Clinical and Population Studies
HDL Remodeling During the Acute Phase Response
Anisa Jahangiri, Maria C. de Beer, Victoria Noffsinger, Lisa R. Tannock, Chandrashekar Ramaiah,
Nancy R. Webb, Deneys R. van der Westhuyzen, Frederick C. de Beer
Downloaded from http://atvb.ahajournals.org/ by guest on October 2, 2016
Objective—The purpose of this study was to examine the interactive action of serum amyloid A (SAA), group IIA secretory
phospholipase A2 (sPLA2-IIA), and cholesteryl ester transfer protein (CETP) on HDL remodeling and cholesterol efflux
during the acute phase (AP) response elicited in humans after cardiac surgery.
Methods and Results—Plasma was collected from patients before (pre-AP), 24 hours after (AP-1 d), and 5 days after
cardiac surgery (AP-5 d). SAA levels were increased 16-fold in AP-1 d samples. The activity of sPLA2-IIA was
increased from 77.7⫾38.3 U/mL (pre-AP) to 281.4⫾57.1 U/mL (AP-1 d; P⬍0.001). CETP mass and activity reduction
was commensurate to the reduction of HDL cholesterol levels. The combined action of SAA, sPLA2-IIA, and CETP in
vitro markedly remodeled HDL with the generation of lipid-poor apoA-I from both pre-AP and AP-1 d HDL. The net
result of this remodeling was a relative preservation of ABCA1- and ABCG1-dependent cholesterol efflux during the
acute phase response.
Conclusions—Our results show that the many and complex changes in plasma proteins during the acute phase response
markedly remodel HDL with functional implications, particularly the relative retention of cholesterol efflux capacity.
(Arterioscler Thromb Vasc Biol. 2009;29:261-267.)
Key Words: SAA 䡲 HDL 䡲 CETP 䡲 apoA-I 䡲 inflammation
I
nflammation induces major changes in HDL levels and
composition. Mediators of inflammation such as tumor
necrosis factor (TNF)-␣ and interleukin (IL)-6 induce expression of serum amyloid A1 and group IIA secretory phospholipase A2 (sPLA2-IIA),2 which dramatically alter HDL apolipoprotein content and levels, respectively. Acute phase
SAA in the plasma is associated with HDL, where it can
comprise the major apolipoprotein.3 The increase in sPLA2IIA activity results in hydrolysis of HDL surface phospholipids and a decrease in HDL particle size.4 The plasma
cholesteryl ester transfer protein (CETP) is an integral component of reverse cholesterol transport and regulates HDL
cholesterol concentrations. By promoting the transfer of
cholesteryl esters (CE) from HDL to apoB-containing lipoprotein particles, HDL-derived CE is taken up via the LDL
receptor and cleared by the liver.5 An additional result of
CETP action is the generation of lipid-poor apoA-I,6 a key
acceptor in ATP-binding cassette transporter AI (ABCA1)mediated lipid efflux.7 The presence of SAA on HDL holds
the potential to impact both the CE transfer and the apoA-I
liberating ability of CETP. sPLA2-IIA could also impact the
latter action of CETP as apoA-I was shown to dissociate more
readily from CETP-remodeled reconstituted HDL after hydrolysis by bee venom phospholipase A2.8
Given the centrality of inflammation in atherogenesis,
there is a paucity of information regarding CETP function
when acute phase HDL is the “substrate.” In the present
study, we used plasma from patients undergoing cardiac
surgery with cardiopulmonary bypass as a “standardized”
insult where the oxygenator membrane activates macrophages to produce cytokines.9 We characterized the SAAcontaining acute phase (AP) HDL during the acute phase to
define the polydisperse HDL “substrate” that CETP would
encounter. We further investigated CETP function in the
acute phase, particularly as it relates to the presence of SAA
and sPLA2 on AP HDL, with respect to its CE transfer and
apoA-I liberating functions.
Teleologically, the dramatic changes in HDL composition
and metabolism during inflammation must serve a short-term
purpose to allow the organism to survive a noxious assault.
Acute tissue injury results in cell death with large quantities
of cell membranes rich in phospholipids and cholesterol
generated. Macrophages are mobilized to such sites, ingest
these fragments, and acquire considerable lipid load.10 We
thus examined the influence of the AP response on the ability
of serum to promote cholesterol efflux as a removal mechanism to mobilize this cholesterol in an ABCA1- and ABCG1dependent manner.
Received January 7, 2008; revision accepted October 30, 2008.
From the Department of Internal Medicine, Division of Endocrinology and Molecular Medicine (A.J., V.N., L.R.T., N.R.W., D.R.v.d.W., F.C.d.B.),
the Departments of Surgery (C.R.) and Physiology (M.C.d.B.), the Cardiovascular Research Center (A.J., M.C.d.B., V.N., L.R.T., N.R.W., D.R.v.d.W.,
F.C.d.B.), and the Graduate Center for Nutritional Sciences (A.J., M.C.d.B., V.N., L.R.T., N.R.W., D.R.v.d.W., F.C.d.B.), University of Kentucky; and
Veterans Affairs Hospital (L.R.T., F.C.d.B.), Lexington, Ky.
Correspondence to Anisa Jahangiri, PhD, Rm 525 CT Wethington Bldg, 900 S Limestone Street, Lexington, KY 40536. E-mail anisa.jahangiri@
uky.edu
© 2009 American Heart Association, Inc.
Arterioscler Thromb Vasc Biol is available at http://atvb.ahajournals.org
261
DOI: 10.1161/ATVBAHA.108.178681
262
Arterioscler Thromb Vasc Biol
February 2009
at discharge, 5 days after surgery (AP-5 d) as outlined in the
supplemental materials (available online at http://atvb.ahajournals.
org). This study was approved by the University of Kentucky
Medical Institutional Review Board (IRB). For the full descriptions
of the methods used, please see the supplemental materials.
Statistical Analyses
Data are presented as mean⫾SEM. Differences between pre-AP and
AP parameters were tested by paired t test (SigmaStat 3.5). Statistical
analyses between pre-AP, AP-1 d, and AP-5 d were performed using
repeated measures 1-way ANOVA with the Holm-Sidak multiple
comparisons test. Significance was set at P⬍0.05. A Wilcoxon
signed rank test was used for post test of CETP mass. The power in
all tests was ⬎0.9.
