Mutuality, Self-Silencing,
and Disordered Eating
in College Women
Lisa S. Wechsler
Shelley A. Riggs
Sally D. Stabb
David M. Marshall
ABSTRACT. The current study examined patterns of association among
mutuality, self-silencing, and disordered eating in an ethnically diverse
sample of college women (N = 149). Partner mutuality and overall selfsilencing were negatively correlated and together were associated with six
disordered eating indices. All four self-silencing subscales were associated with disordered eating patterns. For example, external self-perception was associated with drive for thinness, bulimia, body dissatisfaction,
and interoceptive awareness. Implications of the findings for college
counselors are discussed. [Article copies available for a fee from The Haworth
Document Delivery Service: 1-800-HAWORTH. E-mail address: <docdelivery@
haworthpress.com> Website: <http://www.HaworthPress.com> © 2006 by The
Haworth Press, Inc. All rights reserved.]
KEYWORDS. Eating disorder, feminist theory, mutuality, self-silencing
Lisa S. Wechsler, PhD, earned her doctorate from Texas Woman’s University
(TWU) and is currently a licensed Psychologist in private practice.
Shelley A. Riggs, PhD, is an Assistant Professor, University of North Texas.
Sally D. Stabb, PhD, is an Associate Professor, TWU Department of Psychology
and Philosophy.
David M. Marshall, PhD, is a full Professor, TWU Department of Mathematics.
Address correspondence to: Shelley A. Riggs, Department of Psychology, University of North Texas, P.O. Box 311280, Denton, TX, 76203-1280 (E-mail: riggs@
unt.edu).
Journal of College Student Psychotherapy, Vol. 21(1) 2006
Available online at http://www.haworthpress.com/web/JCSP
© 2006 by The Haworth Press, Inc. All rights reserved.
doi:10.1300/J035v21n01_05
51
52
JOURNAL OF COLLEGE STUDENT PSYCHOTHERAPY
Women are at greater risk for and have a higher incidence of eating
problems than do men (Smolak & Murnen, 2001). In particular, dieting,
weight concerns, and more serious disordered eating patterns have been
shown to be prevalent among college women (McCann, 1995; Mintz &
Betz, 1988; Spitzer, Henderson, & Zivian, 1999). Unhealthy attitudes
about body image, dieting, and exercise are supported and exacerbated
by many college cultures (Boskind-White & White, 2001), especially campuses with a heavy emphasis on dating, where higher rates of bulimia
have been found (Rodin, Striegel-Moore, & Silberstein, 1985). Feminist theorists have proposed that socio-cultural characteristics contribute to the development and expression of eating disorders (Snyder &
Hasbrouck, 1996; Worrell & Todd, 1996) and evidence suggests that
awareness of and internalization of societal standards for appearance are
related to body dissatisfaction (Cusumano & Thompson, 1997; Stice et al.,
1994). Relational-cultural theory (RCT; Jordan, 1991, 1997; Miller &
Stiver, 1997) asserts that the presence of mutual connections may counter
some of the stereotyped images of intimate heterosexual relationships
with their inherent power differentials, which women are exposed to in
the broader culture and experience in their daily lives. On the other hand,
the absence of mutual connection and the protective strategy of withholding authentic experiences are likely to result in psychopathology, including eating problems (Miller & Stiver, 1997). Given the vital role of
interpersonal connections in women’s identity and mental health and
the centrality of intimate partner relationships for most college women,
the current study sought to explore how the perceived quality of intimate relationships and/or the use of self-silencing strategies to maintain
such relationships may be associated with the development of eating
dysfunction.
