Optical Spectroscopy Guided by Structural and Functional MRI for
advertisement

OPTICAL SPECTROSCOPY GUIDED BY STRUCTURAL AND FUNCTIONAL MRI FOR BREAST
CANCER IMAGING
A Thesis
Submitted to the Faculty
In partial fulfillment of the requirements for the
degree of
Doctor of Philosophy
by
Colin M. Carpenter
Thayer School of Engineering
Dartmouth College
Hanover, New Hampshire
June 2009
Examining Committee
Chairman ___________________
Keith D. Paulsen
Member ___________________
Brian W. Pogue
Member ____________________
Solomon G. Diamond
Member ___________________
Hamid Dehghani
Member ___________________
David A. Boas
_____________________
Brian W. Pogue
Dean of Graduate Studies
_____________________
(Signature of Author)
© 2009 Trustees of Dartmouth College
Abstract
Magnetic Resonance (MR)-guided Diffuse Optical Imaging is an emerging technique to
improve breast cancer imaging. This modality combines the high sensitivity of breast
MR with images of tissue physiology, including blood content, oxygen saturation, and
water fraction, which help differentiate benign and malignant lesions. This information
may aid in reducing the high false-positive rates in breast MR that result in invasive
biopsy procedures.
MR supplements optical imaging by providing high spatial resolution images of
tissue properties that improve optical imaging. Conversely, optical imaging provides MR
with additional tissue characteristics that help classify lesions and quantify MR contrasts
such as blood oxygenation. The goal of this thesis was to develop the foundation and
methodology for comprehensively merging these modalities.
A custom-designed fiber interface and MR breast coil were constructed to improve
data quality and improve fiber positioning. The system correctly classified malignant
from non-malignant lesions, yielding greater than 50% lesion to background contrast in
cancers. In one case, it correctly assessed a tissue region that was incorrectly identified
by MRI.
Optical imaging is typically hampered by the non-ideal spectral limitations of the
photodetectors. Incorporating the water content via MR water/fat imaging decreased
quantification error of blood content by ~10% in simulation, and 70% in phantom
imaging, due to the reduction in crosstalk between water and oxyhemoglobin.
Optical imaging and Blood Oxygen Level Dependent (BOLD) MRI were used to
monitor changes in breast tissue due to respiratory gas stimulation. Results showed a
ii
consistent (p<0.05) and significant hemodynamic response (p<0.05) in normal tissues
with an oxygen/carbogen gas stimulus. In 2 tumor cases, results showed a significant
decrease in the modulation of tumor hemoglobin compared to the healthy tissue (p<0.05).
In addition, the first reported results combining BOLD and optics in the breast showed
significant correlation of deoxyhemoglobin (p<0.05).
Finally, a comprehensive image formation model that incorporated MR spatial and
functional images was demonstrated.
This methodology provides a foundation for
quantitatively accurate images with high temporal and spatial resolution.
The techniques developed in this thesis demonstrate the potential of MR-guided
optics to characterize breast cancer, and to aid the understanding of MR contrasts.
iii
Acknowledgements
I sincerely thank my advisor, Brian Pogue, for his guidance, enthusiasm, encouragement,
and generosity during my thesis. Brian has been a role model for both career and
community life, and I am certain that his influence has opened all the doors I would want
in my career. Brian demonstrates the qualities that make engineers invaluable: the
intuition of what will work, and the skills to make them work. His willingness to include
his graduate students in critical decisions, research grants, and conferences, has made us
more confident, more practical, and more efficient. If I have learned by example at
Thayer, I am a better because of it.
Certainly not second on this list, I sincerely thank Keith Paulsen, my other
advisor. Keith’s familial attitude and drive to innovate is the very essence of what makes
the Thayer School an ideal institution for study. His tenacity in research is inspirational,
and his support of the research teams creates an environment where shared resources and
knowledge accelerate progress. I only hope to model my career from Keith’s example.
I am grateful to Shudong Jiang for her assistance and guidance in research, which
I am sure shaved 3 years off my Ph.D. by providing the background I needed to learn
medical imaging instrumentation. Shudong has devoted countless hours to the successful
completion of the experimental work in this thesis
I thank my friends, especially Scott Davis, for being a great friend, helping me
avoid the pitfalls that would have lessened my Ph.D. experience, and critically discussing
the nuts and bolts with me. I thank my long-time Thayer friends Phil, Dax, Dave, Jon,
Phani, Kara, and Clara for providing the happy times that let me clear my mind to
approach a problem from a different perspective. I appreciate the support and friendship
iv
from my group mates. I also thank Dan Lynch and Hamid Dehghani for their advice and
support during my time at Thayer.
Finally, I thank my wife Katie for her patience and support during my long hours
in the office, and her enduring radiance, which inspired me to remain steadfast in solving
a problem. I also thank my mom and dad for their encouragement, and my family for
helping to take my mind off of research every once in a while.
v
Dedication
To my wife Katie and the rest of my family.
vi
Table of Contents
Approval Page..................................................................................................................... ii
Abstract ............................................................................................................................... ii
Acknowledgements............................................................................................................ iv
Dedication .......................................................................................................................... vi
Table of Contents.............................................................................................................. vii
List of Tables ..................................................................................................................... xi
List of Figures and Illustrations ........................................................................................ xii
List of Symbols, Abbreviations and Nomenclature....................................................... xxiv
CHAPTER ONE: INTRODUCTION..................................................................................1
1.1 Overview....................................................................................................................1
1.2 Current state of breast cancer imaging ......................................................................1
1.3 Imaging breast cancer with Magnetic Resonance......................................................2
1.4 Imaging breast cancer with optics .............................................................................3
1.5 Improving optical breast imaging with MRI .............................................................4
1.6 Organization of this Thesis ........................................................................................5
CHAPTER TWO: INSTRUMENTATION FOR MR GUIDED DIFFUSE OPTICAL
SPECTROSCOPIC IMAGING ..................................................................................7
2.1 Introduction................................................................................................................7
2.2 System Operation.......................................................................................................8
2.3 Serial spectroscopic imaging ...................................................................................10
2.4 Dynamic spectroscopic imaging..............................................................................12
2.5 Light illumination ....................................................................................................14
2.6 Light detection .........................................................................................................16
2.6.1 PMT calibration...............................................................................................16
2.6.2 Noise characterization .....................................................................................19
2.7 Patient interface .......................................................................................................23
2.8 Optical Magnetic Resonance mammography coil ...................................................27
2.9 Conclusions..............................................................................................................28
CHAPTER THREE: IMAGING HEMOGLOBIN, WATER, LIPID, AND SCATTER
WITH OPTICAL TOMOGRAPHY .........................................................................31
3.1 Introduction..............................................................................................................31
3.2 Image formation.......................................................................................................34
3.3 Weight Matrices.......................................................................................................35
3.3.1 Incorporating structural information from MR ...............................................36
3.3.2 Incorporating quantitative information from MR............................................38
3.4 Derivation of the inverse solution............................................................................39
3.5 Alternate formulations .............................................................................................41
3.5.1 Tikhonov..........................................................................................................41
3.5.2 Levenberg-Marquardt......................................................................................41
3.6 Conclusions..............................................................................................................42
vii
CHAPTER FOUR: METHODS OF ANATOMICALLY CONSTRAINED MR
GUIDED OPTICAL IMAGING...............................................................................43
4.1 Introduction..............................................................................................................43
4.2 Determining boundaries and fiber locations with MR images ................................43
4.3 Separating adipose, fibroglandular, and suspect tumor tissue .................................44
4.4 Anatomical Constraints............................................................................................47
4.5 From MR images to computational domains...........................................................50
4.6 Computational burden considerations .....................................................................52
4.7 Implementation of Anatomical Constraints.............................................................53
4.7.1 Hard anatomical constraints ............................................................................53
4.7.2 Soft anatomical constraints: second differential Laplacian operator ..............54
4.7.3 Hybrid Edge Constraining Filter .....................................................................56
4.8 Comparison of spatial reconstruction methods with improper segmentation..........57
4.8.1 Case Study 1: High Density Vascular Structure..............................................58
4.8.2 Case Study 2: Low Density Vascular Structure ..............................................61
4.8.3 Conclusions comparing reconstruction methods.............................................63
4.9 Considerations in 3D imaging .................................................................................64
4.10 Conclusions............................................................................................................68
CHAPTER FIVE: MR GUIDED OPTICAL IMAGING FOR TUMOR
CHARACTERIZATION AND NEOADJUVANT CHEMOTHERAPY
MONITORING.........................................................................................................69
5.1 Detection and characterization of breast tumors......................................................70
5.1.1 Reconstruction methodology...........................................................................70
5.1.2 Results .............................................................................................................71
5.1.2.1 Subject 1 ................................................................................................71
5.1.2.2 Subject 2 ................................................................................................73
5.1.2.3 Subject 3 ................................................................................................75
5.1.2.4 Subject 4 ................................................................................................76
5.1.2.5 Subject 5 ................................................................................................78
5.1.3 Discussion........................................................................................................80
5.2 Monitoring neoadjuvant chemotherapy: A case study ............................................83
5.2.1 Study methodology..........................................................................................84
5.2.2 Results .............................................................................................................86
5.3 Conclusions..............................................................................................................91
CHAPTER SIX: INCORPORATING MR WATER FAT SEPARATION ......................93
6.1 Introduction..............................................................................................................93
6.2 Separating water and fat with MR ...........................................................................95
6.3 Previous work correlating optical and MR water and fat ........................................97
6.4 Methods to Incorporate MR water and fat into image reconstruction...................100
6.4.1 Direct substitution of water and fat ...............................................................101
6.4.2 Joint weighted estimation of water and fat....................................................103
6.5 Comparison of MR water-guided reconstructions.................................................105
6.5.1 Influence of MR Water/Fat Separation constraint on crosstalk ....................107
6.5.2 Influence of MR Water/Fat error on the Joint Weighted Estimation
reconstruction.................................................................................................109
viii
6.6 Experimental validation in a breast tissue simulating phantom ............................111
6.6.1 Properties of the tissue simulating phantom..................................................111
6.6.2 Methods to measure gelatin water concentration ..........................................111
6.6.3 Results ...........................................................................................................113
6.7 In vivo results in the human breast.........................................................................115
6.8 Conclusions............................................................................................................119
CHAPTER SEVEN: MONITORING CHANGES IN BREAST PHYSIOLOGY DUE
TO RESPIRATORY CHALLENGE......................................................................121
7.1 Introduction............................................................................................................121
7.2 Tumor contrast identified by respiratory challenge...............................................121
7.3 Modulating tissue hemodynamics with gas stimulus in healthy tissue .................122
7.4 Methods .................................................................................................................126
7.4.1 Gas Breathing ................................................................................................126
7.4.2 Gas stimulus ..................................................................................................128
7.4.3 Data acquisition .............................................................................................130
7.4.4 Data Processing .............................................................................................131
7.5 Results in the healthy breast ..................................................................................133
7.5.1 Time lag response in healthy breast tissue ....................................................136
7.5.2 Noise Considerations.....................................................................................139
7.6 Conclusions in Healthy Tissue ..............................................................................142
7.7 Modulating tissue hemodynamics with gas stimulus in diseased tissue................142
7.8 Results in breast tumors.........................................................................................143
7.9 Conclusions............................................................................................................145
CHAPTER EIGHT: CORRELATING OXYGENATION MEASURED BY BOLD
AND OPTICS IN THE BREAST...........................................................................147
8.1 Introduction............................................................................................................147
8.2 The BOLD Contrast...............................................................................................147
8.3 The rationale for combining BOLD and Optics ....................................................150
8.4 Comparisons between Optical and BOLD contrast mechanisms ..........................151
8.5 Correlations between Optics and BOLD MR ........................................................152
8.5.1 Correlations performed in healthy tissue.......................................................152
8.5.2 Correlations in tumor tissue...........................................................................153
8.6 Methods for the studies in this Thesis ...................................................................154
8.6.1 Subjects..........................................................................................................154
8.6.2 Respiratory challenge ....................................................................................155
8.6.3 Data Collection..............................................................................................156
8.6.4 Data analysis..................................................................................................159
8.7 Results....................................................................................................................164
8.8 Conclusions............................................................................................................169
CHAPTER NINE: A STRUCTURAL AND FUNCTIONAL MULTIMODAL
RECONSTRUCTION MODEL .............................................................................173
9.1 Introduction............................................................................................................173
9.2 Justification for including MR covariance priors ..................................................173
9.3 Multimodal reconstruction.....................................................................................176
ix
9.4 Simulation test problem .........................................................................................178
9.5 Simulation results ..................................................................................................179
9.6 Conclusions............................................................................................................180
CHAPTER TEN: CONCLUDING REMARKS..............................................................182
10.1 Overview of work completed ..............................................................................182
10.2 Future directions ..................................................................................................185
10.3 Opportunities in breast MR-optical imaging .......................................................186
10.3.1 Volumetric interface....................................................................................186
10.3.2 Dynamic contrast enhanced MR for higher specificity / blood volume
maps ...............................................................................................................187
10.3.2.1 Spatial guidance using washout kinetics ...........................................187
10.3.2.2 Imaging blood volume with DSC-MR and DCE-MR .......................188
10.3.2.3 Imaging blood volume Vascular Space Occupancy (VASO)............189
10.3.3 Incorporating Diffusion Weighted MR into optical scatter.........................190
10.4 Unanswered questions .........................................................................................191
10.4.1 2D vs 3D......................................................................................................192
10.4.2 Soft priors vs Hard priors ............................................................................193
APPENDIX A: 3-DIMENSIONAL IMAGE VISUALIZATION...................................195
APPENDIX B: GENERATING BREAST MESHES WITH MIMICS ..........................198
APPENDIX C: RE-CALIBRATING PMT AMPLITUDE AND PHASE......................209
APPENDIX D: FIBER INTERFACE CAD DRAWINGS .............................................213
APPENDIX E: LIST OF MATLAB SUBROUTINES ...................................................215
x
List of Tables
Table 4.1: The different MRI sequences used in this study were all used in the optical
image reconstruction. A breast clip, identifying the location of biopsy, is shown
as a green arrow in the DCE image (bottom). .......................................................... 47
Table 5.1: Overview of imaging sessions for the subject monitored during
neoadjuvant chemotherapy. ...................................................................................... 85
Table 6.1: Tissue properties used in water/fat simulation study..................................... 106
Table 6.2: Phantom true concentrations in the background and region of interest
(ROI). The concentration of HbT was measured with a hemoglobin analyzer,
and water was measured with methods described below. The scatter amplitude
and scatter power were homogeneous, but unknown (UK). ................................... 111
Table 7.1: Expected changes in total hemoglobin (HbT) and oxygen saturation (O2
Sat) due to physiological changes accompanying a switch between gasses in
each stimulus used in this study. A (+) indicates that the administration of the
gas (shown in the columns) will cause a relative increase in the parameter
(shown on the leftmost column of each row). A (-) indicates a relative decrease. 125
Table 7.2: Listing of the different gases used for this study and the number of
volunteers monitored for each stimulus. ................................................................. 130
Table 7.3: Comparison of the correlation while breathing a gas stimulus compared to
the correlation while breathing air (control). Shown are the significance values
resulting from two sample t-tests, determining if the means were significantly
different................................................................................................................... 141
Table 7.4: Time lag results in these 2 cases show no consistent differences between
tumor tissue and non-diseased fibroglandular tissue for total hemoglobin or
oxygen saturation. ................................................................................................... 144
Table 8.1: List of imaging studies performed with optics and BOLD MR. Imaging
studies 1-3 were volunteers with invasive ductal carcinomas (IDCs) of the left.... 155
Table 8.2: Correlations and significance between optically measured
deoxyhemoglobin and BOLD. After removing data where the optically
measured deoxyhemoglobin had a smaller correlation than the air control (SNR
< 1), the O2/CO2 stimulus induces a response in which optics significantly
correlates to BOLD. ................................................................................................ 167
Table 9.1: Differences in tissue properties from Brooksby et al.89 These results from
11 subjects show significant differences between all parameters but oxygenation.175
xi
List of Figures and Illustrations
Figure 2.1: Two fundamental methods to measure tissue optical properties. Shown are
the effects of an absorbing and scattering medium on an ultrafast laser pulse, and
a light source temporally modulated at a fixed frequency. ......................................... 8
Figure 2.2: MR-guided optical instrument used in this thesis. (a) Frequency
generators for the laser diodes and reference, (b) Serial and dynamic source
controllers, (c) Photomultipler detection hardware, (d) System computer, (e)
Laser diode DC current source, and (f) Rotary stage motor controller. Optical
fibers entered into the MR room through (g) a custom built magnetically
shielded conduit, and (h) were mounted on a fiber interface which was attached
to an MR breast coil. ................................................................................................... 9
Figure 2.3: Labview software control. (a) Inputs allow selection of a combination of
serial single wavelengths and the 3 wavelength dynamic source, (b) Indication of
signals above the noise floor, (c) Output of AC amplitude and phase shift data...... 10
Figure 2.4: Schematic of the serial optical instrument. (a) The serial source operates
one laser diode, (LD) at a time by modulating the laser diode current source,
(DC) .......................................................................................................................... 11
Figure 2.5: Schematic of the dynamic optical instrument. (a) All laser diodes (LD13) are simultaneously driven by appropriate current sources (DC1-3) which are
modulated at separate frequencies by independent frequency generators which
are phase locked together (SG1-3). Similar to the serial setup, the source light is
input into the rotary stage, (b) and injected into the appropriate fiber, (c) which
illuminates the target, (d). The detected light is measured with PMTs attached to
the rotary stage. This signal is mixed with a reference signal generator (SGref)
and............................................................................................................................. 13
Figure 2.6: Translational stage design. (a) Shown in black are the 6 laser diodes. The
red arrow indicates the direction of movement of the sources. In gray are the
source fibers of the 16 bifurcated fiber bundles. (b) Photograph of the source
installed in the system. The arrows indicate the translational laser diode sources
and the fixed source fibers. ....................................................................................... 15
Figure 2.7: (a) Design of the top plate on the detection system. Fiber bundles connect
to the top plate and lead to the patient interface. (b) The bottom plate rotates the
laser diode source and detectors in the direction of movement indicated by the
red arrow. (c) Photograph of the rotary stage installed in the system....................... 15
Figure 2.8: (a) Setup for calibration. A laser diode illuminates a homogeneous
cylindrical phantom so that all PMTs have similar intensities. (b) Filter wheels..... 17
Figure 2.9: (a) Uncalibrated and (b) calibrated voltages for a PMT. Since the voltage
response is linear over all gains within the linear detection region, PMT voltage
xii
is calibrated for gain setting by removing the offset between voltages of identical
input .......................................................................................................................... 18
Figure 2.10: (a) Uncalibrated and (b) calibrated phase response for a PMT. Since the
pathlength of the measurement is independent of input light power, the phase
difference should remain constant. However, changes in PMT gain affect the........ 19
Figure 2.11: Amplitude and phase noise for all PMTs. (a) Plot of the standard
deviation in Voltage as a percentage of voltage vs log10 Voltage. (b) Plot of the
standard deviation in phase (in degrees) vs log10 Voltage. ....................................... 20
Figure 2.12: (a) Average AC voltage amplitude noise response of all PMTs for this
system, in (%) and (b) average phase noise (in degrees), compared to (c,d) a
similar system reported by Yalavarthy47................................................................... 21
Figure 2.13: Amplitude of AC voltage for all PMTs vs input power. At low input
light power, the signal is less than the noise floor, (c). When the input voltage is
too high, the PMTs saturate, (a). Between these limits is the linear detection
region, (b). This region is desired for detector amplitude linearity. ........................ 21
Figure 2.14: (a) Uncalibrated phase differences through the same phantom on
different days, without changing fiber positions. Data collected on day 1 (solid),
and day 2 (dotted). Colors denote different PMTs. (b) Phase response for a
constant pathlength for PMT 8 on day 1 (red) and day 2 (blue)............................... 23
Figure 2.15: (a) Circular and (b) slab patient optical interface attached to MR breast
coils with simulated optical overlays. ....................................................................... 24
Figure 2.16: Data points dropped in calibration phantoms and one subject for slab vs
circle geometries. In these cases, the slab geometry yielded more datapoints that
were of good quality. ................................................................................................ 24
Figure 2.17: (c) Percent errors in contrast recovery between identical inclusions in the
(a, blue) circular, and (b, red) slab geometries of resin phantoms. In the slab
case, contrast recovery in the inclusion was accurate within 1%. ............................ 26
Figure 2.18: Fiber interface integrated into an (a) Invivo breast coil in a (c) Philips
scanner, and a (b) USA Instruments coil in a (d) GE scanner. ................................. 27
Figure 2.19: Slab optical interface in three different MR coils. (a,b,c) Fiber interface
shown for the (a) Invivo coil, (b) USA Instruments coil, and the (c) Philips
Medical Systems, Hamburg, GER., custom optical/MR coil. Note the space
constraints which limit available fiber positions in the commercial coils
including, (d) the sloping top plate of the Invivo coil and the bulky support, and
(e) the lack of ............................................................................................................ 29
xiii
Figure 2.20: (a,b) Sketches (courtesy of C. Luessler, Philips Medical Systems,
Hamburg, GER) and (c,d) photographs (courtesy of S. Davis) of the optical/MR
breast coil. ................................................................................................................. 30
Figure 3.1: Tissue chromophore spectra in the near infrared range (from Eker et al.51). . 31
Figure 3.2: Finite element meshes (a,b) and solutions of the light propagation of a
photon source (c,d) in 2D and 3D. ............................................................................ 34
Figure 3.3: Anatomical information can be easily interpolated onto the finite element
mesh if the modalities are coregistered since there is no positional error. In this
case, the anatomical prior is segmented into three distinct regions, 1-3................... 37
Figure 3.4: (a) Homogeneous initial guess from the optical calibration routine, (b)
initial guess both from optical calibration and an MR quantitative water prior. ...... 38
Figure 4.1: MR images which provide accurate tissue boundaries and fiber positions
via fiducial markers. (a) Fibers placed on the ferrule of each fiber, (b) fibers used
for position reference. ............................................................................................... 44
Figure 4.2: DCE-MR subtraction image resulting from pre contrast image subtracted
from post contrast enhancement image. Note the ring enhancement around the
main lesion, identified by arrows on the right side of the image. The left arrow
identifies a small satellite lesion. .............................................................................. 47
Figure 4.3: Physiological properties imaged on the same day using a a) non MRguided optical imaging instrument, and a b) MR-guided optical imaging, using a
soft-prior Laplacian filter technique. Note the increased contrast recovery with
the image-guided approach. ...................................................................................... 50
Figure 4.4: Transforming MRI images for computational use requires 1) segmentation
of tissue types into adipose, fibroglandular, and suspicious lesions,........................ 51
Figure 4.5: A comparison of the number of unknowns calculated in 2D vs 3D for 2D
full, 3D full, and 3D region-based spectral reconstructions, for five parameters. .... 53
Figure 4.6: Segmented breast MR used to guide reconstruction methods. The labels
within the image define regions of adipose (1), fibroglandular (2), and tumor (3)
tissue. Blue x’s and red circles define the source and detector locations around
the breast. .................................................................................................................. 54
Figure 4.7: (a) Example of a spectral graph (from Biyikoglu et al. 97). In optical
tomography, each row of the covariance weight matrix incorporates the regions
labeled in (b) with connectivity described by this graph. ......................................... 55
Figure 4.8: (a) T1-weighted image of case study 1. (b) Coarse segmentation of (a)
used to reconstruct data. (c) Fine segmentation used to generate data. (b-c) are
color coded according to tissue type. ........................................................................ 58
xiv
Figure 4.9: Reconstructions using the (a) Laplacian matrix reconstruction, (b) hybrid
reconstruction, and (c) region fitting reconstruction. (d) True optical contrasts
and spatial heterogeneity........................................................................................... 60
Figure 4.10: Total errors in absorption (the average of oxyhemoglobin,
deoxyhemoglobin, and water) and scatter (the average of scatter amplitude and
scatter power) for all regions of each of the reconstruction algorithms.................... 61
Figure 4.11: (a) T1-weighted image of case study 2 (b) Coarse segmentation of (a)
used to reconstruct data. (c) Fine segmentation used to generate data. (b,c) are
color coded according to tissue type. ........................................................................ 61
Figure 4.12: Reconstructions using the (a) Laplacian matrix reconstruction, (b) hybrid
reconstruction, and (c) region fitting reconstruction. (d) True optical contrasts
and spatial heterogeneity........................................................................................... 62
Figure 4.13: Total percent errors in absorption and scatter for case study 2 for each of
the reconstruction algorithms.................................................................................... 63
Figure 4.14: Memory requirements when using the Laplacian soft priors
reconstruction can be a computational limitation in 3D. By implementing a
hybrid approach, matrix storage for three patients reduces to a computationally
feasible size. .............................................................................................................. 65
Figure 4.15: 3D mesh used in image reconstruction. The mesh consisted of ~20,000
nodes. Tissue regions are identified by color........................................................... 66
Figure 4.16: 3D reconstructions of (a) hybrid method and (b) hard priors compared to
(c) the truth. The hybrid method reduces the adipose tissue to 1 region, and
applies a Laplacian filter to the fibroglandular tissue and region of interest............ 67
Figure 4.17: Percent error between recovered parameters and the truth for the 3D
hybrid method, and 3D hard priors. .......................................................................... 67
Figure 5.1: (a) Anatomically guided optical images and (b-e) MR images of Subject
1 (no malignant tissue, 2 cysts, 1 benign fibrocystic lesion). Note the slight
decrease in total hemoglobin compared to the background. (b) T1-W image in
the plane of the optical fibers. (c) Gadolinium dynamic contrast enhanced MR
image. (d) T2-W image showing increased water content expected in the cyst /
benign lesion (e) Maximum intensity projection of the DCE-MR image. Note
the tumor identified by the green arrows. ................................................................. 72
Figure 5.2: (a) Anatomically guided optical, (b-d) MR, and (e) pathology images
images of Subject 2. (b) T1-W image in the plane of the optical fibers. (c)
Dynamic contrast enhanced subtraction image used to segment region of interest
(green arrow). (d) Maximum intensity projection gadolinium contrast enhanced
image (lesion identified with arrow). (e) Mass pathology slice showing residual
stromal tissue and no viable tumor hemorrhaging. ................................................... 74
xv
Figure 5.3: (a) Anatomically guided optical, (b-d) MR, and (e) pathology images of
Subject 3, who had a malignant lesion. (b) T1-W image in the plane of the
optical fibers. (c) Dynamic contrast enhanced subtraction image used to
segment region of interest (green arrow). (d) Maximum intensity projection
gadolinium contrast enhanced image. (e) Mass pathology slice showing tumor
size post treatment. Note the haemorrhaging (black in color) corresponding to
total hemoglobin contrast, and the surrounding necrotic tissue (tan in color).......... 76
Figure 5.4: (a) Anatomically guided optical and (b-d) MR images of Subject 4, with a
known malignant lesion. (b) T1-W image in the plane of the optical fibers. (c)
Gadolinium dynamic contrast enhanced MR image. (d) Maximum intensity
projection of the DCE-MR image............................................................................. 78
Figure 5.5: (a) Anatomically guided optical and (b-d) MR images of Subject 5. (b)
T1-W image in the plane of the optical fibers. (c) Gadolinium dynamic contrast
enhanced MR image. (d) Maximum intensity projection of the DCE-MR image.
Note the tumor identified by the green arrows. ........................................................ 80
Figure 5.6: Comparison of tumor to fibroglandular total hemoglobin across all
subjects. The subjects denoted in the non-shaded region, subjects 3, 4 and 5, had
known malignant lesions. In contrast, the shaded region consisted of subject 1,
who had a benign/normal lesion, and subject 2, who was fully responding to
chemotherapy. Total hemoglobin is higher than the background fibroglandular
tissue in the known malignant tumors. ..................................................................... 81
Figure 5.7: Tumor to background contrast ratios of total hemoglobin for all subjects.
Negative contrast indicates that the background had higher total hemoglobin
than the region of interest. ........................................................................................ 81
Figure 5.8: No consistent trends between known malignant and suspect nonmalignant lesions are apparent for (a) Oxygen saturation contrast, (b) Water
contrast, (c) Scatter Amplitude contrast, and (d) Scatter Power contrast for all
subjects...................................................................................................................... 83
Figure 5.9: a) DCE MR images of a subject with an IDC taken 1 day prior to
chemotherapy shows slight enhancement of 1 main node with 3 satellite lesions.
b) MR-NIR images overlaid on a). The lesions in the plane of the optical fibers
of the MR-NIR instrument show increased hemoglobin over the background. c)
The colorbar used for quantitative analysis of hemoglobin in b). ............................ 87
Figure 5.10: a) DCE MR images of the subject from taken within 48 hours of the 2nd
cycle of chemotherapy. Two lesions enhance, although the main lesion shows
less enhancement, indicating response to chemotherapy. Note the decrease in
total hemoglobin between b) and the previous figure, demonstrating response.
Pathology (not shown) taken after the completion of chemotherapy showed a
complete response. c) The colorbar has been duplicated here for comparison....... 88
xvi
Figure 5.11: a) DCE MR images of subject 5 within 48 hours of the 3rd cycle of
chemotherapy. By this imaging session, the main lesion no longer enhanced, as
confirmed by the reading radiology (R. D-A.). The satellite lesion exhibited very
slight enhancement. These factors indicate a strong response to chemotherapy.
(b) Total hemoglobin in the lesion was within 0.001 mM of the background.
Pathology (not shown) studied after the completion of chemotherapy showed a
complete response. c) The colorbar has been duplicated here for comparison....... 89
Figure 5.12: Quantitative Comparison of (a) total hemoglobin, (b) oxygen saturation,
and (c) water content in an invasive ductal carcinoma over 3 cycles of
chemotherapy in a complete responder..................................................................... 90
Figure 6.1: Spectral response of the R6357 photomultiplier tubes used in this study
(courtesy of Hamamatsu Photonics). Note the cutoff in sensitivity at
wavelengths longer than 800nm. .............................................................................. 93
Figure 6.2: (a) Tissue absorption spectra for tissue optical properties of 20µM HbO,
20µM Hb, and 60% water. (b) Tissue absorption spectra approximately in the
sensitivity region of the PMTs. Note the spectral similarity between
oxyhemoglobin (HbO) and water. ............................................................................ 94
Figure 6.3: Comparison of the spectral dependency of MR and NIR optics on water
and fat. Because the signal contributions from water and fat can be isolated,
percent water and fat calculated by MR will in principle be the same percentages
determined by optics (Optical spectrum obtained from van Veen et al.139) ............. 98
Figure 6.4: The initial guess determined by (a) optics, and (b) optics including the
MR water image...................................................................................................... 101
Figure 6.5: Test problem used in this simulation study. Total hemoglobin in the
tumor was set at 0.04 mM, a 2:1 contrast over the background fibroglandular
tissue. Oxygen saturation was 50% in the tumor, and 70% in the background.
Data with 5% white noise in AC amplitude and 5 degrees white noise in phase
was generated from this geometry. ......................................................................... 106
Figure 6.6: Error in HbO decreases with additional wavelengths because of the
improved spectral sampling, which in turn leads to more accurate separation
between water and oxyhemoglobin. Comparatively, the direct substitution
method gives superior quantification, even with 3 wavelengths. ........................... 108
Figure 6.7: Error in HbO with 3 wavelengths increases as MR water quantification
error increases. The comparative case of excluding MR water priors is shown at
the far right.............................................................................................................. 109
Figure 6.8: Error in HbO when MR quantification is incorrect by 10%. The percent
error is the average error of 5 ensembles of 3 wavelengths in the wavelength
range used by the system in this thesis. .................................................................. 109
xvii
Figure 6.9: Comparison of recovered errors in water quantification between the direct
substitution approach vs. the joint weighted estimation approach. By
extrapolation, these errors will be equivalent at ~1% estimation error. ................. 110
Figure 6.10: Methods used to compute percent water in gelatin consisted of (a) NIR
spectrophotometry, and (b) DIXON MR. In both cases, pure water was used as a
reference to determine the water content of the gelatin. ......................................... 112
Figure 6.11: Comparison of reconstructions of 3 wavelengths of 661, 785, and 826nm
with and without water priors. (a) Target true values, (b) spatially guided
reconstruction, and (c) spatially and quantitatively guided reconstruction using
the direct substitution reconstruction. ..................................................................... 114
Figure 6.12: Comparison of reconstructions of 6 wavelengths of 661, 761, 785, 808,
826, and 849nm with and without water priors. (a) Target true values, (b)
spatially guided reconstruction, and (c) spatially and quantitatively guided
reconstruction using the direct substitution reconstruction. ................................... 115
Figure 6.13: Absolute percent errors in total hemoglobin (HbT) for the spatially
guided vs direct substitution reconstructions, for different sets of wavelengths. ... 115
Figure 6.14: (a) T1-W Gadolinium MR image of the affected breast (b) T2 weighted
image in the coronal plane of the optical fibers. Tumors are identified with the
red arrows................................................................................................................ 116
Figure 6.15: Images of water (a) and lipid (b) IDEAL MR images. Quantitative (c)
water and (d) lipid images overlaid onto the 2D FEM mesh. ................................. 117
Figure 6.16: (a) In vivo image reconstructions of a diseased breast without MR
spectral priors compared to (b,c) methods that use MR water/fat priors. (b)
Image reconstruction using the direct substitution gives the highest tumor to
background contrast. (c) Image reconstruction using the joint weighted
estimation approach yields higher contrast than ignoring water quantitative
priors, but less contrast than the direct substitution method. ................................. 118
Figure 7.1: (a) Photograph of the gas breathing circuit. (b) Diagram of circuit
operation during oxygen or carbogen breathing. During oxygen or carbogen
stimulus, pressure from gas input 1 would close valve 2, preventing room air
from entering the circuit. All valves were one-way, so that the expired gas
would not be re-breathed. (c) Diagram of circuit operation during air breathing.
During air stimulus, the lack of pressure from the gas input 1 would open valve
2, allowing room air to be drawn through the circuit. A small tube led from near
the mouthpiece to an oxycapnometer to monitor expired gas concentrations. ....... 127
Figure 7.2: Inspired (a) Carbogen and oxygen gases were controlled with a (b) custom
computer-controlled valve. This valve was synchronized via software to the ....... 128
xviii
Figure 7.3: Gas time series for the stimuli combinations in Table 7.2. (a) Timing
diagram indicating duration of gas stimulus. (b) The true timing of each gas,
shown in blue, was approximated by a sine wave, shown in red, for data
processing. The shading indicates which gas is active. (c) Changes in CO2
concentration in a compliant subject. Note the three periods of increased CO2
corresponding to the three periods of the stimulus used in the data processing. .... 129
Figure 7.4: Instrumentation fluctuations in a tissue-simulating phantom. Standard
deviation in fitted total hemoglobin is 0.19% of the amplitude, and standard
deviation in fitted oxygen saturation is 0.22 % of the amplitude. .......................... 131
Figure 7.5: Simulated cross covariance calculations for two signals, signal S1 (blue)
and signal S2 (red), having different amounts of Gaussian noise. (a) No noise (b)
25% of S2 signal amplitude noise (c) 100% of S2 signal amplitude noise. These
examples show the effects of noise on correlation at zero time lag........................ 133
Figure 7.6: Temporal and frequency response of hemodynamics to O2/CO2 gas
stimulus compared to an air control. In (a,c), white bars indicate O2 stimulus,
and gray bars indicate carbogen. For (b,d), both white bars and gray bars indicate
air. (a) Total hemoglobin oscillations during O2/CO2 stimulus show a
significantly larger peak at 0.041Hz than the air control, (b) indicating the tissue
response to the stimulus was larger than the physiological noise. (c) Oscillations
of oxygen saturation during gas stimulus also shows a larger frequency peak at
0.041Hz than the air control, (d), indicating a larger response than the
physiological noise.................................................................................................. 135
Figure 7.7: Phase lags between the start of the gas stimulus and the total hemoglobin
(HbT) and oxygen saturation (O2 Sat) response at maximum correlation for (a)
O2/CO2 (N=8), (b) Air/CO2 (N=4), and (c) Air/O2 (N=3). Note that although the
time lag for the response is volunteer dependent, the O2/CO2 stimulus generally
has a π to 2π phase delay, meaning that the total hemoglobin increases during
carbogen .................................................................................................................. 137
Figure 7.8: Time lag comparison of oxygen saturation vs total hemoglobin for the
three gas stimuli. In stimuli with carbogen, vasodilation allows highly
oxygenated blood to enter the breast tissue, which washes out deoxygenated
hemoglobin, and increases oxygen saturation. Oxygen saturation and total
hemoglobin during Air/O2 stimulus is not dominated by changes in vascular
tone. Instead, these changes could also be due to pO2 induced oxygenation
changes.................................................................................................................... 139
Figure 7.9: Signal to noise ratio for hemodynamic measures for each stimulus. (*)
denotes significance shows that O2/CO2 induces the strongest response compared
to the air control. P-values are given in the table below. ....................................... 141
Figure 7.10: Initial results indicate that the signal to noise for total hemoglobin (HbT)
in tumor tissue is significantly lower than the background fibroglandular tissue.
xix
This separation is not demonstrated with oxygen saturation (Sat) for the 2
patients. Even with this small sampling, HbT has significantly lower SNR than
the............................................................................................................................ 145
Figure 8.1: Example SSFSE image used to measure the BOLD signal. This coronal
slice was taken in the plane of the optical fibers. The low intensity shading in
the lower left of the image is phase wrap from the contralateral breast. Note the
bright motion artefact near the skin at the top. ....................................................... 157
Figure 8.2: (a) The optical imaging interface on the lateral side of the right breast.
