Image-Guided Fine-Needle Aspiration of the Head
advertisement

Reprintedfrom the Archivesof Otolaryngology-Head& Neck Surgery October, 1998 Volume 124 Copyright 1998, AmericanMedicalAssciation
Image-Guided Fine-NeedleAspiration
of the Head and Neck
Five Years'Experience
MarthaJ. Sach,MD;RandalS. Weber,MD; GregoryS. W einstein,MD ;
Ara A. Chalian,MD; Harvey L. Nisenbqum,MD: David M. Yousem.MD
Obieclive: To evaluatethe diagnosticutility of imageguided fine-needleaspiration (FNA) in the headand neck.
Design: All image-guidedFNAs of the head and neck
performed January 1992 through June 1997 were included. All cytohistopathologicdatawere reviewedand
collated.A slide review was performed in all caseswith
c y t o h i s t o l o g idci s c r e p a n c i e s .
Selfing: The Department of Radiology, University of
PennsylvaniaMedical Center, Philadelphia.
Patients: Patientswith deep-seatedor poorly localized
massesin the head and neck, representingboth primary
or recurrenL/metastatic
lesions,were referred.
Reeults: There were 111 computed tomographyguided FNAs performed in 109 patients. Sitessampled
included parapharyngeal(n=20), parotid or submandibular (n=25), thyroid (34), and neck, paratracheay
skull base,and paraspinal(n = 3Z). Oi,paraesophageal,
agnosticsampleswere obtainedin 93 cases(83.8olo).
The
procedureswere well tolerated,without long-term complications. Cytologic examination detecteda total of 39
From the Departments oJ
Patholo g (Cy topathol ogy
Section) (Dr Sack),
O t orhin ol ar y n gologt -H ead
& Nech Surgery (Drs Weber,
'W
einstein, Chalian, and
Yousem),andRadiologt
(Drs Nisenbaum and Yousem),
U niv ersity of Pennsyh,ania
Me di cal C enter, Philddelphia.
Dr Sach is now with the
D epar tment of Patholo gy,
Abingt on M emon al H ospit aI,
Abington, Pa.
malignancies,24 of which were confirmed histologically. Eleven of the remaining malignant FNA casesreflectedrecurrent tumor, there were 3 false-positiveFNA
cases(2.7o/o),2in the setting of previous surgery and/or
radiation therapy. There were 2 false-negativeaspirates
from sitesdeepin the neck (1.8olo)among 7 of the 35 patients with benign aspirateswho underwent surgery.
Twenty six patientsunderwent ultrasound-guidedFNA
(thyroid gland only), revealing 1 papillary carcinoma and
I intrathyroidal parathyroid gland, both of which were
confirmed histologically.The findings in the aspiratesfrom
the rest of the patientswere benign (n = 18), Hurthle cell
neoplasm(n= 1), and nondiagnostic(n= 5).
Gonclusions: (1) The cytologic findings were supported
clinically andlor histologically in 86 (92o/")of the 93 diagnostic computed tomography-guided FNA cases.(2) Unnecessarysurgerywas avoidedin 37oloof the patientswith
recurrent tumor or benign diagnosesby cytologic assessment. (3) Potential pitfalls include false-positivediagnosesafter radiation therapy and procedural or sampling
Iimitations for deep neck and paraspinallesions.
Ar ch Otolaryngol H eadN ech Surg. 1998 ; 124: 1155 - 116 1
INE-NEEDLE
aspiration(FNA)
biopsy has become a wellestablishedtechniquein the
diagnosis,staging, and follow-up of patientswith head
and neck lesions.Endocrinologistsand otorhinolaryngologists use FNA to provide
rapid diagnosticinformation regardingpalpable massesof the thyroid gland, salivary glands, and cervical lymph nodes.