Results
SAA, sPLA2, CETP, and HDL in AP Plasma
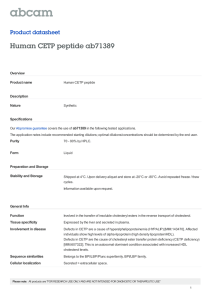
Figure 1. SAA (A) and sPLA2 (B) concentrations in pre-AP, AP-1
d, and AP-5 d plasma. Data are presented as mean⫾SEM;
n⫽12 (SAA), n⫽6 (sPLA2); *P⬍0.05 vs pre-AP by 1-way
repeated measures ANOVA.
Methods
Human Subjects
Patients undergoing cardiac surgery donated plasma before (preacute
phase, pre-AP), 24 hours postoperatively (acute phase, AP-1 d), and
B
3
2
**
1
0
pre-AP
C
AP- 1d
D
450
400
350
300
250
200
150
100
50
0
***
ApoA-I (µg/ml)
CETP(µg/ml)
4
CETP activity (nmoles CE/ml/h)
A
HDL-C (µg/ml)
Downloaded from http://atvb.ahajournals.org/ by guest on October 2, 2016
As expected, plasma SAA levels increased from pre-AP
levels of 47.2⫾19.9 g/mL to 785.6⫾66.4 g/mL in AP-1 d
samples (P⬍0.05) and were still elevated at discharge (AP-5
d; 567.2⫾50.2 g/mL; P⬍0.05; Figure 1A). The activity of
sPLA2-IIA followed a similar pattern: 77.7⫾38.3 U/mL
(pre-AP), 281.4⫾57.1 U/mL (AP-1 d), and 250.5⫾43 U/mL
(AP-5 d; P⬍0.05; Figure 1B). Quantitative immunoblot
analysis showed a 2.9-fold reduction in CETP mass from
2.6⫾0.6 g/mL in pre-AP plasma to 0.9⫾0.2 g/mL in AP-1
d plasma, (Figure 2A P⬍0.01). Consistent with this, CETP
activity was 2.2-fold lower in AP compared to pre-AP plasma
(16.9⫾3.0 nmol/mL/h and 37.9⫾4.1 nmol/mL/h respectively,
P⬍0.001; Figure 2B). HDL-C levels were reduced 1.9-fold,
from 372.2⫾44.6 g/mL to 195.0⫾22.2 g/mL (P⬍0.001;
Figure 2C), and apoA-I dropped from 1590.0⫾84.2 g/mL to
771.4⫾138.7 g/mL (P⬍0.001; Figure 2D). The decrease in
60
50
40
30
***
20
10
0
pre-AP
AP- 1d
2000
1500
***
1000
500
0
pre-AP
AP- 1d
pre-AP
AP- 1d
Figure 2. CETP, HDL cholesterol, and apoA-I are reduced in AP-1 d plasma. A, Plasma CETP concentrations were quantified by densitometric analysis of Western blots. CETP activity (B), HDL-C concentrations (C), and apoA-I (D) concentrations in pre-AP and AP-1 d
plasma. **P⬍0.01, ***P⬍0.001 by paired t test.
Jahangiri et al
B
A
apoA-I
263
pre-AP HDL on anti AII
apoA-I
apoA-II
SAA
apoA-II
preAP
C
Remodeling of AP HDL
AP- 1d SAA-HDL
pre- AP
HDL
D
AP- 1d HDL on anti SAA
FT
E1
E2
AP- 1d HDL on anti AII
apoA-I
apoA-II
SAA
Downloaded from http://atvb.ahajournals.org/ by guest on October 2, 2016
AP- 1d FT
HDL
E1
E2
E3
E4
AP- 1d FT
HDL
E1
E2
E3 E4
E5
Figure 3. Apolipoprotein characterization of pre-AP HDL, AP-1 d HDL, and SAA-HDL (A) SDS gel of HDL (5 g total protein). (B) 125Ipre-AP HDL (5 g) was passed through an anti–apoA-II immunoaffinity column and fractions were electrophoresed and autoradiographed as outlined in the methods (ARG). (C) 125I-AP HDL (10 g) was passed through an anti-SAA immunoaffinity column with subsequent electrophoresis and ARG as described in B. (D) 125I-AP HDL (10 g) was passed through an anti–apoA-II immunoaffinity
column with subsequent electrophoresis and ARG as described in B. Note: the gels in B through D were loaded on the basis of 2000
cpm per lane, and because the majority of counts were present in E1 and E2, E3 through E5 quantitatively represent a smaller percentage of total protein mass.
CETP activity was commensurate with the reduction in
HDL-C and apoA-I, hence the activity of CETP normalized
to HDL-C or apoA-I levels was not different between pre-AP
and AP plasma (not shown).
Characterization of Pre-AP and AP HDL by
Immunoaffinity Chromatography
It was reported that the presence of apoA-II on reconstituted
HDL particles inhibits the CETP-mediated dissociation of
apoA-I.11 To assess the influence of SAA, we studied pre-AP
and AP-1 d HDL as well as HDL2 enriched in vitro with SAA
(SAA-HDL). We subjected 125I-HDL to immunoaffinity
chromatography to determine the proportion of the LpAI
fraction (ie, HDL particles lacking both apoA-II and SAA,
and containing only apoA-I) in AP HDL. Figure 3A is a
Coomassie-stained SDS-PAGE gel showing the major apolipoproteins present in these HDL. Whereas SAA is virtually
undetectable in pre-AP HDL, it is a major component of AP-1
d HDL (27.2% of total protein by mass). In SAA-HDL, SAA
comprised a major apolipoprotein. Figure 3B shows the
autoradiograph (ARG) of the SDS-PAGE analysis of the
fractions when pre-AP HDL was passed through an anti–
apoA-II column so that the FT comprises only LpAI particles.
ApoA-II– containing particles were eluted from the column
with sequential chaotropic washes (E1 and E2). In pre-AP
HDL, 84% of the total apoA-I counts were in LpAI particles,
indicating abundant CETP substrate.