Optical fibers could be moved anterior/posterior along custom built rails and
locked into position with plastic thumb screws. This interface was bolted into
the manufacturer’s breast immobilization plates. (b) Subject entering the magnet
bore. Shown with arrows are the pulse oximeter and respiratory belt................... 159
Figure 8.3: (a) BOLD signal time course for O2/CO2 stimulus. Red (O2) and green
(CO2) bars indicate the inspired gas. (b) BOLD correlation image at a certain
time lag. This image is thresholded at a p=0.05 significance level. The yellow
box indicates the ROI. This was selected to minimize motion noise near the
boundary. (Edited from communication courtesy of Rakow-Penner, 229). ............. 160
Figure 8.4: MR images used for data analysis. (a) BOLD SSFSE image, (b) Water
image used to segment optical regions. .................................................................. 161
Figure 8.5: Hard prior difference reconstructions using region information for 2
consecutive timepoints. (a). HbO, Hb, for timepoint 1 (b,c), and timepoint 2
(d,e). ........................................................................................................................ 162
Figure 8.6: Temporal and frequency response of hemodynamics to O2/CO2 gas
stimulus. White bars indicate O2 stimulus, gray bars indicate carbogen stimulus. 162
Figure 8.7: Phase lag between the gas stimulus and the measured BOLD and optical
deoxyhemoglobin response for (a) O2/CO2, (b) Air/CO2, and (c) Air/O2. The
results for both modalities show little consistency over time for the different
subjects.................................................................................................................... 165
Figure 8.8: Comparison of BOLD signal phase lag vs deoxyhemoglobin measured
optically for all patients for respiratory stimuli of (a) O2/CO2, (b) Air/CO2, and
(c) Air/O2, plotted with the line of equality. Axes are in units of radians. ............ 166
Figure 8.9: Optically measured deoxyhemoglobin correlation to an all air stimulus
(control), and the O2/CO2 gas stimulus. Although most subjects exhibited a
stronger correlation to the gas stimulus than to the control, some subjects did not
respond to the gas stimulus. .................................................................................... 168
Figure 8.10: Correlation between BOLD and optically measured deoxyhemoglobin
during O2/Carborgen gas stimulus. This plot shows that BOLD and optics
xx
correlate significantly r = 0.76, p = 0.0477 only when appropriate consideration
is given to SNR. ...................................................................................................... 169
Figure 8.11: Comparison of regions of interest for a healthy subject. (a) Segmented
fibroglandular tissue used for optical image guided reconstruction, (b) BOLD
stimulus correlation image, (c) segmented fibroglandular region, (d) segmented
BOLD region used for cross correlation. ................................................................ 171
Figure 9.1: Physiological variations in total hemoglobin, oxygen saturation, water
content, and scatter, between adipose and fibroglandular tissue in 3 healthy
subjects. This data shows differentiation between adipose and fibroglandular
tissue in total hemoglobin and water, and less so in scatter. No substantial
difference is seen in tissue oxygenation.................................................................. 174
Figure 9.2: MR images can be incorporated into the image reconstruction either (a)
structurally, or (b) functionally. Here, 0 or 1 indicates spatial regions. The 40-60
for the water color bar indicates percent water. ...................................................... 177
Figure 9.3: Covariance maps for the test problem. (a) For the structural covariance
reconstruction, a T1-weighted image was used for all covariance maps. (b) For
the physiological covariance reconstruction, a homogeneous Hb map was used.
Total hemoglobin, water, and scatter used identical covariance maps. In this
case, the water image was used only as a structural covariance map, and not as a
quantitative map as implemented in Chapter 6....................................................... 178
Figure 9.4: A simulation test problem demonstrated the bias in Hb introduced when
improper covariance maps were used. (a) The target true values. (b) The
structural covariance reconstruction, using covariance maps in Figure 9.3a. (c)
Physiological covariance reconstruction using covariance maps in Figure 9.3b.
Although the bias .................................................................................................... 180
Figure 10.1: Images from dynamic contrast enhanced MR. (a) Pre-contrast image
subtracted from the 1st dynamic post-contrast image shows clear regions of
enhancement. (b) CADstream (Confirma) image analysis provides spatial maps
that identify possible disease status based on the shape of contrast washout
curves. Regions labelled as green are indicative of benign lesions. Blue signifies
an intermediate between benign and malignant characteristics, and red identifies
kinetics that are suspect malignancy....................................................................... 188
Figure 10.2: Images of a subject with an invasive ductal carcinoma of the left breast.
The tumor location is given by the arrows. These results show a case where (a)
optically determined particle number density demonstrated spatial similarities to
(b) apparent diffusion coefficient maps derived from DWI MR imaging
(SNAILS sequence, courtesy of Liu et al.241). ........................................................ 191
Figure A.1: 3D visualization example. (a,b) MR images used to segment tissue type
and identify regions of interest. (c) Single slice of a 3D reconstruction in the
plane of the regions of interest. (d) Visualization sets the transparency at 100%
xxi
at Jacobian values below a set sensitivity threshold. In this case, the threshold
was set at the Jacobian value 1cm above the center of the imaging plane. (e) An
example where the transparency is set at 0% at the fibers, and 100% at
sensitivity values which are lower than the value 1cm above the center of the
image volume. The transparency in these cases is based on the log transform of
the Jacobian............................................................................................................. 196
Figure B.1: Image geometry can be imported either by selecting the desired images,
or selecting the parent directory. If the directory is chosen, images will be
grouped into series, based on the DICOM header. ................................................. 198
Figure B.2: Geometry reference markers are imported from the MR DICOM headers,
which are based on the MR coil. Often, geometry references are not included in
the DICOM header, so these must be manually specified. ..................................... 199
Figure B.3: Grayscale thresholding is the quickest method to segment anatomical
regions, and should be used as a first-step. ............................................................. 200
Figure B.4: Masks should be cropped to avoid meshing the abrupt interface between
the breast and the chest wall. This boundary can create sharp edges that are
difficult to mesh. Additionally, MR images acquired with a breast coil are less
sensitive to regions beyond the chest wall, because the signal is received from
near the breast. These regions have poor signal to noise, and intensity
thresholding is less accurate. Cropping the mask also helps to remove the fiber
fiducials from the image mask. ............................................................................... 200
Figure B.5: Regions of interest segmented from other image stacks, such as dynamic
contrast enhanced MR, can be exported as stl files, and imported into the main
project. .................................................................................................................... 201
Figure B.6: Fiber positions can be placed using the Medcad menu. These points can
be viewed in the 3 planes, and in 3D. Distances from the tissue to reference
fiducial markers may be determined using the ‘measure distance’ tool. ................ 202
Figure B.7: Bitmap images are used to generate meshes in 2D. Mask shades are used
by NIRFAST meshing software to define region boundaries................................. 203
Figure B.8: Elements material properties are assigned based on the masks. The
desired masks can be chosen through the ‘select masks’ button. ........................... 207
Figure C.1:(a) Setup for calibration. A laser diode illuminates a homogeneous
cylindrical phantom so that all PMTs have similar intensities. (b) Filter wheels
attenuate input light through the full dynamic range of the PMTs. A circular
fiber interface fixes fiber locations during all measurements. ................................ 210
Figure C.2: The calibration program can be used to create the original calibration
files, or to adjust the pre-existing calibration files. The existing calibration
filename................................................................................................................... 211
xxii
Figure D.1: Slab system ProE CAD drawings. Dimensions are shown in inches. ......... 213
Figure D.2: Calibration fiber interface used to ensure all fibers are rigidly fixed at an
equal distance from the isocenter of the interface. Measurement units are in
inches. ..................................................................................................................... 214
xxiii
List of Symbols, Abbreviations and Nomenclature
Symbol
NIR
PMT
MR
NMR
DCE-MR
BOLD
TR
TE
PDE
J
FEM
HbT
Sat or O2 Sat
Sc-A
Sc-P
ROI
FG
IDC
DCIS
O2
CO2
SNR
GB
Definition
Near Infrared
Photomultiplier Tube
Magnetic Resonance
Nuclear Magnetic Resonance
Dynamic Contrast Enhanced MR
Blood Oxygen Level Dependent MR
Repetition Time
Echo Time
Partial Differential Equation
Jacobian
Finite Element Method
Total Hemoglobin
Oxygen Saturation
Scatter Amplitude
Scatter Power
Region of Interest
Fibroglandular
Invasive (or Infiltrating) Ductal Carcinoma
Ductal Carcinoma in Situ
Oxygen or Oxygen gas
Carbon Dioxide or Carbogen gas
Signal to Noise Ratio
Gigabyte
xxiv
Chapter One: Introduction
1.1 Overview
This thesis describes efforts to improve magnetic resonance (MR) guided optical imaging
for breast cancer detection. The focus was to utilize tissue information available from
MR to improve upon the limitations of optical imaging, and conversely, to use optical
imaging to improve upon the limitations of MRI. This thesis investigated ways to
optimize data quality and increase mutual information provided by both the MRI and the
optical imaging system, with the goal of improving clinical breast cancer imaging.
1.2 Current state of breast cancer imaging
Breast cancer is currently the second leading cause of cancer deaths in women, with 1.3
million new cases being diagnosed each year1. It is well known that breast cancer
survival rates increase dramatically with early diagnosis, with a patient’s survival being
strongly linked to diagnosis prior to cancer metastasis2. To this end, the standard
screening regimen consists of annual mammograms for women over the age of 40, and
the adoption of magnetic resonance imaging for screening high risk women1. Clearly,
improving the rate of early breast cancer detection is a major focus in healthcare.
However, it can be argued that the technological gains resulting in earlier detection must
not come at the expense of higher rates of false positive diagnoses, which strain the
healthcare system and stress those women who are falsely diagnosed3, 4. There is a need
to develop tools which identify disease at an early stage with high specificity.
The current standard of care in breast cancer screening is x-ray mammography.
However, mammography is limited by the lack of contrast between diseased and normal
1
tissue, and the heterogeneity in tumor tissue. X-ray imaging detects structural changes in
tumors by identifying regions of tissue that have high vascularity or architectural changes
in the breast parenchyma. However, the attenuation contrast in the x-ray energy
spectrum between healthy fibroglandular and tumor tissue is fairly subtle. In addition,
tissue types overlap in the projection images, masking heterogeneity. For these reasons,
mammography will always have fundamental diagnostic limitations that will lead to
significant rates of false negatives5. Secondary methods such as ultrasound are primarily
focused on differentiation of cysts from solid tumors. Although the combination of
mammography and ultrasound further improves sensitivity, it is inferior to Magnetic
Resonance Imaging (MRI) 6, especially in younger subjects with dense breasts and in
high-risk women7.
1.3 Imaging breast cancer with Magnetic Resonance
Routine MRI breast exams involve contrast injection to increase sensitivity and
specificity8. This technique is called Dynamic Contrast Enhanced MRI (DCE–MRI),
where a paramagnetic contrast agent Gadolinium (Gd) is injected into the vasculature and
imaged over time. DCE-MRI is sensitive to regions of increased microvessel density9,
caused by unregulated angiogenesis, a hallmark of invasive cancer8, 10, increased vascular
permeability, and increased interstitial space11. Gd collects in tumors because of the
tortuous and leaky vasculature, and provides contrast by shortening the T1 relaxation of
water12. These methods have been shown in multi-center clinical trials to be extremely
effective in the detection of abnormalities, approaching 100%12. However, the specificity
of MR mammography may be as low as 67%, even with expert analysis13, 14, and benign
lesions that are misclassified during image analysis require invasive biopsy15. The
2
effectiveness in detection coupled with the limitation in accurate malignancy
characterization has encouraged the study of several new imaging techniques to aid
standard MR breast mammography, by both MRI16, 17 and additional modalities attached
to MRI18-20.
1.4 Imaging breast cancer with optics
Optical imaging samples the spectral properties of tissue in the near infrared regime to
provide images of tissue hemoglobin, water, lipid, and microstructure. In optical imaging
of the breast (optical mammography), tissue hemoglobin content has been shown to be
the most effective in differentiating malignant from healthy tissue21, 22, although breast
cancers have been shown in select studies to have lower oxygenation and higher water
content than normal tissue, and lower lipid content23-27. Because it uses non-ionizing
near-infrared light, this technique can be used multiple times to monitor tissue health, and
it can be low-cost.
This information may help improve the delineation of malignant tissue from
healthy tissue because it provides physiological information that identifies characteristics
unique to tumor function. Blood flow and tissue oxygenation are interdependent; it is
well known that because of the growth in metabolic demands of malignant tumors, blood
supply becomes unable to meet oxygenation and nutrient demands11. This insufficiency
leads to the overexpression of several genetic factors which result in the formation of
immature, inadequate vasculature. Of particular importance are vascular endothelial
growth factor (VEGF), which leads to accelerated growth28 of neovasculature and an
increase in blood flow, and vascular permeability factor (VPF), which decreases the
effectiveness of tumor vasculature to adequately perfuse the tissue29. Thus, knowledge
3
of tissue vascular content and oxygenation, provided by optics, may identify important
signatures of malignancy. This information is not only important for the detection of
tumors, but also for the prediction of therapy treatment, because it may indicate the
effectiveness of chemotherapy drugs30, and response to radiation10 and photodynamic
therapy31.
Optical imaging has achieved varying degrees of success, depending on the study
protocol, and has been shown in several clinical trials to improve specificity due to added
lesion characterization21, 22. However, the accuracy of optical mammography with small
lesions below the resolution limit of about 5mm is limited22, 32. The lack of high-spatial
resolution will likely limit the utility of stand-alone optical breast cancer imaging.
1.5 Improving optical breast imaging with MRI
The ideal breast imaging modality would be one that combined high detection rates
(sensitivity) with a high degree of accuracy in lesion characterization (specificity). To
this end, optical mammography, guided by other imaging approaches, has been
developed to integrate the higher resolution of a complimentary modality into optical
spectroscopy19, 33. It has been shown in phantom studies that the inclusion of high
resolution spatial guidance from x-ray or MR can improve the quantification of optical
parameters34-37. However, MRI is an extremely versatile modality which can image more
tissue properties than simply tissue structure. Methods to combine optical imaging with
different MRI contrasts for breast cancer imaging are the major focus of this dissertation.
4
1.6 Organization of this Thesis
The primary instrumentation used in this thesis was developed by Brooksby et al.19. A
brief overview of system function is given in Chapter 2. This chapter presents
improvements to this system through system noise characterization and patient interface
design advances. In addition to the primary “serial wavelength” imaging system, a
“dynamic wavelength” technique is described.
Chapter 3 presents the algorithms used for image reconstruction. In particular,
the diffusion model for light propagation is outlined, and the formulation of the nonlinear reconstruction for the recovery of tissue physiological properties is presented. The
reconstruction model will be developed more fully in later chapters to incorporate the
different images provided by the MR.
Incorporation of structural information provided by MR may be used in several
ways: (1) to provide an accurate map of the tissue boundary, (2) to provide locations of
optical fibers, and (3) to spatially influence the update in the optical reconstruction. The
incorporation of spatial maps will be discussed in detail in Chapter 4.
Chapter 5 presents case studies in characterizing lesions with MR-guided optics.
These cases include malignant lesions, a lesions which completely responded to
chemotherapy, and a benign lesion. A case study investigation of the use of MR-guided
optics to image the response to neoadjuvant chemotherapy is presented.
Because of technological limitations on wavelength sampling and detector
performance, accurate image reconstructions of water have not been possible with this
system to date. Inaccuracies due to the similar spectral features of oxyhemoglobin and
5
water lead to errors in tissue recovery. The use of MR water/fat separation to reduce this
source of error in optical imaging is presented in Chapter 6.
Chapter 7 demonstrates how MR-guided optics may be used to measure
respiratory physiology, and presents case studies of imaging tumor vascular tissue.
Chapter 8 investigates the correlation of deoxyhemoglobin measurements made by MR,
with those of optics. The benefits of this combined imaging modality are described along
with an indication of how this tool may provide a new method to determine lesion
malignancy.
Chapter 9 presents a comprehensive reconstruction model which incorporates the
various functional MR priors discussed in this thesis. Advantages of this model over a
purely spatially-guided approach are discussed.
This thesis concludes in Chapter 10 with suggestions for future research. The
appendix presents methods and additional information on optimizing MR-guided optics.
First, techniques for appropriate 3D visualization of optical images are shown which
provide a means to deemphasize unknowns that are poorly sampled by the optical fibers.
Next, a tutorial for creating 2D and 3D computational meshes from subjects is presented.
The appendix then describes tools for calibrating the photomultiplier tubes. The
appendix also includes computer-aided drawings of the optical interface. Finally, the
MATLAB algorithms used in this thesis are listed at the end of the appendix.
6
Chapter Two: Instrumentation for MR guided diffuse optical
spectroscopic imaging
2.1 Introduction
Light transmitted through tissue is predominantly attenuated by the electronic absorption
of hemoglobin, water, and lipids. The quantities of these absorbers can be determined by
measuring the amount of signal attenuation of various wavelengths in the near infrared
range. However, because of light scatter, determining the amount of light loss due solely
to absorption is more difficult.
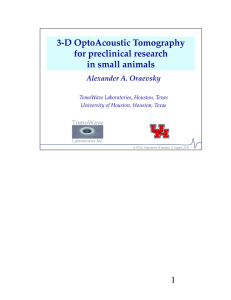
Absorption can be separated from scatter either by time domain38, 39 or frequency
domain39, 40 detection techniques. Time domain methods determine scatter by measuring
the temporal spread of a pulse of light incident upon the tissue. The increase in pulse
width is due to the delay of photons arriving at the detector resulting from optical scatter.
Frequency domain methods measure the phase shift of intensity modulated light exiting
the tissue. This shift is caused by tissue scatter induced changes in the arrival time of the
light, which is dependent on the modulation frequency41. While time domain optical
imaging has inherently more information content, frequency domain techniques are
popular because of the robustness of lock-in detection. Figure 2.1 illustrates the
principles of time domain and frequency domain measurements42.
The frequency-domain instrumentation used in this thesis is nearly identical to the
instruments developed by McBride, Pogue, & Jiang43, and Brooksby et al.19 who
modified the design to remove all ferromagnetic metal from the patient interface. The
key feature of the design is the heterodyne detection technique, which separates
7
amplitude and phase to decouple tissue absorption and scatter. Efforts to improve data
collection through system detector characterization, patient interface modifications, and
increased temporal resolution are discussed below.
Time Domain
time
time
Frequency Domain
time
time
Figure 2.1: Two fundamental methods to measure tissue optical properties. Shown
are the effects of an absorbing and scattering medium on an ultrafast laser pulse,
and a light source temporally modulated at a fixed frequency.
2.2 System Operation
The frequency domain optical imaging system is shown in Figure 2.2. This system
sequentially illuminates one optical fiber, and simultaneously detects the emitted light
with the other 15 fibers. Thirteen-meter long optical fiber bundles (composed of 248
200µm diameter fibers) enter the MR room through a shielded conduit, and attach to a
8
fiber interface which is integrated into an MR breast coil. The interface positions the
fibers to contact the breast. A Labview (© National Instruments) control program, shown
in Figure 2.3, allows automated data collection, which enables either a serial imaging
system or a dynamic imaging system to be used. By connecting the system to an MRI
trigger signal, data collection can be gated simultaneously to the MRI acquisitions.
g
a
b
h
c
d
e
f
Figure 2.2: MR-guided optical instrument used in this thesis. (a) Frequency
generators for the laser diodes and reference, (b) Serial and dynamic source
controllers, (c) Photomultipler detection hardware, (d) System computer, (e) Laser
diode DC current source, and (f) Rotary stage motor controller. Optical fibers
entered into the MR room through (g) a custom built magnetically shielded conduit,
and (h) were mounted on a fiber interface which was attached to an MR breast coil.
9
a
b
c
Figure 2.3: Labview software control. (a) Inputs allow selection of a combination of
serial single wavelengths and the 3 wavelength dynamic source, (b) Indication of
signals above the noise floor, (c) Output of AC amplitude and phase shift data.
2.3 Serial spectroscopic imaging
The serial source scheme implemented in this system is shown in Figure 2.4. In this
implementation a single 100.0005 MHz intensity modulated light source is sequentially
scanned around the breast. The light exiting the tissue is detected with 15
photomultiplier (PMT) photodetectors (Hamamatsu R6357) in parallel. This signal is
mixed with a 100 MHz reference to provide an amplitude and a phase signal. This mixed
signal is compared with the amplitude and phase of a reference mixed signal, which is
composed of 1% of the AC source of the laser and 1% of the AC signal from the
reference, to obtain an attenuation of AC amplitude and a shift in phase.
To optimize the signal to noise ratio of the PMTs, voltage gains were determined
before imaging. In the serial source scheme used for much of the data in this thesis,
10
detector gains were optimized for each wavelength, and cycled through each source
position around the breast. Each wavelength required approximately 2 minutes to find
the ideal gains, depending on tissue optical properties, and 30 seconds for data collection.
Thus, a full dataset for all six wavelengths totalled 12 minutes for gain collection and 3
minutes for data collection.
c
d
b
a
Figure 2.4: Schematic of the serial optical instrument. (a) The serial source operates
one laser diode, (LD) at a time by modulating the laser diode current source, (DC)
with a signal generator, (SG). The source light is input into a rotary stage (b) and
injected into the appropriate fiber, (c) which illuminates the target, (d). The
detected light is measured with PMTs attached to the rotary stage. This signal is
mixed with a reference signal generator (SGref) and converted to a digital signal in
the computer. (Computer icon courtesy of Microsoft Corp).
11
2.4 Dynamic spectroscopic imaging
In order to improve temporal resolution, requisite for the work in Chapters 7 & 8, a
dynamic source was installed which could simultaneously acquire 3-wavelengths. This
system is shown in Figure 2.5, and is described in more detail in Jiang et al.44. The
detection method is identical to the serial system, as it uses the same hardware. However,
this scheme combines 3 wavelengths at 3 different frequencies (100.0006, 100.0009, and
100.0011 MHz) into the source. These frequencies are simultaneously demodulated to
separate each of the wavelengths. By simultaneously imaging with 3 wavelengths, this
implementation improves system speed by a factor of 6, as the gain is optimized only for
1 wavelength. The temporal resolution using this source scheme is 30 sec.
In principle, this scheme could be used to simultaneously image any number of
wavelengths, as long as modulation frequencies are chosen such that the harmonics of
their beat frequencies do not overlap. However, two factors limit the number of
simultaneous wavelengths. First, the nonlinear sensitivity of the photocathode in the
PMTs causes a wavelength dependent variation in signal to noise. Therefore, a gain
setting which may be optimal for one wavelength may be a poor setting for another.
Second, although these multiple wavelengths may have different AC frequencies, their
DC magnitudes all contribute to the total signal in the photodetectors. Eventually, these
signals will saturate the detectors
12
c
d
b
a
Figure 2.5: Schematic of the dynamic optical instrument. (a) All laser diodes (LD13) are simultaneously driven by appropriate current sources (DC1-3) which are
modulated at separate frequencies by independent frequency generators which are
phase locked together (SG1-3). Similar to the serial setup, the source light is input
into the rotary stage, (b) and injected into the appropriate fiber, (c) which
illuminates the target, (d). The detected light is measured with PMTs attached to the
rotary stage. This signal is mixed with a reference signal generator (SGref) and
converted to a digital signal in the computer. (Computer icon courtesy of Microsoft
Corp).
13
2.5 Light illumination
Multiple wavelengths of light in the near infrared are needed to perform spectroscopic
imaging in breast tissue. The light sources must be well characterized, stable, and of
sufficient power to detect signals through ~10cm of tissue. Laser diodes are used in this
instrument because they are very stable and operate at many different wavelengths
throughout the near-infrared spectrum with high output power above 100mW. This
system used laser diode wavelengths of 661nm, 761nm, 785nm, 808nm, 826nm, and
849nm. These light sources were originally coupled to optical fiber bundles through a
translational stage19, shown in Figure 2.6, and later were modified to couple through a
rotational stage43, shown in Figure 2.7.
These designs enable the light source to sequentially illuminate the different fiber
bundles located around the breast. The fiber bundles used in this system are bifurcated;
in the original translational design, 7 fibers in the center were coupled to the sources, and
the remaining fibers directly abutted the photomultiplier detectors. This design isolated
the detection channels from any moving parts45. However, medical laser exposure
standards limit laser power to ~7mW with this configuration. Thus, one factor in
changing the design back to the rotary stage used in previous work43 was that 241 fibers
(total fibers minus 7 unused fibers) in the bundle could be used to illuminate the breast,
with a maximum allowable power of 243mW46. In practice, laser powers incident upon
breast tissue were usually between 30 and 60mW. The other major factor in changing
source geometry was the difficulty in focusing the laser diodes into the small (~600µm)
bifurcated arm of each fiber bundle. With the rotary stage, the source laser could more
easily be focused into the ~4mm fiber bundle.
14
b
a
Figure 2.6: Translational stage design. (a) Shown in black are the 6 laser diodes.
The red arrow indicates the direction of movement of the sources. In gray are the
source fibers of the 16 bifurcated fiber bundles. (b) Photograph of the source
installed in the system. The arrows indicate the translational laser diode sources
and the fixed source fibers.
a
b
c
Figure 2.7: (a) Design of the top plate on the detection system. Fiber bundles
connect to the top plate and lead to the patient interface. (b) The bottom plate
15
rotates the laser diode source and detectors in the direction of movement indicated
by the red arrow. (c) Photograph of the rotary stage installed in the system.
2.6 Light detection
Near infrared light transmitted through breast tissue can be attenuated by 7 orders of
magnitude or more. Thus, not only must photodetectors have the ability to detect low
light levels, but they must also have a large dynamic range. The Hamamatsu R6357
photomultiplier tubes were chosen for these reasons. Photomultiplier tubes allow
tuneable gain by adjusting the voltage applied to the dynode chain. However, these
devices must be characterized properly for optimal performance. The characteristics of
the PMTs used in this thesis were carefully examined before they were used
experimentally in order to determine data quality. This information was used to
determine the detection threshold and the noise characteristics.
2.6.1 PMT calibration
Calibration must be performed on all PMTs to ensure linearity of signal output for all
gain settings. The calibration setup is shown in Figure 2.8. A homogeneous cylindrical
phantom is placed in the middle of the fiber interface, and illuminated from the top
center. Neutral density filters, first characterized with a light power meter (Figure 2.8b),
are used to attenuate the input light over the full dynamic range of the PMTs.
16
b
a
c
Figure 2.8: (a) Setup for calibration. A laser diode illuminates a homogeneous
cylindrical phantom so that all PMTs have similar intensities. (b) Filter wheels
attenuate input light through the full dynamic range of the PMTs. (c) A circular
fiber interface fixes fiber locations during all measurements.
The amplitude response of a PMT is shown in Figure 2.9. Assuming the PMT
amplitude is linear, each PMT’s amplitude voltage (Vcal) can be calibrated by the
following transformation:
(2.1)
where a is the slope of the logarithm of the PMT output voltage (Vuncal) vs the logarithm
of the input light power, which is gain and PMT dependent, and b takes into account the
amplification due to the gain voltage.
17
a
b
Figure 2.9: (a) Uncalibrated and (b) calibrated voltages for a PMT. Since the voltage
response is linear over all gains within the linear detection region, PMT voltage is
calibrated for gain setting by removing the offset between voltages of identical input
light power levels at different gains, and dividing the voltage by the slope at each
gain setting.
The second step in detector calibration is to remove phase changes that are due to gain
voltage. Example phase response is shown in Figure 2.10. Since the pathlength of the
phantom is independent of incident light power, differences in absolute phase can be
removed from the uncalibrated phase (Phaseuncal) to calculate the calibrated phase
(Phasecal) using:
(2.2)
,where b is the gain dependent and PMT dependent offset in phase.
18
a
b
Figure 2.10: (a) Uncalibrated and (b) calibrated phase response for a PMT. Since
the pathlength of the measurement is independent of input light power, the phase
difference should remain constant. However, changes in PMT gain affect the
relative phase. This effect can be calibrated by subtracting the offset at each gain
level.
2.6.2 Noise characterization
Noise characteristics were determined by collecting light signals from varying input
powers. Standard deviations were calculated from 30 samples of light intensity and
phase. Figure 2.11 shows the amplitude and phase noise for all data points. Amplitude
noise was defined as a percentage of the voltage, as:
(2.3)
where σV is the standard deviation of the voltage, V. Phase noise was defined in units of
degrees, as:
19
(2.4)
where σPH is the standard deviation of the phase.
a
b
Figure 2.11: Amplitude and phase noise for all PMTs. (a) Plot of the standard
deviation in Voltage as a percentage of voltage vs log10 Voltage. (b) Plot of the
standard deviation in phase (in degrees) vs log10 Voltage.
These noise characteristics compare favourably to a similar frequency domain optical
system47, and are shown in Figure 2.12.
An undesirable feature of photomultiplier tubes used to record frequency domain
data is the nonlinearity in amplitude response and the lack of repeatability in phase
response. These characteristics determine an optimal voltage range during data
collection.
The amplitude response for a PMT with constant gain setting has a sigmoidal
shape, demonstrated in Figure 2.13. At the noise floor, below ~8mV, the signal drops
below the thermal noise. At this point, a decrease in input light power is not represented
by an equivalent decrease in output voltage. Above ~1V, the PMT is saturated, and an
increase in input light power does not equivalently increase the output voltage.
20
a
b
c
d
Figure 2.12: (a) Average AC voltage amplitude noise response of all PMTs for this
system, in (%) and (b) average phase noise (in degrees), compared to (c,d) a similar
system reported by Yalavarthy47.
a
b
c
Figure 2.13: Amplitude of AC voltage for all PMTs vs input power. At low input
light power, the signal is less than the noise floor, (c). When the input voltage is too
21
high, the PMTs saturate, (a). Between these limits is the linear detection region, (b).
This region is desired for detector amplitude linearity.
While the amplitude is linear over 2 orders of magnitude, the phase exhibits nonlinearity beyond 1 order because of the phase non-repeatability for low intensity light
over time.
Figure 2.14 exhibits PMT phase measurements before and after a system reboot.
The phantom was not removed from the optical fibers between measurements. Phase
measurements at low light levels below ~100 mV reveal the non-repeatability. This may
be attributed to error in detecting zero-crossings with low AC modulation voltages, or
because of different charge profiles across the dynodes upon recharge. Unfortunately,
this lower threshold is ~1 order of magnitude above the amplitude noise floor. In this
thesis, only phase data for output voltages between 100 mV and 1V is used, while
amplitude data between 8 mV and 1V is considered good quality. In this region,
amplitude noise is lower than 2% of the signal, phase noise is near ½ degree, and phase
changes less than 2% on different days for the lowest light levels.
a
b
22
Figure 2.14: (a) Uncalibrated phase differences through the same phantom on
different days, without changing fiber positions. Data collected on day 1 (solid), and
day 2 (dotted). Colors denote different PMTs. (b) Phase response for a constant
pathlength for PMT 8 on day 1 (red) and day 2 (blue).
2.7 Patient interface
Two different fiber interface geometries were used in this thesis to collect data. The
circular geometry that was originally developed was changed to the slab geometry to
improve data quality. These two interfaces are shown in Figure 2.15. This slab interface
was constructed of black acetal, similar to the circular interface, so that it was nonmetallic. A 3D rapid prototyping machine was used to print out grids which were
customizable for a specific application. These grids were printed out of ABS
(acrylonitrile butadiene styrene) and painted black to avoid reflection of stray light within
the interface.
23
Figure 2.15: (a) Circular and (b) slab patient optical interface attached to MR
breast coils with simulated optical overlays.
The slab geometry has several benefits over a circular design for MR guided
breast imaging. First, the slight compression, which is applied to conform the breast to
the parallel plates, results in shorter optical pathlengths and less signal loss. This
geometry maximizes the amount of quality data. Figure 2.16 compares data collected
from two resin tissue-mimicking homogenous phantoms with similar optical properties
and a healthy volunteer in the slab and circular geometries. The bar graph indicates the
amount of data that was below the phase noise floor of 100 mV AC amplitude at the
highest gain setting. Data below this limit should be dropped. In these cases, the slab
geometry yields better quality data with this system, as ~10% and ~30% more phase data
points are kept with the slab geometry for the phantom and volunteer study, respectively.
This is because of the higher density of shorter pathlengths through the tissue.
Figure 2.16: Data points dropped in calibration phantoms and one subject for slab
vs circle geometries. In these cases, the slab geometry yielded more datapoints that
were of good quality.
24
Improved data quality is expected to improve contrast recovery. To prove this
experimentally, slab and circular resin phantoms with India ink inclusions of 2:1 contrast
at identical depths were imaged to evaluate contrast recovery accuracy. Figure 2.17
shows that contrast recovery is improved by an average of ~16% when the slab geometry
is used because of the improvement in data quality. Although one disadvantage of noncircular geometries is that they distort the recovered shapes in standalone optical
mammography, as discussed by Pogue et al.48, MR guided methods used in this thesis are
invariant to shape errors because the shape is defined by MR.
Another important consideration in using the slab geometry for this thesis is the
ease in fiber positioning. By immobilizing the breast with a grid, fibers can be moved to
probe several regions of interest without changing the breast shape. This allows image
reconstructions with multiple planes of data without the expense and bulk of adding more
planes of fibers to the interface. This advantage is critical in patient imaging because
many lesions will not be located with MR until after the contrast agent is administered,
and any changes in breast volume after the injection will hinder accurate coregistration
between the altered breast shape and the contrast enhanced MR dataset.
Lastly, the slab geometry offers improvements to MR imaging because of breast
immobilization. Immobilization reduces image degradation due to patient motion caused
by respiration or discomfort. Patient motion leads to artifacts that affect typical breast
exams, including ghosting, inaccurate references for parallel imaging, and poor fat
saturation. These effects, which often plague proper breast MR images49, are expected to
decrease with the slab geometry.
25
a
b
c
Figure 2.17: (c) Percent errors in contrast recovery between identical inclusions in
the (a, blue) circular, and (b, red) slab geometries of resin phantoms. In the slab
case, contrast recovery in the inclusion was accurate within 1%.
The parallel-plate geometry was integrated into Philips and GE magnets by
coupling the interface to coils made by Invivo and USA Instruments, respectively.
Photographs are shown in Figure 2.18. The slab geometry was especially critical in
coupling to the USA Instruments coil because access was possible in the sagittal plane
only. This coil would not permit circular geometries.
26
a
b
c
d
Figure 2.18: Fiber interface integrated into an (a) Invivo breast coil in a (c) Philips
scanner, and a (b) USA Instruments coil in a (d) GE scanner.
2.8 Optical Magnetic Resonance mammography coil
To acquire images with optimal signal to noise, MR coils are designed to maximize the
fill factor, the volume between the coils filled by tissue. This is important because the
SNR is proportional to the square root of the fill factor50. However, maximizing this
parameter conflicts with maximizing the available space needed for optics. Indeed, the
original breast coil used in this study, designed by Invivo and illustrated in Figure 2.19a,
had significant space constraints, which limited placement of the optical fibers on the
tissue. To better accommodate optics, a custom MR breast coil was designed in
collaboration with Philips Medical Systems, (Hamburg, GER). This coil alleviated the
space constraints on the medial side of the original coil, which was limited because of the
angled top plate. The new breast coil, shown in Figure 2.20, moved the supports to the
27
periphery to increase open space within the coil. A simple circular insert supports the
optical holder and allows arbitrary rotation. We believe this new coil will offer the best
opportunity to image suspect lesions in future exam sessions.
2.9 Conclusions
This chapter focused on the details of the optical imaging hardware, and efforts to
achieve optimal data in MR guided optical breast imaging. The photodetectors in this
system demonstrated voltage amplitude linearity for 2 orders of magnitude (from 0.008 to
1V), and phase linearity for 1 order of magnitude (from 0.1 to 1V). If possible,
photodetector gains should be adjusted to maintain voltage measurements within these
regions. The photodetectors demonstrated amplitude repeatability of less than 2% of the
voltage and phase repeatability of less than 0.5 degrees, on average, within these regions.
It was determined that the slab geometry was the ideal geometry for optical breast
imaging in the MR because of the improvement in data quality. In one phantom and one
healthy subject, the use of the slab geometry allowed an average of ~17% more
datapoints because of the increased number of shorter pathlengths. The increased
number of quality data included more pathlengths across the inclusion, which improved
quantification accuracy in phantoms by ~7%.
This design also allowed the ability to image multiple planes of tissue with one plane of
fibers without altering breast shape, and increased flexibility in patient positioning.