However,the clinical assessment
of deepseatedor poorly localized massesin this
region is highly challenging owing to the
complex anatomy and wide range of
lesions. A transmucosal,peroral FNA
approach to lesions in the parapharyngeal spacecan yield useful results, with
reported accuracyratesranging from 77olo1
to 88%.2However, this approachis accom-
panied by risk to carotid andjugular vessels and the facial nerve. Also, there are
procedural limitations regarding the stabilization of the lesion and the rangeof the
angle of approachthat can result in falsenegativeratesashigh as l9o/o.3Atransoral
open biopsy is generallycontraindicated
for the evaluationof theselesions owing
to unacceptablemorbidity. To minimize
theselimitations, FNA hasbeenpairedwith
imaging-guided localization for the cytologic assessment
of deep-seatedor poorly
Iocalizedlesions.The current study evalu-
ARCH OTOLARYNGOL HEAD NECK SURG/VOL 124, OCT 1998
I 155
PATIEIVTSAND METHODS
The radiology files at the University of PennsylvaniaMedical Center, Philadelphia, were searchedfor all imagingguided FNAs of the head and neck performed January L992
throughJune 1997. Patientsare referredfor theseservices
primarily by the head and neck surgeons,skull basesurgeons,and endocrinologistsat our institution. All corresponding cytology reports and follow-up surgical pathology reports were evaluated, and the slides from all cases
with discrepant cytologic-histologic findings were reviewed. A total of 111 CT-guided FNAs were performed
in 109 patients (59 women and 50 men; agerange, 18-92
years; median age,59 years). Previous palpation-guided
FNAs had been performed in 15 (I3.7'k) of thesepatienrs,
revealing normal salivary gland in 2 patients, a few atypical cells in 4 patients,tumor in I patient, and nondiagnostic results in B patients. Twenty-six patients (18 women and
B men; age range,24-BI years;median age,49 years) underwent ultrasound-guidedFNA. ln 4 of thesepatients,a
nondiagnosticaspiratehad been obtained previously.
All aspirateswere procured by radiologists,with speci
men preparation and evaluationperformed on site by the
cytopathologistsin all but I case.Lesionswere localized
on CT using anteroposterior and lateral scout tomograms
to plan the best angle and puncture site for sampling the
mass.''tAn 1B-gaugeinjection needlewas placedadjacent
to, and along, the line of site of the lesion,which was verified by scan, and then a 22-gauge spinal needle was inserted coaxially through the l8-gauge needle to the edge
of the lesion. After CT confirmation of needleplacement,
suction was applied to the22-gauge needle using a 20-mL
syringe, and the lesion was sampled with several vigorous
l- to 3-cm excursions.Suctionwas then releasedwhile the
1. Compuled
Tomography-Guided
Table
Fine-Needle
Aspiralion
0f Parapharyngeal
Space;Cylohistol0giG
C0rrelation
Diagnosis
Cytologic
No.of Hislologic Sulgery
l{ot
Gases ConfirmalionPerlormed
needle was still in the lesion, and the needle was withdrawn through the l8-gauge needle,leaving the latter in
place for repeatedpassesinto the lesion. For the thyroid
lesions sampled under ultrasound guidance, highfrequency ultrasound probes were used to image the nodules and to guide needleplacement.A 25-gaugeneedleattached to a l0-mL syringe was advancedinto the mass;
negative pressure was applied; and several small excursions were madebeforepressurewas releasedand the needle
was lemoveo.
ln all image-guidedcases,the aspiratedmaterialwasprocessedby the cytopathologist as air-dried direct smearsfor
a Giemsa-typestain (Diff-Quik, EM Diagnostic Systems,Gibbstown, NJ) for immediate microscopic evaluation and aswetfixed smearsfor Papanicolaou stain on return to the laboratory. The needle and syringe were rinsed with normal saline,
which was later concentrated onto a membrane filter (Millipore Corp, Bedford, Mass) and, if adequatematerial remained, into a cell block preparation. The aspiration procedurewas repeateduntil diagnostic material was obtained,
patient tolerance was reached, or 5 inadequate specimens
were accrued. An averageof 2.6 passeswere performed for
CT-guided FNA, with 79o/oof rhe casescompleted in I to 3
passes.The averagenumber of passesfor ultrasoundguided procedureswas 2.5; B0o/oof the caseswere completed in I to 3 passes.Histochemical stains (mucicarmrne,
periodic acid-Schiff, or trichrome) and./or immunohistochemical stainswere performed on direct smearor cell block
preparations in l0 cases.The panel of immunohistochemical stainsincluded thyroglobulin, Sl00 protein, HMB45, cytokeratins (AEl/3 and Cam 5.2), B-cell markers (L26, rc, and
}'), epithelial membrane antigen, HHF35, neuron-specific
enolase,synaptophysin, factor VIII, and CD34. Additional
specialstudiesincluded electronmicroscopyand RNA in situ
hvbridization oerformed on I caseeach.
A definitive cytologic diagnosiswas renderedin 93 (8+"/t
of the 111 CT-guidedFNA cases.A total of 39 malignant neoplasms(35%) were diagnosedcytologieally;benign neoplasmswere reported in 19 cases(I7o/o);35 aspirates (31.5'/') were consideredbenign/nonneoplastic
(including reactive/inflammatorylesions,cysts,and goiter). Therewere 18 nondiagnosticaspirates:3 (3%) were
consideredinconclusive,and l5 (I3.5'k) were not representativeor had insufficient tissue for diagnosis.The
cytologic results were supported histologically and./or
clinically in 86 (92'/") of the 93 diagnosticaspirates.