When AP-1 d HDL was passed through an anti-SAA
column, 20% of the total apoA-I counts and approximately
5% of the apoA-II counts were in the FT, the remainder
associated with SAA-containing particles (Figure 3C). Thus,
80% of apoA-I in AP HDL was present on particles that also
contained SAA or both SAA and apoA-II. This indicates that
less than 20% of apoA-I in AP HDL is present on LpA-I
particles that contain neither apoA-II nor SAA. Specificity of
the column was verified with pre-AP HDL passed through the
same column. This resulted in 97% of the counts being
retrieved in the FT indicating negligible nonspecific binding.
In the case of AP HDL passed through an anti–apoA-II
column (Figure 3D), 66% of the apoA-I counts and 52% of
the SAA counts in AP HDL were in the FT fraction. This
indicated that SAA was distributed relatively equally between
particles that contain only apoA-I and those that contain both
apoA-I and apoA-II. The majority of apoA-I in AP HDL
(66%) was present in particles containing no apoA-II, as in
the case of pre-AP HDL. However, the majority of such
particles contained additional SAA (Figure 3C and 3D),
reducing the LpAI fraction in AP HDL.
Comparative Displacement of ApoA-I in Pre-AP
and AP HDL by CETP
Because ultracentrifugation displaces CETP from HDL,12
recombinant CETP was exogenously added in the remodeling
experiments. The CETP activity in the incubations corresponded to the activity of CETP in normal human plasma.
When the total pre-AP and AP HDL were incubated with
CETP in vitro for 24 hours, a dose-dependent dissociation of
apoA-I was observed (Figure 4A). The dissociation of apoA-I
from pre-AP and AP HDL was comparable. Although it
appears that 50% or more of the apoA-I is in the lipid-poor
state, the enhanced immunoreactivity of dissociated apoA-I
precludes exact quantification. In addition to generating
lipid-poor apoA-I, CETP action also resulted in the formation
of larger HDL particles which are likely TG-enriched because
264
Arterioscler Thromb Vasc Biol
Diameter
(nm)
February 2009
A
B
pre-AP HDL
anti-apoA-I
AP- 1d HDL
anti-SAA
AP- 1d HDL
anti-apoA-I
17.0
12.2
10.4
8.16
7.1
Lipidpoor apo AI
Lipidpoor SAA
CETP
(μg/mg HDL)
0
1
2
4
0
1
2
4
0
1
2
4
Figure 4. Dissociation of lipid-poor apoA-I from pre-AP and AP-1 d HDL after remodeling by CETP. HDLs were incubated with CETP in
the presence of VLDL for 24 hours at 37°C as outlined in the methods. Reactions were analyzed by Western blot for (A) apoA-I and (B)
SAA. The migration of lipid-poor apoA-I and SAA are marked with arrows.
Downloaded from http://atvb.ahajournals.org/ by guest on October 2, 2016
of CE/TG exchange. CETP action on AP HDL liberated a
very limited amount of “lipid-poor” SAA (Figure 4B).
Recombinant SAA exhibited slower mobility than apoA-I on
gradient gels, likely because of increased aggregation under
the nondenaturing conditions (Figure 4B). SAA is dispersed
on a broader spectrum of particle sizes, some likely containing little apoA-I (compare Figure 4A lane 8 and Figure 4B
lane 4).
lane 3). Surface hydrolysis of HDL phospholipids by sPLA2
action alone resulted in a reduction in HDL particle size not
accompanied by the dissociation of apoA-I or SAA (Figure
5A, 5B, 5C, lane 2). However the combined action of sPLA2
and CETP converted the majority of the apoA-I from the
HDL-bound to the lipid-poor form in both HDL2 and SAAHDL (Figure 5A and 5B, lane 4). This combined action may
also result in the dissociation of limited amounts of lipid-poor
SAA from SAA-HDL(Figure 5C, lane 4). We conclude that
CETP action on the core, and sPLA2-IIA hydrolysis on the
HDL surface, synergize to liberate lipid-poor apoA-I.
Comparative Displacement of ApoA-I in Pre-AP
and AP HDL by Concomitant Action of CETP
and sPLA2-IIA
ABCA1 and ABCG1-Dependent Cholesterol Efflux
During the acute phase, dissociation of apoA-I from HDL
could be influenced by acute phase secretory phospholipase
(ie, sPLA2-IIA), which is present in plasma and associates
with HDL.13 We thus used SAA-HDL (Figure 1A) to study
the remodeling of HDL by CETP and sPLA2-IIA. Treatment
of SAA-HDL with CETP alone resulted in the generation of
comparable amounts of lipid-poor apoA-I (Figure 5B, lane 3)
as observed with control HDL2 (Figure 5A, lane 3). CETP
treatment did not result in the displacement of significant
amounts of lipid-poor SAA from SAA-HDL2 (Figure 5C,
A
Diameter (nm)
To test the effects of the acute phase response on HDL
function, efflux assays were carried out using pre-AP, AP-1
d, and AP-5 d serum diluted to 2.5%. When compared to
pre-AP serum, ABCA1-dependent efflux was not significantly decreased at AP-1 d despite a highly significant 53%
fall in plasma apoA-I concentrations (Table). At AP-5 d,
ABCA1 efflux was still maintained despite apoA-I remaining
1.5-fold lower than pre-AP levels. Similarly, ABCG1 efflux
was modestly reduced at AP-1 d, whereas HDL-C decreased
C
B
HDL2
anti-apoA-I
SAA-HDL
anti-apoA-I
SAA-HDL
anti-SAA
17.0
12.2
10.4
8.16
Lipidpoor SAA
7.1
Lipidpoor apoA-I
sPLA2 (μg/mg HDL) CETP (μg/mg HDL) -
2
-
2
2
2
apo
A-I
-
2
-
2
2
2
-
2
-
2
2 SAA
2
Figure 5. The combined action of sPLA2-IIA and CETP on HDL2 and SAA-HDL. HDL were incubated with sPLA2-IIA and CETP as set
out in the methods. Reactions were analyzed by Western blot for apoA-I in (A) HDL2 and (B) SAA-HDL and (C) SAA blot of SAA-HDL.