28
a
b
d
c
e
f
Figure 2.19: Slab optical interface in three different MR coils. (a,b,c) Fiber
interface shown for the (a) Invivo coil, (b) USA Instruments coil, and the (c) Philips
Medical Systems, Hamburg, GER., custom optical/MR coil. Note the space
constraints which limit available fiber positions in the commercial coils including,
(d) the sloping top plate of the Invivo coil and the bulky support, and (e) the lack of
an aperture prohibiting fiber positions in the axial plane of the USA Instruments
coil. The custom designed coil has supports located towards the periphery, (f), and
an aperture near the subject’s head, allowing fiber positions in the superior/inferior
direction. (Optical coil photographs courtesy of S. Davis).
29
a
b
c
d
Figure 2.20: (a,b) Sketches (courtesy of C. Luessler, Philips Medical Systems,
Hamburg, GER) and (c,d) photographs (courtesy of S. Davis) of the optical/MR
breast coil.
30
Chapter Three: Imaging hemoglobin, water, lipid, and scatter with
Optical Tomography
3.1 Introduction
Diffuse optical spectroscopic tomography is a technique that creates images of tissue components by sampling tissue absorption and scattering properties at several
wavelengths in the near infrared range. This spectra is shown in Figure 3.151. The
near infrared spectrum is used because blood and water have similar absorption
magnitudes within the wavelength range of ∼600nm to ∼900nm, allowing the
measurement of these contents simultaneously at depths that are clinically relevant to
breast imaging. By determining endogenous absorption (µa) and scattering (µs’) optical
properties at multiple wavelengths, images of total hemoglobin, hemoglobin oxygen
saturation, water content, lipid content, and scattering properties can be recovered.
Figure 3.1: Tissue chromophore spectra in the near infrared range (from Eker et
al.51).
31
Hemoglobin species, water, and lipid content can be computed with optical
methods by solving a linear system that maps the optical absorption coefficients at
multiple wavelengths to tissue content concentrations. The transformation is given by:
(3.1)
where µa are the absorption coefficients in tissue which are dependent on wavelength, λ, and ε are well known51, 52 molar extinction coefficients which quantify the
absorption of tissue components, C at each wavelength. The contribution from all
wavelengths imaged (nwv) is used to determine these concentrations. Hemoglobin
absorption is determined by the concentrations of both oxy- and deoxyhemoglobin, which
depend on the volume fraction of red blood cells in the blood plasma (hematocrit), and
the amount of blood in the tissue. Water and lipid absorption, on the other hand, are
determined by the relative percentages of these components compared to pure (100%)
water and lipid53.
To compute µa and µa’, light can be modeled with a lossy diffusion equation54, 55
which accurately describes light propagation in tissue when scattering dominates over
absorption, and when source-detector distances are larger than a few scattering lengths.
This equation is given by:
(3.2)
Here, Φ is the fluence of the light at position r propagating with intensity varying
at frequency ω. The diffusion coefficient, D, is defined as:
(3.3)
32
and S is the modeled light source.
Optical light sources are modeled one mean free path
inside the domain.
This “extrapolated boundary condition” ensures that the source is zero at the boundary, a
condition necessary to meet diffusion theory boundary conditions56, 57. Light at the
boundary is modeled with a Type III boundary condition58:
(3.4)
where α incorporates the relative refractive index mismatch between tissue
and air, and is modeled by Fresnel’s law56, 59, 60, and
is the outward pointing normal
to the boundary.
In this work, the diffuse light propagation model is solved with the finite element
method61, a numerical technique used to solve partial differential equations (PDEs). This
method discretizes the domain into small elements on which the light propagation model
is approximated through locally varying basis and weighting functions. Finite element
methods have the advantage that they can solve PDEs over arbitrary, irregular domains.
The main disadvantage is they require sophisticated software to create high quality
computational meshes. The log-transformed magnitude of the light propagation from one
source through a breast domain is shown in 2D and 3D in Figure 3.2.
It is often convenient to solve the image reconstruction problem on these meshes.
However, image reconstruction often involves an inversion of a dense matrix which may
be non-invertible without regularization. This operation is computationally taxing,
especially on dense meshes. In these cases, a coarser grid can be used to represent the
optical properties, which improves memory efficiency and computational speed62.
33
Figure 3.2: Finite element meshes (a,b) and solutions of the light propagation of a
photon source (c,d) in 2D and 3D.
3.2 Image formation
To form images of optical chromophores, a least squares optimization is performed
which minimizes the objective function, Ω:
(3.5)
The goal is to reconstruct the parameters, µ, by minimizing the difference δ between the
measured data, d, and the data generated from the light propagation model, F(µ). In
equation 3.5, we minimize the L2-norm of δ = (d − F (µ)) to find a minimum in the least
squares sense. The influence of system noise may be reduced by including the
covariance of the data into a weight matrix, Wd. The system noise characterized in
Chapter 2 can be incorporated into Wd. The second term in equation 3.5 is included to
minimize the error due to unquantifiable data noise, such as fiber coupling errors, which
34
may guide the solution to unlikely or impossible physiological solutions. Thus, the
expected contrast in µ may be included by minimizing the L2-norm of µ relative to some
best prior estimate, µprior. This term incorporates covariances of the parameters into the
parameter weight matrix, Wµ. This formulation is the “generalized least squares” (GLS)
form63.
3.3 Weight Matrices
In the GLS formulation, weight matrices which characterize the expected noise and
contrast, are incorporated into the objective function. Specifically, Wd and Wµ
incorporate the covariances of the data and the parameters, respectively. They are
organized in matrix form for unknowns x as:
(3.6)
The variances are the repeatability of the unknowns. The covariances incorporate
knowledge about how unknowns vary with respect to each other. Here, the arrows
indicate how column unknowns vary with the row unknown. To use the system noise
weight matrix presented below as an example, 2 → 1 indicates how much measurement 2
varies as a direct result of variations in measurement 1, due to channel crosstalk in the
system hardware. An example of this effect would be the blooming artefact in a CCD
detector, where one pixel collects so much light that electrons spill over from its well into
a neighboring pixel, adding signal64. In an ideal system, the measurement covariances
would be zero. The system noise weight matrix, Wd is formulated as:
35
(3.7)
This matrix includes the noise statistics on the MR-optical instrument, presented in
Chapter 2. Wd has dimensions, (Number of Measurements x Number of Measurements).
In this system, the electrical crosstalk between PMTs is ignored.
The statistics on the chromophores are incorporated into Wc, which is derived
from Wµ, discussed in the next section. Ignoring crosstalk between parameters, this
matrix has the form:
Wc=
(3.8)
where each of the submatrices defines the variance and covariance of the chromophores
across the image. This matrix defines how much change is expected from the initial
guess, and the dependence of chromophores on each other.
3.3.1 Incorporating structural information from MR
The incorporation of structural or functional information has been under intense study
because it may make the inverse problem more immune to system noise, better posed,
and less underdetermined65. A detriment is that it may bias the reconstruction towards
incorrect solutions if incorrect priors are assumed.
36
The MR prior may be included in the image reconstruction by interpolating the
segmented MR image onto the computational mesh. Since image reconstruction is often
performed on coarser meshes, image segmentation may be quite poor, which could affect
the accuracy of the prior. This topic is investigated in more detail in Chapter 4. The
prior is used to form a weight matrix for a parameter or a combination of parameters,
depending on its information. Figure 3.3 gives an example of a structural prior and a
computational mesh that is derived from the same tissue volume.
Figure 3.3: Anatomical information can be easily interpolated onto the finite
element mesh if the modalities are coregistered since there is no positional error. In
this case, the anatomical prior is segmented into three distinct regions, 1-3.
This prior is input into the parameter weight matrix as a covariance matrix. The
covariance matrix describes how each unknown is related to the other unknowns. In a
relatively straightforward implementation, the parameters in each region are assumed to
be homogeneous, with equal expected contrast (variance) of σ2. In this case, the weight
matrix for the parameter, C is:
(3.9)
37
Other forms for this weight matrix will be developed in more detail in Chapter 4.
3.3.2 Incorporating quantitative information from MR
MR quantitative information can also be incorporated into the image reconstruction. If
this information is available, it can be used to form the initial guess. This initial guess is
necessary for Newton based non-linear reconstruction routines66, and is usually a
homogeneous estimate calculated from the optical calibration routine. An example of an
all-optical initial guess vs an initial guess modified to incorporate MR water quantitative
information is shown in Figure 3.4.
a
b
Figure 3.4: (a) Homogeneous initial guess from the optical calibration routine, (b)
initial guess both from optical calibration and an MR quantitative water prior.
This quantitative information could also be used in reconstruction algorithms that
minimize the difference between parameters and the initial guess, such as the objective
function of equation 3.5, where µprior may be:
(3.10)
38
and the value of each parameter is determined optically and/or with MR methods.
3.4 Derivation of the inverse solution
The generalized least squares framework for diffuse optical tomography was developed
by Yalavarthy et al.67. However, its formulation is included here so that the various MR
priors may be introduced into the model where appropriate. Minimizing the objective
function with respect to the parameters requires setting the derivative of equation 3.5
equal to zero. The derivative is:
(3.11)
where J is the Jacobian, the sensitivity of the model data to changes in the parameters68,
69
, described by:
.
The Jacobian can be reformulated to solve for the physiological parameters c, which
consist of oxyhemoglobin, deoxyhemoglobin, water, lipid, scatter power, and scatter
amplitude70-72, by a simple transformation:
(3.12)
This allows the reformulation of the weight matrices of the tissue absorption and scatter
parameters, Wµ, into expected contrast in physiology, Wc.
Since parameter estimation problems are inherently non-linear, they are solved
iteratively. The data model misfit, δ, can be reformulated by approximating F(µ) with a
Taylor approximation:
39
(3.13)
where
, and
. Substituting the Jacobian in for
:
(3.14)
This approximation now contains the iterative update to the parameters, and is substituted
into δ (ignoring higher order terms) as:
(3.15)
Substituting equation 3.15 into equation 3.11 and setting 3.11 equal to zero yields:
(3.16)
Simplifying 3.16 produces:
(3.17)
Substituting
into 3.17 results in:
(3.18)
which can be rearranged to become:
(3.19)
This formulation yields the most general form for recovering image parameters while
allowing control over both the data noise and parameter contrast. It can be simplified
with a few assumptions on the weight matrices to yield more familiar image
reconstruction formulations as illustrated below.
40
3.5 Alternate formulations
3.5.1 Tikhonov
The Tikhonov formulation73 can be derived if the data weight matrix, Wd, and the
parameter matrix, Wµ, are assumed to be diagonal and homogenous. In these cases,
equation 3.5 may be reformulated as:
(3.20)
where cd is the inverse of the variance in the measured data, and cµ is the inverse of the
variance in the parameters. This form can be simplified to:
(3.21)
where λ is the Tikhonov regularization parameter. Solving this equation for the image
update yields the iterative image formation equation:
(3.22)
where I is the identity matrix.
3.5.2 Levenberg-Marquardt
Alternatively, the objective function may be simplified if there is no known noise model
for the data, and no prior knowledge about the parameters, by minimizing:
(3.23)
In this case, the update equation is:
(3.24)
The difficulty with this formulation in optical tomography is the fact that the problem is
ill-posed; small changes in the unknowns at the center of the domain lead to negligible
41
changes in the data, and there is no unique set of unknowns which solves the
minimization. Numerically, the Hessian matrix (
) may be singular. To enable
inversion, a regularization term, λ, is added to enhance diagonal dominance on rows of
the Hessian matrix that have nearly linearly dependent unknowns:
(3.25)
Since this formulation does not minimize the objective function of equation 3.23, the
Levenberg-Marquardt approach decreases the regularization during the numerical update,
ideally until, λ=0, and equation 3.23 is solved 74. In practice, λ may become small, but
never reaches zero.
3.6 Conclusions
This chapter establishes the foundations for fitting numerical models to data. Of primary
interest is the inclusion of MRI priors which may be incorporated into optical
tomography, either spatially through a covariance function in the parameter weight
matrix, or quantitatively as part of the initial guess for the inversion routine. Chapter 4
investigates the inclusion of anatomical priors that define different tissue types. Chapter
6 presents a method to quantitatively and spatially incorporate MR water/fat separation
into optical tomography. Chapter 9 formulates a comprehensive model for recovering
tissue properties using multiple optical/MR priors.
42
Chapter Four: Methods of anatomically constrained MR guided optical
imaging
4.1 Introduction
This chapter describes tools that aid in co-registration and computation of MR-guided
optics. The first section describes the MR sequences that were used to anatomically
guide the optical reconstruction. The next section presents methods to incorporate MR
anatomical images into the optical reconstruction, and several reconstruction methods
which provide flexibility in constraining the solution. This analysis considers practical
issues related to both image segmentation and computational burden to allow selection of
the optimal method to incorporate structural information into the optical reconstruction in
2 and 3 dimensions
4.2 Determining boundaries and fiber locations with MR images
MR images provide a wealth of anatomical information which can be used to improve
optical reconstructions. T1- or T2-weighted MR images provide accurate tissue exterior
boundaries which improves the accuracy of the boundary conditions75 while improving
optical reconstructions76. Through proper marking of optical fibers with MR fiducial
markers, MR may provide accurate optical probe locations, which is critical to
minimizing model errors34, 77, 78. Fiducial markers, such as the ones used in this thesis
(Multimodality, © IZI Medical and Pin-Point, © Beekley), enhance in both T1 and T2
images. These may be placed around the ferrule of each fiber, as shown in Figure 4.1a,
or on the fiber holder, b. Placing fiducials directly at the fiber end is beneficial in fiber
43
interfaces which do not structurally fix the position of the optical fiber, and thus need a
marker closer to the fiber tip/skin boundary. However, markers placed too close to the
boundary may be mistaken for tissue in T1-W MR images, which may cause automatic
segmentation algorithms to fail. Placing a few fiducials to use as location references, as
in Figure 4.1b, may be a better option if fiber positions are rigidly fixed in the fiber
holder.
a
b
Figure 4.1: MR images which provide accurate tissue boundaries and fiber positions
via fiducial markers. (a) Fibers placed on the ferrule of each fiber, (b) fibers used
for position reference.
4.3 Separating adipose, fibroglandular, and suspect tumor tissue
Reconstructing for tissue types and regions of interest identified a priori has been shown
to improve optical quantification and suppress image noise34, 79, 80. Adipose tissue and
fibroglandular tissue may be separated with a T1- or T2-weighted MR sequence, based
on their different relaxivities. Suspect lesions may be identified with a dynamic contrast
enhanced MR technique (DCE-MR), with extremely high sensitivity12. Anatomical MR
44
imaging methods used in this thesis were part of the standard Philips or General Electric
breast imaging packages, and acquired at 3 Tesla field strength.
Adipose and fibroglandular tissue were separated with a 2D T1-weighted spin
echo sequence (TR/TE/flip angle = 900/10/90°, voxel size 0.7 x 0.7 x 3mm) or a 3D
spoiled gradient echo sequence (TR/TE/flip angle = 10/6/20°, voxel size 0.7 x 0.7 x
3mm) at 512 x 512 pixel resolution. 2D T2-weighted images with fat saturation were
taken to help identify cysts or regions with edema (TR/TE/flip angle = 6000/90/90°).
Regions of interest were determined with a DCE-MR sequence which consisted of 5 sets
of images taken at 1 minute temporal resolution beginning 40 seconds after intravenous
injection of a 20 mL bolus of a Gadolinium contrast agent (Magnavist © Bayer
Healthcare). These images were part of the Philips THRIVE sequence, which is a
bilateral high-resolution 3D spoiled gradient echo fat saturated sequence (TR/TE/flip
angle = 10/6/20°). A summary of the sequences used in this study along with
representative images is shown in Table 4.1.
To segment suspect regions of interest from the surrounding fibroglandular tissue,
pre-contrast images were subtracted from post-contrast images. An example image is
shown in Figure 4.2. This technique aids in lesion identification because background
tissues with short T1, such as fat, appear bright in T1-weighted DCE-MR sequences, and
may obscure suspect lesions nearby. Usually, a fat saturation sequence is used to
suppress the fat; however, it is not uncommon for fat saturation to fail in breast imaging.
Thus, subtraction aids lesion identification by subtracting out signal from background
regions devoid of the contrast agent. This method is used clinically at Dartmouth
Hitchcock Medical Center.
45
Image
Use
Representative Image
Sequence
2D T1-W
Adipose /
Spin Echo
Fibroglandular
Tissue
Separation
2D T2-W
Identification of
Spin Echo
cysts / edema
3D
Identification of
THRIVE
suspect lesions
(DCE-MR)
46
Table 4.1: The different MRI sequences used in this study were all used in the
optical image reconstruction. A breast clip, identifying the location of biopsy, is
shown as a green arrow in the DCE image (bottom).
Figure 4.2: DCE-MR subtraction image resulting from pre contrast image
subtracted from post contrast enhancement image. Note the ring enhancement
around the main lesion, identified by arrows on the right side of the image. The left
arrow identifies a small satellite lesion.
4.4 Anatomical Constraints
The optimal method to incorporate MR anatomical information into the optical
reconstruction is an ongoing topic of investigation. Fibroglandular, adipose, and suspectlesion tissue boundaries have all been utilized in various ways to guide how the image is
updated during the inversion process. These different approaches can be separated into
two main categories, referred to as “hard” and “soft” priors. These approaches differ in
the amount of certainty in the correlation between MR and NIR contrast.
47
Hard priors constrain optical properties to update independently in each MRdefined domain. These methods enforce MR boundaries. Thus, hard prior methods
assume perfect correlation exists between MR and optical tissue contrast boundaries.
These algorithms have been implemented in a number of ways. Yalavarthy et al.67, in a
breast geometry, assumed that each segmented tissue type (adipose, fibroglandular, and
lesion) was homogenous in the reconstruction, and recovered simulated physiological
properties within 3% with noisy data. Brooksby et al.81 reconstructed for a homogenous
adipose region, but allowed unknowns to update independently on a finer-resolution pixel
basis in the fibroglandular region, which was assumed to contain the lesion. They found
increased accuracy in a simulated breast domain. Schweiger and Arridge82 used a twostep procedure in the image reconstruction of a simulated human head by first
reconstructing the domain into homogeneous regions of skin, bone, gray matter, and
white matter, then inserting these optical property distributions as the initial guess for a
finer resolution reconstruction. Boas et al.83 simulated functional brain activation and
forced the optical properties to update from the initial guess only in the cortex. They
found that this approach improved reconstruction accuracy, although the accuracy was
limited at depth because of the remission probe geometry. Pogue et al. applied a similar
algorithm to tissue phantoms84 and a rat brain, and recovered optical properties to within
10%85.
Structural MR images can alternatively be used as soft priors, which spatially
influence the update in the tissue boundaries, without forcing the optical boundaries align
perfectly with the MR boundaries. Algorithms that incorporate soft priors allow slight
intra-region variations, while discouraging variations across boundaries. Intuitively, this
48
method should reduce the error for improper image segmentation86, although the effect
will be analyzed in more detail below. These algorithms have been implemented both
approximately and statistically. Barbour et al. 80, 87 demonstrated an algorithm which
assigned optical properties to segmented adipose and fibroglandular tissues. They
simulated small lesions within the fibroglandular tissue, and reconstructed the domain.
They found accurate spatial localization and quantitative recovery, as long as the
simulated lesion was a small perturbation in optical properties from the background.
Brooksby et al.34 and Yalavarthy et al.37 incorporated smoothing operators within each
tissue type in the regularization during inversion. This method was found to yield
accurate recovery of hemoglobin in phantoms to within 10%88, and was used in the
group’s clinical breast MR-optical studies89, 90.
Intes et al.35 and Guven et al.79 incorporated structural priors in the inversion
statistically through a Bayesian framework. The algorithm penalized optical property
updates across boundaries, and allowed for increased contrast to be recovered in regions
where a lesion was thought to exist. Optical property recovery in simulation was accurate
within 15%, even when MR did not specify a tumor region of interest.
A comparison image of a patient imaged on the same day with a stand-alone
optical instrument vs. an MR guided instrument is shown in Figure 4.3. The guided
reconstruction used a hard-prior technique to apply anatomical bounds. A notable feature
of these images is the recovery of optical properties in the fibroglandular tissue, which is
lost with stand-alone optical imaging.
An investigation into the practical considerations of a soft-prior and a hard-prior
based approach are presented below.
49
a
b
Figure 4.3: Physiological properties imaged on the same day using a a) non MRguided optical imaging instrument, and a b) MR-guided optical imaging, using a
soft-prior Laplacian filter technique. Note the increased contrast recovery with the
image-guided approach.
4.5 From MR images to computational domains
Incorporating MR images into the image reconstruction is non-trivial, especially in 3D,
and much effort has gone into processing these irregularly shaped domains91. The steps
to incorporate MR anatomical information, from image segmentation to meshing to
region labeling are overviewed in Appendix B.
50
Tissue types were semi-automatically identified and separated with a commercial
software package (Mimics, © Materialise NV). Tissue segmentation required two steps:
1) segmenting adipose and fibroglandular tissue from the T1-W images, and 2)
segmenting the region of interest in the subtraction image. The DICOM header tags were
Figure 4.4: Transforming MRI images for computational use requires 1)
segmentation of tissue types into adipose, fibroglandular, and suspicious lesions, and
2) creating a finite element mesh of the volume, and 3) tagging the mesh with tissue
regions.
automatically processed to co-register these volumes. In both cases, an intensity
threshold image segmentation technique was used to separate tissues. Some manual
segmentation was always required to eliminate image artifacts or fiducial markers that
were mistakenly included in a tissue type. To create a volume mesh, a surface mesh of
the outer boundary of the domain was exported to an in-house meshing software
package92, 93, which created a mesh at the desired resolution (usually 2-3 mm between
nodes). This mesh was then imported back into Mimics, which tagged the nodes with the
appropriate tissue material labels, and exported the mesh for use in the image guided
51
reconstruction algorithms. The 2D meshes used in this study had an average of 2000
nodes, while 3D meshes usually consisted of 30,000 nodes.
4.6 Computational burden considerations
Incorporation of MR structural information into the reconstruction algorithm helps ease
the dependence of the solution on the regularization, because it lessens the illposedness
and underdeterminedness of the image reconstruction problem by: 1) constraining the
solution space35, and 2) reducing the parameter space to a set number of tissue types and
regions of interest (ROIs)94. Using MR information results in solutions that are less
affected by noise and unexpected variations in contrast. In 3 dimensions, reducing the
number of unknowns is often critical to recovering an accurate solution. A comparison
of the number of computed unknowns for 2D vs. 3D vs. region-based (hard-prior)
imaging is shown in Figure 4.5. As described below, incorporating region information
may be prohibitively demanding in 3D when implementing soft priors. Thus, soft prior
techniques which allow for computationally tractable algorithms may be important in 3D
image-guided optical reconstructions.
52
Figure 4.5: A comparison of the number of unknowns calculated in 2D vs 3D for 2D
full, 3D full, and 3D region-based spectral reconstructions, for five parameters.
4.7 Implementation of Anatomical Constraints
4.7.1 Hard anatomical constraints
Region fitting effectively reduces the image formation to a spectroscopy problem, where
the unknowns in each region are reduced to one set of optical parameters. Thus, in the
three region problem shown in Figure 4.6, there are three sets of parameters, for a total of
15 unknowns. Regions are formed by creating a region matrix, K, which is sized
, where NN is the number of nodes, and NR is the number of regions94.
For each row i, a ‘1’ is placed on the column of node i’s region number. Otherwise, a ‘0’
is placed. This can be described as:
for row: node i, column: node iregion
(4.1)
otherwise
53
By multiplying the Jacobian by this region matrix, a region-based Jacobian is formed
which groups nodes of each region. Thus, the region-based Jacobian is sized
, the number of measurements NM by the number of regions NR.
Figure 4.6: Segmented breast MR used to guide
reconstruction methods. The labels within the image
1
define regions of adipose (1), fibroglandular (2), and
2
tumor (3) tissue. Blue x’s and red circles define the
3
source and detector locations around the breast.
The region-based method forms an overly determined problem if there are 240
measurements and 15 unknowns. Image reconstruction involves solving the image
formation equation with the region-based Jacobian. The region-based update equation
(equation 3.22 in Chapter 3):
(4.2)
is iteratively solved until convergence is reached.
4.7.2 Soft anatomical constraints: second differential Laplacian operator
One implementation of a soft-prior algorithm is based on enforcing tissue boundaries
through a Laplacian34. This formulation encodes the region information into the
regularization instead of reducing the problem to regions of unknowns. This technique is
described in more detail in the electrical impedance tomography literature95, 96. However,
54
the implementation here is a bit different, because the Laplacian is formulated so that it
smoothes across entire anatomical regions instead of at each spatial node location. The
foundation of this formulation lies in spectral graph theory, in which nodes of a given
region are interconnected at a single vertex97. An example of a simple graph is shown in
Figure 4.7.
a
b
Figure 4.7: (a) Example of a spectral graph (from Biyikoglu et al. 97). In optical
tomography, each row of the covariance weight matrix incorporates the regions
labeled in (b) with connectivity described by this graph.
55
The Laplacian matrix for a given region is:
i=j
i,j are not in the same region
i,j are in the same region
(4.3)
In this formulation, the update equation incorporates this Laplacian matrix into the
weight matrix for the parameters, Wµ.
(4.4)
This formulation smoothes within each region, while relaxing the constraint that the
solution cannot vary across the MR defined boundary. An issue with the Laplacian
method is that it can be computationally expensive, especially in 3D, because it does not
reduce the number of unknowns in a region unless a coarser second mesh is used for
reconstruction. Reconstructing on a coarser mesh will decrease the spatial resolution
defined in the spatial prior, because the spatial information is encoded in the nodes. One
method to alleviate the memory requirements is to use an adaptive mesh, where nodes are
placed with higher density near the boundaries. Another method, which is a hybrid hard
prior / Laplacian technique, is described below.
4.7.3 Hybrid Edge Constraining Filter
The hybrid method decreases the number of unknowns by condensing the adipose region
into one set of parameters, and using a Laplacian filter in the fibroglandular and tumor
regions. One can be sure that no tumors will be mistakenly misclassified as adipose
tissue, since vascularized tumors resemble fibroglandular tissue in T1-W MR images.
56
This method accomplishes two goals: 1) it reduces the computational cost, thus
making the problem less underdetermined, and 2) it allows optical variation in the
fibroglandular tissue which may reveal false negatives in breast MR. In most cases,
especially older patients at higher risk for breast cancer, there is a significant percentage
of adipose tissue in the breast89, and computational savings can be significant.
4.8 Comparison of spatial reconstruction methods with improper segmentation
Errors in segmentation may propagate into errors in the reconstruction. It was suggested
by Yalavarthy et al.67 that these errors might destabilize the reconstruction. Specifically,
Yalavarthy et al. found that a 7% dilation in the internal tissue boundaries led to a 368%
overestimation of the absorption coefficient in the region of interest. This error would be
prohibitive to any region-based reconstruction. Therefore, the effect of segmentation
error with a six wavelength spectral reconstruction, instead of a single wavelength
reconstruction used by Yalavarthy et al, was investigated with hard priors , the hybrid
algorithm, and the soft prior algorithms described above. To test different amounts of
segmentation error, two case studies of different breast densities and different
segmentation error were investigated. In both cases, the tumor and fibroglandular tissues
were dilated into the respective background. This approach approximated the error in
segmentation that is typically encountered with the image segmentation routines used in
this thesis. Case 1 is a heterogeneously dense breast, whereas case 2 is a case of scattered
breast density. For each algorithm, tissue types are defined by MRI and segmented.
Tumors were simulated in the fibroglandular tissue for each case. Data was generated on
a high resolution mesh (7.5 µm resolution), and reconstructed on a coarser mesh (450 µm
resolution).
57
4.8.1 Case Study 1: High Density Vascular Structure
Image segmentation is more accurate in breast tissue with high-density structure because
the vascular features are less spiculated. Data was generated on a 12,000 node mesh,
shown in Figure 4.8c, which could more accurately define tissue boundaries.
Reconstructions were performed on a coarser reconstruction mesh (~2000 nodes, Figure
4.8b) which was too coarse to accurately represent the segmented tissues. It is evident
that these two segmentation results are quite comparable, and the difference in region size
error between the two meshes is less than 7%.
Figure 4.8: (a) T1-weighted image of case study 1. (b) Coarse segmentation of (a)
used to reconstruct data. (c) Fine segmentation used to generate data. (b-c) are
color coded according to tissue type.
Figure 4.9a,b,c display images of each reconstruction result compared to the truth (Figure
4.9d). Figure 4.10 presents the error results for the different reconstructions. In this case,
the absorption errors (the average error for the absorbing chromophores of
58
oxyhemoglobin, deoxyhemoglobin, and water) were very accurate, within 2%, for all
reconstruction methods, with the hybrid region obtaining the most accurate chromophore
values. The hybrid reconstruction also obtained the most accurate quantification of
scatter (the average error of scatter amplitude and scatter power). In this case, the region
fitting and Laplacian reconstructions underestimated the scattering amplitude and
scattering power of the tumor, observed in Figure 4.9. This result is not unexpected,
because the tumor region values are the farthest from the initial guess. This
underestimation may be explained by the fact that the absorption becomes so close to the
truth that the stopping criterion is reached before the true solution is found (in these
algorithms, the stopping criteria is defined as a 1% change in the model/data misfit
between iterations).
59
Figure 4.9: Reconstructions using the (a) Laplacian matrix reconstruction, (b)
hybrid reconstruction, and (c) region fitting reconstruction. (d) True optical
contrasts and spatial heterogeneity.
60
Figure 4.10: Total errors in absorption (the average of oxyhemoglobin,
deoxyhemoglobin, and water) and scatter (the average of scatter amplitude and
scatter power) for all regions of each of the reconstruction algorithms.
4.8.2 Case Study 2: Low Density Vascular Structure
This case investigated reconstruction errors from a scattered density breast. Tissue with
fine fibroglandular features may result in more reconstruction error because the structure
is difficult to represent without a very dense mesh. Figure 4.11a shows the MR image,
and (b) and (c) show the reconstruction mesh and data mesh used in this study,
respectively. In this case, the segmentation error in reproducing the fine mesh with the
coarse reconstruction mesh was ~ 50%. This example tested the accuracy of these edgeconstraining algorithms when the anatomical boundaries used in the reconstruction did
not accurately align with the actual boundaries.
Figure 4.11: (a) T1-weighted image of case study 2 (b) Coarse segmentation of (a)
used to reconstruct data. (c) Fine segmentation used to generate data. (b,c) are
color coded according to tissue type.
61
Figure 4.12a-c shows the reconstruction results for the Laplacian filter, the hybrid
method, and the region-based reconstruction, respectively. These algorithms reconstruct
images that appear similar in structure to the reconstruction mesh in Figure 4.11b, since
they are edge-constraining. In addition, there is very little variation within each tissue
region. This is likely due to the edge preserving character of the algorithms which
prevents them from reconstructing fine features that aren’t provided in the spatial prior.
Reconstruction quantification errors are shown in Figure 4.13. These results
show similar errors in absorbing chromophores, within 2%, and are within 7% in total
error. The error in scattering properties decreases as the number of unknowns decreases,
from ~15% for the Laplacian reconstruction, to ~7% for the region reconstruction.
Figure 4.12: Reconstructions using the (a) Laplacian matrix reconstruction, (b)
hybrid reconstruction, and (c) region fitting reconstruction. (d) True optical
contrasts and spatial heterogeneity.
62
Figure 4.13: Total percent errors in absorption and scatter for case study 2 for each
of the reconstruction algorithms.
4.8.3 Conclusions comparing reconstruction methods
Segmentation errors will always creep into image reconstruction algorithms which
assume prior structural knowledge. In breast tissue, vascular features are difficult to
segment, and there is a danger that inaccurate priors will propagate into image estimation
errors. Effort has been devoted to developing methods that do not constrain the
boundaries of the anatomical prior, believing that inaccurate structural data will cripple
the region based edge-constraining algorithm. However, in contrast to the results shown
by Yalavarthy et al.37, these simulation results show that the edge-constraining algorithms
can achieve total errors within 10%, even when region areas are dilated by greater than
50%. It is important to note that these reconstructions were multi-spectral. Thus, this
study provides evidence that multi-spectral reconstructions are more robust not only to
data noise, as found by Srinivasan et al.72, but also to segmentation noise. These results
63
also show that including a Laplacian filter into the regularization yields an image with
similar structural boundaries to the region reconstruction. As expected, the recovered
value in the inclusion with each of these methods is underestimated, due to the spatial
prior which incorporates some lower contrast background tissue into the tumor region.
Thus, this bias towards background values can be expected in patient results. Although
all results provide suitable quantification, the total errors for both case studies are
minimized with the hybrid reconstruction, although there is not enough data to prove
significance. This conclusion is important for 3D geometries, as the number of spatial
nodes required to accurately model the boundaries becomes computationally unfeasible
to invert in the soft prior case.
4.9 Considerations in 3D imaging
The Laplacian soft priors approach suffers from high memory requirements in 3D
because of the need to store the structural information. This matrix can be prohibitively
large if high structural accuracy is desired. It cannot be reduced in size unless advanced
adaptive mesh techniques are used to preferentially apply a high density of nodes near
tissue interfaces. As an alternative, a hybrid region / Laplacian method was introduced
above which alleviates the computational burden for 3D reconstructions using soft prior
methods. This method combines the reduced memory requirement of the region
reconstruction in the adipose tissue with the less rigid constraint in the fibroglandular and
region of interest.
64
In this implementation, high optical contrast regions which are hidden in the MR images
may still be recovered. The computational savings offered by the hybrid approach is
shown in Figure 4.14.
GB
Figure 4.14: Memory requirements when using the Laplacian soft priors
reconstruction can be a computational limitation in 3D. By implementing a hybrid
approach, matrix storage for three patients reduces to a computationally feasible
size.
Figure 4.16 compares the optical recovery in 3 dimensions of a simulated
cylindrical inclusion, shown in Figure 4.15. The true values used to generate data with
5% amplitude and 5 degree phase white noise are shown in Figure 4.16c, whereas the
hybrid and region reconstruction results are shown in Figure 4.16a,b, respectively. As
noted above, the hybrid results look structurally identical to the region-based results
65
because of the high density of nodes which define the fibroglandular and tumor regions,
and because of the simple geometries simulated in this example. The errors in the
recovered parameters averaged over all regions are shown in Figure 4.17. These results
exclude the soft priors approach because of the limitation on computational memory.
The soft priors approach would have consumed 32 GB of memory, making the inversion
computationally unfeasible. In contrast, the hybrid approach consumed ~2GB of
memory. These reconstructions are within 10% accuracy, except for the oxygen
saturation recovery of the hybrid method, which had ~-13% error.
Figure 4.15: 3D mesh used in image reconstruction. The mesh consisted of ~20,000
nodes. Tissue regions are identified by color.
66
a
b
c
Figure 4.16: 3D reconstructions of (a) hybrid method and (b) hard priors compared
to (c) the truth. The hybrid method reduces the adipose tissue to 1 region, and
applies a Laplacian filter to the fibroglandular tissue and region of interest.
Figure 4.17: Percent error between recovered parameters and the truth for the 3D
hybrid method, and 3D hard priors.
67
4.10 Conclusions
Three reconstruction methods were presented above and analyzed for segmentation errors
and computational burden. The results of several reconstructions show that these
algorithms recover quantification with similar accuracy; no algorithm was poorer than
10% in error relative to the other methods. In 3 dimensions, the soft prior algorithm
becomes computationally intractable, while the hybrid method enables a soft prior
approach within the fibroglandular tissue and region of interest.
The similar accuracy provided by these methods allows for flexibility in image
reconstruction. Region fitting will not delineate regions that are missed by MR, because
they will be hidden in the background. These false-negative cases require soft prior
algorithms that allow variation within the regions. With 3-D geometries, the hybrid
method may be the best approach to imaging features missed by MR, as it reduces the
number of unknowns, while still allowing features not identified by MR to enhance. In
cases where MR has imaged a suspect region of interest, optical imaging may be used as
a spectroscopic method via the region-fitting algorithm. Throughout the remainder of
this thesis, the region-fitting algorithm is used because all regions of interest enhance on
MRI.
68
Chapter Five: MR guided optical imaging for tumor characterization
and neoadjuvant chemotherapy monitoring
It has been established in the optical imaging community over the past 10 years that
breast cancers have significantly higher total hemoglobin, water content, and scatter, and
lower lipid fraction relative to normal tissue 23-25, 98-100 and benign lesions22, 101, 102.
Because of its modest cost and non-ionizing radiation, optical imaging may aid in either
the screening100 or diagnosis of breast cancer. In addition, because optical imaging may
be applied frequently without safety concerns, it may hold promise in monitoring the
effectiveness of chemotherapy103-105.
In several clinical trials, optical imaging has been shown to improve upon the
specificity reported from clinical breast imaging21, 22, 101. However, its modest spatial
resolution has resulted in study designs which limit lesions to sizes greater than 8 mm21.
One study which included small lesions noted poorer characterization of tumors less than
6mm22.
Image-guided NIRS has shown promise to rectify these spatial resolution problems
because the high resolution modality (e.g. MRI or x-ray) helps identify tissue types
within the breast which guide contrast distribution19, 89. This technique improves both the
spatial resolution and quantification accuracy of optical imaging34-36, and has been used
in several initial clinical breast cancer studies90, 106. In particular, Ntziachristos et al.
noted trends between increased hemoglobin and lower oxygenation in malignant tumors
with higher spatial accuracy with MR-guided optical imaging33. Carpenter et al. noted not
only increased hemoglobin and decreased oxygenation in tumor tissue, but also increased
69
water and increased average particle size and density with MR-guided optical imaging90.