Sitessampledby CT-guided FNA included parapharyngeal (20), parotid/submandibular (25), thyroid (34),
and a miscellaneousgroup of paratracheaUesophageal,
neck,
skull base,and paraspinallesions (32 cases).Subsequent
surgical resection specimenswere obtained in 55 of the
109 patients.Among the cytologicallydefinitive cases,CTguided FNA correctly classified8lo/oof lesions undergoing surgical resection.Surgerywas avoided in 46 patients
with cytologically confirmed recurrent tumor or benign
disease(including granulomatous inflammation, reactive ly'rnphnode,Warthin tumor, and nodular goiter). Malignancy was found in 4 of the 7 patients with nondiagnostic aspirateswho underwent surgical resection.
il.lrfr:,1i,{:iii#iri:#,,'..
i
U
ilxLo,',".,'J*:'on"
l
lymphoproliferative
11,
U
1:
l): :,
o,i.
5t
,:..:
*1fu,*l-x,,, 15
:l ,'
1',,
'lri .
U
flffi'uuo,'utu
Branchial
cleftcyst
Total
1
m
0
I
1t
11
* Rhabdonyosarcona.
hadprevious
benign
surgical
biopsy
results;
allcases
IFourof6 cases
showed
nochange
inf0llow-up
scans.
atesthe diagnosticutility of computed tomography (CT)and ultrasound-guidedFNA of massesin the head and
neck.
ARCH OTOLARYNGOL HEAD NECK SURG/VOL 124, OCT 1998
I 156
Table
Tomography{uided
2. Compuled
Fine-Needle
Aspiration
Regions:
of ParotidAubmandibular
Cylohlstologic
Conelation
Cytologic
Diagnosis
No.of Cases
Squamous
cellcarcinoma
Mucoepidermoid
carcinoma
Acinic
cellcarcinoma
Pleomorphrc
adenoma
Warthin
tumor
Reactive
lymphnode
gland
Normal
Nondiagnostic
Hislologic
Confirmation
. .'l
a
i1'
t
.i
28
Total
Findings
Discrcpanl
NotPerformed
Surgery
l Sialadenitis
1 Suppurative
sialadenitis
None
1 Mucoepidermoid
carclnoma
None
None
None
1 Adenocarcinoma
(arising
adenoma);
in pleomorphic
1 squamous
cellcarcrnoma
(maxilla)
S
1l
Table
Tomography-Guided
Fine-Needle
Aspiration
0l ParatraGheal/Esophageal/Spinal,
3. C0mputed
andNeDk
Regions:
Gytohislologic
Conelation
SkullBase,Inlratemporal,
,Solgtryfior
Fa*o*nsd:l
::|ligfsl$gif:,]
No.oleases
Gylologic
Diagnosis
rtonllrmili0n
l EeniOn
cystwithfibrosis
7
Squamous
cellcarcinoma
Adenocarcinoma
Poorly
carcinoma
differentiated
(recurrent)
Papillary
carcinoma
thyroid
Hemangiopericytoma
Findings
Discrepanl
,c
J
1il131'n""'
1
1
7
Nondiagnostic
7
1.
. .: . . . .
,u
None
carcinoma;
fllt rrrmcerr
,;1,,:'::;:"'
'Tolal
il:t:
u,
3?
ltl
l0
'',r,1':,:i',
r,,,'illi,li
:ti
'|i lli,I.i,'l
a
1 poorlydifferenliated
carcinoma
1 Intraspinal
myxopapillary
ependymoma:
1 squamous
cellcarcinoma;
'1poorlydifferentiated
carcinoma;
t heterotopic
brainiissue;
and1 schwannoma
,
t
12
Aspiration
oftheThyroid
Gland*
Fine-Needle
forlmage-Guided
Table
4. Cytohistologic
Gonelation
No.of Cases
F-*
Cylologic
Dia0nosi$
Papillary
thyroidcarcinoma
Poorly
differentiated
carcinoma
Squamous
cellcarcinoma
Follicular
neoplasm
Hilrthle
cellneoplasm
Goitelbenign
Parathyroid
lesion
Inconclusive
N_ond
iagnostic
Total
i
Surgery
Not
Perlorm6d
HistologiG
Conlirmalion
.,s---..-F-----T
21:
101
Findinost
Discrepanl
None
None
None
None
1 Hilrthle
cell
ri--
--c
00
00
10
10
01
j
,.,
.,,,....'.,i..
