC group (P = .002) and 284 ± 45 pg/mL in the prearrest group (P b .002). The NT-proBNP concentration observed in the prearrest group was significantly lower than that of the post-ROSC group (P = .006). 3.5. Echocardiographic data As in Table 4, at 240 minutes after ROSC, the EF and CO were lower in the Norm group than in the other 2 groups (P b .01). End-diastolic volume of the prearrest group is bigger than that of the Norm group (P b .01). Also, the EF and CO in the post-ROSC group were lower those in than prearrest group (P b .05 and P b .01, respectively). 3.6. Myocardial histology Morphologic changes were more pronounced in cells from rabbits in the Norm group. The myocardial fibers were obviously disordered, mitochondria were severely swollen, and the cristae were vague, arranged irregularly. In the other 2 groups, the heart morphologic structure was much better, and myocardial fibers and mitochondrial crista structure was clearer (Fig. 2). 4. Discussion In this study, defibrillation was carried out before chest compression, as that is more feasible in hospitalized intensive care patients than in those experiencing out-of hospital cardiac arrest. In the prearrest group, ROSC occurred in 7 rabbits after the first shock and without any chest compressions, which has not been reported in similar studies. The mechanism by which hypothermia affects defibrillation is not known. Buckberg et al [16] found that hypothermia during 1388 L. Jiang et al. / American Journal of Emergency Medicine 33 (2015) 1385–1390 Table 3 Hemodynamic data 30 to 240 minutes after achieving ROSC 30 min HR (beats/min), mean ± SEM Norm (n = 9) Post-ROSC (n = 8) Prearrest (n = 9) MAP (mm Hg) mean ± SEM Norm (n = 9) Post-ROSC (n = 8) Prearrest (n = 9) dp/dtmax (mm Hg/s), mea ± SEM Norm (n = 9) Post-ROSC (n = 8) Prearrest (n = 9) dp/dtmin (mm Hg/s), mean ± SEM Norm (n = 9) Post-ROSC (n = 8) Prearrest (n = 9) LVEDP (mm Hg), mean ± SEM Norm (n = 9) Post-ROSC (n = 8) Prearrest (n = 9) LVESP (mm Hg), mean ± SEM Norm (n = 9) Post-ROSC (n = 8) Prearrest (n = 9) 60 min 293 ± 40 208 ± 30⁎ 227 ± 18⁎ 289 ± 21 219 ± 16⁎ 226 ± 19⁎ 77 ± 16 76 ± 6 78 ± 12 79 ± 10 77 ± 6 77 ± 12 2337 ± 484 2267 ± 148 2625 ± 346 2192 ± 297 2200 ± 402 2814 ± 395⁎ 2344 ± 482 1768 ± 184⁎⁎ 2212 ± 534 120 min 292 ± 27 220 ± 21⁎ 243 ± 21⁎ 180 min 240 min 292 ± 31 230 ± 10⁎ 234 ± 19⁎ 289 ± 38 229 ± 17⁎ 229 ± 22⁎ 72 ± 10 79 ± 4 85 ± 9⁎ 73 ± 11 79 ± 4 85 ± 10⁎ 2177 ± 390 2193 ± 476 2814 ± 444⁎ 2371 ± 507 2391 ± 383 2876 ± 351⁎⁎ 2374 ± 525 2388 ± 426 2866 ± 389⁎⁎ 2199 ± 372 1776 ± 352⁎⁎ 2166 ± 271 2245 ± 464 1779 ± 349⁎⁎ 2134 ± 327 2454 ± 345 1823 ± 413⁎ 2343 ± 301 2389 ± 443 1858 ± 502⁎⁎ 2368 ± 278 7.7 ± 2.8 6.9 ± 3.5 3.7 ± 3.4 5.6 ± 1.6 5.8 ± 1.6 5.4 ± 1.1 5.7 ± 1.9 4.9 ± 3.3 5.7 ± 1.6 5. 8 ± 0.9 5.7 ± 1.6 5. 3 ± 1.1 5.5 ± 1.2 5.7 ± 1.7 5.4 ± 1.1 91 ± 14 96 ± 10 105 ± 11⁎⁎ 95 ± 5 94 ± 10 107 ± 9⁎ 86 ± 11 96 ± 13 108 ± 13⁎ 93 ± 13 100 ± 9 109 ± 10⁎ 94 ± 13 100 ± 9 109 ± 11⁎ 72 ± 12 75 ± 6 84 ± 11⁎⁎ ⁎ P ≤ .01 vs Norm. ⁎⁎ P ≤ .05 vs Norm. defibrillation decreased energy requirements as evidenced by reduced oxygen consumption by the myocardium. Balaji et al [2] reported that systemic hypothermia led to a decrease in the occurrence of arrhythmia in patients with resistant automatic-focus tachycardias. Hypothermia might reduce injury to myocardial cell mitochondria [17] and the cardiac sympathetic nerve activity [18] that is associated with ventricular tachyarrhythmias [19]. A better understanding of how hypothermia affects defibrillation will help optimize CPR. Diastolic function in prearrest group was inferior to that in the Norm group when hypothermia was induced, but systolic function was less affected. This result is similar to previously published findings of Fischer et al [20] and Post et al [21]. However, diastolic function in prearrest and Norm group animals after ROSC did not differ even if the hypothermia effect it negatively, and systolic function was better in the prearrest rabbits at that time. Hemodynamic properties were better (closer to baseline values) in the prearrest group than in the Norm group, and cardiac function from echocardiography was the best in the 3 groups. Troponin I was significantly less elevated in the prearrest group than in the other 2 groups. However, the histology of myocardial cells from Norm rabbits was more disturbed than that of cells from both post-ROSC Table 4 Echocardiographic data at baseline and at 240 minutes after the ROSC Baseline ROSC 4 h EDV (mm3) ESV (mm3) EF CO (mL/min) EDV (mm3) ESV (mm3) EF CO (mL/min) Norm Post-ROSC Prearrest 286.98 ± 19.48 102.86 ± 7.61 0.64 ± 0.01 77.77 ± 3.63 167.43 ± 44.52 114.37 ± 34.11 0.32 ± 0.06 27.73 ± 4.80 280.77 ± 11.42 101.27 ± 5.93 0.64 ± 0.01 78.08 ± 3.79 181.35 ± 50.54 93.10 ± 28.43 0.48 ± 0.07⁎ 44.17 ± 3.66⁎ 266.80 ± 45.12 93.67 ± 19.03 0.65 ± 0.02 71.96 ± 10.66 252.76 ± 14.07⁎ 104.80 ± 7.01 0.59 ± 0.01⁎,⁎⁎ 62.93 ± 4.09⁎,⁎⁎⁎ Values are means ± SEM. ⁎ P ≤ .01 compared with Norm. ⁎⁎ P ≤ .05 compared with post-ROSC. ⁎⁎⁎ P ≤ .01 compared with post-ROSC. and prearrest rabbits, which did not differ markedly in appearance. Thus, no matter when hypothermia is induced, it may protect the myocardium [22–24]. Overall, the results show that improvement in myocardial function cannot be directly attributed to the effects of hypothermia and that some other factors may have contributed to the observed improvement in myocardial performance. First, resuscitation was easier in the prearrest group, less defibrillation and epinephrine was needed, and less cardiac function may have been lost. Second, because of hypothermia, the prearrest group might have experienced less cardiac injury after VF than the other 2 groups did. Third, delayed cooling might have resulted in decreased protection of myocardial function. Hypothermia was induced in this animal model before cardiac arrest; which occurs in fibrillation during hypothermic therapy or cold injury. For postcardiac arrest patients, hypothermia is widely adopted as a protective intervention and some hypothermic patients will redevelop VF [25]. We need more data about effect of hypothermia on defibrillation success. The American Heart Association guidelines 2010 do not specifically state when cooling of patients should begin. Some studies have evaluated the benefits of therapeutic hypothermia initiated during CPR [26–28]. Some investigators have suggested that hypothermia should be initiated as soon as possible, even intra-arrest [29,30]. Intraarrest cooling may become feasible in a clinical setting in the future with development of rapid cooling techniques, such as liquid ventilation of the lungs with temperature-controlled perfluorocarbons. In rabbits, these techniques have been shown to decrease left atrial [31,22,32] or esophageal temperature [33] to 32°C in 5 minutes. Ultrafast cooling may become practical in humans, and in the future, maybe we would cool down cardiac arrest patients before CPR and then resuscitate under conditions of hypothermia in order to facilitate resuscitation. 4.1. Limitations Some study limitations should be mentioned. First, it was not possible to blind investigators to the animals' body temperature. Second, the mechanism of the hypothermia effect on resuscitation was not investigated. Third, the cardiac arrest model was a dysrhythmic arrest caused by electrical shock and not caused by ischemia, which is considered as the most common cause of death from CVD. L. Jiang et al. / American Journal of Emergency Medicine 33 (2015) 1385–1390 1389 Fig. 2. Representative electron micrographs of subendocardial mitochondria. The myocardial fibers were obviously disordered (magnification at ×18 500, scale bar = 500 nm). A close look at single mitochondrion of each group. Ultrastructural changes of mitochondria, including swelling and decreased cristae disintegration, were more discernible in the Norm group and moderate in the post-ROSC group and in the prearrest group (magnification at ×23 650, scale bar = 100 nm). 