Jahangiri et al
Table. Cellular Cholesterol Efflux During the Acute Phase
Response
Pre-AP
AP-1 Day
AP-5 Days
ABCA1-efflux (% of pre-AP)
100
82.5⫾3.5
99.2⫾2.9
ABCG1- efflux (% of pre-AP)
100
70.0⫾14.3a 108.5⫾16.7
Plasma apoA-I (g/ml)
Plasma HDL-C (g/ml)
1161.7⫾117.6b 545.0⫾62.4
389.7⫾60.5
785.0⫾36.6
196.6⫾39.1c 238.7⫾27.9
ABCA1- and ABCG1-dependent cholesterol efflux was determined as
outlined in the methods. Efflux experiments were performed at 37°C by
incubating cells with serum (diluted to 2.5%) from patients pre-AP, AP-1 d, and
AP-5 d for 16 hours in DMEM containing 0.2% BSA. Values represent the
average of triplicate determinations of n⫽6 to 8 patients. Results are presented
as a percentage of pre-AP serum efflux. ApoA-I was measured using an
automated turbidimetric immunoassay (Mayo Medical Laboratories). HDL was
quantitated using a commercial kit. aP⬍0.05 vs pre-AP and AP-5 d; b P⬍0.001
vs AP-1 d and AP-5 d; c P⬍0.5 vs pre-AP.
Downloaded from http://atvb.ahajournals.org/ by guest on October 2, 2016
by 48.1%. When efflux was normalized to HDL-C concentrations, there was a doubling in the ABCG1-dependent
cholesterol efflux efficiency of AP-1 d serum compared to
pre-AP serum, and this was maintained at AP-5 d. Thus
cholesterol efflux appears to be relatively well maintained in
the acute phase response despite large reductions in HDL-C
and apoA-I.
Discussion
Data presented here indicate the following: (1) The reduction
in CETP concentration and activity during the acute phase
response is commensurate with the reduction in HDL levels.
(2) Despite the striking alterations in HDL composition
during the acute phase, CETP activity was maintained both
with respect to its cholesteryl ester transfer function and its
capacity to liberate apoA-I. (3) sPLA2-IIA enhances the
ability of CETP to liberate apoA-I, and this is not impaired by
the presence of SAA on the HDL. (4) Although SAA has
been shown to be an effective acceptor in lipid efflux, CETP
action liberates it to a limited extent in a lipid-poor form. (5)
The interplay between the numerous acute phase proteins
impacting HDL remodeling result in the relative preservation
of ABCA1- and ABCG1-dependent cholesterol efflux.
There is an inverse relationship between CETP activity and
HDL concentrations in the normal state.14 This was the basis
for developing CETP inhibitors to increase HDL levels for
potential therapeutic benefit. During inflammation this inverse relationship does not hold as both CETP and HDL
levels are reduced. Studies have shown that inflammatory
cytokines reduce CETP transcription and levels.15,16 This
could result in increased HDL levels. However, our data
shows a commensurate decrease in HDL and CETP in the
acute phase. This suggests that during inflammation factors
operate to reduce HDL despite the normal tendency of CETP
to increase HDL. A number of mechanisms could operate to
decrease plasma HDL during the acute phase. It was originally assumed that SAA enrichment of HDL was the basis for
decreased apoA-I and HDL levels. However, this is unlikely
because the decrease in plasma HDL during inflammation
occurs rapidly, before SAA accumulation.17 An alternative
explanation for decreased HDL levels during inflammation
could be remodeling by acute phase group II phospholipases,
Remodeling of AP HDL
265
particularly sPLA2-IIA, which increases HDL catabolism.18,19
SAA itself can also enhance the activity of sPLA2.20 The
proinflammatory cytokines that induce SAA and sPLA2-IIA,
simultaneously decrease apoA-I expression.21 Thus the decreased levels of apoA-I and increased levels of SAA on HDL
during inflammation are attributable at least in part to
reciprocal coordinated regulation. Finally, the combined remodeling action of sPLA2-IIA and CETP during the acute
phase response (Figure 5) may also result in the increased
catabolism of HDL. Given the numerous factors that operate
during inflammation it is notable that the ratio of CETP to
HDL is maintained. CETP reduction during inflammation
could be viewed as a defensive adaptation to prevent “excessive” HDL reduction mediated by the mechanisms discussed.
It was reported that apoA-II abrogates the CETP-mediated
liberation of apoA-I from reconstituted HDL containing both
apoA-I and apoA-II.11 In pre-AP HDL, we demonstrated that
approximately 80% of apoA-I is present in LpAI particles
(Figure 3B). Lipid-poor apoA-I dissociating from pre-AP
HDL in our study is thus likely derived from these LpAI
particles. In contrast, in AP HDL, less than 20% of the apoA-I
was present as LpAI, the remainder being associated with
SAA and/or apoA-II (Figure 3C). However, CETP action
resulted in the liberation of the bulk of apoA-I from AP HDL.
This establishes that SAA, in contrast to apoA-II, does not
interfere with the liberation of apoA-I induced by CETP
remodeling.
Our data indicate that SAA is present on most AP HDL
particles (Figure 3C). Unlike SAA, CETP is present as a
dynamic exchange protein rather than a structural protein and
undergoes rapid bidirectional transfer between HDL particles
and acceptors. At any given time, only ⬇1 in 1000 HDL
particles carry a CETP molecule. The fact that the activity of
CETP when normalized to HDL-C is unaltered during the
acute phase suggests that CETP dynamics are also unchanged
during the APR. Our results strongly suggest that any
decrease in total cholesteryl ester transfer from HDL during
the acute phase is the result of the concomitant reduction of
plasma CETP and HDL-C rather than the reduced functionality of the HDL/CETP interaction.