..,,,,,,,
00
1n
00
30
01
no'
00,
72
*CTindicates
tomography;
US,ultras,und.
computed
FNA.
were
allobtained
byCT-guided
specimens
lThese
The use ofultrasound-guided FNA for headand neck
lesions was limited to the thyroid gland during the 5.5year study period. A definitive diagnosiswas established
in 22 (79o/,)of the 28 aspiratesobtained under ultrasound guidance. Two of these cases,a papillary carci-
noma and a parathy'roidlesion, were confirmed histologically. Nineteen of the remaining diagnostic aspirateswere
benign, and there was I follicular neoplasm. The cytoIogic results with histologic correlation are presentedfor
each anatomical site in foble I through fabb 4.
ARCH OTOLARYNGOL HEAD NECK SURG/VOL I 24, OCT 1998
I 157
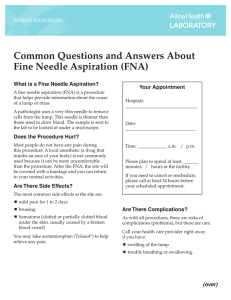
Figure
1. Cellblockfroma fine-needle
aspirate
obtained
froma left
nasopharyngeal
massinapatientwhohasundergone
lungtransplantation
populati0n
showing
a mononorphic
ceilswithlarge,irregular
oflymphoid
nuclei
andproninent
nucleoli.
lmmunohistochemical
stains
dem0nstrate
a
population,
I\-restricted
cl0nal
withlymphoma
consistent
-eos
(hematoxy
Iin in,originalmag
x 630).
nification
PARAPHARYNGEAL SPACE (20 PATIENTS)
Squamouscell carcinomaswere encounteredin 6 of the
9 malignanciesdiagnosedin the parapharyngealspace
by CT-guided FNA. Four of thesecasesrepresentedrecurrent diseasefrom primary tumors of larynx, tonsil,
tongue, and soft palate. The second most common lesion sampledin the parapharyngealspacewas pleomorphic adenomainvolving the deeplobe of the parotid gland
or the minor salivaryglands (4 cases,including I recurrent case).Other malignanciesdiagnosedcytologically
in this region included a recurrent poorly differentiated
carcinoma of the larynx and a spindle cell neoplasm in
an lS-year-old man that, afterresectionand ancillary studies (immunohistochemical,electronmicroscopic,and moIecular studies), proved to be a rhabdomyosarcoma, embryonal type. The final malignancy in this group was a
caseof posttransplant lymphoproliferative disorder in a
patient who had undergone lung transplantation. The aspirate in this caserevealeda monomorphic population
of large, predominantly single cells (Figure | ) that were
X restricted by immunohistochemical stains. The results of Epstein-Barrvirus in situ hybridization were negative in the li.mited material available for study. Adequate
material was obtained for all the parapharyngeal aspirates,and there were no false-negativeor false-positive
cytologic results.
Figure
2. Tjp,Direct
snearofafine-needle
aspirate
obtained
froma mass
in theanterior
aspect
oftheneckina patientwhohasundergone
radiation
therapy
forsquamous
cellcarcinona
ofthelarynx.
Highly
atypical
epithelial
todense
cellsadjacent
stromawereoriginally
nisinterpreted
asrecurrent
(Diff-Auik,
cellcarcinona
magnification
x 630).Bottom,
squamous
original
surgical
resection
showing
Corresponding
specinen
a benign
thyroidcyst
walllinedbyfollicular
witha sclerotic
cellswithreactive
aupia,reflecting
(hematoxylin-eosin,
x400).
radiation
therapy
changes
original
nagnification
neoplasm preoperatively. Finally, 5 aspiratesof parotid
gland (20o/oof the aspiratesobtained in this group) were
insufficient for diagnosis. Surgical procedures were performed in 2 of thesecases,one of which revealedadenocarcinomaarisingin a pleomorphic adenoma,and the other
a squamous cell carcinoma of the maxilla, with lymphoma in the accompanyingneck nodes(the parotid gland
was normal in the resection specimen).
MISCELLANEOUS SITES (31 PATIENTS)
PAROTID/SUBMANDIBULAR SITES
(25 PATIENTS)
This group included 4 patients who had undergone resection and radiation therapy of primary squamous cell
carcinomas(tonsil, tongue,retromolar trigone,and maxilla), 4 patientswith historiesof primary salivarygland neoplasms, and I patient with a history of breast carcinoma.