Studies by Gulsen et al.107 and Xu et al.108 recovered optical properties in small animals
with MR guidance. Gulsen et al. confirmed an anticipated increase in optical properties in
the tumor tissue; Xu et al. confirmed anticipated changes in optically recovered tissue
oxygen saturation and hemoglobin concentration due to inspired O2.
Although the clinical performance of these co-registered multimodality approaches
has yet to be fully evaluated in a complete trial, these results suggest that MRI-guided
NIRS will improve upon the results obtained with stand-alone NIR imaging. This section
will present several case studies demonstrating the potential for image-guided optical
tumor characterization and treatment monitoring.
5.1 Detection and characterization of breast tumors
This section reports the results from five patients. Three patients were imaged prior to
the start of neoadjuvant chemotherapy, one patient was imaged during the late stages of
chemotherapy, and one patient was imaged during a callback for a mammographically
determined suspicious lesion. All subjects provided informed consent and were imaged
according to study protocols approved by the Institutional Review Board at Dartmouth
Hitchcock Medical Center.
5.1.1 Reconstruction methodology
All patients images were reconstructed using anatomical maps provided from MR.
Tissue types were encoded with region-based constraints. As discussed in Chapter 3,
choosing the appropriate regularization is a compromise between system noise and image
contrast. Since noise depends partly on fiber contact, which is not repeatable, it is
70
expected that one regularization scalar would not suffice for every patient. Therefore,
each reconstruction used the minimum regularization that would allow the solution to
converge (in this case, defined as iterating more than 3 times). Additionally, if a
recovered value was not physiologically possible in breast tissue, a larger regularization
value was chosen. These steps were taken to balance the detrimental effects of noise on
the inversion, while ensuring that the contrast was not suppressed unnecessarily. All
datasets were processed according to the signal noise floor limits discussed in Chapter 2;
amplitude or phase data that was below the noise floor was not used in image
reconstruction. In subject 5, the soft prior algorithm would not converge for any
regularization. Thus, to be able to compare all subjects, only region-based
reconstructions are presented. Additionally, volumetric MR was not available for subject
2, so all subjects were reconstructed in 2D. In the text below, the fibroglandular tissue is
referred to as the “background.” Because MR can easily distinguish vascular tissue,
including highly vascular lesions, from fatty tissue, the goal of MR guided optical
spectroscopy is to separate the malignant vascular tissue from the background nonmalignant vascular tissue.
5.1.2 Results
5.1.2.1 Subject 1
This subject had three suspicious lesions in her right breast. MR imaging results showed
that two of the lesions were cysts. These were clinically aspirated and found to be nonmalignant. One lesion was biopsied and found to be benign fibrocystic disease. Imaging
was performed prior to biopsy. Optical imaging results show a slight decrease in total
hemoglobin of 0.018 mM in the lesion in the plane of the fibers compared to the
71
fibroglandular tissue at 0.020 mM. These results are expected in cysts which are usually
filled with fluid, and are void of the densely packed vasculature indicative of breast
tumors. Oxygen saturation was slightly higher than the fibroglandular tissue, at 78%
compared to 73%. As expected in fluid filled cysts, water was found to be higher than
the background tissue, at 60% compared to 40-50% in the background. The cyst showed
no contrast in scatter amplitude, but a slight increase in scatter power.
a
b
d
c
e
Figure 5.1: (a) Anatomically guided optical images and (b-e) MR images of Subject
1 (no malignant tissue, 2 cysts, 1 benign fibrocystic lesion). Note the slight decrease
72
in total hemoglobin compared to the background. (b) T1-W image in the plane of
the optical fibers. (c) Gadolinium dynamic contrast enhanced MR image. (d) T2-W
image showing increased water content expected in the cyst / benign lesion (e)
Maximum intensity projection of the DCE-MR image. Note the tumor identified by
the green arrows.
5.1.2.2 Subject 2
This subject, a 36 yr. old woman at the time of imaging, had a 3cm IDC & DCIS lesion in
the right breast. Imaging was performed 1 day following the 3rd cycle of treatment. The
reading radiologist reported a suspicious lesion appearing in the DCE-MR which was not
apparent on previous MR scans. Pathology performed 7 weeks later revealed a complete
response to chemotherapy with no viable tumor remaining. However, residual scar tissue
remained in the area, which likely contributed to the lower quantities of hemoglobin,
oxygenated hemoglobin, and water, and contrast in scatter, as compared to the
background. The fibroglandular features in this case were too finely structured to be
properly segmented and analyzed independently (see Figure 5.2b), so tissue was
segmented into the region of interest and the background (fibroglandular and adipose).
Results show slightly decreased hemoglobin of ~0.010 mM in the region of interest,
compared to ~0.014 mM in the background. Oxygen saturation in the region of interest
was lower than the background, and water concentration was also reduced. Contrast is
also seen in scatter. This case is an interesting demonstration of where the NIR
information could have significant diagnostic potential to eliminate the false positive
reading of the MR exam, which would have in some cases lead to an additional biopsy.
73
a
b
c
d
e
Figure 5.2: (a) Anatomically guided optical, (b-d) MR, and (e) pathology images
images of Subject 2. (b) T1-W image in the plane of the optical fibers. (c) Dynamic
contrast enhanced subtraction image used to segment region of interest (green
arrow). (d) Maximum intensity projection gadolinium contrast enhanced image
(lesion identified with arrow). (e) Mass pathology slice showing residual stromal
tissue and no viable tumor hemorrhaging.
74
5.1.2.3 Subject 3
This subject was a 29 yr old woman with 2cm infiltrating ductal carcinoma of the right
breast. She was imaged 5 days post biopsy, just prior to the start of neoadjuvant
chemotherapy. A region of interest can clearly be delineated from the gadolinium
dynamic contrast enhanced MR images, shown in Figure 5.3. Optical imaging results
show increased total hemoglobin in the tumor, at about 0.080 mM, whereas the
background was around 0.025 mM. Hemorrhaging in the tumor can be identified
visually in the pathology specimen as dark regions. This area had high vascular density
and epithelial content. An increase in oxygen saturation of ~80% compared to ~65% in
the background also exists in the tumor area. A decrease in water content is apparent.
This region also exhibited increased scatter amplitude and scatter power compared to the
background.
a
75
b
d
c
e
Figure 5.3: (a) Anatomically guided optical, (b-d) MR, and (e) pathology images of
Subject 3, who had a malignant lesion. (b) T1-W image in the plane of the optical
fibers. (c) Dynamic contrast enhanced subtraction image used to segment region of
interest (green arrow). (d) Maximum intensity projection gadolinium contrast
enhanced image. (e) Mass pathology slice showing tumor size post treatment. Note
the haemorrhaging (black in color) corresponding to total hemoglobin contrast, and
the surrounding necrotic tissue (tan in color).
5.1.2.4 Subject 4
This subject, a 51 year old woman, had a 7cm IDC in her left breast prior to
chemotherapy. Imaging was performed 1 week prior to the first cycle of chemotherapy.
This tumor did not fully respond to the chemotherapy, according to pathologist
76
assessment post operation. MR-NIR results showed an increase in hemoglobin to ~0.250
mM compared to 0.045 mM in the background. Hemoglobin oxygenation was increased
to about 90% in the region of interest, slightly higher than the background, and water
showed increased contrast of near 95% compared to the background at ~90%. A slight
decrease in both scatter amplitude and scatter power was seen in the region of interest
defined by DCE-MR. It is important to note that in this case the optical system was not
able to fully sample the center of the volume of the tumor. Instead, a plane was imaged
near the extreme anterior of the tumor. A full mastectomy specimen was not obtained in
this case because the patient transferred to another hospital for surgery. Instead, biopsy
specimens were used to confirm chemotherapy response.
a
77
b
c
d
Figure 5.4: (a) Anatomically guided optical and (b-d) MR images of Subject 4, with
a known malignant lesion. (b) T1-W image in the plane of the optical fibers. (c)
Gadolinium dynamic contrast enhanced MR image. (d) Maximum intensity
projection of the DCE-MR image.
5.1.2.5 Subject 5
This subject, a 36 year old woman at the time of imaging, had a 3cm IDC with 3 satellite
lesions in her left breast. The plane of optical fibers intersected with a satellite lesion.
Imaging was performed prior to the start of chemotherapy. Images show increased total
hemoglobin of 0.020 mM in the region of interest compared to the background., at 0.015
mM Oxygen saturation, at 65%, is higher than the background, at about 55%, and water
is decreased at 60% compared to background tissue. The region of interest exhibits a
78
10% decrease scatter amplitude compared to the background, and there is no contrast in
scatter power. A more detailed investigation into monitoring this patient during
neoadjuvant chemotherapy is presented below.
a
b
c
d
79
Figure 5.5: (a) Anatomically guided optical and (b-d) MR images of Subject 5. (b)
T1-W image in the plane of the optical fibers. (c) Gadolinium dynamic contrast
enhanced MR image. (d) Maximum intensity projection of the DCE-MR image.
Note the tumor identified by the green arrows.
5.1.3 Discussion
Total hemoglobin seems to be the only consistent delineator between the malignant tissue
and the benign and responding tissue. This differentiation is likely due to the increase in
vascular content in malignant tumors. These results are summarized below. Figure 5.6
shows a comparison of the total hemoglobin in the region of interest vs the background
tissue for all subjects. Since tumor tissue is a subregion of the fibroglandular tissue,
fibroglandular tissue is designated as the background in this analysis. Malignant tumors
in subjects 3, 4, and 5 clearly have higher hemoglobin than the background
fibroglandular tissue, whereas the normal / benign and responding cases show
comparable or less total hemoglobin than the background.
80
Figure 5.6: Comparison of tumor to fibroglandular total hemoglobin across all
subjects. The subjects denoted in the non-shaded region, subjects 3, 4 and 5, had
known malignant lesions. In contrast, the shaded region consisted of subject 1, who
had a benign/normal lesion, and subject 2, who was fully responding to
chemotherapy. Total hemoglobin is higher than the background fibroglandular
tissue in the known malignant tumors.
Figure 5.7 displays tumor to fibroglandular contrast ratios for each subject,
defined as
. For this metric, a value of zero indicates that the
region of interest had the same amount of total hemoglobin as the background, whereas
positive/negative contrasts indicate more/less total hemoglobin than the background.
Figure 5.7: Tumor to background contrast ratios of total hemoglobin for all
subjects. Negative contrast indicates that the background had higher total
hemoglobin than the region of interest.
81
The total hemoglobin results agree with established trends in total hemoglobin,
but are larger than typical findings reported in the literature. Tumor to background total
hemoglobin contrast ratios of 0.16101, 0.3522, ~0.599, 0.36100, and 4.8109 have been
reported for various optical systems around the world. The average contrast ratio
reported here of 3.3 is at the high end of these results, especially considering that the
background is fibroglandular tissue. Total hemoglobin in fibroglandular tissue typically
is higher than the adipose and fibroglandular tissues averaged together (the background
tissue for the studies with non-MR guided systems). This higher contrast could be
explained by the improved contrast recovery of image-guided systems.
Investigation of oxygen saturation, water percentage, and scatter amplitude and
power show no consistent trends. Although tumors are known to have local regions of
hypoxia, near infrared imaging of macroscopic regions has shown inconclusive trends in
the literature. Several larger studies99, 103 have shown no significant separation between
malignant tissue and background, even with wavelengths in the water sensitive band
beyond 900nm109. This is probably due to the low-resolution bulk measurements of
optical imaging, which cannot resolve the microscopic regions of hypoxia. Water has
been shown to have significantly higher concentration in malignant tissue25 than the
background. This trend is not consistently observed in these cases. However, this study
may be hampered by a lack of longer wavelengths in the spectral region most sensitive to
water, and water contrast may have crosstalked to oxyhemoglobin. This factor will be
investigated further in Chapter 6. Scatter amplitude and power have shown inconsistent
differentiation in the literature, and the data here support these results. Spinelli et al.109
82
showed no significant differentiation, while Cerussi et al.25 showed increased scatter
power.
a
b
c
d
Figure 5.8: No consistent trends between known malignant and suspect nonmalignant lesions are apparent for (a) Oxygen saturation contrast, (b) Water
contrast, (c) Scatter Amplitude contrast, and (d) Scatter Power contrast for all
subjects.
5.2 Monitoring neoadjuvant chemotherapy: A case study
The use of neoadjuvant chemotherapy to manage breast cancer treatment is increasing
because it has been shown to be as effective as post-operative adjuvant chemotherapy110,
111
, while enabling the option of breast conserving surgery in some cases112. Imaging
83
tumor response has the potential to gauge the effectiveness of the therapy, allowing the
possibility of tailoring a drug regimen to the individual, or determining survival
outcomes. Because of its potential, imaging disease response to neoadjuvant
chemotherapy has become a significant topic of interest in the literature.
Magnetic resonance studies to date have shown significant response to treatment
with a number of indicators, including tumor size113, DCE-MR enhancement kinetics114,
diffusion weighted imaging115, and spectroscopy116. However, diffusion weighted MR
and dynamic enhancement methods have also been shown to be inconsistent prognostic
indicators117, 118, suggesting that the efficacy of these tools may be sensitive to technique.
MR determination of tumor volume appears to best indicate response, based on a number
of successful pilot studies118-121.
Alternatively, optical imaging has also been shown to be an effective way to
monitor chemotherapy response in the breast. Cerussi et al.104 demonstrated in eleven
subjects that NIRS could perfectly separate chemotherapy responders vs. non-responders
within the first week of treatment via monitoring the absolute concentration of total
hemoglobin, and relative differences in deoxyhemoglobin and water. Jiang et al.105
confirmed the trend of decreasing total hemoglobin in four responding patients vs three
patients who showed incomplete response. These trends, along with the successes in
MR, indicate a potential opportunity to use MR guided optical imaging to monitor
chemotherapy.
5.2.1 Study methodology
Subject 5, investigated above, was scheduled for seven imaging sessions during
neoadjuvant chemotherapy. Table 1 displays the timeline of all imaging exams. The
84
3cm invasive ductal carcinoma and three satellite lesions fully responded to
chemotherapy, according to pathologist assessment post-operation. Session 3 was
cancelled because of a malfunction in the cable that connected the breast coil to the MR.
Session 2 was not analyzed because the fibers did not intersect with the plane of the
contrast enhancing tumors. Sessions 6 and 7 were not analyzed because the tumors were
not visible in the MR, most likely due to full chemotherapy response.
Imaging Session
Treatment
1
Pre
2
2 days post Cycle 1
Notes
Fibers out of tumor plane
3
Cancelled
4
2 days post cycle 2
5
2 days post cycle 3
6
No visible tumor in MR
7
No visible tumor in MR
Table 5.1: Overview of imaging sessions for the subject monitored during
neoadjuvant chemotherapy.
Lesions were identified from the dynamic breast MR images with the aid of 2 radiologists
(S.P. and R.D-A) that had 15 and 10 years of experience, respectively. All imaging sets
were reconstructed with the hard priors region reconstruction in 3 dimensions, to allow
recovery of out-of-plane features. Reconstructions used the minimal regularization that
would allow the solution to iterate, as described above. At regularization values greater
than this level, the results were invariant to changes in regularization.
85
5.2.2 Results
Optically recovered total hemoglobin images overlaid on DCE-MR subtraction images
for session 1 (Figure 5.9), session 2 (Figure 5.10), and session 3 (Figure 5.11) are shown
below, displayed with VolView software (© Kitware, Inc.). These results show the
volumetric changes in contrast enhanced MR that are typically seen in tumors that
respond to chemotherapy118. The anterior satellite lesion was consistently located in the
optical fiber plane in each of the 3 successful imaging exams, and its values were used
for analysis. Optical imaging indicates a decrease in total hemoglobin over the course of
the treatment. The changes in total hemoglobin, oxygen saturation, and water content are
shown in Figure 5.12. Total hemoglobin decreased from ~ 0.038 mM to ~ 0.020 mM
between cycle 1 to cycle 2, due to the reduction in the tumor size, and likely the
normalization of tumor vasculature. Tumor total hemoglobin did not change significantly
between cycle 2 and cycle 3. Oxygen saturation also decreased, likely because of
destruction of functioning tumor vasculature, restricting tumor perfusion. Water
diminished in this lesion from about 52% to 38%, most likely because of the reduction in
functional vascular tissue in the tumor.
86
a
b
c
Figure 5.9: a) DCE MR images of a subject with an IDC taken 1 day prior to
chemotherapy shows slight enhancement of 1 main node with 3 satellite lesions. b)
MR-NIR images overlaid on a). The lesions in the plane of the optical fibers of the
MR-NIR instrument show increased hemoglobin over the background. c) The
colorbar used for quantitative analysis of hemoglobin in b).
87
a
b
c
Figure 5.10: a) DCE MR images of the subject from taken within 48 hours of the 2nd
cycle of chemotherapy. Two lesions enhance, although the main lesion shows less
enhancement, indicating response to chemotherapy. Note the decrease in total
hemoglobin between b) and the previous figure, demonstrating response. Pathology
(not shown) taken after the completion of chemotherapy showed a complete
response. c) The colorbar has been duplicated here for comparison.
88
a
b
c
Figure 5.11: a) DCE MR images of subject 5 within 48 hours of the 3rd cycle of
chemotherapy. By this imaging session, the main lesion no longer enhanced, as
confirmed by the reading radiology (R. D-A.). The satellite lesion exhibited very
slight enhancement. These factors indicate a strong response to chemotherapy. (b)
Total hemoglobin in the lesion was within 0.001 mM of the background. Pathology
(not shown) studied after the completion of chemotherapy showed a complete
response. c) The colorbar has been duplicated here for comparison.
89
a
b
c
Figure 5.12: Quantitative Comparison of (a) total hemoglobin, (b) oxygen
saturation, and (c) water content in an invasive ductal carcinoma over 3 cycles of
chemotherapy in a complete responder.
Discussion
This section presents results measuring tumor optical properties with MR guided optical
imaging. The ability to obtain spectroscopic information about the tissue is likely to add
pertinent information to MR monitoring of neoadjuvant therapies. Optical imaging
identifies a trend of decreasing total hemoglobin, oxygen saturation, and water in the
responding tumor. These changes correspond to subsequent changes in the size of the
enhancing lesion identified by DCE-MR.
90
A notable complication with this study is the significant partial volume effects in
imaging the tumor volume during different imaging sessions. Inconsistencies in patient
positioning and optical fiber positioning may cause the tumor region of interest to be out
of plane. This may result in an underestimation of tumor optical properties because the
tumor is not properly sampled. In this study, a breast clip was inserted into the tissue at
the center of the main lesion. This clip provided magnetic resonance contrast, which was
used to determine the position of the tumor relative to the optical fibers. Only those
imaging sessions that were determined to sample the lesion were used. Without this clip,
precise knowledge of the tumor plane must be based on tissue morphology, which is
extremely difficult to determine because of the tissue changes during chemotherapy
response and menstrual cycle changes. This complication must be addressed when
conducting larger scale studies in the effectiveness of monitoring treatment with MR
guided optics. A possible solution could be to use a skin marker to appropriately position
the fiber plane.
5.3 Conclusions
MR-guided optical imaging shows promise in both determining breast cancer malignancy
and monitoring neoadjuvant chemotherapy outcomes. Although this sample size is small,
image guidance appeared to improve hemoglobin contrast between tumor tissue and
background healthy tissue. In all known malignant cases, hemoglobin was at least 50%
higher than the background fibroglandular tissue. In addition, MR guidance allowed
discrimination of tissue regions which may be compared or monitored separately via
optical imaging. In one patient who was undergoing neoadjuvant chemotherapy, a trend
of decreasing total hemoglobin, oxygen saturation, and water was observed. These
91
changes were consistent with the decrease in tumor volume, which is an indication of
therapy response.
Acknowledgements
Special thanks are extended to Dr. Stephen Poplack and Dr. Roberta Diflorio-Alexander
for their aid in the interpretation of the breast MR images in this study. Special thanks
are also extended to Dr. Wendy Wells for her help in the interpretation of the breast
pathology.
92
Chapter Six: Incorporating MR water fat separation
6.1 Introduction
Quantitative accuracy in optical imaging is greatly improved if wavelengths are chosen
that are most sensitive to the spectral features of the tissue chromophores122. However,
wavelength choice is often limited by the spectral sensitivity of the photodetectors. It is
well known that crosstalk between the spectral features of the tissue, caused by
insufficient spectral sampling, can introduce errors in quantification with optical imaging.
In this study, the photomultiplier photodetectors had inherent limitations in spectral
sensitivity (Figure 6.1, R6357) due to the wavelength dependent quantum efficiency of
the photocathodes. With these detectors, SNR is insufficient for optical imaging in deep
tissue above ~850nm.
Figure 6.1: Spectral response of the
R6357 photomultiplier tubes used in
this study (courtesy of Hamamatsu
Photonics). Note the cutoff in sensitivity
at wavelengths longer than 800nm.
93
Unfortunately, the spectral features of water in the near infrared are most
pronounced above 850nm (with a spectral peak at ~975nm). A lack of longer
wavelengths will lead to errors in water quantification. Since the water spectrum
overlaps with oxyhemoglobin in the spectral region of these photomultiplier tubes
(shown in Figure 6.2), there will be significant crosstalk, leading to quantification errors
in hemoglobin and oxygen saturation.
a
b
Figure 6.2: (a) Tissue absorption spectra for tissue optical properties of 20µM HbO,
20µM Hb, and 60% water. (b) Tissue absorption spectra approximately in the
sensitivity region of the PMTs. Note the spectral similarity between oxyhemoglobin
(HbO) and water.
Several groups have studied the hemoglobin errors incurred from spectral
crosstalk with water. Franceschini et al. 123 determined that with two wavelengths in
these PMTs’ spectral window (715 and 825nm), water errors elevated calculated
oxygenation to 75%, while the true quantities of total hemoglobin and oxygen saturation
94
were 30µM and 60%, respectively. These errors increased as both total hemoglobin and
oxygenation decreased. Cerussi et al.53 found that water errors caused by imaging with
672, 806, and 849nm compared to imaging using the broadband NIR spectrum could
induce errors as high as 60% and 10% in total hemoglobin and oxygenation, respectively,
in a diseased breast.
In order to correct for water quantification errors, investigators have either
attempted to remove water crosstalk by assuming water values106, 124, or calculated the
water content from scattering power124. These techniques are suboptimal because each
subject has a unique water distribution, and scatter power measurements are sensitive to
structural tissue properties that are independent of water concentration.
This chapter investigates the use of MRI water/fat separation to provide water
quantification. MR water/fat separation has been proposed previously by Li et al.125, who
used this information to provide a map to spatially guide the optical reconstruction. This
section describes efforts to extend this technique by using the MR’s ability to accurately
quantify water and fat, in addition to spatially guiding the reconstruction. By utilizing the
quantitative images of water and fat, it will be shown that hemoglobin recovery is more
quantitatively accurate.
6.2 Separating water and fat with MR
There are several different approaches to separate water and fat signals in the MR. These
methods are based on the proton chemical shift, where differences in the local electronic
environment of lipids and water cause differences in the resonant frequency of protons
that are exposed to an external magnetic field. The choice in method involves a trade-off
between speed and quantitative accuracy.
95
The faster water/fat sequences either reduce the signal of the unwanted
component by spectrally saturating it (e.g. Short Tau Inversion Recovery126, or Spectrally
Attenuated Inversion Recovery127), or enhance the signal of the desired component by
spectrally selecting it (e.g. ProSet128). These sequences are commonly used clinically to
suppress undesired fat signal, such as during dynamic contrast enhanced breast MR12.
However, these sequences have relatively poor fat and water quantification, especially at
3 Tesla, because of their sensitivity to the high magnetic field inhomogeneities in the
breast129. These inhomogeneities in the main magnetic field (B0) and the RF excitation
field (B1) cause incomplete spectral selection, resulting in poor diagnostic images130, and
poor water/fat separation.
This study required the most quantitatively accurate water/fat separation
technique. The DIXON-type sequences, originally developed by Dixon et al.131 and
Glover et al.,132 are optimal for this purpose. These sequences sample the magnetic
signal in the tissue at 2 or more echo times to enable the decomposition of the total signal
into water signal and lipid signal. Since the proton density of these two constituents
dominate the signal in MRI, images of water and fat percentage can be calculated simply
by taking the ratio of either component to the total signal133. These methods are slower
than the signal suppression sequences mentioned above because they require three
images to separate water, fat, and the B0 field. However, the increased accuracy far
outweighs the cost of longer acquisition times.
In this study, a DIXON-type sequence named IDEAL (Iterative Decomposition of
water and fat with Echo Asymmetry and Least-squares estimation) was used, which
improves SNR of the DIXON sequence by minimizing the effects of noise on each
96
component134. This sequence has been shown to have extremely high lipid quantification
accuracy in the liver135 and ex vivo swine samples 136. One particular study of oil/water
phantoms, which used the same sequence as in this thesis, found a 3.7% mean difference
in lipid quantification between IDEAL and the “gold standard” (MR spectroscopy)137.
This study concluded that the IDEAL MR sequence was the optimal sequence to provide
quantitative water and fat content. In the work that follows, lipids are ignored in the
optical reconstruction since their spectral contributions to the photodetectors is
insignificant. Once water images are formed, lipid images can be calculated simply by
subtracting the water percentage from 100.
6.3 Previous work correlating optical and MR water and fat
It is critical in this study that the water and fat measured by the MR are the same
substances that are measured optically. In principle, optical and MR imaging are
sensitive to different characteristics of water and lipids; whereas optical imaging is
sensitive to the electronic structure, MR imaging is sensitive to the proton resonance,
which is affected by local magnetic shielding. However, for a given voxel of tissue, these
modalities can separate signal into water and lipid volume fractions.
The total signal detected by MR depends on the proton density, ρ, a scaling
factor, k, which depends on coil sensitivity138, and a relaxation factor, R, which is
dependent on tissue relaxation parameters and sequence selection. Since the proton
density is dominated by the contributions from water and fat, the signal is:
(6.1)
97
The coil sensitivity factor is difficult to determine in practice. However, k and R are not
critical if the goal is to separate the signal into relative water and fat components. The
spectrum near the water resonance is shown in Figure 6.3. Knowing these spectra, water
and fat can be determined by solving a linear system for the relative signal Srel:
(6.2)
where ε is the known spectrum of water and lipids, and the summation is computed over
the range of frequencies, f, excited by the RF excitation pulse. Since the MR coil detects
a range of frequencies simultaneously, water and fat are separated in MRI by measuring
the changes in signal due to the different phase of protons in water and fat over time.
Using this technique, the relative percentages of water and fat can be determined.
H 2O
Lipid
Figure 6.3: Comparison of the spectral dependency of MR and NIR optics on water
and fat. Because the signal contributions from water and fat can be isolated,
98
percent water and fat calculated by MR will in principle be the same percentages
determined by optics (Optical spectrum obtained from van Veen et al.139).
In optical imaging, light absorption of a certain wavelength in the NIR from a
voxel of tissue is due to the concentration of water, lipids, and hemoglobin.
(6.3)
If hemoglobin and scatter are accurately accounted for, the remaining signal absorption is
due to either water or lipids. Thus, a relative percentage of water and lipids may be
determined. These spectra are shown in Figure 6.3139.
Merritt et al.140, 141 investigated the correlation between water and fat measured
optically with their broadband handheld scanner, and measured by MR with a 3-point
Dixon sequence. In water and soybean oil emulsion phantoms, they found an R2
agreement of 0.97 in water, and 0.99 in lipid. The difference in water between the
modalities was highest, 5% and 8%, when water percentages were 10% and 100%,
respectively. MR measured lipids showed better correlation to the true fat fraction than
did optical measures, as lipid was always 9% higher than the MR measured lipid.
Since the phantom was constructed of lipid (soybean oil) and water, it was made
of the identical water and lipid chemical species that are found in the human body. These
spectra are expected to be indistinguishable in tissue. However, there are slight changes
in these spectra due to the tissue environment. In the NIR spectrum, the absorption of
bound water142 is shifted ~5 nanometers at 930nm, although this effect is much smaller
below 849nm143. Thus, this shift is insignificant in the sensitivity region of the
99
photodetectors used in this study. The NMR spectra of bound water broaden in tissue,
but do not shift.
6.4 Methods to Incorporate MR water and fat into image reconstruction
MR quantitative water/fat separation is incorporated into the optical reconstruction by
two methods: the direct substitution method, and the joint weighted estimation method.
For both cases, the problem is reformulated in terms of the tissue contents71, 72. This
approach not only acts as a noise filter72, but also allows control over the tissue contents
µ, through Wµ100, if desired. The following results show that the optimal method depends
on knowledge of the accuracy of the MR technique.
For both methods, MR quantitative information can be used in the initial guess.
This initial guess is usually computed from the optical calibration routine144. With the
added information from MR water/fat separation, MR water can be used as the initial
guess for the optical estimation. An example of an all-optical initial guess from a
volunteer is shown in Figure 6.4a, whereas the initial guess including the MR water
image is shown in Figure 6.4b.
a
b
100
Figure 6.4: The initial guess determined by (a) optics, and (b) optics including the
MR water image.
6.4.1 Direct substitution of water and fat
As introduced previously, images are formed by jointly minimizing differences between a
light propagation model and measurements, and non-physical variations in tissue
contents. The objective function:
(6.4)
contains oxyhemoglobin, deoxyhemoglobin, water, scatter amplitude, and scatter power
represented by the vector µ, the initial guess of these contents, µprior, the misfit between
the photon propagation model and the measurements, δ, and the weighting functions on
the data and chromophore concentrations, Wd and Wµ, respectively. In this formulation,
Wµ is not chosen statistically, but is instead chosen to normalize the magnitude of the
different chromophores for the inversion145.
If we assume that the MR water and fat information is perfectly accurate, we can
substitute the value of MR water directly into the objective function, so that µ is:
(6.5)
for all voxels 1 to N.
101
The water is fixed throughout the reconstruction, since it is assumed to be the true
value. Thus, the water contribution to the Jacobian is removed. In general, the spectral
Jacobian is:
(6.6)
where I and θ are the measurements, and NN is the number of unknowns (e.g. nodes in a
finite element mesh). In the direct substitution method, the Jacobian is modified to:
(6.7)
Its dimensions are reduced by Number of Measurements x Number of Unknowns. The
parameter update function is:
(6.8)
This formulation has several advantages. First and foremost, the water is the true value.
By inputting the correct water percentage, the oxyhemoglobin estimation will improve
102
because of reduced crosstalk to water. Additionally, the inversion is more stable because
of the reduction in the number of unknowns.
6.4.2 Joint weighted estimation of water and fat
A concern with the direct substitution method is in the assumption that the MR
quantitative information is considered perfect. Even in MR sequences that are
quantitatively accurate in phantoms, effects from T1 relaxation and spectral deviations
from the model will lead to inaccuracies. These errors in MR estimation will corrupt not
only the MR measured water, but also other parameters because of crosstalk in the optical
absorption spectrum. The joint weighted estimation method estimates tissue properties
using both optical and MR information jointly. Since both datasets are available, bias in
water estimation in one modality will have a smaller effect on parameter recovery. In
contrast to the direct substitution approach, this method uses the spectral Jacobian of
equation 6.6. The update to the properties is:
(6.9)
In this method the weighting function can be adjusted to control the expected contrast of
not only the hemodynamic content in the tissue35, but also the MR water and fat, as
proposed by Li et al.125. Here, we add the scatter contrast. These quantities are
incorporated into the parameter weighting function:
103
(6.10)
where Wµ contains the variance, or contrast bound, of each of the parameters on the
diagonal, and the covariance, or spatial interdependence of the parameters on the offdiagonal. The water weighting function, WWater , incorporates the known accuracy of
MR
the MR water quantification measurement:
(6.11)
This formulation allows a joint determination of water, and therefore maintains the
dimensions of the Jacobian. Solving equation 6.4 yields the update to the optical
properties, found by homogeneous fitting of the bulk tissue144:
(6.12)
where µprior reinforces the initial guess of oxyhemoglobin, deoxyhemoglobin, scatter
amplitude, scatter power provided from optical fitting, and water provided from the MR.
104
6.5 Comparison of MR water-guided reconstructions
The performance of these algorithms under different conditions is presented in a
simulation study below. The goal of the study was to determine the amount of crosstalk
between water and oxyhemoglobin produced by algorithms that either ignore or include
MR water. Specifically, this study investigated the error in oxyhemoglobin
quantification due to different experimental conditions and wavelength sets.
First, the direct substitution method will be used to show improvement in
oxyhemoglobin estimation over non-MR water guidance. Second, the limitations of this
algorithm will be examined by considering error in MR water quantification. The direct
substitution method is expected to yield erroneous results with improper MR water
estimation. Lastly, the advantage of using the joint weighted estimation method to
improve both oxyhemoglobin and water estimation with increasing error in MR water
quantification will be presented.
A test problem created from a patient is shown in Figure 6.5. A 1921 node finite
element mesh was created from a breast MR scan, segmented, and used to generate noisy
data (5% Gaussian noise in amplitude, 5 degrees Gaussian noise in phase). The inclusion
was a 5mm diameter tumor embedded in the fibroglandular region. The diameter of the
domain was ~90mm. The contrast added to the breast was typical of recovered breast
properties89, 90, and is shown in Table 6.1.
105
Figure 6.5: Test problem used in this simulation study. Total hemoglobin in the
tumor was set at 0.04 mM, a 2:1 contrast over the background fibroglandular tissue.
Oxygen saturation was 50% in the tumor, and 70% in the background. Data with
5% white noise in AC amplitude and 5 degrees white noise in phase was generated
from this geometry.
Tissue Type
HbO (mM)
Hb (mM)
Water (%)
Sc-A
Sc-P
Adipose
0.007
0.003
10
1
1
Fibroglandular
0.014
0.006
50
1
1
Tumor
0.020
0.020
90
1
1
Table 6.1: Tissue properties used in water/fat simulation study.
A reconstruction mesh of 1983 nodes was used to reconstruct tissue properties.
Reconstructions were performed with ensembles of 3, 4, and 5 wavelengths typically
used in optical tomography24, 32 (chosen from 661nm, 761nm, 785nm, 808nm, 826nm,
849nm). The error is reported as the percent error from the truth; a perfect
oxyhemoglobin recovery yields 0% error. Results for 3,4, and 5 wavelengths are the
averaged oxyhemoglobin error over the ensemble of wavelength sets.
106
6.5.1 Influence of MR Water/Fat Separation constraint on crosstalk
Two reconstruction algorithms, one excluding and one including MR water priors via the
direct substitution method, were compared for error in oxyhemoglobin. Because of the
spectral similarities between oxyhemoglobin and water, it is expected that a decreased
number of wavelengths will lead to poorer quantification of water, and thus crosstalk to
oxyhemoglobin. Without MR water, Figure 6.6 shows that errors in oxyhemoglobin
decrease with increasing numbers of wavelengths, from 17% with 3 wavelengths, to 7%
with 5 wavelengths. This behavior is expected since fewer wavelengths do not
adequately sample the optical spectra, and oxyhemoglobin contrast crosstalks into water.
Using the direct method with a mere 3 wavelengths gave superior oxyhemoglobin
quantification, within 3%. Since water is fixed to the correct value, contrast for
oxyhemoglobin will not influence the water estimation. Therefore, optical contrast in
oxyhemoglobin will influence only the estimate of oxyhemoglobin, thus providing
greater accuracy. If water is known perfectly through MR, superior quantification is
achieved.
107
Figure 6.6: Error in HbO decreases with additional wavelengths because of the
improved spectral sampling, which in turn leads to more accurate separation
between water and oxyhemoglobin. Comparatively, the direct substitution method
gives superior quantification, even with 3 wavelengths.
However, MR water quantification is not expected to be perfect, and imperfect
water estimation, if constrained, will lead to errors in oxyhemoglobin. These errors will
eventually lead to poorer estimation than excluding the water priors. Figure 6.7 displays
errors in oxyhemoglobin as a function of errors in MR water quantification, with a 3wavelength direct substitution reconstruction. The 3-wavelength set was used to simulate
a worst-case scenario for optical quantification of oxyhemoglobin, deoxyhemoglobin,
and water. These results suggest that if MR water quantification is worse than ~6%, HbO
quantification will be worse than excluding the MR water/fat prior altogether. Thus,
based on this simulation study, cases where MR water quantification has error greater
than 6%, the joint weighted estimate method of including MR water quantification may
be a better option.
108
Figure 6.7: Error in HbO with 3 wavelengths increases as MR water quantification
error increases. The comparative case of excluding MR water priors is shown at the
far right.
6.5.2 Influence of MR Water/Fat error on the Joint Weighted Estimation
reconstruction
MR water quantification can be included statistically into the optical reconstruction, as
long as the variance in the measurement of the water content can be determined. Figure
6.8 compares reconstruction results using both water quantification reconstructions, and
the standard reconstruction. This simulation investigated the effects of 10% water
quantification error in the a priori MR water estimate. This error is typical137 with MR
sequences which perform poorly in separating water and fat, such as chemical shift fat
suppression. This result shows that HbO recovery can be improved by 10.5% with the
joint weighted estimation method instead of the direct substitution method.