Women who develop disordered eating often believe that others
evaluate them according to personal appearance to the exclusion of
other personal qualities and abilities. For example, they may internalize
a moral injunction that thinness equals goodness and therefore believe
that excess weight equates with being weak, lazy, incompetent, or unlovable (Cooper & Fairburn, 1987; Kaschak, 1992). Feminist theorists
(e.g., Bloom et al., 1994; Boskind-White & White, 2000; Kaschak, 1992;
Surrey, 1991) `argue that women with eating disorders have all too fully
and accurately internalized the messages they have received from the
culture at large, with tragic consequences. Thus, eating problems are
conceptualized as symbolic of the various ways women use their physical
selves to confront the psychological consequences of these societal messages and socially imposed roles.
Wechsler et al.
53
Eating problems in women are also triggered or exacerbated by the
increased complexities in relational connection due to developmental
and life transitions such as entering college (Surrey, 1991). According
to relational-cultural theory (RCT; Jordan, 1991, 1997; Miller & Stiver,
1997), the primary and ultimate goal of human development is “the ability
to participate actively in relationships that foster the well-being of everyone involved . . . as the relationship grows, so does the individual”
(Miller & Stiver, 1997, p. 22). In turn, the absence of safe, nurturing and
empowering connections, along with the rigid internalization of socialization messages that narrowly define individual worth and gender-appropriate behavior in relationships, are often sources of psychological
distress. Socialization within a patriarchal culture leads to the formation of
restricted, limiting relational schemas that may then inhibit both women’s and men’s ability to express the wholeness of their being within
relationships (Miller, 1986).
The process of relational mutuality is considered to be a major pathway toward establishing growth-enhancing connections (Miller, 1988).
Mutuality, as described by Miller, includes the qualities of engagement
(attention and presence), empathy, zest (energy), knowledge (clarity),
empowerment (ability to take action within and on behalf of the relationship) and diversity (acknowledging and appreciating differences).
Low perceived mutuality within intimate partner relationships has been
found to correlate with women’s depression (Genero, Miller, Surrey &
Baldwin, 1992), anger suppression (Sperberg & Stabb, 1998), low selfesteem and marital dissatisfaction (Lippes, 1998). Recent work has
established a negative correlation between mutuality and self-silencing
among female cancer patients (Kayser, Sormanti & Strainchamps, 1999),
whose higher scores on quality of life and self-care agency were linked
with higher mutuality in intimate relationships. Potential associations between mutuality and eating disorders are just beginning to be explored;
suggestive evidence of such a link is found in reports that healthier eating attitudes among college women are positively correlated with interpersonal connection, greater psychological differentiation, and social support (Hirsch, 1999) and in the work of Jackson, Weiss, Lunquist and
Soderlind (2005), who found that lessened social support in close relationships contributed to increases in disordered eating among college-aged
women.
In studying the narratives of depressed women, Jack (1991) noted
transitions in the participants’ use of the first-person voice, referred to
as the “authentic I,” to that of a third-person voice, labeled the “OverEye,” which seemed to emerge as participants reported behaviors or
54
JOURNAL OF COLLEGE STUDENT PSYCHOTHERAPY
emotions that differed from the traditional societal notion of a “good
woman.” With the Over-Eye often overriding the authentic self’s viewpoint, many participants evaluated their notion of goodness according
to external standards (i.e., patriarchal culture) rather than their own and
developed a pervasive process of self-scrutiny to ensure compliance with
such standards. Perceived failure to live up to these internalized standards
(Jack, 1991; Jack & Dill, 1992) is thought to play a role in women’s
greater vulnerability to certain psychological disorders. Manifestations
of the “Over-Eye” in American society that impact the mental health of
women in general, and the development of disordered eating in particular, include the adoption of white male-dominant standards of beauty and
the normative experiences of being scrutinized for one’s appearance. Pervasive monitoring and scrutiny, or objectification of women’s bodies by
males, and by other women as well, necessarily leads to an internalized
process of self-scrutiny. This internalized process of self-scrutiny, referred to by other investigators as “self-objectification,” is thought to
lead to recurrent experiences of shame and anxiety and to the increased
risk of eating, depressive and sexual disorders among females (Fredrickson & Roberts, 1997).