It is notable that CETP action results in an apparent
increase in size of the HDL particles (Figures 4 and 5). In
addition to liberating apoA-I, CETP-mediated remodeling has
been reported to result in particle fusion.22 The increased
particle size of CETP-remodeled HDL may also relate to the
exchange of CE for TG by CETP action. As TG molecules
are larger than CE molecules, HDL size would increase as TG
content increases.23 CETP action on HDL results in core/
surface disequilibrium that is alleviated by the dissociation of
lipid-poor apoAI.24 Notably, in our study, CETP-remodeling
of HDL resulted in both an increase in size of the particles, as
well as the dissociation of lipid-poor apoA-I. Increased
sPLA2-IIA activity during the acute-phase response may
further potentiate the generation of lipid-poor apoA-I.
The increased sPLA2 activity in acute phase plasma (Figure 1B) is likely attribtuable to an increase in sPLA2-IIA.25
sPLA2-IIA was shown to be present in atherosclerotic plaques
bound to heparan-sulfate proteoglycans of the subendothelial
extracellular matrix.2 Proteoglycan binding of sPLA2-IIA
266
Arterioscler Thromb Vasc Biol
February 2009
Downloaded from http://atvb.ahajournals.org/ by guest on October 2, 2016
serves to “concentrate” the enzyme, and it is more active in
the bound form.26 Thus the effect of sPLA2-IIA on HDL
remodeling may be more pronounced in the intima of a
vessel. Furthermore, sPLA2 is more active when SAA is
present on HDL.20 It may also be relevant that like sPLA2,
SAA is also bound by proteoglycans in lesions.27 Although
efflux of cholesterol from macrophages at this site represents
only a small fraction of overall cellular cholesterol efflux, it
is critically protective in the context of atherosclerosis.7 The
interaction of sPLA2 and SAA might constitute a defensive
mechanism against lipid accumulation. SAA-HDL is particularly enriched in SAA compared to AP HDL, with SAA
present on 80% of particles.3 In our study, CETP action on
SAA-HDL liberated significant amounts of lipid-poor
apoA-I. This confirms that the presence of SAA does not
impair the dissociation of apoA-I. In our study, there was
no clear evidence that SAA was significantly displaced in
a lipid-poor form by either CETP or sPLA2-IIA (Figures 4
and 5), though one has to recognize the limitations of
analyzing SAA on nondenaturing gels as its tendency to
self-aggregate and associate with the acrylamide matrix is
well established.
Given the extensive remodeling of HDL during the acute
phase that affects both the polydisperse particles themselves
as well as the equilibrium between bound and free apolipoproteins, we evaluated the integral of all these actions on
ABCA1- and ABCG1-dependent cholesterol efflux. We show
an overall preservation of cholesterol efflux capacity of
serum during the acute phase response. A large body of
evidence suggested that HDL is part of the innate immune
system,28 and that acute phase HDL remodeling could impact
the unique cargo of proteins on HDL,29 reducing its antiinflammatory functions. For example, the incorporation of
SAA and sPLA2-IIA onto AP HDL particles results in the
loss of paraoxonase activity of HDL.30 During acute injury
when macrophages accumulate lipid, relative preservation
have more impact of efflux mechanisms could not only by
altering the antiinflammatory nature of HDL, but also by
depleting HDL levels and cholesterol acceptors than the
impairment of the antiinflammatory properties of HDL.
However, during chronic inflammatory conditions, the
latter might constitute a much more important risk factor
for atherogenesis.
Inhibition of CETP results in elevated HDL levels,14 but
this could abrogate its two antiatherogenic functions. The
recent cessation of a human clinical trial testing such an
inhibitor31 illustrates the need to better understand CETP
function, not only on circulating lipoproteins, but also on
apoA-I liberation at the level of the atherosclerotic lesion in
the vessel wall. One can imagine a scenario where CETP
inhibition could increase plasma HDL but also alter the
equilibrium between HDL and lipid-poor apoA-I and consequently efflux potential. Our results indicate that AP HDL is
not impaired in its ability to liberate apoA-I after CETP
remodeling. This combined with the potentiation of apoA-I
release by the combined action of CETP and the acute phase
sPLA2-IIA, supports our results showing that during the acute
phase, cholesterol effluxing capacity may be preserved despite a reduction of plasma HDL. However, prolonged
inflammation and continual HDL remodeling may eventually
lead to proatherogenic conditions by limiting the levels of
HDL and apolipoprotein cholesterol acceptors and the proinflammatory nature of AP HDL having an impact.
Acknowledgments
The authors acknowledge the technical assistance of John Cranfill, Nathan Whitaker, Nick Whitaker, Matt Mains, and
Connie Dampier.
Sources of Funding
This study was supported by an NIH Program Project Grant
(PO1HL086670; to D.R.v.d.W.) and a VA Merit Review Funded by
Veterans Affairs (VACO to F.C.D.).
Disclosures
None.
References
1. Cabana VG, Siegel JN, Sabesin SM. Effects of the acute phase response
on the concentration and density distribution of plasma lipids and apolipoproteins. J Lipid Res. 1989;30:39 – 49.
2. Menschikowski M, Hagelgans A, Siegert G. Secretory phospholipase A2
of group IIA: is it an offensive or a defensive player during atherosclerosis and other inflammatory diseases? Prostaglandins Other Lipid
Mediat. 2006;79:1–33.
3. Coetzee GA, Strachan AF, van der Westhuyzen DR, Hoppe HC, Jeenah
MS, de Beer FC. Serum amyloid A-containing human high density
lipoprotein 3. Density, size, and apolipoprotein composition. J Biol Chem.
1986;261:9644 –9651.
4. de Beer FC, de Beer MC, van der Westhuyzen DR, Castellani LW, Lusis
AJ, Swanson ME, Grass DS. Secretory non-pancreatic phospholipase A2:
influence on lipoprotein metabolism. J Lipid Res. 1997;38:2232–2239.
5. Barter PJ. Hugh sinclair lecture: the regulation and remodelling of HDL
by plasma factors. Atheroscler Suppl. 2002;3:39 – 47.
6. Rye KA, Hime NJ, Barter PJ. The influence of cholesteryl ester transfer
protein on the composition, size, and structure of spherical, reconstituted
high density lipoproteins. J Biol Chem. 1995;270:189 –196.