Figure 6.8: Error in HbO when MR quantification is incorrect by 10%. The
percent error is the average error of 5 ensembles of 3 wavelengths in the wavelength
range used by the system in this thesis.
109
The joint weighted estimation approach can also improve the estimation of water,
since both optical and MR measures are used to estimate tissue properties. Figure 6.9
shows the errors in water quantification when MR water is constrained vs. when MR
water is included statistically. In this case, MR water quantification error was adjusted
from 2.5% to 10%. At all levels of error, the joint weighted estimation approach yields
superior water quantification.
Figure 6.9: Comparison of recovered errors in water quantification between the
direct substitution approach vs. the joint weighted estimation approach. By
extrapolation, these errors will be equivalent at ~1% estimation error.
By including MR water quantification in a joint weighted sense, error in recovered water
is reduced by 5% while the MR error is 10%.
110
6.6 Experimental validation in a breast tissue simulating phantom
6.6.1 Properties of the tissue simulating phantom
A gelatin tissue-simulating phantom was used to test the methodology of including MR
water/fat priors. This phantom was made following techniques described elsewhere45, 146,
147
. The optical properties of this phantom are shown in Table 6.2. An inclusion with 2:1
contrast in total hemoglobin was mixed in a similar concentration of gelatin solution, and
poured into a 24mm diameter cylindrical hole in the hardened phantom. This phantom
was then cooled and allowed to solidify for several hours.
HbT (mM)
O2 Sat (%)
Water (%)
Sc-A
Sc-P
Background
0.015
100
90
UK
UK
ROI
0.03
100
90
UK
UK
Table 6.2: Phantom true concentrations in the background and region of interest
(ROI). The concentration of HbT was measured with a hemoglobin analyzer, and
water was measured with methods described below. The scatter amplitude and
scatter power were homogeneous, but unknown (UK).
6.6.2 Methods to measure gelatin water concentration
To determine the water content in the gelatin (G2625, Sigma), measurements were
performed using both a UV-VIS-NIR spectrophotometer (Varian) and an MR water/fat
separation gradient echo DIXON technique (Philips).
Optical absorbance data was collected by placing water and prepared gelatin into
cuvettes and measuring their spectra with a spectrophotometer. These spectra were
111
calibrated with a blank cuvette. The spectral absorbance for water and a gelatin phantom
are shown in Figure 6.10a.
a
b
0%
25%
gel
100%
75%
50%
Figure 6.10: Methods used to compute percent water in gelatin consisted of (a) NIR
spectrophotometry, and (b) DIXON MR. In both cases, pure water was used as a
reference to determine the water content of the gelatin.
A power law fit was performed on the gelatin data to remove the offset due to scatter
signal from the gelatin, which was more prominent at shorter wavelengths. Using pure
water as a reference, the gelatin had 87% water.
To measure the water content in gelatin with MR, DIXON images (TR =
500msec, TE = 2.3/3.5/4.6msec) of phantoms containing varying amounts of water and
soybean oil were acquired. These phantoms were blended together by adding 1% Tween
(Sigma) and mixing on the blender’s high setting for ~3 min. The well-mixed phantoms
had a milky consistency. These phantoms were poured into a cylindrical mold to form 6
phantoms: 0%, 25%, 50%, 75%, 100% water, and 1 gelatin. The signals from the
resulting water images were normalized to the signal of the phantom containing100%
112
water. Using this method, it was determined that the gelatin phantom had a water
concentration of 90 +/- 2%.
6.6.3 Results
Calibrated data from 6 wavelengths (661, 761, 785, 808, 826, 849nm) was reconstructed
with the direct substitution approach, since water was known exactly. These results were
compared to the standard reconstruction without water priors. Three reconstructions used
3 wavelengths of data (one with 661, 761, and 785nm, one with 661, 785, and 826nm,
and one with 661, 785, and 849nm) and one used the full 6 wavelength dataset. Example
image sets are shown in Figure 6.11 and Figure 6.12. Absolute percent errors are shown
in Figure 6.13
When the MR water/fat image is used, errors in total hemoglobin decrease
compared to the non MR water/fat technique, especially when using a 3-wavelength set.
In one case, the 661, 785, and 849nm wavelength set, total hemoglobin is severely
underestimated. This can most likely be attributed to noise in the 849nm dataset, which
poorly estimates water. This data is noisier because of the insensitivity in the PMTs to
this wavelength. These reconstruction results show that utilizing the MR water
information yields a more accurate and consistent (N=4, p<0.001, chi-square test)
estimation of total hemoglobin, which is more insensitive to wavelength specific data
noise.
113
a
b
c
Figure 6.11: Comparison of reconstructions of 3 wavelengths of 661, 785, and
826nm with and without water priors. (a) Target true values, (b) spatially guided
reconstruction, and (c) spatially and quantitatively guided reconstruction using the
direct substitution reconstruction.
a
b
c
114
Figure 6.12: Comparison of reconstructions of 6 wavelengths of 661, 761, 785, 808,
826, and 849nm with and without water priors. (a) Target true values, (b) spatially
guided reconstruction, and (c) spatially and quantitatively guided reconstruction
using the direct substitution reconstruction.
Figure 6.13: Absolute percent errors in total hemoglobin (HbT) for the spatially
guided vs direct substitution reconstructions, for different sets of wavelengths.
6.7 In vivo results in the human breast
A 47 year old woman with an invasive ductal carcinoma of the left breast was imaged 12
days post-biopsy. MR images were taken in the coronal plane, including a gradient echo
T2-weighted sequence (Figure 6.14b) and a spoiled gradient echo IDEAL water/fat
sequence. Anatomical boundaries of the fibroglandular tissue and suspect lesion were
manually segmented under supervision of the radiologist (B.D.). Gadolinium images
were collected 11 days prior to the imaging session according to the clinical breast
115
protocol at Stanford University Medical Center (Figure 6.14a). IDEAL water/fat
separation images in the plane of the optical fibers are shown in Figure 6.15.
b
a
Figure 6.14: (a) T1-W Gadolinium MR image of the affected breast (b) T2 weighted
image in the coronal plane of the optical fibers. Tumors are identified with the red
arrows.
a
b
c
d
116
Figure 6.15: Images of water (a) and lipid (b) IDEAL MR images. Quantitative (c)
water and (d) lipid images overlaid onto the 2D FEM mesh.
The optical image results are shown in Figure 6.16. Without MR water priors, the
tumor hemoglobin was 0.035 mM compared to 0.026 mM in the fibroglandular and 0.016
mM in the adipose tissue. Without quantitative MR water, the fibroglandular water
content is underestimated, which leads to an overestimation in total hemoglobin in the
fibroglandular tissue because of crosstalk. Thus, the tumor to fibroglandular contrast is
reduced. Oxygen saturation was highest in the tumor at 70%, slightly above the
background tissue around 60%.
By including MR water values via the direct substitution method, total
hemoglobin was estimated to be 0.039 mM in the tumor, and 0.019 mM and 0.015 mM in
the fibroglandular and adipose tissues, respectively. Because the direct method more
accurately estimates water at 60%, oxyhemoglobin estimates are lower, which results in
more hemoglobin contrast between the fibroglandular tissue and the tumor tissue. The
effect of including MR water priors via this method increased tumor to fibroglandular
contrast by ~42%, to ~103%.
The joint estimation method was implemented using the MR water quantification
error reported by Bernard el al137. The joint weighted estimation approach led to total
hemoglobin recovery of 0.031 mM, while fibroglandular and adipose were 0.018 mM
and 0.017 mM, respectively. This led to an increase in contrast compared to excluding
water priors of ~7%. The decrease in contrast in total hemoglobin of the JWE method vs
the direct method could likely be attributed to the decrease in water in the fibroglandular
117
tissue by ~5%, from 60.2% to 54.9%, and no significant change in water content in the
tumor tissue.
a
b
c
Figure 6.16: (a) In vivo image reconstructions of a diseased breast without MR
spectral priors compared to (b,c) methods that use MR water/fat priors. (b) Image
118
reconstruction using the direct substitution gives the highest tumor to background
contrast. (c) Image reconstruction using the joint weighted estimation approach
yields higher contrast than ignoring water quantitative priors, but less contrast than
the direct substitution method.
6.8 Conclusions
This section shows that including MR water/fat separation can yield superior
chromophore recovery when limited wavelengths are used in MR guided near infrared
spectroscopy. In a tissue-simulating phantom, including the MR water prior in the image
reconstruction yielded hemoglobin quantification improvements of greater than 25%
when imaging with 3 wavelengths. In one case, the improvement was well over 200%.
This improvement is due to the decrease in crosstalk between oxyhemoglobin and water
content. The MR water prior also yielded more consistent reconstruction results in
phantom imaging, as the variance of the recovered hemoglobin was significantly lower
than the recovered values without the water prior (N=4, p < 0.001, chi-square test).
These results also demonstrate that if MR water/fat separation is imperfect, water
errors will crosstalk to oxyhemoglobin. By incorporating the known variance of the MR
sequence (here varied between 2.5% and 10%), a statistical algorithm recovered tissue
properties with less error. In a case where there was a 10% error in the MR water prior,
the direct substitution method recovered less accurate values than when the MR water
prior was ignored. However, including the water prior jointly yielded a 5% improvement
over ignoring the MR water, and a 10% improvement over including the water directly.
119
Thus, in cases where the water/fat separation is expected to be poor, such as with
chemical shift water suppression methods, the joint weighted estimation method should
be used.
A confounding factor in the comparison of the direct method and the joint
weighted estimation method is the influence of the number of unknowns. Although the
direct method may yield slight errors due to imperfect MR water estimation, it reduces
the number of unknowns, leading to a less under-determined inverse problem. The best
approach ultimately will depend on the signal to noise of the detectors across the
wavelength spectrum, the wavelengths used, and the accuracy of the MR water/fat prior.
120
Chapter Seven: Monitoring changes in breast physiology due to
respiratory challenge
7.1 Introduction
This chapter describes a technique to image blood content and oxygenation changes
during gas breathing. The study goal was to identify a protocol which would induce
significant changes in breast physiology. This work demonstrates that a gas stimulus of
oxygen followed by carbogen induces changes that are significantly greater than the
underlying physiological variations. In contrast, air/carbogen and air/oxygen do not
significantly alter breast tissue response consistently. Three cases involving breast
tumors are presented, and the differences in vascular function between the tumors and the
normal background tissue are examined in two of these subjects. The next chapter
compares the optical and BOLD MRI contrasts in the breast.
7.2 Tumor contrast identified by respiratory challenge
The development of new vasculature begins with the formation of endothelial cells. In
healthy tissue, smooth muscle cells are recruited to these endothelial cells to form a
durable, functioning neo-vascular network148. In tumor vasculature, the recruitment of
smooth muscle cells is compromised, as a disproportionate amount of growth factors
VEGF and Ang- 1 and 2 leads to the formation of highly permeable, immature vessels149.
This dysfunctional vasculature, also characterized by high vessel density and high
metabolic activity, leads to blood flow, blood volume, and oxygenation levels which vary
considerably from normal tissue11.
121
Because of the lack of proper functionality of tumor vasculature, tumors are
expected to respond differently to changes in the local environment than normal tissue.
Tumor characteristics, such as vasoconstriction of feeding vasculature150, and anemia in
tumor vessels151, may result in poor oxygen delivery to the tumor during oxygen
respiratory stimulus. This is critical in therapy, where increased oxygenation has been
shown to improve in radiotherapy152-155, hyperthermia156, and photodynamic157 therapy.
Tumor physiology which prevents an increase in tissue oxygenation from gas breathing
will affect certain therapy outcomes158. Thus, determining induced vascular changes due
to respiratory stimulus may indicate subjects that will respond more successfully to
therapy.
In addition to predicting radiation response, the vascular response to gas stimulus
may be used to characterize tumor vascular maturity. In turn, this may predict response
to anti-angiogenic therapies159, and provide knowledge of tumor function.
7.3 Modulating tissue hemodynamics with gas stimulus in healthy tissue
Hemodynamics and tissue oxygenation are actively controlled during metabolism.
During times of increased oxygen consumption, such as during exercise, CO2
concentration increases because it is a by-product of oxidative metabolism. Its presence,
along with other metabolites, causes a dilation in the vascular system. This dilation
decreases vascular resistance which increases blood flow to the tissue160, 161. These
changes are controlled by the smooth muscle cells lining the endothelial cells in the
vasculature162.
An alternative means to induce changes in vascular function is to alter the
chemical environment by introducing oxygen or carbon dioxide in the blood through gas
122
breathing. Specifically, gases containing 100% oxygen, or carbogen, a 95% O2:5% CO2
mixture, have been extensively studied to control vascular function and investigate their
effects on tissue oxygenation, blood flow, and vascular resistance.
Breathing 100% oxygen has been shown to increase tissue oxygenation due to the
increased pO2 of the blood163 compared to air breathing. An increase in pO2 causes the
loading of oxygen onto hemoglobin in a proportion dictated by the oxygen dissociation
curve164. At the same time, increased blood oxygenation causes the smooth muscle cells
lining the vasculature to contract, due to the lack of carbon dioxide in the blood161. In
turn, this causes an increase in vascular resistance and blood pressure, and a decrease in
blood flow, due to increased vascular constriction in the peripheral vascular bed165, 166.
The decrease in blood flow may lead to hyperoxia-induced hypercapnia, which may then
reduce oxygen content166. Although tissue oxygenation is increased compared to air
breathing, these conflicting factors may limit the delivery of oxygen to tissue, especially
compared to carbogen breathing167.
Carbogen has been shown to increase both tissue oxygenation and tissue blood
flow. Because of the introduction of CO2, dilatory effects can offset the vasoconstrictive
effects that occur in 100% oxygen breathing. In particular, carbogen with CO2 fractions
above 1% have produced significantly higher blood flow and decreased vascular
resistance than 100% oxygen163, 168. In addition, carbogen has been shown to induce
elevated levels of pO2. These increases have been shown in the cerebrum168, liver,
spleen, paraspinal muscle, subcutaneous fat169, and head and neck tumors154. Tumor pO2
levels were observed to be slightly lower than those resulting from pure oxygen
123
breathing163. No significant change in the metabolic rate of O2 has been found with the
administration of carbogen in these tissues168, 170.
This study analyzed the tissue hemodynamic response in the breast due to three
gas stimuli: Air/Carbogen, Air/Oxygen, and Oxygen/Carbogen. It was expected that a
switch from air to oxygen would result in decreased blood flow, and decreased tissue
oxygenation. A switch from air to carbogen would increase blood flow, due to the
presence of CO2. Tissue oxygenation might be expected to increase because of the
increased oxygen levels in carbogen compared to air167. However, CO2 in the blood will
cause a rightward shift in the oxygen dissociation curve, which may decrease oxygen
saturation. Periodically breathing oxygen and switching to carbogen causes an increase
in blood flow which increases oxygen saturation and total hemoglobin. Offsetting this
change is the relative decrease in pO2 and increase in pCO2, which acts to decrease
oxygen saturation. These effects are summarized in Table 7.1. This study investigated
the relative strength of these competing factors.
Oxygen
Carbogen
Cause
HbT
-
+
Vasomotor
O2 Sat
-
+
Vasomotor
HbT
N/A
N/A
pO2
O2 Sat
Small +
Small -
pO2
HbT
N/A
N/A
pCO2
O2 Sat
+
-
pCO2
124
Air
Carbogen
Cause
HbT
-
+
Vasomotor
O2 Sat
-
+
Vasomotor
HbT
N/A
N/A
pO2
O2 Sat
-
+
pO2
HbT
N/A
N/A
pCO2
O2 Sat
+
-
pCO2
Air
Oxygen
Cause
HbT
+
-
Vasomotor
O2 Sat
+
-
Vasomotor
HbT
N/A
N/A
pO2
O2 Sat
-
+
pO2
Table 7.1: Expected changes in total hemoglobin (HbT) and oxygen saturation (O2
Sat) due to physiological changes accompanying a switch between gasses in each
stimulus used in this study. A (+) indicates that the administration of the gas
125
(shown in the columns) will cause a relative increase in the parameter (shown on the
leftmost column of each row). A (-) indicates a relative decrease.
7.4 Methods
7.4.1 Gas Breathing
This study investigated three different gas compositions. For oxygen and carbogen
breathing stimuli, medical gases (Praxair) were fed from the gas tanks to a respiratory
circuit, shown in Figure 7.1, which controlled the source of inhaled gas. As shown in
Figure 7.1, when valve 1 from the gas tanks was opened, positive pressure from the
feeding gas line would close valve 2, preventing the breathing of room air. During air
stimulus, valve 1 from the gas tanks would close. The lack of air pressure from the gas
tanks would open valve 2, allowing the breathing of room air. Thus, respiratory gases
could be controlled.
Flow rates coming from the gas tanks were kept at 9 liters/min and were
monitored by flowmeters attached to the tanks. A gas line was attached to the mask just
below the mouthpiece which led to a oxycapnograph (capnomac ultima, © Datex), which
monitored CO2, O2, and respiratory rate. These metrics were then recorded by a
computer running tracerdaqpro (© Measurement Computing) software. A customized
computer controlled valve, shown in Figure 7.2b, was used to switch between oxygen and
carbogen gas. All subjects had their noses sealed to ensure breathing only through the
mouthpiece.
126
a
1
b
2
1
2
c
Figure 7.1: (a) Photograph of the gas breathing circuit. (b) Diagram of circuit
operation during oxygen or carbogen breathing. During oxygen or carbogen
stimulus, pressure from gas input 1 would close valve 2, preventing room air from
entering the circuit. All valves were one-way, so that the expired gas would not be
re-breathed. (c) Diagram of circuit operation during air breathing. During air
stimulus, the lack of pressure from the gas input 1 would open valve 2, allowing
127
room air to be drawn through the circuit. A small tube led from near the
mouthpiece to an oxycapnometer to monitor expired gas concentrations.
a
b
c
Figure 7.2: Inspired (a) Carbogen and oxygen gases were controlled with a (b)
custom computer-controlled valve. This valve was synchronized via software to the
desired modulation rate. (c) A diagram shows the gas inputs leading to the output
valve, which fed into a breathing circuit located in the MR room.
7.4.2 Gas stimulus
We chose a breathing stimulus period of four minutes (1/240 = 0.041 Hz), two minutes
per gas, for a total of four cycles. Gas stimuli combinations are shown in Figure 7.3. In
this text, a gas stimulus of CO2 indicates carbogen stimulus. A timing diagram is also
128
shown in Figure 7.3. Expired gas concentration was monitored during respiratory
challenge to ensure subject compliance. Each subsequent stimulus was started within 1
minute of the conclusion of the previous stimulus.
All imaging participants provided informed consent, and procedures were
performed according to the protocol approved by the Institutional Review Board of the
Stanford University Medical Center.
a
b
c
Figure 7.3: Gas time series for the stimuli combinations in Table 7.2. (a) Timing
diagram indicating duration of gas stimulus. (b) The true timing of each gas, shown
in blue, was approximated by a sine wave, shown in red, for data processing. The
shading indicates which gas is active. (c) Changes in CO2 concentration in a
129
compliant subject. Note the three periods of increased CO2 corresponding to the
three periods of the stimulus used in the data processing.
Gas 1
Gas2
Stimulus 1
CO2
O2
Number of
Subjects
2
Stimulus 2
O2
CO2
11
Stimulus 3
Air
CO2
5
Stimulus 4
Air
O2
7
Table 7.2: Listing of the different gases used for this study and the number of
volunteers monitored for each stimulus.
7.4.3 Data acquisition
Optical data was collected with the MR-NIR instrument described in this thesis. To
improve temporal performance, the dynamic source was used (described in Chapter 2),
which imaged three wavelengths (661, 785, 826nm) simultaneously. This provided a
temporal resolution of 30 seconds per image. Optical and BOLD MR data were collected
concurrently. Data collection was synchronized to begin within 1 second of the start of
the gas stimulus. The measurement stability of the system is shown in Figure 7.4. It
demonstrates adequate stability for dynamic measurements.
130
-- HbO
-- Hb
Figure 7.4: Instrumentation fluctuations in a tissue-simulating phantom. Standard
deviation in fitted total hemoglobin is 0.19% of the amplitude, and standard
deviation in fitted oxygen saturation is 0.22 % of the amplitude.
7.4.4 Data Processing
Each timepoint used in the data analysis consisted of one image guided reconstruction.
Measurements of amplitude and phase were calibrated on the data from the first image
acquired in each stimulus set, thus providing a robust calibration free from fiber coupling
noise. Data below the system noise floor (defined in chapter 2) was dropped. A full
temporal dataset consisted of 23 timepoints.
All correlations were performed on either healthy fibroglandular tissue or tumor
tissue. Tumors were identified by DCE-MR and segmented with the aid of a radiologist
(B.D.). Gas modulation was modeled with a sine wave at the stimulus frequency, shown
131
in Figure 7.3b. This approximation is valid since the body acts as a temporal low pass
filter. Tissue response was modeled with the cross correlation function. This provided
measures of the strength of correlation, and the time lag between gas stimulus and tissue
response.
Specifically, the temporal de-meaned cross covariance between the modeled gas
stimulus and the measured hemodynamic changes in the breast was used to determine
correlations and time lags. The measure of cross covariance compares two signals, S1
and S2. In this case, S1 and S2 are the stimulus and the tissue response, respectively. The
cross covariance is defined as:
(7.1)
These signals (with means
and
removed) are compared while S1 is temporally
shifted by a time lag t. S1 and the complex conjugate of S2 are multiplied together over
both periods, 2T. The resulting vector is then summed to compute a correlation at a
specific time lag, t. Examples of the cross covariance of simulated signals S1 and S2 at
zero time lag with different amounts of Gaussian noise are shown in Figure 7.5.
This measure calculates correlations at each time lag. The time lag at maximum
correlation represents the lag in time between the stimulus and the tissue response. Since
the stimulus is a modulation of gases, the time lag indicates the tissue response to a
specific gas. These time lags are calculated for total hemoglobin and oxygen saturation
for each subject.
132
a
b
c
Figure 7.5: Simulated cross covariance calculations for two signals, signal S1 (blue)
and signal S2 (red), having different amounts of Gaussian noise. (a) No noise (b)
25% of S2 signal amplitude noise (c) 100% of S2 signal amplitude noise. These
examples show the effects of noise on correlation at zero time lag.
7.5 Results in the healthy breast
Temporal responses in the breast tissue were recorded during gas stimuli and during air
breathing only. Results using air breathing alone provided a control study to determine
background physiological noise. The temporal total hemoglobin and oxygen saturation
responses of a healthy subject breathing the O2/CO2 stimulus are shown in Figure
7.6.(a,c). Compared to the control measurement of all room air breathing (Figure 7.6b,d),
133
this data demonstrates that in this subject, the tissue response is greater than the
background physiological response. This is most apparent in the amplitude of the Fourier
spectra at the stimulus frequency, shown in the right-hand column of Figure 7.6. The gas
stimulus is not always greater than the background physiology. The comparison of the
relative strength of the response compared to the control will be addressed in a later
section.
a
b
c
134
d
e
Figure 7.6: Temporal and frequency response of hemodynamics to O2/CO2 gas
stimulus compared to an air control. In (a,c), white bars indicate O2 stimulus, and
gray bars indicate carbogen. For (b,d), both white bars and gray bars indicate air.
(a) Total hemoglobin oscillations during O2/CO2 stimulus show a significantly larger
peak at 0.041Hz than the air control, (b) indicating the tissue response to the
stimulus was larger than the physiological noise. (c) Oscillations of oxygen
saturation during gas stimulus also shows a larger frequency peak at 0.041Hz than
the air control, (d), indicating a larger response than the physiological noise.
135
7.5.1 Time lag response in healthy breast tissue
Time lag responses for all healthy subjects are shown in Figure 7.7. This data is plotted
in terms of phase lag; a phase lag of 0 indicates a positive response to Gas 1, whereas a
phase lag of π indicates a positive response to Gas 2. These datasets exclude cases where
the tissue response was less than the air control. This topic will be investigated in more
detail in Section 7.5.2. These data show that the response in the breast is subjectdependent for both total hemoglobin and oxygen saturation, which is most likely due to
differences between the physiology of each subject, as differences in cardiac and vascular
health cause differences in blood gas delivery and exchange171.
However, this data does show a consistent total hemoglobin phase lag of π to 2π
for the O2/CO2 gas stimulus. These results may be explained by the vascular motor
function. As carbogen is breathed, total hemoglobin is expected to increase, while it is
expected to decrease with oxygen. This could indicate a strong response due to the
opposing vascular effects of carbogen and oxygen.
On the other hand, the air/O2 and air/CO2 stimuli do not show consistent trends in
time lag. This may be due to the relatively weak stimuli, which do not induce sufficiently
strong responses. In these cases, the body may be able to maintain homeostasis for a
longer period of time before the response to the gas occurs. Comparing the time lags of
the interplay between total hemoglobin and oxygen saturation, however, yields more
insight into the physiological changes.
136
a
b
c
Figure 7.7: Phase lags between the start of the gas stimulus and the total hemoglobin
(HbT) and oxygen saturation (O2 Sat) response at maximum correlation for (a)
O2/CO2 (N=8), (b) Air/CO2 (N=4), and (c) Air/O2 (N=3). Note that although the time
137
lag for the response is volunteer dependent, the O2/CO2 stimulus generally has a π to
2π phase delay, meaning that the total hemoglobin increases during carbogen
breathing. This agrees with the expected vasodilatory response caused by CO2. In
contrast, the total hemoglobin has a 0 to pi phase delay during the Air/O2 stimulus,
meaning that vasodilation occurs during air breathing, and vasoconstriction occurs
during oxygen breathing.
The difference between time lag of total hemoglobin and oxygen saturation,
shown in Figure 7.8, indicates a significant correlation between total hemoglobin and
oxygen saturation for O2/CO2 (R2 = 0.825, p = 0.0018, N=8) and Air/CO2 (R2 = 0.923, p
= 0.0039, N=4). This data is consistent with the theory that carbogen induces an increase
in blood flow. During carbogen stimulus, the vasodilation brings freshly oxygenated
arterial blood (~98-100% oxygenated) into the tissue, washing out deoxygenated blood
from the vasculature, and increasing oxygen saturation. Thus, total hemoglobin and
oxygenation are expected to vary together. In the air/O2 stimulus, oxygen saturation
changes may be independent of total hemoglobin changes (as the variation in HbT is not
explained by the variation on oxygen saturation, p = 0.82, N=3). Thus, other factors
besides vasomotor control contribute substantially to the regulation of the hemodynamic
response during the air/O2 stimulus. As presented above in Table 7.1, these changes are
most likely due changes in pO2, which induce changes in the loading and unloading of
oxygen onto hemoglobin. Without a pO2 probe, this effect can not be explained with
confidence.
138
Figure 7.8: Time lag comparison of oxygen saturation vs total hemoglobin for the
three gas stimuli. In stimuli with carbogen, vasodilation allows highly oxygenated
blood to enter the breast tissue, which washes out deoxygenated hemoglobin, and
increases oxygen saturation. Oxygen saturation and total hemoglobin during Air/O2
stimulus is not dominated by changes in vascular tone. Instead, these changes could
also be due to pO2 induced oxygenation changes.
7.5.2 Noise Considerations
An important confounding factor in determining the effect of a stimulus on tissue
hemodynamics is the body’s low frequency fluctuations at steady state. These
fluctuations were often found to have stronger amplitude than the tissue response to the
stimulus. Without proper measurements of the oscillations of tissue during air breathing,
139
changes in hemodynamics could be mistakenly attributed to the gas stimuli. Indeed,
significant oscillations in blood flow and blood pressure exist between 0 Hz to 0.5Hz172.
The frequency used in this study, 0.041 Hz, coincides with the “very-low” frequency
range observed in spectral analyses of hemodynamics, possibly arising from fluctuations
in tissue metabolism173. In order to consider the effects of physiological noise, a signal to
noise (SNR) measure was calculated for total hemoglobin and oxygen saturation, which
compared the relative magnitude of the maximum correlations between gas stimulus and
air control breathing. SNR was calculated as:
(7.2)
An SNR < 1 indicated that the gas did not induce a meaningful change in breast
physiology.
Results of SNR for all stimuli are shown in Figure 7.9. These results show that
many cases had SNR < 1. Of the three stimuli, O2/CO2 induced a response in oxygen
saturation which was significantly stronger than the control (p = 0.02, two-sample t-test,
N=11). The response in total hemoglobin strongly suggested a greater correlation than
the control, although this claim is not significant (p = 0.06 two-sample t-test, N=11).
Because of these strong physiological changes, O2/CO2 exhibits the most promise
compared to the other stimuli for inducing consistently strong responses in breast tissue.
In comparison, Air/CO2 was not significantly greater than the control for either total
hemoglobin (p = 0.30 two-sample t-test, N=4) or oxygen saturation (p = 0.25 two-sample
t-test, N=4). Air/O2 was also not significantly greater than the control for either total
hemoglobin (p = 0.49 two-sample t-test, N=7) or oxygen saturation (p = 0.33 two-sample
t-test, N=7).
140
*
Figure 7.9: Signal to noise ratio for hemodynamic measures for each stimulus. (*)
denotes significance shows that O2/CO2 induces the strongest response compared to
the air control. P-values are given in the table below.
O2/CO2 : Control
Air/CO2 : Control
Air/O2 : Control
HbT
p = 0.062, N=11
p = 0.297, N=4
p = 0.489, N=7
O2 Sat
p = 0.035, N=11
p = 0.251, N=4
p = 0.33, N=7
Table 7.3: Comparison of the correlation while breathing a gas stimulus compared
to the correlation while breathing air (control). Shown are the significance values
resulting from two sample t-tests, determining if the means were significantly
different.
141
7.6 Conclusions in Healthy Tissue
These results show that significant changes can be induced in healthy breast tissue with
the appropriate gas stimulus. In gas stimuli with carbogen, vasomotor effects dominate
the hemodynamics, whereas gas stimuli with air and oxygen depend on other, often
conflicting factors. This may be the reason why air and oxygen do not show consistent
response in the literature, especially when monitoring larger volumes of tissue.
Based on these results, O2/CO2 may be the best gas combination to use for tumor
imaging because the breast response to this stimulus is the most significant compared to
air.
7.7 Modulating tissue hemodynamics with gas stimulus in diseased tissue
One goal of monitoring respiratory induced changes in the breast is to determine tumor
vascular function, which may indicate sensitivity to therapy. Tumors often have elevated
blood flow in steady state174, and gas breathing of oxygen or carbogen can cause sharp
changes in tissue oxygenation and blood flow 163, 175, 176, especially in poorly vascularized
regions177.
However, most studies examining blood flow and oxygenation recorded
measurements with oxygen microelectrodes or laser Doppler flowmetry. Because tumors
are highly heterogeneous, these point measurements often give inconsistent results, which
are not indicative of the whole volume. For example, Kim et al. 178 identified consistent
increases in tissue oxygenation of prostate tumors with NIRS, while measuring
inconsistent changes in pO2 recorded by microelectrodes and F19 MR when rats were
challenged with carbogen stimulus. It is these large changes which are more likely to
142
tumor vascular maturity159. Optical imaging, which can non-invasively image the
vascular function of larger volumes of tissue, may be a better tool to determine regions of
compromised tumor vasomotor control.
7.8 Results in breast tumors
Four patients were imaged during dynamic breathing stimulus. Because of time
constraints, only one gas stimulus was administered. The O2/CO2 gas combination was
used because of the more consistent signal response measured with both optics and
BOLD MR. One patient dataset was thrown out due to unusually small changes in
expired CO2 and O2, monitored with the oxycapnograph. This was most likely due to the
patient bypassing the mouthpiece, and breathing room air during the exam. Difficulty in
patient compliance in gas breathing exams have been noted in previously published
studies179 because gas masks may be uncomfortable. The breathing setup used in this
study seemed more effective than a breathing mask, based on our success rate (18/19
subjects), because subject compliance was high. The data from one other subject was not
included because both the healthy and tumor tissue response were smaller than the air
control.
The hemodynamics from the data of the two patients included shows SNR > 1 for
tumor tissue and the non-diseased background fibroglandular tissue are analyzed below.
The time lag results, shown in Table 7.4, indicate that the tumor tissue in these two
subjects do not have a consistently different time lag response than the normal
background tissue for either total hemoglobin or oxygen saturation. These results are not
unexpected, as normal background tissue around the tumor is responsible for feeding
blood to the cancer.
143
Patient 2
Patient 3
Normal FG
Tumor
Normal FG
Tumor
HbT
1.75
1.5
0
1
O2 Sat
1.25
1.5
0
0
Table 7.4: Time lag results in these 2 cases show no consistent differences between
tumor tissue and non-diseased fibroglandular tissue for total hemoglobin or oxygen
saturation.
Changes in tumor vascular function are identified in Figure 7.10, by plotting the
SNR of the tumor tissue compared to the normal surrounding tissue. In these two
patients, there is a significant separation in SNR between the normal and tumor tissue in
HbT (p = 0.018 two-sample t-test, N=2). This SNR change is due to a weaker correlation
in the tissue response to the gas stimulus in both cases. These results could be explained
by a lack of adequate smooth muscle cells to allow proper vasodilatory response.
144
Figure 7.10: Initial results indicate that the signal to noise for total hemoglobin
(HbT) in tumor tissue is significantly lower than the background fibroglandular
tissue. This separation is not demonstrated with oxygen saturation (Sat) for the 2
patients. Even with this small sampling, HbT has significantly lower SNR than the
background normal tissue (p = 0.018). Without the control of air breathing, the
correlation coefficient measure provides no significant difference between tumor
and the surrounding normal tissue (p=0.76). The importance of an air control is
critical, as one patient is not shown because all SNRs were <1.
7.9 Conclusions
Investigators have been studying gas breathing as a means to elevate oxygen levels for
improved therapy sensitivity for over 50 years180. The ability to determine the sensitivity
of a subject to these respiratory stimuli would have a significant impact on radiation
treatment. In practice, this method could be used to screen for patients who would
benefit from gas breathing during radiation therapy. For tumor detection, abnormal blood
flow and oxygenation have been shown to be hallmarks of cancer8. The data presented
above indicates that consistent physiological changes can be induced with the appropriate
gas breathing stimulus - specifically, O2/CO2. Subjects who breathed the O2/CO2
stimulus showed consistent (p<0.05) and significant (p<0.05) response. In addition,
imaging of tissue functional immaturity may be possible with gas breathing and optical
imaging. In 2 cases, it was shown that the total hemoglobin in tumor tissue did not
respond as strongly as the surrounding normal tissue to the gas stimulus (p<0.05).
145
However, the data presented here also indicates that these respiratory
measurements can be highly corrupted by physiological noise. Even with the appropriate
choice in breathing stimulus, specifically, the O2/CO2 stimulus, four of eleven datasets
from healthy volunteers had SNR < 1. This study highlights both the need for correct
choice in stimulus, and the importance of monitoring steady state fluctuations for use as a
control. If this technique is to be used for further proof of concept studies in tumor
imaging, it is highly recommended that the O2/CO2 gas stimulus is used.
146
Chapter Eight: Correlating oxygenation measured by BOLD and Optics
in the Breast
8.1 Introduction
This chapter aims to provide the foundation for understanding how optics and blood
oxygen level dependent (BOLD) MR correlate in the breast. The advantage of this
multimodality approach is that the quantitative accuracy of measuring total hemoglobin
and oxygen saturation with optics can be combined with the spatial and temporal
resolution of BOLD imaging of deoxyhemoglobin. This section begins with a
description of the BOLD contrast, and how its signal relates to the optical signal.
Experimental results are shown which validate the assumption that optics and spin echo
BOLD yield similar contrast values in deoxyhemoglobin, as long as the appropriate
inspired gas is used, and appropriate controls are considered which identify noise. The
next chapter will investigate a comprehensive spatial/physiological reconstruction model
which combines these BOLD images for better estimation of tissue oxygenation maps.
8.2 The BOLD Contrast
Since the discovery by Ogawa181 in 1990 that the MRI could measure signal changes due
to changes in blood oxygenation in the rat cortex, there has been a vast amount of
research into blood oxygenation dependent (BOLD) MR. Although Ogawa originally
used different gas compositions to induce hypoxia, it was also established that the
metabolic increases in oxygen consumption during functional brain activation resulted in
147
similar MR signal changes182. The field of functional MRI (fMRI) is based upon this
observation.
The mechanism behind BOLD contrast is the change in magnetic susceptibility
caused by the paramagnetic nature of deoxygenated hemoglobin183. Areas of
concentrated deoxyhemoglobin, such as venous vasculature, locally perturb the main
magnetic field, which de-phases surrounding protons. This de-phasing causes signal
dropout in the collected image, and these regions appear darker. The presence of
deoxyhemoglobin affects two types of tissue relaxation parameters: T2’, the spin-spin
relaxation decay time constant attributed to magnetic field inhomogeneity184, and T2, the
relaxation due to diffusion. While gradient-echo BOLD is the most common sequence
used to image deoxyhemoglobin because of its sensitivity to the field inhomogeneity,
spin-echo BOLD has been used successfully in certain applications.