The Silencing the Self Scale (STSS; Jack, 1991; Jack & Dill, 1992)
was developed to assess the degree to which individuals have internalized gender-role stereotypes that are manifested in their attitudes and
behaviors in relationships (Jack, 1991; Jack & Dill, 1992). The term
self-silencing refers to what is initially an active process of withholding
emotions, opinions, strengths, and capabilities perceived to be threatening to one’s partner in order to maintain the relationship (Jack, 1999).
The self-silencing process is similar to the “central relational paradox,”
described by the relational-cultural theorists as the attempt to preserve
what little connection one has within a non-mutual relationship by paradoxically keeping important parts of the self out of relationship (Miller
& Stiver, 1997). In addition to the STSS Total scale, four separate
schemas reflecting gender-role stereotypes were identified and comprise
the four STSS subscales: (1) external standards are more important than
internal standards in defining one’s worth (Externalized Self-Perception), (2) caring for others in relationships necessitates self-sacrifice
(Care as Self-Sacrifice), (3) differing or conflicting emotions and opinions should be suppressed rather than expressed (Silencing the Self), and
(4) the outer self should be presented as compliant and “positive,” even if
one’s true internal feelings are “negative” or rebellious (Divided Self).
Given that the Silencing the Self Scale instrument has a subscale by the
same name, to reduce confusion, in this article, the term “self-silencing”
Wechsler et al.
55
will refer to the theory and/or the general construct of self-silencing,
“STSS” will refer to the instrument, “STSS Total” will refer to the entire scale score, and “Silencing the Self subscale” will refer to one of the
four separate subscales.
Self-silencing beliefs and strategies have been linked to depression in
women (Carr et al., 1996; Cramer, Gallant & Langlois, 2005; Jack &
Dill, 1992; Kayser et al., 1999; Thompson, 1995; Wechsler, 1999), decreased self-care (Kayser et al., 1999), a tendency toward unsafe sexual
behavior (Bruner, 1997), and reduced use of positive power strategies
(Cowan et al., 1995). In addition, recent work has established a negative
correlation between mutuality and self-silencing among female cancer
patients (Kayser, Sormanti & Strainchamps, 1999). However, certain
relational and social contexts appear to be more empowering for women
than other contexts. For instance, college women scored lower on selfsilencing than did women in a battered women’s shelter (Jack & Dill,
1992). Greater levels of self-silencing are correlated with poor self-esteem and experiences of physical and emotional abuse in a broader, heterogeneous sample of women drawn from shelters, community agencies,
and colleges (Woods, 1999). Self-silencing has also been associated with
a greater likelihood of a woman leaving a battered women’s shelter and
returning to her abusive partner (Pohle, 1996).
Recent investigations have begun to explore the link between selfsilencing, emotional eating, and disordered eating. For example, compared to psychiatric and non-psychiatric control groups, women with
anorexia nervosa had significantly higher scores on each of the STSS
subscales and higher anger suppression scores, even after controlling
for depression, self-esteem and global functioning (Geller, Cockell &
Goldner, 2000). For the entire sample, significant correlations emerged
between three STSS subscales (i.e., Care as Self-Sacrifice, Silencing
the Self, and Divided Self), and the emotional and cognitive aspects of
body image. In another investigation, the Externalized Self-Perception
subscale was found to predict anxiety-based eating and binge eating among
undergraduate women, while restrained eating was predicted by the Silencing the Self subscale (Smolak & Munstertieger, 2002). Additionally, the Externalized Self-Perception and Silencing the Self subscales
both predicted anger-based eating. Among lower division female undergraduates, McCann (1995) reported that the Care as Self-Sacrifice
subscale accounted for most of the association between the STSS and
the Eating Attitudes Test (EAT; Garner & Garfinkel, 1979). A very recent study using a community sample of young women given measures
56
JOURNAL OF COLLEGE STUDENT PSYCHOTHERAPY
of self-silencing, self-objectification and anger (Piran & Cormier, 2005)
found these variables were significant predictors of disordered eating.