7. Lewis GF, Rader DJ. New insights into the regulation of HDL metabolism and reverse cholesterol transport. Circ Res. 2005;96:
1221–1232.
8. Rye KA, Duong MN. Influence of phospholipid depletion on the size,
structure, and remodeling of reconstituted high density lipoproteins. J
Lipid Res. 2000;41:1640 –1650.
9. Hacquebard M, Ducart A, Schmartz D, Malaisse WJ, Carpentier YA.
Changes in plasma LDL and HDL composition in patients undergoing
cardiac surgery. Lipids. 2007;42:1143–1153.
10. Tam SP, Ancsin JB, Tan R, Kisilevsky R. Peptides derived from serum
amyloid A prevent, and reverse, aortic lipid lesions in apoE-/- mice. J
Lipid Res. 2005;46:2091–2101.
11. Rye KA, Wee K, Curtiss LK, Bonnet DJ, Barter PJ. Apolipoprotein A-II
inhibits high density lipoprotein remodeling and lipid-poor apolipoprotein
A-I formation. J Biol Chem. 2003;278:22530 –22536.
12. Tall AR. Plasma cholesteryl ester transfer protein. J Lipid Res. 1993;34:
1255–1274.
13. Gijon MA, Perez C, Mendez E, Sanchez Crespo M. Phospholipase A2
from plasma of patients with septic shock is associated with high-density
lipoproteins and C3 anaphylatoxin: some implications for its functional
role. Biochem J. 1995;306:167–175.
14. de Grooth GJ, Klerkx AH, Stroes ES, Stalenhoef AF, Kastelein JJ,
Kuivenhoven JA. A review of CETP and its relation to atherosclerosis. J
Lipid Res. 2004;45:1967–1974.
15. Hardardottir I, Moser AH, Fuller J, Fielding C, Feingold K, Grunfeld C.
Endotoxin and cytokines decrease serum levels and extra hepatic protein
and mRNA levels of cholesteryl ester transfer protein in syrian hamsters.
J Clin Invest. 1996;97:2585–2592.
16. Masucci-Magoulas L, Moulin P, Jiang XC, Richardson H, Walsh A,
Breslow JL, Tall A. Decreased cholesteryl ester transfer protein (CETP)
mRNA and protein and increased high density lipoprotein following
lipopolysaccharide administration in human CETP transgenic mice.
J Clin Invest. 1995;95:1587–1594.
Jahangiri et al
Downloaded from http://atvb.ahajournals.org/ by guest on October 2, 2016
17. Khovidhunkit W, Kim MS, Memon RA, Shigenaga JK, Moser AH,
Feingold KR, Grunfeld C. Effects of infection and inflammation on lipid
and lipoprotein metabolism: mechanisms and consequences to the host. J
Lipid Res. 2004;45:1169 –1196.
18. de Beer FC, Connell PM, Yu J, de Beer MC, Webb NR, van der
Westhuyzen DR. HDL modification by secretory phospholipase A(2)
promotes scavenger receptor class B type I interaction and accelerates
HDL catabolism. J Lipid Res. 2000;41:1849 –1857.
19. Tietge UJ, Maugeais C, Cain W, Grass D, Glick JM, de Beer FC, Rader
DJ. Overexpression of secretory phospholipase A(2) causes rapid
catabolism and altered tissue uptake of high density lipoprotein cholesteryl ester and apolipoprotein A-I. J Biol Chem. 2000;275:
10077–10084.
20. Pruzanski W, de Beer FC, de Beer MC, Stefanski E, Vadas P. Serum
amyloid A protein enhances the activity of secretory non-pancreatic
phospholipase A2. Biochem J. 1995;309:461– 464.
21. Han CY, Chiba T, Campbell JS, Fausto N, Chaisson M, Orasanu G,
Plutzky J, Chait A. Reciprocal and coordinate regulation of serum
amyloid A versus apolipoprotein A-I and paraoxonase-1 by inflammation
in murine hepatocytes. Arterioscler Thromb Vasc Biol. 2006;26:
1806 –1813.
22. Rye KA, Hime NJ, Barter PJ. Evidence that cholesteryl ester transfer
protein-mediated reductions in reconstituted high density lipoprotein size
involve particle fusion. J Biol Chem. 1997;272:3953–3960.
23. Borggreve SE, De Vries R, Dullaart RP. Alterations in high-density
lipoprotein metabolism and reverse cholesterol transport in insulin
resistance and type 2 diabetes mellitus: role of lipolytic enzymes, lecithin:
cholesterol acyltransferase and lipid transfer proteins. Eur J Clin Invest.
2003;33:1051–1069.
Remodeling of AP HDL
267
24. Rye KA, Barter PJ. Formation and metabolism of prebeta-migrating,
lipid-poor apolipoprotein A-I. Arterioscler Thromb Vasc Biol. 2004;24:
421– 428.
25. Nevalainen TJ, Eerola LI, Rintala E, Laine VJ, Lambeau G, Gelb MH.
Time-resolved fluoroimmunoassays of the complete set of secreted phospholipases A2 in human serum. Biochim Biophys Acta. 2005;1733:
210 –223.
26. Sartipy P, Johansen B, Camejo G, Rosengren B, Bondjers G, HurtCamejo E. Binding of human phospholipase A2 type II to proteoglycans.
J Biol Chem. 1996;271:26307–26314.
27. O’Brien KD, McDonald TO, Kunjathoor V, Eng K, Knopp EA, Lewis K,
Lopez R, Kirk EA, Chait A, Wight TN, deBeer FC, LeBoeuf RC. Serum
amyloid A and lipoprotein retention in murine models of atherosclerosis.
Arterioscler Thromb Vasc Biol. 2005;25:785–790.
28. Barter PJ, Nicholls S, Rye KA, Anantharamaiah GM, Navab M,
Fogelman AM. Antiinflammatory properties of HDL. Circ Res. 2004;95:
764 –772.
29. Vaisar T, Pennathur S, Green PS, Gharib SA, Hoofnagle AN, Cheung
MC, Byun J, Vuletic S, Kassim S, Singh P, Chea H, Knopp RH, Brunzell
J, Geary R, Chait A, Zhao XQ, Elkon K, Marcovina S, Ridker P, Oram
JF, Heinecke JW. Shotgun proteomics implicates protease inhibition and
complement activation in the antiinflammatory properties of HDL. J Clin
Invest. 2007;117:746 –756.