The BOLD signal is believed to have two contributions: water protons in
extravascular tissue, and water protons in intravascular tissue185. In the extravascular
tissue, the effect is vessel size dependent. Water protons will diffuse a substantial
distance during the echo time compared to the diameter of the capillaries. Because these
capillaries may have different amounts of deoxyhemoglobin, the water protons will
experience a variety of magnetic fields, which will de-phase them. Around larger
vasculature (greater than the diffusion length of water during the echo time), water
protons will tend to remain in the same magnetic field. These protons will not be
dephased as greatly. Thus, the T2 will shorten in the extravascular tissue surrounding
small vasculature, and will be less affected around larger vasculature185. The
intravascular component to the BOLD signal is mainly due to the amount of
148
deoxygenated blood in the vessel. This signal depends on the T2 of the blood, which is
field strength dependent186. At higher fields > 4T, the T2 of the blood shortens
significantly187, minimizing its effect on the reference and activation image188.
One limitation of gradient echo BOLD imaging is that the great majority of the
signal comes from larger venous, draining vessels189. These larger structures not only
have a higher concentration of deoxyhemoglobin, but they also have more blood volume
than the surrounding tissue. Additionally, the susceptibility caused by the larger
vasculature structure is enhanced, causing greater signal dropout186. The signal produced
in these regions dominates the smaller signal produced by the capillaries in close
proximity to the activated tissue190. This effect intrinsically limits the spatial resolution
of the technique. It also may overwhelm the signal from local regions of
microvasculature or tumor tissue which is in close proximity to these draining vessels.
Another limitation of this technique is that it may spatially distort anatomy in anatomical
regions of high B0 inhomogeneity, such as the breast191.
In order to eliminate these detrimental effects, spin echo has been developed for
BOLD imaging. Since spin-echo imaging is insensitive to T2’, it is unaffected by
magnetic field changes due to susceptibility, and may be more effective at imaging the
deoxyhemoglobin content in the microvasculature186. Spin echo sequences eliminate the
T2’ effect by refocusing spins that are locally precessing much faster or slower than the
surrounding tissue. This will improve spatial resolution in regions of high magnetic
nonuniformity. However, spins that have diffused to a region with a different magnetic
field are considered irreversible, and cannot be refocused. Thus, spin echo is sensitive
only to T2. It has been shown to be insensitive to the large pools of deoxygenated
149
hemoglobin in large venous structures, and also to the extravascular signal surrounding
larger vasculature. Although signal to noise is lower in spin echo BOLD than gradientecho BOLD, its advantages for breast BOLD far outweigh its disadvantages. This study
used spin echo BOLD for these reasons.
8.3 The rationale for combining BOLD and Optics
A great deal of effort has been devoted to the interpretation of the BOLD signal. This
work is motivated by the promise of BOLD in cognitive studies, and clinical
pathophysiology studies investigating Alzeimer’s disease 192 schizophrenia193, and
epilepsy194, among other neurological diseases. However, the inherent sensitivity of the
BOLD signal to deoxy- and not oxy-hemoglobin limits its interpretation. Additionally,
the difficulty in quantifying deoxyhemoglobin complicates longitudinal or inter-patient
studies. It is these two areas that optics has the opportunity to aid BOLD.
First, because optical imaging is sensitive to both oxy and deoxyhemoglobin,
optical imaging can help decouple changes due to oxygen consumption, blood volume,
and blood flow. However, there is an inherent trade-off between spatial and temporal
resolution. Optical imaging systems with high temporal resolution usually use few
source-detector pairs, which limits spatial resolution. Spatial resolution erodes with
depth195, although many strategies have helped alleviate the problem196, most notably for
this thesis, image guided techniques34, 79. High temporal resolution usually occurs at the
expense of quantitative accuracy - usually tissue scatter properties. If MRI is available
and a compromise must be made, the optimal approach would be one where the optics
system would sacrifice temporal resolution for quantitative accuracy. This combined
150
approach could aid the interpretation of BOLD signals with optics, while improving
optics with the temporal resolution of BOLD.
There are numerous models which aim to quantify the BOLD signal, such as
qBOLD (quantitative BOLD)197, 198. These have been used to quantify cerebral blood
volume197-201. However, the source of contrast in fMRI is not sufficiently well
understood to allow for accurate quantification of blood oxygenation202, especially in
tumor tissue202, because of the many physiological components aside from
deoxyhemoglobin that contribute to the BOLD signal, including hematocrit, blood
volume, and tissue pH. In addition, magnetic inhomogeneities (B0) and Rf absorption
(B1), which take substantial time and effort to quantify203, 204, may affect the BOLD
signal202. Therefore, in most BOLD studies, relative signal changes from baseline are
measured.
On the other hand, optics has been shown to provide quantitatively accurate
estimation oxy- and deoxy- hemoglobin in tissue simulating phantoms, accurately
reproducing the oxygen dissociation curve205-208. Thus, optical imaging may provide
more accurate quantification of tumor hemodynamics72, 209, 210. Therefore, the
combination of these modalities seems advantageous.
8.4 Comparisons between Optical and BOLD contrast mechanisms
It is important to identify the contrast mechanisms between BOLD and optical imaging to
ensure that these techniques are sensitive to the same vascular tissue. While the gradient
echo BOLD signal arises from deoxygenated blood from a mix of large and small vessels
211
, spin echo BOLD should have more sensitivity to the microvasculature185. NIR
contrast arises from both the oxygenated and deoxygenated blood contained in smaller
151
vessels that make up the capillary bed212. Thus, these techniques should give consistent
information about the relative amounts of deoxyhemoglobin.
8.5 Correlations between Optics and BOLD MR
8.5.1 Correlations performed in healthy tissue
In order to establish the correlation between optical and BOLD measured hemoglobin,
several studies have examined optical imaging and fMRI in both the small-animal and
human brain. Although these studies show significant spatial correlation between optical
and fMRI, there are conflicting results on the relative strength and direction of correlation
between optically measured hemoglobin and BOLD. All studies demonstrated
concurrent increases in BOLD signal and oxyhemoglobin, including in the rat brain
during whisker213 and forepaw stimulation214, and hypoxic respiratory challenge108, 215,
and in the human brain during visual212 and motor216, 217 stimulation. However, studies
have demonstrated both positive correlation214, 217 and negative correlation212, 213, 216, 218220
between BOLD and optically measured deoxyhemoglobin.
Some discrepancies in the results can be explained by differences in techniques,
and the difficulty in spatially coregistering these two modalities. While BOLD MR
imaging samples signals produced in the tissue, optical imaging is a boundary
measurement technique. In the human head especially, transmission measurements
across the brain are technologically infeasible because of the large source detector
distances. Therefore, reflectance measurements must be taken, which are heavily
weighted towards the surface. In this region, BOLD MR may suffer from susceptibility
artifacts near the skull221, which may cause increased noise in the region of optical
sampling.
152
To alleviate multimodality sampling errors, several groups have either
reconstructed optical data tomographically219, or projected BOLD data onto the optical
data through the optical photon density function216, 217. Tomographic reconstructions
with reflectance measurements suffer from partial volume effects, in which the sensitivity
of the measurements does not completely encompass the region of contrast. The effect is
a recovered contrast which is located shallower than the actual position83. Improvements
in reconstruction algorithms may aid in more accurate depth recovery83, providing more
accurate optical maps to coregister with BOLD. Projection of the BOLD data through
the optical sensitivity function helps coregister optical and BOLD signals. However, one
confounding factor in these studies has been that they assume a scattering function which
may lead to errors in the determination of the correct projection function222.
As these studies were all performed in healthy brain tissue, generalizing these
results to include breast tissue may not be valid. To the best of our knowledge, the
correlation between BOLD MRI and optics in the breast has yet to be studied.
8.5.2 Correlations in tumor tissue
Hemodynamics have been studied in tumor vasculature in the MR, and changes in tumor
oxygenation, blood volume, and/or blood flow have been detected in small animal model
223
, brain 224, and breast 225, 226 tumors.. However, to date, hemodynamic studies of
tumors involving both optical and MR imaging have been very limited. Xu et al. found
strong correlation in tissue oxygenation between R2* and optically measured
deoxyhemoglobin108 in a healthy rat. Tumor blood volume and blood flow estimates
from MR and optical imaging have yet to be compared.
153
8.6 Methods for the studies in this Thesis
8.6.1 Subjects
This study was approved by the Internal Review Board at the Stanford University
Medical Center. Six healthy subjects and three patients with invasive ductal carcinomas
were imaged. Volunteers with presumed normal breasts were young adults in good
health. Of the six healthy subjects, three were imaged a second time 1-2 weeks after the
original exam. One dataset was dropped because of poor fiber contact (3/16 fibers
contacted the breast). One dataset was dropped because the MR malfunctioned. In the
results presented below, each imaging session is labelled individually, as it is expected
that respiratory response is not repeatable on different days, and there were not enough
subjects to analyze intra-subject variation over the menstrual cycle. Of these subjects,
only one was taking birth control. The imaging studies are detailed in Table 8.1.
Imaging
O2/CO2
Air/CO2
Air/O2
Notes
study
1
X
IDC
2
X
IDC
3
X
X
5
X
X
X
Healthy
6
X
X
X
Healthy
7
X
X
Poor fiber contact
8
X
X
Healthy
9
X
X
Healthy
IDC
154
10
X
11
X
Healthy
X
12
Healthy
Equipment failure
13
X
X
X
Healthy
14
X
X
X
Healthy
Table 8.1: List of imaging studies performed with optics and BOLD MR. Imaging
studies 1-3 were volunteers with invasive ductal carcinomas (IDCs) of the left
breast. Imaging studies 5-14 were healthy subjects. Studies 5&7, 6&11, and 13&14
were the same person. In the table, an ‘X’ indicates data that was collected.
Volunteers with IDCs were imaged with a radiologist (B.D.) and an MR
technologist (S.S.) on site to aid in the appropriate placement of the fibers. Tumors were
identified by B.D. and by the location of a breast clip that was inserted during biopsy.
All tumors were confirmed by pathology.
8.6.2 Respiratory challenge
As explained in further detail in Chapter 7, subjects were given three sets of gas stimuli
to induce hemodynamic changes in the breast. The three stimuli, oxygen/carbogen,
air/carbogen, and air/oxygen, were introduced to the volunteer via a custom breathing
circuit with a 1-2 min pause in between each stimulus set. During a stimulus, a custom
built computer-controlled valve switched to the opposing gas every two minutes. The
switch between gases in a stimulus was repeated 8 times, for a total of 4 periods for each
gas stimulus. Gas flow was kept at a constant rate of 9L/min. Expired gases were
155
analyzed with a gas analyzer (Ultimax Capnomac) so that subject compliance could be
ensured. The circuit used for respiration had two valves which controlled inhaled gas.
During times of air stimulus, a valve would open which would allow breathing of room
air. When the oxygen or carbogen was turned on, the valve leading to room air would
close, while a valve leading to the gas tanks would open. There was a ~20 second delay
between the initiation of a gas and a corresponding change in the expiration monitor.
Subject heart rate and respiratory rate were monitored with pulse oximetry and a
respiratory belt.
Carbogen (also identified in this text as “CO2”), a mixture of 95% oxygen / 5%
carbon dioxide, has been found to induce panic in subjects when inhaled. In one study at
another institution, 100% of the subjects227 became uncomfortable after breathing
carbogen for 12 minutes. No subject enrolled in this study reported any feelings of
discomfort, probably because of the relatively short duration of carbogen breathing (2
minutes at a time).
8.6.3 Data Collection
As discussed previously in this chapter, spin echo sequences yield better BOLD images
than gradient echo sequences in breast tissue191. For this study, a 2D Single Shot Fast
Spin Echo (SSFSE) susceptibility weighted sequence provided high temporal resolution
(TR=4sec) and high spatial resolution (1.56mm x 1.56mm in-plane resolution). A total
of 60 images were captured during each stimulus period, for a total of 240 images /
stimulus. A limitation in this technique is the amount of energy deposited in the tissue,
known as the specific absorption rate (SAR). Because of SAR limitations, image
acquisition was limited to 1 or 2 slices, depending on subject weight. These slices were
156
co-registered with the optical imaging array by using fiducial markers as references, and
by manually inspecting the distortions at the tissue surface caused by the optical fibers.
An example SSFSE image in the plane of the optical fibers is shown in Figure 8.1.
Figure 8.1: Example SSFSE image used to measure the BOLD signal. This coronal
slice was taken in the plane of the optical fibers. The low intensity shading in the
lower left of the image is phase wrap from the contralateral breast. Note the bright
motion artefact near the skin at the top.
Optical imaging was performed simultaneously during BOLD MR acquisition so
that image contrasts could be correlated in time. A custom optical interface was built into
the 8-channel MR breast coil (USA Instruments). This interface, shown in Figure 8.2a,
was integrated with the breast immobilization plates designed by the manufacturer. Rails
were bolted into these plates to allow vertical positioning of the optical interface. Plastic
157
thumbscrews allowed the interface to be moved and secured once the desired height was
chosen. In most cases, the interface was positioned at the extreme posterior of the plates
to image as close to the chest wall as possible. The immobilization plates could be easily
removed from one side of the coil and repositioned on the other side depending on which
breast was being imaged. Figure 8.2b shows a subject with all imaging and monitoring
equipment attached, prepared to enter the MR bore for the imaging study. The arrows in
Figure 8.2b identify the pulse oximeter and respiratory belts that were used to reduce
BOLD noise. The three wavelength dynamic source unit was used in this study to image
all wavelengths simultaneously, with temporal resolution of ~30 seconds. This
resolution allowed 8 images to be captured during each stimulus period, and 32 images /
stimulus.
a
b
158
Figure 8.2: (a) The optical imaging interface on the lateral side of the right breast.
Optical fibers could be moved anterior/posterior along custom built rails and locked
into position with plastic thumb screws. This interface was bolted into the
manufacturer’s breast immobilization plates. (b) Subject entering the magnet bore.
Shown with arrows are the pulse oximeter and respiratory belt.
8.6.4 Data analysis
Because the BOLD data was sensitive to changes in the magnetic field, patient motion
caused significant noise. To remove this unwanted noise, BOLD data was pre-processed
with an algorithm which removed respiratory and pulsatory motion from the signal228.
Removing this noise was critical to achieving images with adequate signal to noise
because the temporal resolution of the BOLD data collection (4 seconds) overlapped with
the frequency of respiration, and a harmonic of the heart rate. This algorithm also
reduced gross patient motion by estimating movements in the centroid of the image
domain.
All voxels in the BOLD images were temporally correlated to the gas stimulus, as
discussed in Chapter 7. This calculation formed voxel by voxel images of the strength of
correlation at various time lags in the stimulus period. An example of the correlation at
one such time lag is shown in Figure 8.3b. To minimize the effects of patient motion on
the cross correlation calculation, a rectangular region of interest (ROI) was selected
which excluded the interface between the breast and air. The time point which had the
most significant correlation, as indicated by signal intensity, was selected as the time lag
159
between the stimulus and the response. Example BOLD temporal data is shown in
Figure 8.3a229. Similarly to the optical timecourse data, the BOLD data shows a strong
response at the frequency of the stimulus.
a
b
Time
Figure 8.3: (a) BOLD signal time course for O2/CO2 stimulus. Red (O2) and green
(CO2) bars indicate the inspired gas. (b) BOLD correlation image at a certain time
lag. This image is thresholded at a p=0.05 significance level. The yellow box
indicates the ROI. This was selected to minimize motion noise near the boundary.
(Edited from communication courtesy of Rakow-Penner, 229).
Optical data was calibrated with a reference image from the subject at rest108, and
reconstructed via the hard priors method. This imaging method provided a global
estimate of the oxygenation of the fibroglandular tissue, while being more robust to noise
than a non image-guided reconstruction technique. The IDEAL fat/water sequence was
used to separate fibroglandular from the adipose tissue (Figure 8.4b). This resulted in a
2-pixel optical image for each healthy subject. An example region segmentation is
160
shown in Figure 8.5a. Images of oxyhemoglobin, deoxyhemoglobin, and water were
reconstructed at each time point. (This methodology varies from chapter 7, where total
hemoglobin and oxygen saturation images were correlated). Two such time points are
shown in Figure 8.5b-e. Scatter signal was fixed at the value calculated in the reference
image, as tissue structure was not expected to change during functional stimulus. The
oxyhemoglobin and deoxyhemoglobin timecourse is shown for one subject in Figure
8.6(a,c). Note the dominant frequency of 0.041Hz (1/240 sec) in the frequency spectrum
for each component in Figure 8.6(b,d).
a
b
Figure 8.4: MR images used for data analysis. (a) BOLD SSFSE image, (b) Water
image used to segment optical regions.
161
a
b
c
d
e
Figure 8.5: Hard prior difference reconstructions using region information for 2
consecutive timepoints. (a). HbO, Hb, for timepoint 1 (b,c), and timepoint 2 (d,e).
a
b
c
d
Figure 8.6: Temporal and frequency response of hemodynamics to O2/CO2 gas
stimulus. White bars indicate O2 stimulus, gray bars indicate carbogen stimulus.
162
(a,c) Oscillations of oxy and deoxy hemoglobin in time, and (b,d) the corresponding
frequency spectrum showing peaks at (1/240) Hz.
One advantage of the optical imaging data acquisition was that its low temporal
resolution was immune to aliasing from the higher frequency biological signals, in
contrast to the BOLD MR data. This is because each optical time point consisted of data
averaged over 30 seconds. In effect, the data collection would average out the high
frequency fluctuations. Thus, no temporal noise correction was applied to the optical
data before computing cross-correlations.
Both BOLD and optical measured responses were cross-correlated to the gas
stimulus using MATLAB (Mathworks, cov function). Although gas content changes in
the lung were abrupt and step-like upon a switch in gas, the body is expected to low-pass
filter changes in blood flow throughout the body230. Thus, the stimulus was
approximated with a sinusoidal function, where the first gas would be on during any time
where a zero mean sinusoid was negative, and the second gas would be on during any
time the sinusoid was positive. A more in depth explanation is given in Chapter 7. To
ensure that there were no lingering effects of a previous gas, the first period out of four
periods was dropped from the data analysis.
The cross correlation analysis provides a robust method to determine the strength
of signal oscillatory response, and the time lag between gas inhalation and tissue
response. Chapter 7 showed that the strength of correlation could be used to determine
an effective noise level. Cross correlations of the tissue response with the stimulus time
series while the subject breathed strictly air provided a control to determine which
163
oscillations were due to normal physiology, and which oscillations were due to the gas
stimulus. The measure of time lag was identified as the direction of tissue response to a
specific gas. Because the signal is periodic, this lag is measured in units of π. For
example, if oxyhemoglobin had a time lag of π/2 during an air/oxygen gas stimulus, it
would indicate that oxyhemoglobin was increasing during air breathing, and decreasing
during oxygen breathing. Again, the reader is referred to Chapter 7 for a more detailed
discussion.
8.7 Results
The time lag values between each stimulus and the measured response of
deoxyhemoglobin are shown below. For each imaging case, the BOLD results were
analyzed using the spatial region with the maximum correlation to the stimulus. For
volunteers 1-3, this region coincided with the tumor region of interest. For all healthy
volunteers, the region analyzed was the fibroglandular region.
Similar to the results in Chapter 7, each subject had a different phase response to a
given stimulus. These time lag values for BOLD and optics are plotted below in Figure
8.7. This heterogeneity in temporal response can be explained by intra-subject
differences in vascular function, aerobic health, and metabolism, which may change
daily. A more direct comparison of optical and BOLD is shown in Figure 8.8. This data
examines the phase lag of optically measured deoxyhemoglobin vs. BOLD, where a
perfect correlation would yield a straight line at “y = x.” This data suggests that the
O2/CO2 stimulus should give the highest correlation between optical and BOLD
164
measurements. In comparison, the air/CO2 stimulus and air/O2 stimulus resulted in nonstatistically significant optical/BOLD correlation.
a
b
c
Figure 8.7: Phase lag between the gas stimulus and the measured BOLD and optical
deoxyhemoglobin response for (a) O2/CO2, (b) Air/CO2, and (c) Air/O2. The results
for both modalities show little consistency over time for the different subjects.
165
b
a
c
Figure 8.8: Comparison of BOLD signal phase lag vs deoxyhemoglobin measured
optically for all patients for respiratory stimuli of (a) O2/CO2, (b) Air/CO2, and (c)
Air/O2, plotted with the line of equality. Axes are in units of radians.
In Chapter 7, it was demonstrated that the strength of the O2/CO2 response was
significantly greater than the control, compared to the air/oxygen and air/carbogen
166
stimulus. This increased signal was attributed to the amplification of vasomotor
modulation due to the oxygen/carbogen stimulus controlling
vasoconstriction/vasodilation. However, the response in some volunteers was still less
than the control. Thus, it was considered prudent to remove data from volunteers that
exhibited insignificant responses compared to the control, as BOLD and optics are not
expected to correlate in these noise-dominated cases.
The correlation of deoxyhemoglobin during the oxygen/carbogen stimulus
compared to the control is plotted in Figure 8.9. This data suggests that the stimulus in
some subjects, notably subjects 5, 9, 11, and 13, did not result in any significant response,
and the data should be removed. The phase lags for the oxygen/carbogen stimulus are replotted with non-responding subjects removed from the dataset in Figure 8.10. This data
shows significant linear correlation between the BOLD response and the optical response
(r=0.76, p=0.048, N=7, two-sample t-test). This dataset also implies that the BOLD
response is generally π/4 earlier than the optical response. By comparison, if the poor
air/O2 or air/CO2 data is removed, no significant correlation is found using these stimuli.
These results are summarized in Table 8.2.
Gas protocol
O2/CO2
All data
(r-values & p-values)
r = 0.11
p = 0.76, N=11
Hb SNR > 1
(r-values & p-values)
r = 0.76
p < 0.05,N=7
Air/CO2
r = 0.50
p = 0.67, N=3
r = 0.5
p = 0.66,N=3
Air/O2
r = -0.39
p = 0.44, N=6
r = -0.31
p = 0.61,N=5
Table 8.2: Correlations and significance between optically measured
deoxyhemoglobin and BOLD. After removing data where the optically measured
167
deoxyhemoglobin had a smaller correlation than the air control (SNR < 1), the
O2/CO2 stimulus induces a response in which optics significantly correlates to
BOLD.
Figure 8.9: Optically measured deoxyhemoglobin correlation to an all air stimulus
(control), and the O2/CO2 gas stimulus. Although most subjects exhibited a stronger
correlation to the gas stimulus than to the control, some subjects did not respond to
the gas stimulus.
168
Figure 8.10: Correlation between BOLD and optically measured deoxyhemoglobin
during O2/Carborgen gas stimulus. This plot shows that BOLD and optics correlate
significantly r = 0.76, p = 0.0477 only when appropriate consideration is given to
SNR.
8.8 Conclusions
The results from this section indicate that BOLD and optically determined
deoxyhemoglobin correlate significantly in the breast when the oxygen/carbogen
stimulus is used in conjunction with proper control measurements (p<0.05). These
caveats highlight the difficulty in generating sufficient hemodyanamic changes in breast
tissue with gas breathing stimuli, and the importance of multimodality measurements. If
optical data is absent, there will be no control data because there is not sufficient BOLD
signal during air breathing to induce signal in the region of activation.
169
The region of BOLD activation yields a new tool in MR guided optical imaging.
Even though optics and BOLD can correlate significantly, the BOLD signal has higher
noise than optics. This noise decreases in the region of the BOLD image which
significantly correlates to the stimulus. Thus, the BOLD image gives high resolution
maps of where the functional changes in deoxyhemoglobin are strongest. A comparison
of the optical and BOLD maps is shown in Figure 8.11. In Figure 8.11(a,c), the
segmented IDEAL image generates the tissue regions. In contrast, the BOLD image,
shown in Figure 8.11(b,d), is a higher resolution map. By selecting a region of interest
which correlates significantly to the stimulus, a region of higher deoxyhemoglobin
response is found. This region will be used to guide the optical reconstruction in the next
chapter.
The combination of these modalities offers new opportunities in studying tissue
oxygenation with BOLD MR. Since optical is able to decouple oxygenation from blood
volume, it may be used to verify the origin of contrast changes in BOLD imaging. This
technique could be used to validate BOLD sequences that are faster or attempt to quantify
hemodynamics. In addition, the opportunity now exists to “calibrate” the BOLD signal
with optics in the breast. A practical approach could be a simple pad of optical fibers
which would monitor changes in physiology. The overlapping optical and BOLD voxels
could then be used to determine absolute concentrations of hemodynamics, which could
be related to the tissue volume.
The stimulus in this work was chosen to isolate the stimulus frequency from the
heart rate and respiratory frequencies, and to induce significant changes in breast
physiology. However, increases in SNR may be possible by decreasing the modulation
170
rate of the gases. Results from other groups have shown that tissue oxygenation changes
may increase for 10 minutes or more, allowing for increasingly perfused tissues.
However, there is a limit where carbogen will induce anxiety in volunteers. In addition,
longer stimulus periods will result in fewer cycles of the stimulus, which may hinder
cross correlation results. An important study will be the examination of the optimal
stimulus period to maximize SNR while minimizing patient discomfort.
a
b
c
d
Figure 8.11: Comparison of regions of interest for a healthy subject. (a) Segmented
fibroglandular tissue used for optical image guided reconstruction, (b) BOLD
stimulus correlation image, (c) segmented fibroglandular region, (d) segmented
BOLD region used for cross correlation.
Acknowledgements
171
This study would not have been possible without the great help from Rebecca RakowPenner, who designed the breathing circuit and implemented the breast BOLD sequence.
Additionally, the support and participation of Dr. Bruce Daniel, Dr. Gary Glover, Dr.
Brian Hargreaves, Anne Sawyer, and Sandra Rodriguez is gratefully acknowledged.
172
Chapter Nine: A Structural and Functional Multimodal Reconstruction
Model
9.1 Introduction
This chapter develops a reconstruction model which incorporates MR-derived spatial and
functional covariance images into the optical reconstruction. The foundations for
including these images were developed in previous chapters. This model aims to
incorporate total hemoglobin images available from T1-weighted MR, deoxyhemoglobin
images from breast BOLD, and water images from MR water/fat separation. This
algorithm is tested in simulation and compared to the case where identical structural
priors are applied uniformly.
9.2 Justification for including MR covariance priors
Earlier in this text, and in previous work 34, 82, 87, 90, 94, 107, 231, it was assumed that each
tissue type identified by MR could be applied as a structural map for each tissue
physiological parameter. Specifically, breast anatomy determined by T1 relaxation was
applied as a spatial covariance map either forcibly (region reconstruction), or more
leniently, allowing slight variations within a tissue region (soft prior reconstruction).
Based on the MR-NIR results for 14 healthy subjects in a previous work89, oxygenation
was not significantly different between tissue subtypes, though total hemoglobin, water,
and scatter did have significant differences. The results from three of these subjects are
shown in Figure 9.1, and the other healthy values are shown in Table 9.1, from Brooksby
et al.89. These results show that this tissue-type spatial map should not be applied to the
173
recovery of oxygen saturation, since oxygenation is not dependent on tissue type as
defined by T1-W MR.
By applying an improper spatial map, image-guided reconstructions risk biasing
recovered values to inaccurate solutions. Grouping tissues with different contrasts into
one region will overestimate one tissue type, while simultaneously underestimating
another. Thus, it is important to only apply spatial covariance maps which have
significant correlation to the tissue physiological contents.
Figure 9.1: Physiological variations in total hemoglobin, oxygen saturation, water
content, and scatter, between adipose and fibroglandular tissue in 3 healthy
subjects. This data shows differentiation between adipose and fibroglandular tissue
in total hemoglobin and water, and less so in scatter. No substantial difference is
seen in tissue oxygenation.
Property
Mean difference between Adipose & FG
(p-values)
174
HbT
0.022
Oxygen Sat.
0.798
Water
0.040
Sc-A
0.005
Sc-Power
0.045
Table 9.1: Differences in tissue properties from Brooksby et al.89 These results from
11 subjects show significant differences between all parameters but oxygenation.
The similarities between functional MR and optical parameters have been
investigated in this text, in the context of breast imaging. In chapter 6, MR water images
were shown to provide quantitative estimates of water content. This work was based on
the correlation studies performed by Merritt et al.140, who showed that water and fat
measured by MR and optical methods correlated significantly. This water image
intuitively is a more appropriate covariance map for water estimation than the T1 Nuclear
Magnetic Resonance (NMR) relaxation map.
In chapter 8, it was shown that with the appropriate choice in gas stimulus and
taking into account noise, BOLD and optical imaging correlated significantly. It is
important to establish that even though the BOLD contrast is “Blood Oxygen levelDependent,” BOLD contrast is actually “deoxyhemoglobin dependent.” This BOLD
image provides a spatial covariance map of regions of tissue that have similar amounts of
deoxyhemoglobin.
The physiological spatial and quantitative maps for total hemoglobin,
deoxyhemoglobin, water, and scatter may be incorporated into an algorithm that provides
175
optimal spatial guidance for the tissue contents. This information is expected to improve
physiological image recovery.
9.3 Multimodal reconstruction
The incorporation of these multiple priors requires the formulation of an objective
function which corresponds to these physiological covariance maps: total hemoglobin,
deoxyhemoglobin, water, and scatter. In chapter 3, the objective function was presented
as:
(9.1)
This formulation was derived from the extinction coefficients in the tissue, where
(9.2)
The spatial prior, either implemented via the Laplacian or the region based parameter
reduction technique, was applied to the parameter weight matrix:
(9.3)
In the case of the Laplacian matrix, the spatial prior which defined the covariance matrix
was:
i=j
i,j are not in the same region
i,j are in the same region
(9.4)
To incorporate the appropriate physiological covariance maps, an objective function:
176
(9.5)
is defined in terms of:
(9.6)
The covariance weight matrix Wµ’ includes the appropriate MR images in the covariance
matrices:
(9.7)
Example covariance maps with the properties defined previously in chapters 6 and 8 are
shown in Figure 9.2. In Figure 9.2a, the application of the structural T1-weighted image
forms identical structural images for all parameters, whereas in Figure 9.2b, T1-W,
BOLD, and water images form the respective parameter priors.
a
b
Figure 9.2:: MR images can be incorporated into the image reconstruction either (a)
structurally, or (b) functionally. Here, 0 or 1 indicates spatial regions. The 40-60 for
the water color bar indicates percent water.
177
9.4 Simulation test problem
A test problem simulated the utility of the reconstruction model. To examine the effect
of a uniform structural coviariance model vs. the physiological covariance model, a 2:1
HbO contrast inclusion was added to a homogeneous background, and 5% amplitude, 5
degree phase Gaussian noise was added to the data. Two reconstructions were used to
recover tissue properties. For the structural covariance reconstruction, covariance maps
were consistent for all parameters (shown in Figure 9.3a). In contrast, the physiological
covariance reconstruction used the appropriate maps for the tissue properties: T1-W for
total hemoglobin, BOLD for deoxyhemoglobin, water/fat for water, and T1-W for scatter.
These maps are shown Figure 9.3b. Because the goal of this simulation was to determine
what effect an improper spatial map would have on the resulting Hb image, the
quantitative water values were ignored. The reconstructions were performed with the
hard-priors (region-based) method, with the same regularization and stopping criteria.
a
b
Figure 9.3: Covariance maps for the test problem. (a) For the structural covariance
reconstruction, a T1-weighted image was used for all covariance maps. (b) For the
physiological covariance reconstruction, a homogeneous Hb map was used. Total
178
hemoglobin, water, and scatter used identical covariance maps. In this case, the
water image was used only as a structural covariance map, and not as a quantitative
map as implemented in Chapter 6.
9.5 Simulation results
The reconstruction results are presented below. The target results are shown in Figure
9.4a, the structural covariance reconstruction results in Figure 9.4b, and the physiological
covariance reconstruction results in Figure 9.4c. The covariance maps in Figure 9.3 were
applied to these reconstructions. Both reconstructions show accurate parameter recovery
in the absorbing chromophores. Accuracy is slightly less in recovered scattering
parameters. As expected, there is a slight bias in Hb in the inclusion region of the
standard reconstruction, due to the improper covariance map that was applied. Although
no contrast change is forced with these covariance maps, noise will bias the recovery to
slightly incorrect values. Both reconstructions recover HbO extremely well, with the
physiological covariance method having a slightly increased bias in the background.
Water is biased in the inclusion region of both reconstructions, as the target water
contrast is homogenous, and a heterogeneous water covariance map was applied. Again,
this bias demonstrates error that can occur when improper covariance maps are chosen.
179
a
b
c
Figure 9.4: A simulation test problem demonstrated the bias in Hb introduced when
improper covariance maps were used. (a) The target true values. (b) The structural
covariance reconstruction, using covariance maps in Figure 9.3a. (c) Physiological
covariance reconstruction using covariance maps in Figure 9.3b. Although the bias
is very slight (~5%), this simulation demonstrates the bias resulting from applying
improper covariance maps.
9.6 Conclusions
This section demonstrated that covariance maps derived from several MR contrasts can
be incorporated into a comprehensive model. In particular, MR T1-weighted images,
MR water/fat separation images, and BOLD MR images were used to form covariance
maps for the parameters. A simulated test problem showed that improper covariance
maps applied to the image reconstruction results in bias in the parameter recovery of Hb
180
of 5%. Although the effect of this bias was small in this case, it demonstrates that
applying appropriate covariance maps is important to ensure that the best estimate is
achieved.
181
Chapter Ten: Concluding Remarks
10.1 Overview of work completed
MR-guided optical imaging shows promise as a clinical instrument that can add
information content to breast MR, which may aid in the characterization and monitoring
of breast disease. This work extended the synergy of MR and optical imaging by
incorporating several other MR contrasts into the optical image reconstruction. This was
shown to improve optical image quality both spatially and quantitatively. It also enables
the possibility of improving the temporal resolution of optical images. This modality not
only improves optical imaging with MR, but also may aid in the identification of the
origins of MR contrasts, by providing both quantification and the ability to decouple MR
contrasts.
A significant effort was devoted to the improvement of optical data quality by
characterizing system noise and identifying unreliable data. The effect of poor data
quality is often not recognized during image reconstruction. Poor data increases the
model/data misfit, but often not to such an extent that it is obvious, e.g. if the algorithm
were to diverge. If not incorporated into the noise model in the reconstruction, this noise
will prevent the optimization from approaching the global minimum. In practice, an
iterative reconstruction will not iterate sufficiently to provide quantitatively accurate
images, and may reach a poor solution. Therefore knowledge of noise bounds is
important in the implementation of this system, as signal levels are more than an order of
magnitude lower than to the standalone optical system at Dartmouth.
182
Optical breast exams are not only limited by system noise. Sampling the region
of interest is the most important aspect of breast imaging. A slab geometry optical fiber
holder was developed to replace the single-plane circular holder. With this geometry, it
was demonstrated that a higher percentage of quality data could be collected. This
geometry also has the critical advantage over circular single-plane geometries in that it
offers the ability to sample multiple planes without distorting the coregistration between
the optical interface and the breast shape. This interface was used to collect multiple
planes of data on a volunteer (data not shown), and MR images showed little change in
breast shape. However, removing a subject from the MR bore is impractical because of
time constraints, and is inconvenient for the subject. Although the slab geometry allows
multiple planes of data to be collected with one fiber plane, an upgrade is vital for larger
clinical studies.
In the clinical case studies presented, MR-guided optical imaging was able to
correctly determine malignancy based on contrast in total hemoglobin, which in one case
was incorrectly diagnosed by MR. Total hemoglobin contrast of known lesions was
shown to be higher than many other optical imaging systems. It is tempting to attribute
this contrast increase to image guidance. However, with this limited dataset, the results
are not significant. Water and oxygenation were found to be inconsistent measures of
malignancy. Although some studies have found these to be positive predictors of
malignancy, others have not. With only six wavelengths, and with the noise levels in this
system, it is quite possible that crosstalk between water and oxyhemoglobin contributed
to the inconsistent results.
183
This crosstalk could be reduced with the incorporation of water quantification
from MR. It was shown that a number of methods could improve the estimate of
hemodynamics by including the water priors. However, a good estimate of the MR
quantification error is important to avoid biasing the reconstruction to incorrect values. It
was shown that even with three wavelengths, the minimum number of wavelengths
needed to recover oxy-, deoxyhemoglobin, and water, the recovered estimate was better
than using six wavelengths below 850nm. This estimate should be improved further in
larger tissue volumes, where data noise will be higher, especially for longer wavelengths.
This technique has important implications for optical imaging, as fewer wavelengths will
help improve the speed of the optical data acquisition.
A faster optical imaging system was implemented to monitor the changes in
breast physiology to respiratory challenge concurrently with BOLD MR. The results
indicate that optical imaging can monitor changes in tissue hemodynamics. These
changes were the most significant and consistent using a respiratory challenge of pure
oxygen and a 95% O2:5% CO2 carbogen mixture. These results also indicate that
carbogen induces vasodilatory changes in breast physiology that have been demonstrated
for other anatomy. This contrast may have the potential to identify vascular structure that
is compromised in tumors, due to the lack of vasomotor control. In two cases, tumors
were shown to respond less than the surrounding healthy tissue, possibly indicating the
poor vascular motor control, characteristic of tumors.