There were 2 false-positivecytologic diagnoses:both were
casesofsialadenitis (l in the setting ofradiation therapy)
in which atypical squamousmetaplastic changeswere interpretedasmalignant. Overlapping cytologic featuresbetween pleomorphic adenomasand mucoepidermoid carcinomas led to misclassificationof I salivary gland
Computed tomography-guided aspiratesof paratracheaV
esophageal,neck, paraspinal, skull base, and infratemporal massesmake up this group. The majority of the malignant aspiratesreflectedprimary (3 cases)and recurrent
(3 cases)squamouscell carcinomas.A caseof hemangiopericytoma was accuratelydiagnosedin the cytologic material using ancillary studies (immunocytochemistry and
electron microscopy). There was I false-positiveaspirate
from a massin the anterior aspectof the neck in a patient
with a history of laryngeal carcinoma: a small number of
atJpical cells from a fibrotic thy'roid cyst were misinterpreted as malignant (Figure 2). Two false-negativeaspirates were also identified in this group. These 2 cases
ARCHOTOLARYNGOLHEAD NECK SURG/VOLT24.OCT 1998
I 158
reflect inadequate sampling due to technical limitations
encounteredin FNA of the oericarotid sheathin one case
and a previousoperativesite near the mandiblein the other
case.These technicaVsampling limitations are also evident in the 7 nondiagnostic aspirates;5 of the target Iesionswere resected,revealing2 casesof carcinoma,I intraspinal ependymomawith accompanyingparaspinal
fibrosis, I schwannoma,and the rare entity of heterotopic brain tissue in the pterygopalatine fossa.
THYROID GLAND (59 PATIENTS)
The majority of thyroid lesions sampledby both CT- and
ultrasound-guided FNA were cytologically benign, reflecting goiters,thyroiditis, and parathyroid tissue.Nodule size,which was recordedfor 22 of the 28 ultrasoundguided FNAs, ranged from 0.7 to 4.2 cm in greatest
dimension,with a mean of 2.29 cm. All of the malignant
aspiratesobtainedby both imaging techniqueswere confirmed histologicallywith the exception of I caseof recurrent squamouscell carcinoma(unknown primary site).
The cytologic material obtainedby CT-guidedFNA in I
caseof papillary carcinomawith extensivecystic degeneration was considered suggestiveof papillary carcinoma, but the scant cellularity and cystic background features precluded a definitive diagnosis.Two additional
samplesobtained by CT-guided FNA were consideredinconclusive for neoplasm; however, the patients involved were unavailablefor follow-up. Of the 3 resected
nodules. 2 were reDortedasneoadenomas/adenomatous
plastic on the basisof the aspirate.An intratiryroidal parath1'roid adenoma was identified preoperatively as parathyroid tissue by ultrasound-guided FNA. The
nondiagnosticrate was higher in the ultrasound-guided
thyroid aspirates(21 .4oh)than in those guided by CT imaging (8.8%).
The treatmentof patientswith deep-seatedor poorly localizedlesionsof the head and neck requiresa multimodal approach that combines clinical, radiographic,and
pathologic data.Anatomical location, growth pattern, and
anticipated histologic findings all play an important role
in preoperative planning.6-8Modern imaging techniques are recognized for their ability to delineate deep
tissueanatomy. Magnetic resonanceimaging is considered superior for soft tissuecontrast resolution, while CT
Yet these
is bestsuited for evaluatingsubtlebony changes.e
techniquescan only rarely provide specifichistopathologic diagnoses.Similarly, when used in the follow-up
of patients with malignanciesin the head and neck, these
studies are of limited value in distinguishing among recurrent tumor, scar tissue, radiation edema, or infection.e Palpation-guidedFNA is an establisheddiagnosof palpable
tic techniquefor the preoperativeassessment
lesionsof the head and neck.r0-ra
More recently, experience with image-guidedFNA of nonpalpable abdominal and thoraciclesionshasbeenappliedin the headand
neck region.15Using a technique describedin previous
reports,a'5
lesions arising in the pericarotid sheath,thyroid gland, skull base, and parapharyngeal, parotid./
submandibular, paratracheal,paraesophageal,
paraspinal, and infratemporal regions have been sampled under
CT guidanceat our institution.
The most common tumors diagnosedby aspiration
in the parapharyngeal region were squamous cell carcinomas (severalof which were recurrent) and pleomorphic adenomas.These 2 diagnosesaccount for 50oloof
parapharyngeallesionssampled,with the remaining neoplasmsarising from neural, mesenchymal,and hematopoeitic tissues.Benign processesspecificallydiagnosed
by CT-guided FNA included granulomatousinflammation, granulation tissue,and branchial cleft cyst. While
the numbers are small, the distribution of diagnosesestablishedby FNA in this region are similar to those reported in the surgical literature.bAlso, the technique
proved to be highly effectivein terms of diagnosticyield
and accuracy,documentingtumor recurrencein 6 cases,
avoiding unnecessarysurgery in 6 casesof benign diseaseand a l1'rnphoproliferativelesion, and providing histologic data for surgical procedure planning in the remaining cases.These results are in contrast to those
achievedby Shosset alt6in an earlier study of the preoperativeand intraoperativeassessmentof parapharyngeal masses.ln their study, 10 of 42 patientsunderwent
open biopsy via an external (ie, transcervical)approach
for what proved to be unresectablemalignant neoolasrns.