30. Van Lenten BJ, Hama SY, de Beer FC, Stafforini DM, McIntyre TM,
Prescott SM, La Du BN, Fogelman AM, Navab M. Anti-inflammatory
HDL becomes pro-inflammatory during the acute phase response. Loss of
protective effect of HDL against LDL oxidation in aortic wall cell
cocultures. J Clin Invest. 1995;96:2758 –2767.
31. Cholesterol: the good, the bad, and the stopped trials. Lancet. 2006;
368:2034.
Downloaded from http://atvb.ahajournals.org/ by guest on October 2, 2016
HDL Remodeling During the Acute Phase Response
Anisa Jahangiri, Maria C. de Beer, Victoria Noffsinger, Lisa R. Tannock, Chandrashekar
Ramaiah, Nancy R. Webb, Deneys R. van der Westhuyzen and Frederick C. de Beer
Arterioscler Thromb Vasc Biol. 2009;29:261-267; originally published online November 13,
2008;
doi: 10.1161/ATVBAHA.108.178681
Arteriosclerosis, Thrombosis, and Vascular Biology is published by the American Heart Association, 7272
Greenville Avenue, Dallas, TX 75231
Copyright © 2008 American Heart Association, Inc. All rights reserved.
Print ISSN: 1079-5642. Online ISSN: 1524-4636
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://atvb.ahajournals.org/content/29/2/261
Data Supplement (unedited) at:
http://atvb.ahajournals.org/content/suppl/2008/11/14/ATVBAHA.108.178681.DC1.html
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published
in Arteriosclerosis, Thrombosis, and Vascular Biology can be obtained via RightsLink, a service of the
Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for
which permission is being requested is located, click Request Permissions in the middle column of the Web
page under Services. Further information about this process is available in the Permissions and Rights
Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Arteriosclerosis, Thrombosis, and Vascular Biology is online
at:
http://atvb.ahajournals.org//subscriptions/
Methods
Human subjects
Patients undergoing cardiac surgery (coronary artery bypass, valve replacement) using a
membrane oxygenator, donated blood prior to (pre-acute phase, pre-AP), 24 hr post-operatively
(acute phase, AP- 1d), and at discharge, 5 days after surgery (AP- 5d). This study was
approved by the University of Kentucky Medical Institutional Review Board (IRB) and blood was
only collected from patients who underwent successful uncomplicated surgery and who gave
informed consent.
Blood sampling
Blood was collected into EDTA-tubes. Plasma was isolated after a 10 min centrifugation at 530
x g and stored at minus 80ºC after addition of protease inhibitor (aprotinin (2 µg/ml)).
Measurements of SAA, sPLA2, CETP, HDL-C and apoA-I were performed on individual patient
plasma samples. Due to IRB restrictions, only small volumes of blood could be obtained from
each patient. This necessitated the pooling of plasma from 4 – 7 patients for HDL isolation. The
HDL remodeling studies are representative of two such HDL preparations. For efflux studies,
plasma was clotted in a glass tube using 25 mM CaCl21.
Measurement of plasma proteins and lipids
Plasma SAA levels were determined by ELISA (Biosource International, Camarillo, CA). CETP
activity was determined using the Roar Biomedical kit (NY, New York). sPLA2 activity was
measured
according
to
the
protocol
of
Wooton-Kee
using
1-palmitoyl-2-oleoyl1
phosphatidylglycerol (POPG) as a substrate2. Plasma CETP and apoA-I was determined by
densitometric scanning of Western blots (Kodak 1D, New Haven, CT). Briefly, 1 µl of plasma
from patients was separated by 4 – 20% SDS-PAGE, transferred onto a PVDF membrane and
immunoblotted using either anti-human CETP TP2 (University of Ottawa, Canada) or antihuman apoA-I (Calbiochem, San Diego, CA). A standard curve was obtained from the same gel
by quantifying the densitometric signal produced by four different amounts of recombinant
human CETP (Cardiovascular Targets, Inc, NY) or apoA-I (Biodesign International, Saco,
Maine). CETP or apoA-I mass in plasma samples was determined by densitometric analysis
against this standard. HDL-cholesterol levels were determined using a commercial kit (Wako
Diagnostics, Richmond, VA). For the efflux experiments, apoA-I was measured using an
automated turbidimetric immunoassay (Mayo Medical Laboratories, Rochester, MN). Total
protein was measured by the Lowry method3.
HDL isolation
Pre-AP and AP- 1d HDL (1.063 < ρ < 1.21 g/ml) were isolated from pooled patient plasma by
sequential ultracentrifugation as described4, dialyzed against 150 mM NaCl, 0.01% (w/v) EDTA
(pH 7.4), sterile filtered and stored at 4ºC under argon gas. VLDL was isolated from normal
volunteers by ultracentrifugation (ρ < 1.019 g/ml), dialyzed and stored as above. SAA-HDL was
prepared by incubating 1.4 mg HDL2 with 1 mg recombinant human SAA (Biovision, Mountain
View, CA) for 4 hr at room temperature. The SAA-HDL was recovered by ultracentrifugation (ρ <
1.25 g/ml), dialyzed and stored as above.
2
In vitro HDL remodeling
Pre-AP and AP- 1d HDL (0.7-0.9 mg/ml total HDL protein, 30 µg apoA-I) were incubated in a
final reaction volume of 50 µl in Tris-buffered saline, pH 7.4 at 37ºC for 24 hr with human
recombinant CETP (0, 1, 2 or 4 µg per mg HDL protein, Cardiovascular Targets, Inc, NY),
human VLDL (4 mM final triglyceride concentration), fatty-acid free bovine serum albumin (BSA)
(10 mg/ml) and CaCl2 (2 mM). We attempted to make our incubations as close as possible to
physiological conditions, by using physiological concentrations of HDL, CETP, VLDL, calcium
and albumin. In order to allow the HDL remodeling to proceed to completion, reactions were
incubated for 24 hr. These methods are comparable to those employed in the literature 5,6,7.