5. Conclusion Induction of hypothermia before VF led to improved cardiac function in a rabbit VF model through improving achievement of perfusing rhythm by first-shock defibrillation and facilitating resuscitation. Acknowledgments This study was supported by funding from CPR New Theory, New Technology in Improving Cardiac Arrest Resuscitation Success Rate (xm201313). The funders had no role in the study design, data collection, analysis, decision to publish, or the preparation of the manuscript. References [1] Fritz HG, Bauer R. Secondary injuries in brain trauma: effects of hypothermia. J Neurosurg Anesthesiol 2004;16(1):43–52. [2] Balaji S, Sullivan I, Deanfield J, James I. Moderate hypothermia in the management of resistant automatic tachycardias in children. Br Heart J 1991;66(3):221–4. [3] Ofoma UR, Ramar K, Kashyap R. Mild therapeutic hypothermia in cardiogenic shock syndrome. Crit Care Med 2013;41(2):e14–5. [4] Zobel C, Adler C, Kranz A, Seck C, Pfister R, Hellmich M, et al. Mild therapeutic hypothermia in cardiogenic shock syndrome. Crit Care Med 2012;40(6):1715–23. [5] Dixon SR, Whitbourn RJ, Dae MW, Grube E, Sherman W, Schaer GL, et al. Induction of mild systemic hypothermia with endovascular cooling during primary percutaneous coronary intervention for acute myocardial infarction. J Am Coll Cardiol 2002; 40(11):1928–34. [6] Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med 2002;346(8):549–56. [7] Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W, Gutteridge G, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med 2002;346(8):557–63. [8] Menegazzi JJ, Rittenberger JC, Suffoletto BP, Logue ES, Salcido DD, Reynolds JC, et al. Effects of pre-arrest and intra-arrest hypothermia on ventricular fibrillation and resuscitation. Resuscitation 2009;80(1):126–32. [9] Wang H, Barbut D, Tsai MS, Sun S, Weil MH, Tang W. Intra-arrest selective brain cooling improves success of resuscitation in a porcine model of prolonged cardiac arrest. Resuscitation 2010;81(5):617–21. [10] Boddicker KA, Zhang Y, Zimmerman MB, Davies LR, Kerber RE. Hypothermia improves defibrillation success and resuscitation outcomes from ventricular fibrillation. Circulation 2005;111(24):3195–201. [11] Tsai MS, Barbut D, Tang W, Wang H, Guan J, Wang T, et al. Rapid head cooling initiated coincident with cardiopulmonary resuscitation improves success of defibrillation and post-resuscitation myocardial function in a porcine model of prolonged cardiac arrest. J Am Coll Cardiol 2008;51(20):1988–90. [12] Abella BS, Zhao D, Alvarado J, Hamann K, Vanden HTL, Becker LB. Intra-arrest cooling improves outcomes in a murine cardiac arrest model. Circulation 2004;109(22): 2786–91. [13] Rhee BJ, Zhang Y, Boddicker KA, Davies LR, Kerber RE. Effect of hypothermia on transthoracic defibrillation in a swine model. Resuscitation 2005;65(1): 79–85. [14] Staffey KS, Dendi R, Brooks LA, Pretorius AM, Ackermann LW, Zamba KD, et al. Liquid ventilation with perfluorocarbons facilitates resumption of spontaneous circulation in a swine cardiac arrest model. Resuscitation 2008;78(1):77–84. [15] Hu CL, Li H, Xia JM, Li X, Zeng X, Liao XX, et al. Ulinastatin improved cardiac dysfunction after cardiac arrest in New Zealand rabbits. Am J Emerg Med 2013;31(5): 768–74. [16] Buckberg GD, Brazier JR, Nelson RL, Goldstein SM, McConnell DH, Cooper