Computed tomography-gulded FNA of the parotid and submandibular regions documented recurrentbenign (l case)andmalignant (3 cases)salivarygland
tumors, as well recurrent squamous cell carcinoma (2
cases).An additional I1 primary neoplasmswere diagnosed by FNA, 7 of which were confirmed histologically. Interpretive errors were made in 3 casesfrom this
group. ln I case,a low-grade mucoepidermoid carcinoma was misclassifiedcytologically as a pleomorphic
adenomaowing to misinterpretation of the mucoid material in the background of the specimen as representing the myxoid stroma seenin benign mixed tumors. The
secondwas a caseof suppurative sialadenitisin which
the inflammatory component was not appreciatedand
the atypicalmetaplasticsquamoidcellsin a background
of proteinaceous and cellular debris led to a falsepositive diagnosisof mucoepidermoidcarcinoma.These
casestJpify the well-recognized diagnostic pitfalls characteristicof the cytologic evaluationof this low-grade salivary gland malignancy.lTThe third diagnosticerror was
a misinterpretation of atSryicalsquamous metaplasia in
postradiationsialadenitis.Five asphatesin this group were
consideredinsufficientfor diagnosis;2 of the patientsinvolved underwent surgery, revealing malignant tumors
in both cases.One of these caseswas a recurrent squamous cell carcinoma involving the maxilla, underlying
the parotid gland. Reviewof the aspirateslidesrevealed
only normal salivarygland tissue,indicating that the bony
Iesionwas not effectivelysampled.The secondcasewas
an adenocarcinomain situ arising within a pleomorphic
adenomaof the parotid gland that was adjacentto a Warthin tumor, highlighting the potential complexity of lesions in this region. Similar problemswith nondiagnostic specimens were encountered in aspirates from
paraspinal,pericarotid, and anterior neck regions (Table
ARCH OTOLARYNGOL HEAD NECK SURG/VOL 124. OCT 1998
I 159
3). These results suggestthat attempts to optimize the
FNA sampling of lesionsin thesesitesvia image-guided
needleplacement and on-site cytologic assessmentcan
not always circumvent the technicaVprocedurallimitations of accessto thesedeeplesionsadjacentto vital anatomical structures.In a large seriesof 1022 aspiratesof
tumors and tumorlike conditions of the oral and maxillofacial region, Daskalopoulouet alloencountered18 cases
with false-negativecytologicresultsand stressedthat negative FNA resultsshould not be relied on when the clinical assessmentindicatesmalignancy.The presentstudy
findings also serveto emphasizethe critical importance
of generoussamplingand a conservativeapproachto diagnosingrecurrent tumor after radiation therapy.
HEEXPERIENCI
with image-guidedFNA of
the thyroid gland in this serieswas relatively limited, with the majority of aspiratesindicative ofbenign processes.All but
I of the primary thyroid malignancies,
along with a metastaticsquamouscell carcinoma,were
definitively diagnosedby FNA. Sampling of the remaining case,a cystic papillary carcinoma,was insufficient
for a definitive diagnosis(papillary carcinomawas suspected),despiteCT guidanceto ensureaspirationofsolid
areas.A number of recentreoortshavedemonstratedthe
diagnosticaccuracyof ultrasound-guidedFNA in the managementof thyroid nodules.rs-2r
ln a study by Yokozawa
et a1,18
a group of 678 patients diagnosedas having benign thyroid nodules by palpation-guidedFNA underwent ultrasound-guidedFNA within 2 to 24 months of
the conventionalprocedure.Malignancy was suspected
in 107 of thesepatientsbasedon the ultrasound-guided
procedureand was confirmed histologically in 99 of the
I07. The most common causefor the cancersmissedby
conventional FNA was the presenceof nonpalpablelesions (those associatedwith benign nodules or autoimmune thyroid diseaseand solitary small cancers).Inadequate sampling (eg, cystic lesions) (29.3Vo)and poor
technique (l5.2tk) accountedfor the missed cancers
among the palpablelesionssampledby conventionalFNA.
In contrast,there was no significant differencein sensitivity and specificitybetweenpalpation-and ultrasoundguided FNA of thyroid nodules reported by Takashima
et a|e; however,insufficiencyrateswere significantlylower
with the image-guidedtechnique(3.7o/ovs
19%).The recognized advantagesof ultrasound-guided FNA of thyroid nodules in this studv included the specific sampling of solid areaswithin cystic massesand ihe sampling
of nonpalpable,relatively large nodules in glands with
diffuse diseaseor following surgery or radiation therapy.