Reactions were terminated by the addition of EDTA (final concentration 20 mM). Human VLDL
was used as a cholesteryl ester acceptor and triglyceride donor for CETP action. SAA-HDL (1
mg/ml) was incubated with CETP (2 µg/mg HDL) and human recombinant sPLA2-IIA (2 µg/mg
HDL) under the same conditions described above. The purity of the recombinant CETP was
assessed by SDS-gel electrophoresis which showed only one band corresponding to the size of
CETP at ~ 70kDa. The specific activity was reported by the manufacturer at 25 fold over normal
human plasma. In the in vitro studies, we used CETP at physiological concentrations (approx 1
in 25 dilution of the stock CETP) which is in the activity range of CETP in vivo.
Gradient gel electrophoresis and Western blots
Aliquots of incubation mixtures (1 µg apoA-I) were electrophoresed on 4-20% non-denaturing
polyacrylamide gels for 3.5 hr at 200 V, 4ºC. They were then transferred to PVDF membranes
(100 min at 100 V at 4ºC) for subsequent Western blotting with anti-human apoA-I (Calbiochem)
or anti-human SAA (Behring, Germany) antibodies. Bound antibodies were detected by
enhanced chemiluminescence (GE Healthcare, NJ).
3
Immunoaffinity chromatography
HDL was radiolabeled by the iodine monochloride method8 and characterized using the Seize®
Primary Mammalian Immunoprecipitation kit (Pierce, Rockford, IL). Briefly, immunoaffinity spin
columns were made containing anti-SAA or anti-apoA-II antibodies (200 µg antibody/ 200 µl
coupling gel) according to the manufacturer’s instructions.
125
I-labeled pre-AP and AP HDL (10
µg total protein) was allowed to bind to the column (with rotation) overnight at 4ºC. Unbound
HDL particles (flow through, FT) were spun down (1 min at 1180 x g). After 5 washes with 400
µl Tris-buffered saline (pH 7.4), the bound HDL was eluted using 200 µl elution buffer containing
a primary amide (pH 2.8) into 10 µl of 1M Tris (pH 9.5) to give a final pH of 7.4. Equal counts
(2000 dpm) of the FT and eluted fractions (E1-E5) were subjected to SDS-PAGE using 4 – 20%
acrylamide gels and analyzed by subsequent autoradiography (ARG).
Cholesterol Efflux
ABCA1-dependent cholesterol efflux was determined in skin fibroblasts isolated from normal
and Tangier disease patients as described previously9. Cells were labeled with 0.2 µCi/ml
[3H]cholesterol in medium for 48 h. Cellular ABCA1 expression was stimulated with free
cholesterol loading by incubating fibroblasts with 30 µg/ml cholesterol in medium containing
0.2% fatty acid-free BSA for 48 h. Total cellular efflux was calculated following overnight
incubation in 300 µl serum-free DMEM containing 0.2% fatty acid-free BSA and 2.5% pre-AP,
AP- 1d or AP- 5d AP- 5d serum. ApoA-I (10 µg/ml) was used as a positive control. ABCA1specific efflux was calculated by subtracting the value obtained in Tangier disease fibroblasts
from the value in normal fibroblasts. ABCG1-dependent cholesterol efflux was determined in
mock- and ABCG1 transfected cells as described previously 10. Cells were labeled as described
above and treated with 10 nM mifepristone for 18 hr prior to efflux experiments which were
4
carried out as outlined above. ABCG1-dependent cholesterol was calculated as the difference in
cholesterol efflux between mock- and ABCG1 transfected cells. HDL (25 µg/ml) was used as a
positive control). All the cell lines were kindly provided by Dr. John Oram (University of
Washington).
5
References
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
Asztalos BF, de la Llera-Moya M, Dallal GE, Horvath KV, Schaefer EJ, Rothblat GH.
Differential effects of HDL subpopulations on cellular ABCA1- and SR-BI-mediated
cholesterol efflux. J Lipid Res. 2005;46:2246-2253.
Wooton-Kee CR, Boyanovsky BB, Nasser MS, de Villiers WJ, Webb NR. Group V
sPLA2 hydrolysis of low-density lipoprotein results in spontaneous particle aggregation
and promotes macrophage foam cell formation. Arterioscler Thromb Vasc Biol.
2004;24:762-767.
Lowry OH, Rosebrough NJ, Farr AL, Randall RJ. Protein measurement with the folin
phenol reagent. J. Biol. Chem. 1951;193:265-275.
Coetzee GA, Strachan AF, van der Westhuyzen DR, Hoppe HC, Jeenah MS, de Beer
FC. Serum amyloid A-containing human high density lipoprotein 3. Density, size, and
apolipoprotein composition. J Biol Chem. 1986;261:9644-9651.
Rye KA, Hime NJ, Barter PJ. The influence of cholesteryl ester transfer protein on the
composition, size, and structure of spherical, reconstituted high density lipoproteins. J
Biol Chem. 1995;270:189-196.
Rye KA, Wee K, Curtiss LK, Bonnet DJ, Barter PJ. Apolipoprotein A-II inhibits high
density lipoprotein remodeling and lipid-poor apolipoprotein A-I formation. J Biol Chem.
2003;278:22530-22536.
Rye KA, Hime NJ, Barter PJ. Evidence that cholesteryl ester transfer protein-mediated
reductions in reconstituted high density lipoprotein size involve particle fusion. J Biol
Chem. 1997;272:3953-3960.
Bilheimer DW, Eisenberg S, Levy RI. The metabolism of very low density lipoprotein
proteins. I. Preliminary in vitro and in vivo observations. Biochim Biophys Acta.
1972;260:212-221.
van der Westhuyzen DR, Cai L, de Beer MC, de Beer FC. Serum amyloid A promotes
cholesterol efflux mediated by scavenger receptor B-I. J Biol Chem. 2005;280:3589035895.
Vaughan AM, Oram JF. ABCG1 redistributes cell cholesterol to domains removable by
high density lipoprotein but not by lipid-depleted apolipoproteins. J Biol Chem.
2005;280:30150-30157.
6