This study also demonstrated the first correlation between optics and BOLD MR,
both in the breast, and using a spin-echo BOLD sequence. These findings have
184
implications for aiding in the validation of BOLD sequences, and for improving optical
imaging by improving temporal resolution.
By including the MR contrasts examined above, a comprehensive MR-guided
optical reconstruction model was developed. This model relaxed the invalid assumption
that deoxy- and oxy-hemoglobin correlate significantly to tissue types segmented in T1W MR. Instead, this model incorporated the results of BOLD-MR to give an estimate of
deoxyhemoglobin. Instead of applying the same T1-W structural map for all parameters,
as had been demonstrated in literature, this model used separate MR images for total
hemoglobin, deoxyhemoglobin, water, and scatter, to spatially separate these contrasts.
This thesis developed tools to better incorporate the various MR contrasts which
correlate to optical contrasts. However, MR also is sensitive to a variety of other tissue
contrasts which have been shown to aid in the characterization of malignant tissue. It is
in the investigation of these new contrasts which optical imaging may have undiscovered
ability aid in image interpretation.
10.2 Future directions
The future of MR-guided optics exists both in the clinical and academic settings.
Clinically, MR-guided optics may be used to provide diagnostic information to identify
disease status. The possibilities of using this combined modality to identify new tumor
contrasts are promising. Academically, optics has been used in conjunction with BOLD
to investigate functional brain activation by a number of research groups. The addition of
critical hemodynamic information derived by optics is compelling. Because it is a
quantitative device, the possibilities of using optics to identify the origins of MR
contrasts is encouraging for the development and validation of new MR methods.
185
10.3 Opportunities in breast MR-optical imaging
10.3.1 Volumetric interface
The major limitation with all medical imaging modalities is the ability to sample the
region of interest. Eclipsing their ability to determine contrast for diagnosis, the biggest
advantage of MR, Computed Tomography (CT), and Positron Emission Tomography
(PET) is the volumetric, non-contact sampling. This allows data acquisition of any
anatomical region. On the other hand, fiber-positioning requisite for optical imaging is
difficult, especially when confined to the MR coil. The most significant limitation is due
to the fact that fibers need to contact the tissue to acquire data because of the enormous
light attenuation in breast imaging. Positioning becomes critical when the region of
interest is not known during patient setup.
There are two strategies to acquiring volumetric optical images in the MR. The
first option is to simply place more optical fibers in the fiber interface. This may allow
multiple planes of fibers to sample the tissue. This strategy is the only option if many
planes of data are needed simultaneously, such as during a respiratory challenge
experiment. However, the added complexity, burden, and expense of adding many fibers
may be prohibitive.
The other strategy is to design a motorized interface that would allow repositioning
of the optical fiber on different planes of the tissue. Besides requiring fewer fibers than
the other option, the added advantage of this strategy is that if the lesion location is not
known a priori (such as during a screening examination), the fiber plane may be moved
to sample a region of interest identified by the MR. However, operating a motor in a
high magnetic field is an engineering challenge. A current investigation is underway at
186
Dartmouth to identify the optimal method to move the fiber plane remotely. This
interface would use either a glass plate or a light fiber guide to couple the optical fibers to
the tissue, so that the tissue would not be distorted during fiber movement.
Although it is a challenging problem, the ability to probe a volume of interest is
the most important aspect to solve before optical imaging may be used in any large-scale
clinical trial or longitudinal study.
10.3.2 Dynamic contrast enhanced MR for higher specificity / blood volume maps
An unexplored direction in combining MR and optical contrasts is to utilize tissue
washout kinetics or blood volume images with dynamic contrast enhanced MR. This
information could be used either to provide a more accurate map of malignancy, or to
provide a spatial or quantitative map to guide the total hemoglobin concentration during
image reconstruction. The following approaches may offer unique opportunities in
multimodality optical/MR imaging.
10.3.2.1 Spatial guidance using washout kinetics
Identification of malignant tumors with dynamic washout kinetics is a standard clinical
tool which has been shown to improve the specificity of breast MR232, 233. Since it offers
improved specificity, it may be beneficial to use this image as a spatial map instead of the
full volume of enhancing tissue. This map is compared to CE subtraction in Figure 10.1.
This approach may help reduce bias in regions of interest.
187
a
b
Figure 10.1: Images from dynamic contrast enhanced MR. (a) Pre-contrast image
subtracted from the 1st dynamic post-contrast image shows clear regions of
enhancement. (b) CADstream (Confirma) image analysis provides spatial maps that
identify possible disease status based on the shape of contrast washout curves.
Regions labelled as green are indicative of benign lesions. Blue signifies an
intermediate between benign and malignant characteristics, and red identifies
kinetics that are suspect malignancy.
10.3.2.2 Imaging blood volume with DSC-MR and DCE-MR
The most established method for blood volume imaging in the MR is to measure the
changes in the rate of transverse NMR relaxation, ΔR2* (DSC-MR), or the change in
longitudinal NMR relaxation rate, ΔR1 (DCE-MR), due to Gadolinium contrast injection.
These techniques have been shown to vary linearly with contrast concentration234. Of
these techniques, T2* weighted sequences are more sensitive to changes in contrast agent
than T1 weighted sequences, although they both provide similar diagnostic
information235.
188
To determine blood volume, changes in signal must be related to changes in blood
volume. Typical models assume that the contrast agent is homogeneously distributed in
the blood - its volume is the blood volume. If changes in signal intensity are solely due
to the effects of the contrast agent, then the concentration of contrast agent in the tissue at
a specific time is measured by: C(t) = ΔR2*. Integrating this curve over time yields the
relative blood volume170, 236. Absolute quantification of blood volume requires
knowledge of the arterial input function (AIF) and necessitates the assumption that
vascular permeability is low, which is false in breast tissue237.
Nevertheless, this method has been applied successfully in the breast. Kuhl et
al.225 found that DSC-MR identified highly dense regions of perfused capillaries in
malignant tumors. Delille et al.226 used a DSC-echo planar imaging (EPI) based
sequence to obtain values for relative blood flow, relative blood volume, and vessel
permeability using a two-compartmental model. This group identified feeding vessels to
obtain local estimates of the AIF to obtain blood flow. In contrast to Kuhl et al., this
study was able to measure relative blood volume in the glandular tissue. This study
showed statistically significant increases in blood volume values in malignant tumors vs
benign and normal tissue.
10.3.2.3 Imaging blood volume Vascular Space Occupancy (VASO)
Absolute blood volume can also be quantified using the Vascular-Space-Occupancy
technique199, as long as the blood volume in a reference tissue is known. Blood volume
is calculated from two blood-nulling T2*-W GE-EPI image sets: one taken before
contrast injection, and one after contrast injection. The T1 relaxation of blood is
shortened by the contrast, and the change in signal is due to the volume of contrast.
189
Similar to DSC/DCE-MR methods, this theory in its current form is invalid in highly
permeable tissue, as the model assumes that contrast agent only affects signal in the
vasculature. An additional concern is the low signal to noise because it acquires data
when much of the signal is nulled - therefore, multiple averages must be used to obtain
sufficient SNR. This technique may still yield valuable information about relative blood
volume, but it has yet to be tested in breast tissue.
10.3.3 Incorporating Diffusion Weighted MR into optical scatter
Diffusion was the first contrast effect observed by Hahn in his seminal paper in 1950238.
Today, diffusion weighted imaging (DWI) is able to measure diffusion coefficients,
which are sensitive to the size and packing density of cellular and vascular structures.
This technique applies equal spatially variant gradients on either side of the slice
selection gradient. Molecules that diffuse into a new region magnetically interact with
surrounding molecules which have different frequencies, and de-phase. Areas with
greater diffusion have lower signal intensities. This technique has been used to identify
breast tumors, where the dense vascular packing impedes motion, providing diffusion
weighted contrast239. This contrast may relate to optical scatter, which is related to
particle size and number density through Mie theory240. A preliminary comparison of a
DWI image241 and optically determined scatter size and number density is given in Figure
10.2. These images were taken of a subject with an invasive ductal carcinoma of the left
breast, who was imaged pre-Gadolinium contrast injection. These images show an
increase in particle number density that corresponds to a decrease in the apparent
diffusion coefficient. If these contrasts could be correlated in a larger population, this
190
spatial map could be incorporated in the model of chapter 9, which could improve the
recovery of optical scatter parameters.
a
b
Figure 10.2: Images of a subject with an invasive ductal carcinoma of the left breast.
The tumor location is given by the arrows. These results show a case where (a)
optically determined particle number density demonstrated spatial similarities to
(b) apparent diffusion coefficient maps derived from DWI MR imaging (SNAILS
sequence, courtesy of Liu et al.241).
10.4 Unanswered questions
The issues of 2D vs 3D and soft priors vs hard priors have been addressed in optical
imaging for a number of years. However, based on the fact that both approaches are
currently in use for each case, these questions have not been adequately solved. The
implications that these choices have on MR-guided optics are discussed below.
191
10.4.1 2D vs 3D
Logically, since the light propagation model in 3D is more accurate than 2D, volumetric
imaging will lead to a smaller data/model misfit than in 2D, which would lead to more
accurate image reconstructions. In practice however, computational considerations
during image reconstruction make this choice less clear.
As discussed more fully in chapter 4, 3D spatially guided reconstructions of
breast tissue can use an enormous amount of memory, even with modest mesh resolution.
Unlike non-image guided schemes, which may reconstruct on a coarse grid, spatial
algorithms encode tissue information into the Hessian. This matrix needs to be inverted,
which is a computationally expensive, and more importantly, memory expensive task.
These memory restrictions may be relieved either by using hybrid methods, as discussed
in chapter 4, or adaptive meshes which are coarse far from tissue boundaries. However,
these techniques may still yield intractable problems. An additional problem with 3D
reconstructions is the increased number of unknowns, which results in more
underdetermined matrices, and often more ill-conditioned matrices. These factors may
reduce the accuracy of parameter recovery.
Because of the competing factors affecting 2D and 3D reconstructions, the choice
in whether to use 2D or 3D in MR guided optics should depend on the application. In
cases where parameters are estimated from an object that is out-of-plane from the fibers,
3D reconstructions are unavoidable. Also, longitudinal studies that monitor the changes
in disease over multiple imaging sessions, such as neoadjuvant chemotherapy monitoring,
should use a 3D approach so that partial volume effects are minimized. On the other
hand, 2D reconstructions are suitable for a number of applications, including dynamic
studies, when changes over time are measured. This approach will be especially accurate
192
if the data is calibrated with an earlier timepoint, as modeling inaccuracies will
eliminated through calibration. Additionally, tumor imaging is suitable in 2D, as long as
the region of interest is adequately sampled, as a number of phantom studies over the past
decade have shown the ability of 2D reconstructions to quantitatively estimate contrasts
with high accuracy.
10.4.2 Soft priors vs Hard priors
Hard priors have been maligned by a number of groups because they are unable to
recover objects that have not been spatially identified a priori. Indeed, if MR-guided
optics were to be used in a screening trial, hard priors would be illogical. In these cases,
soft prior algorithms, which allow a variable degree of variation within a defined region,
are more appropriate.
However, a number of reasons indicate that reconstructing with hard priors might
be a prudent choice. First, because hard priors are usually highly overdetermined,
parameter recovery is less affected by noise. This enables the use of smaller
regularization parameters, which may aid in the recovery of higher contrast. In addition,
this method minimizes the influence of the selection of an arbitrary regularization
parameter which may drastically affect the recovered parameter values. Next, hard priors
are computationally efficient, as they reduce the number of unknowns to a few select
regions. This has important implications in enabling 3D reconstructions. Finally,
although soft-prior algorithms allow contrast variations within tissue types, the spatial
weighting must be input as a parameter into the model. This raises concern over which
values are the most appropriate. Ideally, these parameters would be found by imaging
tissue simulating phantoms. However, these phantoms are constructed of simple
193
geometries; no phantom will ever mimic the complexity of human tissue. Thus, if
disease characterization is to be performed, such as the improvement of MR specificity,
hard priors are the logical choice to recover tissue contrast.
194
APPENDIX A: 3-Dimensional Image Visualization
The visualization of three-dimensional MR guided optical volumes can be misleading if
the display is not handled appropriately. Even though the entire volume is reconstructed,
the sensitivity of the optical detectors to optical contrast decreases rapidly at large
distances from the optical fibers. On the other hand, MRI provides volumetric data
which is sensitive to all tissue in the stack of images. Thus, it is critical to visualize the
optical data appropriately to avoid interpretation errors. In the planar geometries used in
this thesis, sensitivity 1cm above and below the imaging plane is nearly zero. Using this
information, images can be presented in a way that reflects the sensitivity in the data to
the unknowns.
To account for the optical sensitivity, a visualization method can be used which
sets the transparency proportional to the Jacobian, the sensitivity of the measurements to
the tissue. This relation is shown in equations A.1 and A.2 for light amplitude, I, and
phase, φ, respectively, where β is a scaling parameter, and c are the appropriate
parameters. By scaling the transparency to the Jacobian matrix values, tissue properties
far outside the imaging plane will not be displayed and misinterpreted as true contrasts.
(A.1)
(A.2)
An example image is shown in Figure A.1, a case presented in chapter 5. Two
methods are shown to alter the display. In these cases, the transparency of the total
195
hemoglobin was scaled by the natural log of the Jacobian. In Figure A.1d, the
transparency is set to 100% at Jacobian values below a set threshold. This method
removes poorly quantified optical values which may occlude the region of interest. In
Figure A.1e, the transparency was set to 0% at the fibers, and 100% 1 cm above the
center of the domain. Intermediate transparency values were chosen based on equation 1.
Using this approach, transparency may vary according to fiber geometry.
a
b
c
d
e
Figure A.1: 3D visualization example. (a,b) MR images used to segment tissue type
and identify regions of interest. (c) Single slice of a 3D reconstruction in the plane of
the regions of interest. (d) Visualization sets the transparency at 100% at Jacobian
values below a set sensitivity threshold. In this case, the threshold was set at the
Jacobian value 1cm above the center of the imaging plane. (e) An example where the
196
transparency is set at 0% at the fibers, and 100% at sensitivity values which are
lower than the value 1cm above the center of the image volume. The transparency
in these cases is based on the log transform of the Jacobian.
197
APPENDIX B: Generating breast meshes with Mimics
Generating finite element meshes for image-guided reconstructions requires segmentation
tools to separate tissue types, and meshing tools to generate the mesh. This tutorial
highlights how to generate these meshes in 2D and 3D using the software package
Mimics and some in-house meshing tools courtesy of WPI.
B.1 Image Loading / Segmentation
Under the File menu, import the images:
Figure B.1: Image geometry can be imported either by selecting the desired images,
or selecting the parent directory. If the directory is chosen, images will be grouped
into series, based on the DICOM header.
198
Enter the subject orientation, following the geometry in the following figure.
Figure B.2: Geometry reference markers are imported from the MR DICOM
headers, which are based on the MR coil. Often, geometry references are not
included in the DICOM header, so these must be manually specified.
Create a mask of each tissue type via the thresholding button on the toolbar or through
the segmentation menu. Although there is a tool to manually edit multiple slices (from
the segmentation menu), optimal masking will be improved (and faster) by using the
various segmentation tools such as Region growing, Morphology operations, and
Boolean operations; only use manual editing as a last resort!
199
Figure B.3: Grayscale thresholding is the quickest method to segment anatomical
regions, and should be used as a first-step.
Crop the mask to the desired size:
Figure B.4: Masks should be cropped to avoid meshing the abrupt interface between
the breast and the chest wall. This boundary can create sharp edges that are
200
difficult to mesh. Additionally, MR images acquired with a breast coil are less
sensitive to regions beyond the chest wall, because the signal is received from near
the breast. These regions have poor signal to noise, and intensity thresholding is less
accurate. Cropping the mask also helps to remove the fiber fiducials from the image
mask.
Region of interest masks located in other MR image stacks, such as contrast enhanced
MR images, may be saved as .stl files through the Export menu, and imported as stl into
the current project through the File menu. A mask is then created from this stl by using
the Calculate mask from object button.
Figure B.5: Regions of interest segmented from other image stacks, such as dynamic
contrast enhanced MR, can be exported as stl files, and imported into the main
project.
201
B.2 Choosing Reference Points
Place a point at appropriate coordinates using: MedCad > Point > Draw
Export the points in igs format by selecting: MedCad > Export All Objects to IGES
Figure B.6: Fiber positions can be placed using the Medcad menu. These points can
be viewed in the 3 planes, and in 3D. Distances from the tissue to reference fiducial
markers may be determined using the ‘measure distance’ tool.
B.3 Exporting segmented masks
Once masks are segmented, they are exported to meshing software for either 2D or 3D
image computation. It is important to ensure that these masks do not overlap. The
Boolean tool can subtract, unite, or intersect masks.
B.3.1 Meshing in 2D
1. Select the panel in mimics to export.
202
2. Select View > Mask Shade > Binary.
3. Make sure all masks are visible in the 2d plane. It is also important to ensure there
are no holes (uncolored pixels) within the convex hull of the domain in the bitmap,
which will crash the meshing program.
4. Save the masks as bitmap images using Export > BMP. Make sure to select the
correct view (Coronal, Axial, or Sagittal). An example of an exported bitmap is
presented below.
Figure B.7: Bitmap images are used to generate meshes in 2D. Mask shades are
used by NIRFAST meshing software to define region boundaries.
This bitmap can be imported into MATLAB and converted to a NIRFAST mesh via
create2dmesh_from_mimics.m, created by Scott Davis, and modified by Colin Carpenter.
This program can create standard, spectral, or fluorescence meshes.
Routine:
203
create2dmesh_from_mimics.m (Likely the only one you will use. The others are
subroutines)
Subroutines:
nml2nirfast_fluor_2d_from_mimics.m
nml2nirfast_spec_2d_from_mimics.m
nml2nirfast_stnd_2d_from_mimics.m
extract_fibers_from_mimics.m
img2mesh.exe, img2mesh (UNIX executable)
Required Files:
The exported bitmap of the segmented mask
The fiber position file created in mimics
Usage:
Once the above files are created, simply run:
[mesh] = create2dmesh_from_mimics(fn_bmp_img, fn_sd, op_fn, mesh_type, nnodes, pixel_dim)
fn_bmp_img
- the exported segmented bmp from Mimics
fn_sd
- filename of the igs file containing coordinates for the sd-pairs
op_fn
- filename of nirfast mesh to save
mesh_type
- type of nir mesh to save ('fluor' or 'stnd' or 'spec')
nnodes
- desired number of nodes in the mesh
pixel_dim
- pixel dimension in mm (i.e. 0.703)
204
NOTE: Once the mesh has been created, the ordering of the fiber positions (source and
meas files) will need to be manually adjusted to match the optical imaging session. Also,
the link file may need to be manually adjusted to remove any s-d pairs.
Example:
[mesh] = create2dmesh_from_mimics('Example_Coronal.bmp', 'Example_points.igs', 'breast_mesh', ‘spec’,
2000, [0.703])
B.3.2 Meshing in 3D
There are several options for meshing in 3D, as an optimal method has yet to be
determined. The 3D meshing software routines convert files to the correct formats for
the meshing software packages. These routines were created by Aritra Sengupta,
Subhadra Srinivasan, Colin Carpenter, and Tim Monahan. They are contained in a
package of Matlab codes which convert the Mimics surface meshes to volumetric
NIRFAST meshes. These routines were created to allow flexibility for the user to input
any volume meshing tool. Below, meshing using the 3D meshing software ‘spmesh’92,
will be demonstrated.
1. Export the surface mesh as an abacus file through the Export menu.
2. Run the routine mesh3D.
Routine:
mesh3D.m
Subroutines:
205
main.m
convert2nodelem.m
mimicsnml.m
nml2abacus.m
spmesh12.m
spmesh.exe, spmesh (UNIX executable)
Required Files:
The exported surface mesh created from mimics and saved in abacus format (*.inp)
Usage:
Besides the mesh filename, mesh3D has one other input variable, the desired mesh
resolution. The resolution is defined as the average desired distance between nodes, in
mm.
mesh3D(surf_mesh_fn,res)
surf_mesh_fn
- the exported surface mesh from Mimics, in abacus format
res
- the desired mesh resolution, in mm
3. Import the volume mesh, which is saved in abacus format, into Mimics, using the
FEA/CFD menu. Assign material properties to the nodes by selecting FEA/CFD:
206
Figure B.8: Elements material properties are assigned based on the masks. The
desired masks can be chosen through the ‘select masks’ button.
4. Export the volume mesh through the Export>Abacus>Mesh tab. The NIRFAST
mesh is created by running abacus2nirfast.m.
Routine:
abacus2nirfast.m
Subroutines:
ab2nf.c (Although this mex file is not required, it greatly speeds mesh conversion)
Required Files:
The exported volume mesh created from mimics and saved in abacus format (*.inp)
Usage:
[region,mesh] = abacus2nirfast(mesh_fn,fname)
mesh_fn
- the exported volume mesh from Mimics, in abacus format
fname
- the output mesh name
207
5. Create the source detector files with extract_fibers_from_mimics.m
Routine:
extract_fibers_from_mimics.m
Subroutines:
Required Files:
The fiber position file created in mimics
Usage:
[x,y,z] = extract_fibers_from_mimics(filename)
filename
- the fiber position filename
208
APPENDIX C: Re-calibrating PMT amplitude and phase
To ensure the photomultiplier tubes are linear and give the same response for the same
input power, each photomultiplier tube uses a calibration file to convert the raw
amplitude and phase to a calibrated amplitude and phase. These files only need to be
created once. However, since these devices are on a cart that gets jostled during
movement, the amplitude and phase offsets of the photomultiplier tubes need to be
recalibrated every 6 months or so, depending on movement. A program in Labview
rewrites these calibration offsets to easily perform re-calibration. This program was
written by Ben Brooksby and Colin Carpenter. The following steps are required for recalibration.
1. Place a homogeneous phantom in the middle of the circular calibration phantom
holder. MAKE ABSOLUTELY SURE THAT ALL FIBERS ARE TOUCHING
THE PHANTOM. Place a source fiber from the laser diodes onto the top of the
phantom.
209
b
a
c
Figure C.1:(a) Setup for calibration. A laser diode illuminates a homogeneous
cylindrical phantom so that all PMTs have similar intensities. (b) Filter wheels
attenuate input light through the full dynamic range of the PMTs. A circular fiber
interface fixes fiber locations during all measurements.
2. Place the appropriate neutral density filter in the source side to attenuate the source
light so that for each gain setting, input voltages read between 0.3V and 1V (shown in
Figure C.1b). Run the calibration program for each gain setting (shown in Figure
C.2.
210
Figure C.2: The calibration program can be used to create the original calibration
files, or to adjust the pre-existing calibration files. The existing calibration filename
is input in the ‘Calibration File Path’ field, and the output file is saved as the
filename specified in the ‘Calibration File Path 2’ field. At least 30 samples should
211
be selected to average out noise. Each gain setting should be re-calibrated. Make
sure output voltages are between 0.3V and 1V.
212
APPENDIX D: Fiber interface CAD drawings
1. Slab fiber interface:
Figure D.1: Slab system ProE CAD drawings. Dimensions are shown in inches.
2. Calibration fiber interface:
This interface was designed to rigidly fix fibers in position, normal to the inner
surface of the interface. Since fibers cannot be moved in and out, this interface works
for 80-90 mm diameter phantoms only.
213
Figure D.2: Calibration fiber interface used to ensure all fibers are rigidly fixed at
an equal distance from the isocenter of the interface. Measurement units are in
inches.
214
APPENDIX E: List of MATLAB subroutines
Data manipulation, calibration, and reconstruction for typical dataset:
static_recon.m
Data manipulation, calibration, and reconstruction
from start to end for static data
dynamic_recon.m
Data manipulation, calibration, and reconstruction
from start to end for dynamic data
convertspectralmesh.m
Convert NIRFAST V1 mesh to spectral NIRFAST
V3 mesh
convertspectraldata.m
Convert individual wavelength data to spectral
NIRFAST V3 data
remove_data.m
Remove datapoints below noise floor and above
PMT saturation. Returns a spectral, data noise
mesh. The link file has 0’s for fibers that do not
touch, -#’s for s-d pairs where phase should be
dropped, and +#’s for s-d pairs where no data
should be dropped
calibrate_specdata_MR.m
Calibration program for each wavelength for MR
derived meshes. This backwards compatible
program has been modified to accept spectral link
files, which are sized [NSrc x NWv X NDet]
gen_initialguess_spec.m
Generates the initial guess for chromophore
properties based on the homogeneous fitting of each
wavelength.
jacobian_spectral_hardpriors.m
Creates the spectral Jacobian, inserting NaNs into
the datafile where data should be dropped
reconstruct_spectral_hardpriors.m
Hard priors spectral reconstruction modified to
accept spectral and data noise link files
215
reconstruct_spectral_softpriors.m
Soft priors spectral reconstruction modified to
accept spectral and data noise link files
List of algorithms modified to handle data noise:
get_boundary_data.m
calibrate_specdata_MR.m
jacobian_spectral.m
jacobian_spectral_hardpriors.m
reconstruct_spectral_hardpriors.m
reconstruct_spectral_hardpriors.m
reconstruct_spectral_softpriors.m
Assortment of reconstruction algorithms:
reconstruct_spectral_hardpriors.m
Hard priors spectral reconstruction
reconstruct_spectral_softpriors.m
Soft priors spectral reconstruction
reconstruct_spectral_hybrid.m
Hybrid spectral reconstruction
reconstruct_spectral_hardpriors_gls.m
Hard priors GLS formulation
reconstruct_spectral_softpriors_gls.m
Soft priors GLS formulation
reconstruct_spectral_hardpriors_HbHbO.m
Direct water substitution method
reconstruct_spectral_hardpriors_HbHbO_GLS.m Joint Weighted Estimation method
reconstruct_spectral_MM.m
Physiological covariance form
reconstruction, which uses
Jacobian_spectral_hardpiors_MM.m
reconstruct_spectral_hardpriors_FDCW.m
Hard priors reconstruction which
allows reconstruction if an entire
phase dataset for a wavelength needs
216
to be dropped
Various algorithms for display and other miscellaneous functions:
sol2pix.m.m
Interpolate volumetric solution file
and mesh onto 2D slices
sol2pix_and_dicom.m
Interpolate volumetric solution file
onto MR dicom volume and export as
2D slices
convertall2tec.m
Convert volumetric solution file to
data format suitable for importing
into TecPlot
convert2tec_region.m
Convert volumetric mesh region
information to data format suitable
for importing into TecPlot
overlayWF.m
Interpolate water/fat MR images onto
2D NIRFAST mesh
create_L_fast.mex
Mex implementation to calculate the
Laplacian matrix
217
References
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
ACS, American Cancer Society. 2007.
Tabar, L., et al., Mammography service screening and mortality in breast cancer
patients: 20-year follow-up before and after introduction of screening. Lancet,
2003. 361(9367): p. 1405-10.
Salzmann, P., K. Kerlikowske, and K. Phillips, Cost-Effectiveness of Extending
Screening Mammography Guidelines To Include Women 40 to 49 Years of Age.
Annals of Internal Medicine, 1997. 127(11): p. 955-965.
Elmore, J., et al., Ten-Year Risk of False Positive Screening Mammograms and
Clinical Breast Examinations. NE Journal of Medicine, 1998. 338(16): p. 10891096.
Berg, W., et al., Combined screening with ultrasound and mammography vs
mammography alone in women at elevated risk of breast cancer. JAMA-Journal
of the American Medical Association, 2008. 299(18): p. 2151-2163.
Lehman, C., et al., Cancer yield of mammography, MR, and US in high-risk
women: prospective multi-institution breast cancer screening study. Radiology,
2007. 244(2): p. 381-8.
Jackson, V., et al., Imaging of the radiographically dense breast. Radiology,
1993. 188: p. 297-301.
Kuhl, C., The Current Status of Breast MR Imaging Part I, Choice of Technique,
Image Interpretation, Diagnostic Accuracy, and Transfer to Clinical Practice.
Radiology, 2007. 244(2).
Kneeshaw, P.J., L.W. Turnbull, and P.J. Drew, Current applications and future
direction of MR mammography. British Journal of Cancer, 2003(88): p. 4-10.
Folkman, J., et al., Tumor Angiogenesis - Therapeutic Implications. New England
Journal of Medicine, 1971. 285(21): p. 1182-&.
Vaupel, P., F. Kallinowski, and P. Okunieff, Blood Flow, Oxygen and Nutrient
Supply, and Metabolic Microenviroment of Human Tumors: A Review. Cancer
Research, 1989. 49: p. 6449-6465.
Orel, S.G. and M. Schnall, MR Imaging of the Breast for Detection, Diagnosis,
and Staging of Breast Cancer. Radiology, 2001. 220: p. 13-30.
Bluemke, D., et al., Magnetic Resonance Imaging of the Breast Prior to Biopsy.
JAMA-Journal of the American Medical Association, 2004. 292(22).
Kuhl, C.K., Current status of breast MR imaging - Part 2. Clinical applications.
Radiology, 2007. 244(3): p. 672-691.
Kuhl, C.K., et al., Breast MR imaging screening in 192 women proved or
suspected to be carriers of a breast cancer susceptibility gene: Preliminary
results. Radiology, 2000. 215(1): p. 267-279.
Guo, Y., et al., Differentiation of clinically benign and malignant breast lesions
using diffusion-weighted imaging. Journal of Magnetic Resonance Imaging, 2002.
16(2): p. 172-178.
218
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
Katz-Brull, R., P.T. Lavin, and R.E. Lenkinski, Clinical utility of proton magnetic
resonance spectroscopy in characterizing breast lesions. Journal of the National
Cancer Institute, 2002. 94(16): p. 1197-1203.
Ntziachristos, V., X.H. Ma, and B. Chance, Time-correlated single photon
counting imager for simultaneous magnetic resonance and near-infrared
mammography. Review of Scientific Instruments, 1998. 69(12): p. 4221-4233.
Brooksby, B., et al., Magnetic Resonance-Guided Near-Infrared Tomography of
the Breast. Rev. Sci. Instr., 2004. 75(12): p. 5262-5270.
Sinkus, R., et al., MR elastography of breast lesions: Understanding the
solid/liquid duality can improve the specificity of contrast-enhanced MR
mammography. Magnetic Resonance in Medicine, 2007. 58(6): p. 1135-1144.
Chance, B., et al., Breast Cancer Detection Based on Incremental Biochemical
and physiological Properties of Breast Cancers: A Six-Year, Two-Site Study.
Academic Radiology, 2005. 12(8): p. 925-933.
Poplack, S.P., et al., Electromagnetic Breast Imaging: Results of a Pilot Study in
Women with Abnormal Mammograms. Radiology, 2007. 243(2).
Srinivasan, S., et al., Near-Infrared Characterization of Breast Tumors In-Vivo
using Spectrally-Constrained Reconstruction. Tech. Cancer Res. Treat., 2005.
4(5): p. 513-526.
Pogue, B.W., et al., Quantitative Hemoglobin Tomography with Diffuse NearInfrared Spectroscopy: Pilot Results in the Breast. Radiology, 2001. 218(1): p.
261-6.
Cerussi, A., et al., In vivo absorption, scattering, and physiologic properties of 58
malignant breast tumors determined by broadband diffuse optical spectroscopy.
Journal of Biomedical Optics, 2006. 11(4).
Fantini, S., Walker, S. A., Franceschini, M. A., Kaschke, M., Schlag, P. M.,
Moesta, K. T., Assessment of the size, position, and optical properties of breast
tumors in vivo by noninvasive optical methods. Appl. Opt., 1998. 37(10): p. 198289.
Grosenick, D., et al., Concentration and oxygen saturation of haemoglobin of 50
breast tumours determined by time-domain optical mammography. Phys. Med.
Biol., 2004. 47(9): p. 1165-1181.
Benjamin, L.E., et al., Selective ablation of immature blood vessels in established
human tumors follows vascular endothelial growth factor withdrawal. Journal of
Clinical Investigation, 1999. 103(2): p. 159-165.
Connolly, D.T., et al., Tumor Vascular-Permeability Factor Stimulates
Endothelial-Cell Growth and Angiogenesis. Journal of Clinical Investigation,
1989. 84(5): p. 1470-1478.
Jain, R.K., Barriers to drug delivery in solid tumors. [Review]. Scientific
American, 1994. 271(1): p. 58-65.
Wilson, B.C. and M.S. Patterson, The physics, biophysics and technology of
photodynamic therapy. Physics in Medicine and Biology, 2008. 53(9): p. R61R109.
Culver, J.P., et al., Three-dimensional diffuse optical tomography in the parallel
plane transmission geometry: evaluation of a hybrid frequency
219
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
domain/continuous wave clinical system for breast imaging. Medical Physics,
2003. 30(2): p. 235-47.
Ntziachristos, V., et al., MRI-guided diffuse optical spectroscopy of malignant
and benign breast lesions. Neoplasia, 2002. 4(4): p. 347-54.
Brooksby, B., et al., Combining near infrared tomography and magnetic
resonance imaging to study in vivo breast tissue: implementation of a Laplaciantype regularization to incorporate MR structure. J. Biomed. Opt., 2005. 10(5): p.
050504-1-10.
Intes, X., et al., Diffuse optical tomography with physiological and spatial a
priori constraints. Phys. Med. Biol., 2004. 49: p. N155-N163.
Li, A., et al., Tomographic optical breast imaging guided by three-dimensional
mammography. Applied Optics, 2003. 42(25): p. 5181-5190.
Yalavarthy, P.K., et al., Structural information within regularization matrices
improves near infrared diffuse optical tomography. Optics Express, 2007. 15(13).
Patterson, M.S., B. Chance, and B.C. Wilson, Time Resolved Reflectance and
Transmittance for the Noninvasive Measurement of Tissue Optical-Properties.
Applied Optics, 1989. 28(12): p. 2331-2336.
Sevick, E.M., et al., Quantitation of time- and frequency-resolved optical spectra
for the determination of tissue oxygenation. Analytical Biochemistry, 1991.
195(2): p. 330-51.
Patterson, M.S., Moulton, J. D., Wilson, B. C., Berndt, K. W., Lakowicz, J. R.,
Frequency-domain reflectance for the determination of the scattering and
absorption properties of tissue. Appl. Opt., 1991. 30(24): p. 4474-4476.
Gratton, E., et al., A novel approach to laser tomography. Bioimaging, 1993. 1: p.
40-46.
Hebden, J.C., S.R. Arridge, and D.T. Delpy, Optical imaging in medicine: I.
Experimental techniques. Physics in Medicine & Biology, 1997. 42(5): p. 825-40.
McBride, T.O., et al., A parallel-detection frequency-domain near-infrared
tomography system for hemoglobin imaging of the breast in vivo. Review of
Scientific Instruments, 2001. 72(3): p. 1817-1824.
Jiang, S., et al., Measurement of pressure-displacement kinetics of hemoglobin in
normal breast tissue with near-infrared spectral imaging. Applied Optics, 2009.
48(10): p. D130-D136.
Brooksby, B., Combined near-infrared tomography and MRI to improve breast
tissue chromophore and scattering assessment, in Engineering. 2005, Dartmouth
College: Hanover NH. p. 228.
Suess, M.J., Development of a Long-Term Program on Nonionizing Radiation
Protection. Health Physics, 1974. 27(5): p. 514-522.
Yalavarthy, P., A Generalized Least-Squares Estimation Minimization Method for
Near Infrared Diffuse Optical Tomgraphy, in Thayer School of Engineering.
2007, Dartmouth College: Hanover, NH.
Pogue, B.W., et al., Comparison of imaging geometries for diffuse optical
tomography of tissue. Opt. Exp., 1999. 4(8): p. 270-286.
Ojeda-Fournier, H., K.A. Choe, and M.C. Mahoney, Recognizing and interpreting
artifacts and pitfalls in MR imaging of the breast. Radiographics, 2007. 27: p.
S147-S164.
220
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
Lufkin, R.B., et al., Solenoid Surface Coils in Magnetic-Resonance-Imaging.
American Journal of Roentgenology, 1986. 146(2): p. 409-412.
Eker, C., Optical Characterization of Tissue for Medical Diagnosis. PhD Thesis,
Department of Physics, Lund Institute of Technology, 1999.
Prahl, S.A., Oregon Medical Laser Center Website.
Cerussi, A.E., et al., Spectroscopy enhances the information content of optical
mammography. Journal of Biomedical Optics, 2002. 7(1): p. 60-71.
Ishimaru, A., Diffusion of light in turbid material. Appl. Opt., 1989. 28: p. 22102215.
Arridge, S.R., et al., A Finite-Element Approach for Modeling Photon Transport
in Tissue. Medical Physics, 1993. 20(2): p. 299-309.
Haskell, R.C., et al., Boundary conditions for the diffusion equation in radiative
transfer. J. Opt. Soc. Am. A, 1994. 11(10): p. 2727-2741.
Kienle, a. and M.S. Patterson, Improved solutions of the steady-state and the timeresolved diffusion equations for reflectance from a semi-infinite turbid medium.
Journal of the Optical Society of America a-Optics Image Science and Vision,
1997. 14(1): p. 246-254.
Arridge, S.R. and J.C. Hebden, Optical imaging in medicine: II. Modelling and
reconstruction. Physics in Medicine & Biology, 1997. 42(5): p. 841-53.