However, the use of this technique as a screeningprocedureis controversial,asit may lead to the detectionof
small cancersthat are of questionablebiological significance.20
22
Controversyalso surrounds the role of ultrasoundguided FNA in the assessmentof cervical lymph node
status in patients with head and neck cancers.Currently, elective (prophylactic) treatment of the neck is
performed when the risk of occult metastasesis greater
ihan or equal to L5okto 2}o/o,23
resulting in overtreat-
ment in the majority of patients.Comparativestudiesof
modern imaging techniquespaired with FNA suggestthat
this approachmay be refined in certainsettings.In a prospectiveevaluation of 132 patients with squamouscell
carcinoma of the head and neck, van den Brekel et al23
found CT, ultrasonography,and magneticresonanceimaging to be superior to palpationfor cervicallymph node
staging.Ultrasound-guided FNA was significantly better than any other technique evaluated,with sensitivity
and specificity rates of 90o/oand 100o/o,
respectively.In
this study, ultrasound-guidedFNA detected75o/oof the
patients with histologically proved lymph node metastasesand negativepalpation findings. However, theseand
other investigatorsemphasizethat the technique is highly
operatordependentand bestapplied to patientswith inconclusiveCT and,/ormagneticresonanceimaging results or uncertain palpatory findings.23-25
Thesestudies,along with the presentreport, demonstratethe expandingrole of image-guidedFNA in the
evaluationof the head and neck lesions.Improvements
in the accuracyofpreoperative diagnostictechniqueshave
been realized,with significant impact on patient treatment. For parapha4mgealmasses,image-guidedFNA can
define whether surgeryis needed,along with the appropriate surgical approach.In the setting of an immunocompromised patient, a distinction between neoplastic
(eg, lymphoma) and inflammatory/infectiousprocesses
can be made,reducing dependenceon open biopsy,with
the accompanyingrisks. However,limitations remain,particularly in the setting of previous surgeryand radiation
therapy.Someof theselimitations will be reducedby in...ur"d experience.which, when combined with refined patient selectioncriteria.will lead to optimized diu g n o s i i cu t i l i t y o I t h e s et e c h n i q u e s .
AcceptedforpublicqtionApril 29, 1998.
Presentedinpart ds 6posterqt the87th Annuql Meeting oJ the US and CanadianAcademyoJ Pathology,Boston, Mass,March 2, 1998.
Reprints:Martha J . Sach,MD, DepartmentoJPathologt, AbingtonMemonql Hospital,1200 Old,Yorh Rd,Abington,PA 19001.
1. DasDK,GulatiA, BhattNC,Mandal
AK,KhanVA,Bhambhani
S.Fineneeore
aspiration
cytol0gy
0f oralandpharyngeal
lesions:
a studyof 45 cases.
ActaCytol.
19 9 3 : 3 7 : 3 3 3 - 3 4 2 ,
2. lvlondal
{ineneedle
A, Raychoudhur
BK.Peroral
aspiration
cytology
of paraphalesi0ns.
ActaCytoL1993;37:694-698.
ryngeal
3. Castelli
M, Gattuso
P, Reyes
C,SolansEP.Fineneedle
aspiration
biopsyof intraoralandpharyngeal
lesions.lcla Cytol.1993;37
:448-450.
4. YousemDlVl,SackMJ,ScanlanKA.Biopsyofparapharyngealspacelesions.RadioIogy.1994;19361I -622.
5. Yousem
D M ,S a c kl V UH
, a y d eR
n E ,W e i n s t e iGnS .C o m p u t et d
0m0graphyguidedaspirations
0f parapharyngeal
andskullbasemasses.
SkullBaseSurg.
19 9 5 : 5 3
: 11- 13 6 .
6. KletzkerGR,SmithPG,BigelowDC,LeonettiJP,GrubbRL.l\ilanagement0fhigh
parapharyngeal
spacetumors.EarN1seThroat
J. 1991;70:639-647.
preopera7. SomPM,BillerHF,Lawson
W.Tumorsof theparapharyngeal
space:
tiveevaluation,
diagn0sis
approaches.,4rr
andsurgical
otolBhin1lLaryng1l
Suppl.
19 8 1 ; 9 0 ( 4
p )t : 3 -51.
8. SomPM,Sacher
M, Stollman
AL,BillerHF,Lawson
W. Common
tumors0t the
parapharyngeal
space:refined
imaging
diagnosis.
Radi0l1gy.1988;169:81-85.
jmaging
9. vandenBrekel
IMWM,
JA,SnowGB.Therole0f modern
Castelijns
stud-
ARCH OTOLARYNGOL HEAD NECK SURG/VOL 124, OCT 1998
I 160
tf
h i. T h y r o i dn o d u l e sc:l i n i c ael f f e c o
Semin0nc0l.1994;21.