N. Studies of the effects of hypothermia on regional myocardial blood flow and metabolism during cardiopulmonary bypass. I. The adequately perfused beating, fibrillating, and arrested heart. J Thorac Cardiovasc Surg 1977;73(1): 87–94. [17] Ning XH, Xu CS, Portman MA. Mitochondrial protein and HSP70 signaling after ischemia in hypothermic-adapted hearts augmented with glucose. Am J Physiol 1999;277(1 Pt 2):R11–7. [18] Helwig BG, Parimi S, Ganta CK, Cober R, Fels RJ, Kenney MJ. Aging alters regulation of visceral sympathetic nerve responses to acute hypothermia. Am J Physiol Regul Integr Comp Physiol 2006;291(3):R573–9. [19] Jardine DL, Charles CJ, Frampton CM, Richards AM. Cardiac sympathetic nerve activity and ventricular fibrillation during acute myocardial infarction in a conscious sheep model. Am J Physiol Heart Circ Physiol 2007;293(1):H433–9. [20] Fischer UM, Cox CS, Laine GA, Mehlhorn U, Allen SJ. Mild hypothermia impairs left ventricular diastolic but not systolic function. J Invest Surg 2005;18:291–6. [21] Post H, Schmitto JD, Steendijk P, Christoph J, Holland R, Wachter R, et al. Cardiac function during mild hypothermia in pigs: increased inotropy at the expense of diastolic dysfunction. Acta Physiol (Oxf) 2010;199(1):43–52. [22] Chenoune M, Lidouren F, Ghaleh B, Couvreur N, Dubois-Rande J-L, Berdeaux A, et al. Rapid cooling of the heart with total liquid ventilation prevents transmural myocardial infarction following prolonged ischemia in rabbits. Resuscitation 2010;81: 359–62. [23] Tsai MS, Barbut D, Wang H, Guan J, Sun S, Inderbitzen B, et al. Intra-arrest rapid head cooling improves postresuscitation myocardial function in comparison with delayed postresuscitation surface cooling. Crit Care Med 2008;36:S434–9. [24] Lee JH, Suh GJ, Kwon WY, Kim KS, Rhee JE, Kim MA, et al. Protective effects of therapeutic hypothermia in post-resuscitation myocardium. Resuscitation 2012;83: 633–9. [25] Koster Rudolph W, Walker Robert G, Chapman Fred W. Recurrent ventricular fibrillation during advanced life support care of patients with prehospital cardiac arrest. Resuscitation 2008;78:252–7. [26] Bruel C, Parienti JJ, Marie W, Arrot X, Daubin C, Du Cheyron D, et al. Mild hypothermia during advanced life support: a preliminary study in out-of-hospital cardiac arrest. Crit Care 2008;12(1):R31. [27] Kamarainen A, Virkkunen I, Tenhunen J, Yli-Hankala A, Silfvast T. Prehospital induction of therapeutic hypothermia during CPR: a pilot study. Resuscitation 2008; 76(3):360–3. [28] Garrett JS, Studnek JR, Blackwell T, Vandeventer S, Pearson DA, Heffner AC, et al. The association between intra-arrest therapeutic hypothermia and return of spontaneous circulation among individuals experiencing out of hospital cardiac arrest. Resuscitation 2011;82(1):21–5. [29] Nagao K. Therapeutic hypothermia following resuscitation. Minerva Anestesiol 2011;77:927–33. 1390 L. Jiang et al. / American Journal of Emergency Medicine 33 (2015) 1385–1390 [30] Taccone FS, Donadello K, Beumier M, Scolletta S. When, where and how to initiate hypothermia after adult cardiac arrest. Minerva Anestesiol 2011;77:927–33. [31] Tissier R, Couvreur N, Ghaleh B, Bruneval P, Lidouren F, Morin D, et al. Rapid cooling preserves the ischaemic myocardium against mitochondrial damage and left ventricular dysfunction. Cardiovasc Res 2009;83(2):345–53. [32] Tissier R, Hamanaka K, Kuno A, Parker JC, Cohen MV, Downey JM. Total liquid ventilation provides ultra-fast cardioprotective cooling. J Am Coll Cardiol 2007;49(5):601–5. [33] Chenoune M, Lidouren F, Adam C, Pons S, Darbera L, Bruneval P, et al. Ultrafast and whole-body cooling with total liquid ventilation induces favorable neurological and cardiac outcomes after cardiac arrest in rabbits. Circulation 2011;124(8):901–11 [1-7].