Aronson, R., Boundary-conditions for diffusion of light. J. Opt. Soc. Am. A, 1995.
12(11): p. 2532-2539.
Jiang, H., Paulsen K. D., Osterberg, U. L., Pogue, B. W., Patterson, M. S., Optical
image reconstruction using frequency-domain data: simulations and experiments.
J. Opt. Soc. Am. A, 1996. 13(2): p. 253-266.
Paulsen, K.D., and Jiang H., Spatially varying optical property reconstruction
using a finite element diffusion equation approximation. Med. Phys., 1995. 22(6):
p. 691-701.
Paulsen, K.D., et al., A Dual Mesh Scheme for Finite-Element Based
Reconstruction Algorithms. Ieee Transactions on Medical Imaging, 1995. 14(3):
p. 504-514.
Lynch, D., Numerical Partial Differential Equations for Environmental Scientists
and Engineers: a first practical course. 2005, New York: Springer.
Rieke, G., Detection of Light from the Ultraviolet to the Submillimeter. 2 ed.
2003, Cambridge, UK: Cambridge University Press.
Kaipio, J.P., et al., Inverse problems with structural prior information. Inverse
Problems, 1999. 15(3): p. 713-729.
Arridge, S.R., Schweiger, M., Inverse methods for optical tomography, in
Information Processing in Medical Imaging, A.F.G. H.H. Barrett, Editor. 1993,
Springer-Verlag: Flagstaff, AZ. p. 259-277.
Yalavarthy, P.K., et al., Weight-Matrix Structured Regularization Provides
Optical Generalized Least-Squares Estimate in Diffuse Optical Tomography.
Medical Physics, 2007. 34(6).
Arridge, S.R., Photon-Measurement Density-Functions.1. Analytical Forms.
Applied Optics, 1995. 34(31): p. 7395-7409.
Arridge, S.R. and M. Schweiger, Photon-measurement density functions. Part 2:
Finite-element-method calculations. Appl. Opt., 1995. 34: p. 8026-8037.
221
70.
71.
72.
73.
74.
75.
76.
77.
78.
79.
80.
81.
82.
83.
84.
85.
Corlu, A., et al., Diffuse optical tomography with spectral constraints and
wavelength optimization. Applied Optics, 2005. 44(11): p. 2082-93.
Li, A., et al., Reconstructing chromosphere concentration images directly by
continuous-wave diffuse optical tomography. Optics Letters, 2004. 29(3).
Srinivasan, S., et al., Spectrally Constrained Chromophore and Scattering NIR
Tomography Improves Quantification and Robustness of Reconstruction. Appl.
Opt., 2004. 44(10): p. 1858-1869.
Tikhonov, A. and V. Arsenin, Solutions of Ill-Posed Problems. Scripta series in
mathematics. 1977, New York: WH Winston & Sons.
Marquardt, D.W., An Algorithm for Least-Squares Estimation of Nonlinear
Parameters. Journal of the Society for Industrial and Applied Mathematics, 1963.
11(2): p. 431-441.
Li, C., et al., Using a priori structural information from magnetic resonance
imaging to investigate the feasibility of prostate diffuse optical tomography and
spectroscopy: A simulation study. Medical Physics, 2007. 34(1).
Dehghani, H., et al., Breast deformation modeling for image reconstruction in
near-infrared tomography. Phys. Med. Biol., 2004. 49: p. 1131-1145.
Ntziachristos, V., et al., Concurrent MRI and diffuse optical tomography of breast
after indocyanine green enhancement. Proceedings of the National Academy of
Sciences of the United States of America, 2000. 97(6): p. 2767-72.
Zhang, X., V. Toronov, and A. Webb, Simultaneous integrated diffuse optical
tomography and functional magnetic resonance imaging of the human brain.
Optics Express, 2005. 13(14): p. 5513-5521.
Guven, M., et al., Diffuse optical tomography with a priori anatomical
information. Physics in Medicine and Biology, 2005. 12: p. 2837-2858.
Chang, J., Graber, H. L., Koo, P. C., Aronson, R., Barbour, S. S., Barbour, R. L.,
Optical imaging of anatomical maps derived from magnetic resonance images
using time independent optical sources. IEEE Trans. Med. Imag., 1997. 16: p. 6877.
Brooksby, B., et al., Near infrared (NIR) tomography breast image reconstruction
with a priori structural information from MRI: algorithm development for
reconstructing heterogeneities. IEEE J. STQE, 2003. 9(2): p. 199-209.
Schweiger, M. and S.R. Arridge, Optical tomographic reconstruction in a
complex head model using a priori region boundary information. Physics in
Medicine & Biology, 1999. 44(11): p. 2703-21.
Boas, D. and A. Dale, Simulation study of magnetic resonance imaging-guided
cortically constrained diffuse optical tomography of the human brain function.
Applied Optics, 2005. 44(10).
Pogue, B.W., Zhu, H., Nwaigwe, C., McBride, T. O., Osterberg, U. L., Paulsen,
K. D., Dunn, J. F., Hemoglobin Imaging With Hybrid Magnetic Resonance and
Near-Infrared Diffuse Tomography. Adv. Expt. Med. Biol., 2003. 530: p. 215224.
Pogue, B.W. and K.D. Paulsen, High-resolution near-infrared tomographic
imaging simulations of the rat cranium by use of a priori magnetic resonance
imaging structural information. Optics Letters, 1998. 23(21): p. 1716.
222
86.
87.
88.
89.
90.
91.
92.
93.
94.
95.
96.
97.
98.
99.
100.
101.
102.
Boverman, G., et al., Quantitative spectroscopic diffuse optical tomography of the
breast guided by imperfect a priori structural information. Physics in Medicine
and Biology, 2005. 50: p. 3941-3956.
Barbour, R.L., et al., MRI-Guided Optical Tomography: Prospects and
Computation for a New Imaging Method. IEEE Comp. Sci. Eng., 1995. 2: p. 6377.
Brooksby, B., et al., Spectral-prior information improves Near-Infrared diffuse
tomography more than spatial-prior. Opt. Lett., 2005. 30(15): p. 1968-1970.
Brooksby, B., et al., Imaging Breast Adipose and Fibroglandular Tissue
Molecular Signatures using Hybrid MRI-Guided Near-Infrared Spectral
Tomography. Proc. Nat. Acad. Sci. USA, 2006. 103: p. 8828-8833.
Carpenter, C.M., et al., Image-guided spectroscopy provides molecular specific
information in vivo: MRI-guided spectroscopy of breast cancer hemoglobin,
water, and scatterer size. Optics Letters, 2007. 32(8): p. 933-935.
Zhang, J., et al. Image-guided multimodality registration and visualization for
breast cancer detection. in SPIE. 2005.
Wu, Z. and J. Sullivan. Automatic finite element mesh generation from MRI scans
for breast cancer investigations. in Proceedings of the IEEE 27t Annual Northeast
Bioengineering Conference. 2001. Storrs, CT, USA.
Wu, Z. and J. Sullivan, Multiple material marching cubes algorithm. International
Journal for Numerical Methods in Engineering, 2003. 58(2): p. 189-207.
Dehghani, H., et al., Three-dimensional optical tomography: resolution in smallobject imaging. Applied Optics, 2003. 42(16): p. 3117-28.
Hua, P., J. Webster, and W. Tompkins, A regularised electrical impedence
tomography reconstruction algorithm. Clinical Physics and Physiological
Measurement, 1988. 9(A): p. 137-141.
Borsic, A., Regularisation Methods for Imaging from Electrical Measurements, in
School of Engineering. 2002, Oxford Brookes University.
Biyikoglu, T., J. Leydold, and P.F. Stadler, Laplacian Eigenvectors of Graphs Perron-Frobenius and Faber-Krahn type theorems. Laplacian Eigenvectors of
Graphs, 2007. 1915: p. 1-+.
Fantini, S., et al., Assessment of the size, position, and optical properties of breast
tumors in vivo by noninvasive optical methods. Applied Optics, 1998. 37(10): p.
1982-1989.
Grosenick, D., et al., Time-domain scanning optical mammography: I. Recording
and assessment of mammograms of 154 patients. Physics in Medicine and
Biology, 2005. 50(11): p. 2429-2449.
Intes, X., Time-Domain Optical Mammography SoftScan Initial Results.
Academic Radiology, 2005. 12(8): p. 934-947.
Choe, R., et al., Differentiation of benign and malignant breast lesions by in-vivo
three-dimensional diffuse optical tomography. Cancer Research, 2009. 69(2): p.
102S-102S.
Zhu, Q., et al., Benign versus malignant breast masses: Optical differentiation
with US-guided optical imaging reconstruction. Radiology, 2005. 237(1).
223
103.
104.
105.
106.
107.
108.
109.
110.
111.
112.
113.
114.
115.
116.
Choe, R., et al., Diffuse optical tomography of breast cancer during neoadjuvant
chemotherapy: A case study with comparison to MRI. Medical Physics, 2005.
32(4): p. 1128-1139.
Cerussi, A., et al., Predicting response to neoadjuvant chemotherapy using diffuse
optical spectroscopy. PNAS, 2007. 104(10).
Jiang, S., et al., Evaluating tumor response to neoadjuvant chemotherapy with
Diffuse Optical Spectroscopic Tomography: Case studies of tumor Region of
Interest changes. Radiology, 2009. In press.
Fang, Q.Q., et al., Combined Optical Imaging and Mammography of the Healthy
Breast: Optical Contrast Derived From Breast Structure and Compression. Ieee
Transactions on Medical Imaging, 2009. 28(1): p. 30-42.
Gulsen, G., et al., Combined Diffuse Optical Tomography (DOT) and MRI System
for Cancer Imaging in Small Animals. Technology in Cancer Research &
Treatment, 2006. 5(4).
Xu, H., et al., Magnetic-resonance-imaging–coupled broadband near-infrared
tomography system for small animal brain studies. Appl. Opt., 2005. 44(10): p.
2177-2188.
Spinelli, L., et al., Characterization of female breast lesions from multiwavelength time-resolved optical mammography. Physics in Medicine and
Biology, 2005. 50(11): p. 2489-2502.
Fisher, B., et al., Effect of preoperative chemotherapy on the outcome of women
with operable breast cancer. Journal of Clinical Oncology, 1998. 16(8): p. 26722685.
Mauri, D., N. Pavlidis, and J.P.A. Ioannidis, Neoadjuvant versus adjuvant
systemic treatment in breast cancer: A meta-analysis. Journal of the National
Cancer Institute, 2005. 97(3): p. 188-194.
Fisher, B., et al., Effect of preoperative chemotherapy on local-regional disease in
women with operable breast cancer: Findings from National Surgical Adjuvant
Breast and Bowel Project B-18. Journal of Clinical Oncology, 1997. 15(7): p.
2483-2493.
Loo, C.E., et al., Dynamic Contrast-Enhanced MRI for Prediction of Breast
Cancer Response to Neoadjuvant Chemotherapy: Initial Results. American
Journal of Roentgenology, 2008. 191(5): p. 1331-1338.
Yu, H.J., et al., MRI measurements of tumor size and pharmacokinetic parameters
as early predictors of response in breast cancer patients undergoing Neoadjuvant
anthracycline chemotherapy. Journal of Magnetic Resonance Imaging, 2007.
26(3): p. 615-623.
Sharma, U., et al., Longitudinal study of the assessment by MRI and diffusionweighted imaging of tumor response in patients with locally advanced breast
cancer undergoing neoadjuvant chemotherapy. Nmr in Biomedicine, 2009. 22(1):
p. 104-113.
Meisamy, S., et al., Neoadjuvant chemotherapy of locally advanced breast
cancer: Predicting response with in vivo H-1 MR spectroscopy - A pilot study.
Radiology, 2004. 233(2): p. 424-431.
224
117.
118.
119.
120.
121.
122.
123.
124.
125.
126.
127.
128.
129.
130.
131.
132.
133.
134.
Manton, D.J., et al., Neoadjuvant chemotherapy in breast cancer: early response
prediction with quantitative MR imaging and spectroscopy. British Journal of
Cancer, 2006. 94(3): p. 427-435.
Padhani, a.R., et al., Prediction of clinicopathologic response of breast cancer to
primary chemotherapy at contrast-enhanced MR imaging: Initial clinical results.
Radiology, 2006. 239(2): p. 361-374.
Drew, P.J., et al., Evaluation of response to neoadjuvant chemoradiotherapy for
locally advanced breast cancer with dynamic contrast-enhanced MRI of the
breast. European Journal of Surgical Oncology, 2001. 27(7): p. 617-620.
Rieber, a., et al., Breast MRI for monitoring response of primary breast cancer to
neo-adjuvant chemotherapy. European Radiology, 2002. 12(7): p. 1711-1719.
Abraham, D.C., et al., Evaluation of neoadjuvant chemotherapeutic response of
locally advanced breast cancer by magnetic resonance imaging. Cancer, 1996.
78(1): p. 91-100.
Corlu, A., et al., Uniqueness and wavelength optimization in continuous-wave
multispectral diffuse optical tomography. Optics Letters, 2003. 28(23): p. 233941.
Franceschini, M., et al., Quantitative Spectroscopic Determination of Hemoglobin
Concentration and Saturation in a Turbid Medium: Analysis of the Effect of
Water Absorption. Journal of Biomedical Optics, 1997. 2(2): p. 147-153.
McBride, T.O., et al., Multispectral near-infrared tomography: a case study in
compensating for water and lipid content in hemoglobin imaging of the breast.
Journal of Biomedical Optics, 2002. 7(1): p. 72-9.
Li, A., et al., Optical linear inverse solution with multiple priors in diffuse optical
tomography. Applied Optics, 2005. 44(10).
Bydder, G., et al., The short TI inversion recovery sequence -- an approach to MR
imaging of the abdomen. Magnetic Resonance Imaging, 1985. 3(3): p. 251-254.
Meyer, C.H., et al., Simultaneous Spatial and Spectral Selective Excitation.
Magnetic Resonance in Medicine, 1990. 15(2): p. 287-304.
Delfaut, E.M., et al., Fat suppression in MR imaging: Techniques and pitfalls.
Radiographics, 1999. 19(2): p. 373-382.
Kuhl, C.K., et al., Effect of B-1 inhomogeneity on breast imaging at 3.0 T.
Radiology, 2007. 244(3): p. 929-930.
Harvey, J.A., et al., Breast MR imaging artifacts: How to recognize and fix them.
Radiographics, 2007. 27: p. S131-S145.
DIxon, W., Simple Proton Spectroscopic Imaging. Radiology, 1984. 153: p. 189194.
Glover, G.H. and E. Schnieder, Three-point dixon technique for true water/fat
decomposition with B0 inhomogeneity correction. Magnetic Resonance in
Medicine, 1991. 18(2).
Graham, S.J., et al., Changes in fibroglandular volume and water content of
breast tissue during the menstrual cycle observed by MR imaging at 1.5 T.
Journal of Magnetic Resonance Imaging, 1995. 5(6): p. 695-701.
Reeder, S., et al., Multi-coil Dixon chemical species separation with an iterative
least squares method. Magnetic Resonance in Medicine, 2004. 51.
225
135.
136.
137.
138.
139.
140.
141.
142.
143.
144.
145.
146.
147.
148.
149.
150.
151.
Guiu, B., et al., Multiecho MR Imaging and Proton MR Spectroscopy for Liver
Fat Quantification. Radiology, 2008. 249(3): p. 1081-1081.
Hu, H. and K. Nayak, Quantification of Absolute Fat Mass Using an Adipose
Tissue Reference Signal Model. Journal of Magnetic Resonance Imaging, 2008.
28: p. 1483-1491.
Bernard, C.P., et al., Comparison of fat quantification methods: A phantom study
at 3.0T. Journal of Magnetic Resonance Imaging, 2008. 27(1): p. 192-197.
Liang, Z. and P. Lauterbur, Principles of Magnetic Resonance Imaging A Signal
Processing Perspective. IEEE Press Series in Biomedical Engineering, ed. M.
Akay. 2000, New York: IEEE Press.
van Veen, R., et al. Determination of VIS-NIR absorption coefficients of
mammalian fat, with time- and spatially resolved diffuse reflectance and
transmission spectroscopy. in OSA Annual BIOMED Topical Meeting. 2004.
Merritt, S., et al., Comparison of Water and Lipid Content Measurements Using
Diffuse Optical Spectroscopy and MRI in Emulsion Phantoms. Technology in
Cancer Research & Treatment, 2003. 2(6).
Merritt, S., Combination of Broadband Diffuse Optical Spectroscopy with
Magnetic Resonance Imaging, in Physics. 2005, Univerity of California, Irvine.
Chung, S.H., et al., In vivo water state measurements in breast cancer using
broadband diffuse optical spectroscopy. Physics in Medicine and Biology, 2008.
53(23): p. 6713-6727.
Chung, S.H., Unnormalized Gelatin Spectra, C.M. Carpenter, Editor. 2008. p.
Full spectrum of gelatin containing bound water from 650-1000nm.
McBride, T.O., et al., Strategies for absolute calibration of near infrared
tomographic tissue imaging. Advances in Experimental Medicine & Biology,
2003. 530: p. 85-99.
Eames, M. and H. Dehghani, Wavelength Dependence of Sensitivity in Spectral
Diffuse Optical Tomographic Imaging: Effect of Normalization on Image
Reconstruction. Optics Express, 2008. 16(22): p. 17780.
Pogue, B.W. and M.S. Patterson, Review of tissue simulating phantoms for optical
spectroscopy, imaging and dosimetry. Journal of Biomedical Optics, 2006. 11(4):
p. -.
Wang, J., et al., Spectral tomography with diffuse near-infrared light: inclusion of
broadband frequency domain spectral data. Journal of Biomedical Optics, 2008.
13(4): p. -.
Carmeliet, P., Angiogenesis in health and disease. Nature Medicine, 2003. 9(6): p.
653-660.
Gilad, A.A., et al., Functional and molecular mapping of uncoupling between
vascular permeability and loss of vascular maturation in ovarian carcinoma
xenografts: The role of stroma cells in tumor angiogenesis. International Journal
of Cancer, 2005. 117(2): p. 202-211.
Dische, S., What Have We Learnt from Hyperbaric-Oxygen. Radiotherapy and
Oncology, 1991. 20: p. 71-74.
Rojas, a., et al., Effect of Anemia on Tumor Radiosensitivity under Normo and
Hyperbaric Conditions. International Journal of Radiation Oncology Biology
Physics, 1987. 13(11): p. 1681-1689.
226
152.
153.
154.
155.
156.
157.
158.
159.
160.
161.
162.
163.
164.
165.
166.
167.
168.
Nordsmark, M., et al., Prognostic value of tumor oxygenation in 397 head and
neck tumors after primary radiation therapy. An international multi-center study.
Radiotherapy and Oncology, 2005. 77(1): p. 18-24.
Evans, N.T.S. and P.F.D. Naylor, The Effect of Oxygen Breathing and
Radiotherapy Upon the Tissue Oxygen Tension of Some Human Tumours. British
Journal of Radiology, 1963. 36(426): p. 418-425.
Martin, L., et al., Changes in the Oxygenation of Head and Neck Tumors during
Carbogen Breathing. Radiotherapy and Oncology, 1993. 27(2): p. 123-130.
Henk, J.M., Late Results of a Trial of Hyperbaric-Oxygen and Radiotherapy in
Head and Neck-Cancer - a Rationale for Hypoxic Cell Sensitizers. International
Journal of Radiation Oncology Biology Physics, 1986. 12(8): p. 1339-1341.
Frank, H., et al., Efficacy of thrombolytic therapy in pulmonary embolism
determined by MION-enhanced MRA: an experimental study in rabbits.
Investigative Radiology., 1998. 33(12): p. 853-7.
Foster, T.H. and L. GAO, Dosimetry in Photodynamic Therapy - Oxygen and the
Critical Importance of Capillary Density. Radiation Research, 1992. 130(3): p.
379-383.
Dische, S., et al., Carcinoma of the cervix and the use of hyperbaric oxygen with
radiotherapy: a report of a randomised controlled trial. Radiotherapy and
Oncology, 1999. 53(2): p. 93-98.
Abramovitch, R., et al., In vivo prediction of vascular susceptibility to vascular
endothelial growth factor withdrawal: Magnetic resonance imaging of C6 rat
glioma in nude mice. Cancer Research, 1999. 59(19): p. 5012-5016.
Brown, S., W. Miller, and J. Eason, Exercise Physiology: Basis of Human
Movement in Health and Disease. 2006: Lippincott Williams & Wilkins.
Guyton, A. and J. Hall, Textbook of Medical Physiology. 11 ed. 2006: Elsevier.
Busse, R., G. Trogisch, and E. Bassenge, The Role of Endothelium in the Control
of Vascular Tone. Basic Research in Cardiology, 1985. 80(5): p. 475-490.
Thews, O., D.K. Kelleher, and P. Vaupel, Dynamics of tumor oxygenation and
red blood cell flux in response to inspiratory hyperoxia combined with different
levels of inspiratory hypercapnia. Radiotherapy and Oncology, 2002. 62(1): p.
77-85.
West, J., Respiratory Physiology: The Essentials. Vol. 8. 2008: Lippincott
Williams & Wilkins. 171.
Eggers, G.W.N., et al., Hemodynamic Responses to Oxygen Breathing in Man.
Journal of Applied Physiology, 1962. 17(1): p. 75-&.
Floyd, T.F., et al., Independent cerebral vasoconstrictive effects of hyperoxia and
accompanying arterial hypocapnia at 1 ATA. Journal of Applied Physiology,
2003. 95(6): p. 2453-2461.
Berkowitz, B.A., Adult and newborn rat inner retinal oxygenation during
carbogen and 100% oxygen breathing - Comparison using magnetic resonance
imaging Delta P-O-2 mapping. Investigative Ophthalmology & Visual Science,
1996. 37(10): p. 2089-2098.
Ashkanian, M., et al., Improvement of Brain Tissue Oxygenation by Inhalation of
Carbogen. Neuroscience, 2008. 156(4): p. 932-938.
227
169.
170.
171.
172.
173.
174.
175.
176.
177.
178.
179.
180.
181.
182.
183.
184.
O'Connor, J., et al., Organ-Specific Effects of Oxygen and Carbogen Gas
Inhalation on Tissue Longitudinal Relaxation Times. Magnetic Resonance in
Medicine, 2007. 58: p. 490-496.
Axel, L., Cerebral Blood-Flow Determination by Rapid-Sequence ComputedTomography - a Theoretical-Analysis. Radiology, 1980. 137(3): p. 679-686.
Brischetto, M.J., et al., Effect of Aging on Ventilatory Response to Exercise and
Co2. Journal of Applied Physiology, 1984. 56(5): p. 1143-1150.
Kuo, T.B.J., et al., Frequency domain analysis of cerebral blood flow velocity and
its correlation with arterial blood pressure. Journal of Cerebral Blood Flow and
Metabolism, 1998. 18(3): p. 311-318.
Yan, L., et al., Physiological Origin of Low-Frequency Drift in Blood Oxygen
Level Dependent (BOLD) Functional Magnetic Resonance Imaging (fMRI).
Magnetic Resonance in Medicine, 2009. 61: p. 819-827.
Wilson, C.B.J.H., et al., Measurements of Blood-Flow and Exchanging Water
Space in Breast-Tumors Using Positron Emission Tomography - a Rapid and
Noninvasive Dynamic Method. Cancer Research, 1992. 52(6): p. 1592-1597.
Powell, M.E.B., et al., Human tumor blood flow is enhanced by nicotinamide and
carbogen breathing. Cancer Research, 1997. 57(23): p. 5261-5264.
Alonzi, R., et al., Carbogen breathing increases prostate cancer oxygenation: a
translational MRI study in murine xenografts and humans. British Journal of
Cancer, 2009. 100(4): p. 644-648.
Kruuv, J.a., W.R. Inch, and J.a. Mccredie, Blood Flow and Oxygenation of
Tumors in Mice.3. Effects of Breathing Amyl Nitrite in Oxygen on Radiosensitivity
of C3H Tumor. Cancer, 1967. 20(1): p. 66-&.
Kim, J.G., et al., Interplay of tumor vascular oxygenation and tumor pO(2)
observed using near-infrared spectroscopy, an oxygen needle electrode, and F-19
MR pO(2) mapping. Journal of Biomedical Optics, 2003. 8(1): p. 53-62.
Hoskin, P.J., et al., Inspired and expired gas concentrations in man during
carbogen breathing. Radiotherapy and Oncology, 1999. 51(2): p. 175-177.
Urbach, F. and W.K. Noell, Effects of Oxygen Breathing on Tumor Oxygen
Measured Polarographically. Journal of Applied Physiology, 1958. 13(1): p. 6165.
Ogawa, S., et al., Brain magnetic resonance imaging with contrast dependent on
blood oxygenation. PNAS, 1990. 87.
Frahm, J., et al., Dynamic Mr Imaging of Human Brain Oxygenation during Rest
and Photic-Stimulation. Jmri-Journal of Magnetic Resonance Imaging, 1992.
2(5): p. 501-505.
Pauling, L. and C.D. Coryell, The magnetic properties and structure of
hemoglobin, oxyhemoglobin and carbonmonoxyhemoglobin. Proceedings of the
National Academy of Sciences of the United States of America, 1936. 22: p. 210216.
Ogawa, S. and T. Lee, Magnetic Resonance Imaging of Blood Vessels at High
Fields - Invivo and Invitro Measurements and Image Simulation. Magnetic
Resonance in Medicine, 1990. 16(1): p. 9-18.
228
185.
186.
187.
188.
189.
190.
191.
192.
193.
194.
195.
196.
197.
198.
199.
200.
Parkes, L.M., et al., Quantifying the spatial resolution of the gradient echo and
spin echo BOLD response at 3 Tesla. Magnetic Resonance in Medicine, 2005.
54(6): p. 1465-1472.
Duong, T., et al., High-resolution, Spin-Echo BOLD, and CBF fMRI at 4 and 7 T.
Magnetic Resonance in Medicine, 2002. 48: p. 589-593.
Ugurbil, K., et al., Functional mapping in the human brain using high magnetic
fields (vol B 354, pg 1195, 1999). Philosophical Transactions of the Royal Society
of London Series B-Biological Sciences, 1999. 354(1392): p. 2084-2084.
Yacoub, E., et al., Imaging brain function in humans at 7 Tesla. Magnetic
Resonance in Medicine, 2001. 45(4): p. 588-594.
Hyde, J., B. Biswal, and A. Jesmanowicz, High-resolution fMRI using multislice
partial k-space GR-EPI with cubic voxels. Magnetic Resonance in Medicine,
2001. 46: p. 114-125.
Bandettini, P.a., et al., Spin-Echo and Gradient-Echo Epi of Human Brain
Activation Using Bold Contrast - a Comparative-Study at 1.5 T. Nmr in
Biomedicine, 1994. 7(1-2): p. 12-20.
Rakow-Penner, R., et al. BOLD Contrast in the Breast at 3T. in 16th Annual
Meeting of the International Sociey of Magnetic Resonance in Medicine. 2008.
Toronto, CAN.
Rombouts, S.A.R.B., et al., Delayed rather than decreased BOLD response as a
marker for early Alzheimer's disease. Neuroimage, 2005. 26(4): p. 1078-1085.
Bluhm, R.L., et al., Spontaneous low-frequency fluctuations in the BOLD signal
in schizophrenic patients: Anomalies in the default network. Schizophrenia
Bulletin, 2007. 33(4): p. 1004-1012.
Patel, M.R., et al., fMR imaging bold signal changes with concurrent subclinical
EEG discharge monitoring in temporal lobe epilepsy patients. Radiology, 1997.
205: p. 1658-1658.
Dunn, J.F., et al., BOLD MRI vs. NIR spectrophotometry. Will the best technique
come forward? Advances in Experimental Medicine & Biology, 1998. 454: p.
103-13.
Pogue, B.W., McBride, T. O., Prewitt, J., Osterberg, U. L., Paulsen, K. D.,
Spatially variant regularization improves diffuse optical tomography. Appl. Opt.,
1999. 38(13): p. 2950-61.
He, X. and D. Yablonskiy, Quantitative BOLD: Mapping of Human Cerebral
Deoxygenated Blood Volume and Oxygen Extraction Fraction: Default State.
Magnetic Resonance in Medicine, 2007. 57: p. 115-126.
van Zijl, P., et al., Quantitative assessment of blood flow, blood volume and blood
oxygenation effects in functional magnetic resonance imaging. Nature Medicine,
1998. 4(2).
Lu, H., et al., Novel Approach to the Measurement of Absolute Cerebral Blood
Volume Using Vascular-Space-Occupancy Magnetic Resonance Imaging.
Magnetic Resonance in Medicine, 2005. 54.
Ogawa, S., et al., Functional Brain Mapping by Blood Oxygenation LevelDependent Contrast Magnetic-Resonance-Imaging - a Comparison of Signal
Characteristics with a Biophysical Model. Biophysical Journal, 1993. 64(3): p.
803-812.
229
201.
202.
203.
204.
205.
206.
207.
208.
209.
210.
211.
212.
213.
214.
215.
216.
He, X., M. Zhu, and D.A. Yablonskiy, Validation of oxygen extraction fraction
measurement by qBOLD technique. Magnetic Resonance in Medicine, 2008.
60(4): p. 882-888.
Baudelet, C. and B. Gallez, Current issues in the utility of blood oxygen level
dependent MRI for the assessment of modulations in tumor oxygenation. Current
Medical Imaging Reviews, 2005. 1(3).
Sumanaweera, T.S., et al., Mr Susceptibility Misregistration Correction. Ieee
Transactions on Medical Imaging, 1993. 12(2): p. 251-259.
Stollberger, R. and P. Wach, Imaging of the active B-1 field in vivo (vol 35, pg
246, 1996). Magnetic Resonance in Medicine, 1997. 38(2): p. 336-336.
Quaresima, V., S.J. Matcher, and M. Ferrari, Identification and quantification of
intrinsic optical contrast for near-infrared mammography. Photochem.
Photobiol., 1998. 67: p. 4-14.
Hull, E.L., M.G. Nichols, and T.H. Foster, Quantitative broadband near-infrared
spectroscopy of tissue-simulating phantoms containing erythrocytes. Physics in
Medicine & Biology, 1998. 43(11): p. 3381-404.
Kurth, C.D., et al., A dynamic phantom brain model for near-infrared
spectroscopy. Physics in Medicine & Biology, 1995. 40(12): p. 2079-92.
Holzschuh, M., et al., Dynamic changes of cerebral oxygenation measured by
brain tissue oxygen pressure and near infrared spectroscopy. Neurological
Research, 1997. 19.
Weidner, N., et al., Tumor angiogenesis and metastasis--correlation in invasive
breast carcinoma. New England Journal of Medicine., 1991. 324(1): p. 1-8.
Stefflova, K., et al., Targeted photodynamic therapy agent with built-in apoptosis
sensor for in vivo near-infrared imaging of tumor apoptosis triggered by its
photosensitization in situ. Molecular Imaging, 2006. 5(4).
Dunn, J.F., Zaim Wadghiri, Y., Pogue, B., Kida, I., BOLD vs. NIR spectroscopy:
will the best technique come forward? Adv. Exp. Med. Biol., 1998. 454(103-113).
Toronov, V., X. Zhang, and A. Webb, A spatial and temporal comparison of
hemodynamic signals measured using optical and functional magnetic resonance
imaging during activation in the human primary visual cortex. Neuroimage, 2007.
34(3).
Kennerley, A., et al., Concurrent fMRI and Optical Measures for the Investigation
of the Hemodynamic Response Function. Magnetic Resonance in Medicine, 2005.
54: p. 354-365.
Siegel, A., et al., Temporal comparison of functional brain imaging with diffuse
optical tomography and fMRI during rat forepaw stimulations. Physics in
Medicine and Biology, 2003. 48: p. 1391-1403.
Chen, Y., et al., Correlation between near-infrared spectroscopy and magnetic
resonance imaging of rat brain oxygenation modulation. Physics in Medicine and
Biology, 2003. 48: p. 417-427.
Sassaroli, A., et al., Spatially weighted BOLD signal for comparison of functional
magnetic resonance imaging and near-infrared imaging of the brain.
NeuroImage, 2006. 33: p. 505-514.
230
217.
218.
219.
220.
221.
222.
223.
224.
225.
226.
227.
228.
229.
230.
231.
232.
Huppert, T., et al., Quantitative spatial comparison of diffuse optical imaging with
blood oxygen level-dependent and arterial spin labeling-based functional
magnetic resonance imaging. Journal of Biomedical Optics, 2006. 11(6).
Xu, H., et al., Spectral Derivative Based Image Reconstruction Provides Inherent
Insensitivity to Coupling and Geometric Errors. Opt. Lett., 2005. 30(21): p. 29122914.
Chen, Y., et al., Probing rat brain oxygenation with near-infrared spectroscopy
(NIRS) and magnetic resonance imaging (MRI). Advances in Experimental
Medicine & Biology, 2003. 510: p. 199-204.
Seiyama, a., et al., Circulatory basis of fMRI signals: relationship between
changes in the hemodynamic parameters and BOLD signal intensity.
Neuroimage, 2004. 21(4): p. 1204-1214.
Ojemann, J.G., et al., Anatomic localization and quantitative analysis of gradient
refocused echo-planar fMRI susceptibility artifacts. Neuroimage, 1997. 6(3): p.
156-167.
Strangman, G., M.A. Franceschini, and D.A. Boas, Factors affecting the accuracy
of near-infrared spectroscopy concentration calculations for focal changes in
oxygenation parameters. Neuroimage, 2003. 18(4): p. 865-879.
Karczmar, G., et al., Effects of hyperoxia on T2* and resonance frequency
weighted magnetic resonance images of rodent tumors. NMR in Biomedicine,
1994. 7(1-2).
Provenzale, J.M., S. Mukundan, and D.P. Barboriak, Diffusion-weighted and
Perfusion MR Imaging for Brain Tumor Characterization and Assessment of
Treatment Response. Radiology, 2006. 239(3): p. 632-649.
Kuhl, C.K., et al., Breast neoplasms: T2* susceptibility-contrast, first-pass
perfusion MR imaging. Radiology, 1997. 202(1): p. 87-95.
Delille, J.P., et al., Breast cancer: Regional blood flow and blood volume
measured with magnetic susceptibility-based MR imaging - Initial results.
Radiology, 2002. 223(2): p. 558-565.
O'connor, J.P.B., et al., Comparison of Normal Tissue R-1 and R-2* Modulation
by Oxygen and Carbogen. Magnetic Resonance in Medicine, 2009. 61(1): p. 7583.
Glover, G.H., T.Q. Li, and D. Ress, Image-based method for retrospective
correction of physiological motion effects in fMRI: RETROICOR. Magnetic
Resonance in Medicine, 2000. 44(1): p. 162-167.
Rakow-Penner, R., BOLD MR slides from Thesis Defense. 2009.
Diehl, R.R., et al., Phase Relationship between Cerebral Blood-Flow Velocity and
Blood-Pressure - a Clinical-Test of Autoregulation. Stroke, 1995. 26(10): p.
1801-1804.
Brooksby, B., et al. Quantifying adipose and fibroglandular breast tissue
properties using MRI-guided NIR tomography. in Proc. SPIE. 2005. San Jose CA.
Kuhl, C.K., et al., Dynamic breast MR imaging: Are signal intensity time course
data useful for differential diagnosis of enhancing lesions? Radiology, 1999.
211(1): p. 101-110.
231
233.
234.
235.
236.
237.
238.
239.
240.
241.
Kelcz, F., et al., Clinical testing of high-spatial-resolution parametric contrastenhanced MR imaging of the breast. American Journal of Roentgenology, 2002.
179(6): p. 1485-1492.
Rosen, B.R., et al., Perfusion Imaging with Nmr Contrast Agents. Magnetic
Resonance in Medicine, 1990. 14(2): p. 249-265.
Bruening, R., et al., Echo-planar MR determination of relative cerebral blood
volume in human brain tumors: T1 versus T2 weighting. American Journal of
Neuroradiology, 1996. 17(5): p. 831-840.
Rosen, B.R., et al., Susceptibility Contrast Imaging of Cerebral Blood-Volume Human-Experience. Magnetic Resonance in Medicine, 1991. 22(2): p. 293-299.
Zhong, J.H., et al., Quantification of intravascular and extravascular
contributions to BOLD effects induced by alteration in oxygenation or
intravascular contrast agents. Magnetic Resonance in Medicine, 1998. 40(4): p.
526-536.
Hahn, E., Spin Echoes. Physical Review, 1950. 80: p. 580-584.
Sinha, S. and U. Sinha, Functional magnetic resonance of human breast tumors Diffusion and perfusion imaging. Techniques in Bioinformatics and Medical
Informatics, 2002. 980: p. 95-115.
Wang, X., et al., Image Reconstruction of Effective Mie Scattering Parameters Of
Breast Tissue In Vivo with Near-Infrared Tomography. J. Biomed. Opt., 2006.
11(4).
Liu, C.L., et al., Self-navigated interleaved spiral (SNAILS): Application to highresolution diffusion tensor imaging. Magnetic Resonance in Medicine, 2004.
52(6): p. 1388-1396.
232