1 9 .T a k a s h i mSa, F u k u d aH , K o b a y a s T
iesin staging
andtherapy
0f headandneckneoplasms.
biopsy.J ClinUltrasound.1994i22:
aspiration
fine-needle
ultrasound-guided
340-348.
d sl ep i r a t i 0 n
535-542.
10 . D a s k a l o p o uD
l o, R
u a p i d iAsD ,M a o u n iNs , M a r k i d oSu. F i n e - n e e a
T, Fukata
S, KumaK, et al.Thyroid
reB. ln discussi0n
0f: Yokozawa
20 Hamberger
0f the oralandmaxillofacial
cytologyin tumorsandtumorlikeconditi0ns
World
fine-needle
aspiration
biopsy.
J Surg.
gion:diagnostic
(Cancer
Cytopathol).1997
cancer
detected
byultrasound-guided
reliability
Cancer
andlimitations.
1996;20:853.
81:238-252.
c l u eo {
ch
e tu i l l a u s s ePaJu,C h a g n oSn,e ta l .T h ed i a g n o s tvi a
1 1 . F r a b l e W J . N e e d l e a s p i r a t i 0 n b i o p s y : p a s t , p r e s e n t a n d f u t u r e . H u m P aZ tI h oCl .ol 9
Sa9n, d - P r i 0Bl,lG
thyroidn0dinn0nJuncti0nal
bi0psy
underultrasonography
line-needle
aspirati0n
20:504-517.
findings.
/m J Med
andhistol0gic
cytologic
studyc0mparing
1 2 . C o h e n M B , R e z n l c e k l V l J , M i l l e r T R . F i n e - n e e d l e a s p i r a t i o n b i o p s y 0 l t h e sules:
a l i vaaprospective
ry
glands.PatholAnnu.1992;27
(pt 2):213-245.
.152-157
.
1994:97
c pact
l de c o n o mi m
glandtum0rsby fine-needle
t zP .C l i n i c a n
22 Y o u s e m
D M ,H u a n T
g , L o e v n eLrA ,L a n g l oC
asBJ.Diagnosis
of salivary
13. Layfield
LJ,Glasgow
f0undwithCTandMR.AJM,4mJ Neuroradiol.1997:
lesions
pirationcytologyr
o1incidentalthyroid
a review0{ clinicalutilityandpitfalls.DiagnCytopathol.l9g1,
18:1423-1428.
7:267-272.
, o l d i nR
, n 0 wG B .
g P ,M e y eCr J LS
, a s t e l i jJnAs ,S t e H
l VG
23.v a nd e nB r e k eMl W MC
1 4 , G h a r i bH , G 0 e l l n eJrR .F i n e - n e e dalsep i r a t i obni o p s yo f t h et h y r 0 i da: n a p for the
aspiration
cytology
andultrasound-guided
imaging
techniques
lvlodern
oraisal.Ann lnternMed.1993:118:282-289.
sludy.EutArch
c0mparalive
percutaneous
a prospective
0f necknodemetastases:
biopsies
0l head
assessment
J, CT-guided
t c Gatenby
RA,Mulhern
CB,Strawitz
1-17.
1993;250:1
1torhinolaryngol.
Radiology.
1983;146:717-719.
andneckmasses.
ultrasound,
MJ, KurkiTJl,KlemiPJ.Palpation,
R,Varpula
24 AtulaTS,Grenman
space.Arch
DT,Al{ordBR.Tumorsoftheparapharyngeal
t o ShossSM,Donovan
intheassessment
0f cercytol0gy
fine-needle
aspirati0n
andultras0und-guided
11:753-757.
1tolaryngol.
1985;1
HeadNeck.1996;18:
T, BottlesK. Fineneedle
vicallymphnodestatusin headandneckcancerpatients.
17. C0henlVlJ,FisherPE,HollyEA,LlunglVlB,Lowhagen
5 4 5 - 5 5. 1
statistical
analysis.
carcin0ma:
ot muc0epiderm0id
aspirati0n
bi0psydiagn0sis
L ,N o y e k A MB,e d a rYdC .U l t r a s o n 0 g S ,E l d e n
25. l M c l v oNr P ,F r e e m aJnL ,S a l e m
.
ActaCytol.1
990;34:43-51
aspiration
biopsyof headandnecklefine-needle
raphyandultrasound-guided
by ultrasoundS, KumaK, et al.Thyroidcancerdetected
18. Yokozawa
T, Fukata
perspective.
1994;104:669-674.
Laryngoscope.
guidedtine-needle
sions:a surgical
aspiration
bi0psy.WoildJ Surg.1996l20:848-853.
ARCH OTOLARYNGOL HEAD NECK SURG/VOL I24, OCT T998
I 161
Printed and Published in the United States ol America