The present study sought to extend the literature in several ways.
First, we attempted to replicate reported negative associations between
relational mutuality and self-silencing among female cancer patients
(Kayser, Sormanti & Strainchamps, 1999) in a healthy college population. Second, in contrast to previous research in college samples, which
generally has used brief screening measures, we used the more comprehensive EDI-2, a widely used and well-validated instrument. The EDI-2
was considered the most appropriate choice of instrument because it can
be administered individually or in groups in a relatively brief time, and
does not require specialized training to administer like some interview
measures. In addition, we were interested in sub-clinical features that
may precede full-blown symptoms of eating disorders rather than clinical diagnoses per se, and the EDI-2 has the advantage of measuring both
eating symptomatology and other psychological characteristics or attitudes associated with dysfunctional eating attitudes and behaviors.
Finally, this is the first study we know of that investigates the role of relational mutuality in connection with disordered eating.
Based on RCT and self-silencing theory, as well as previous research, we predicted that partner mutuality and self-silencing would be
negatively correlated. The EDI-2 scales Drive for Thinness, Bulimia,
Body Dissatisfaction, Interpersonal Distrust, and Interoceptive Awareness scales were each expected to correlate negatively with the partner
mutuality score, but to positively correlate with the STSS total score.
Among the STSS subscales, we hypothesized that (1) Externalized
Self-Perception would be correlated with Drive for Thinness and Body
Dissatisfaction, and (2) Silencing the Self and Divided Self would be
correlated with Interpersonal Distrust. We did not make predictions for
the STSS Care as Self-Sacrifice subscale because of the scale’s questionable reliability. Lastly, we predicted that a pattern would emerge
whereby higher EDI-2 scores would coincide with a combination of
lower partner mutuality scores and higher self-silencing scores (total
and subscale scores).
METHOD
Participants
The current sample comprised 149 female volunteers enrolled in undergraduate courses at a small public university primarily for women in
Wechsler et al.
57
the Southwest United States. Age ranged from 18 to 56 (M = 20.67; SD
= 5.50). In terms of ethnicity, 47% of the sample identified as Caucasian/European American (n = 71), 24% African American/Black (n =
36), 17% Latina/Hispanic (n = 26), 7% Asian American (n = 11), 1.3%
Native American (n = 2), and 2% endorsed “other” (n = 3). One participant did not indicate her ethnicity. The majority (94.6%) of the participants identified themselves as heterosexual, 2.1% lesbian (n = 3), and
1.4% bisexual (n = 2). Three participants did not indicate their sexual
orientation. In terms of relationship status, 30% of the sample indicated
they were not currently in a dating or partner relationship and consequently were excluded from analyses examining partner mutuality,
leaving an N of 105 participants for those tests. In addition, missing data
dropped the total N for STSS analyses to 144 and for other mutuality
analyses to 143.
Procedures and Instruments
All procedures were approved by the IRB of the women’s university.
Participants were recruited via flyers, letters to instructors, and classroom presentations. In addition to earning extra credit, students could
enter a drawing for a $50.00 store gift certificate. After signing consent
forms, participants received packets in which background questionnaires were presented first, while the order of the MPDQ, STSS, and
EDI-2 were counterbalanced to control for sequence effects.
In addition to a demographic questionnaire, each participant completed the Mutual Psychological Development Questionnaire (MPDQ;
Genero et al., 1992), which is a self-report instrument measuring perceived mutuality within close relationships. Twenty-two items on the
MPDQ are intended to measure the six elements of mutual interactions
(empathy, engagement, authenticity, zest, diversity and empowerment)
articulated by Miller (1988). Respondents rate one set of 11 MPDQ items
according to their own behavior or feelings in the relationship (e.g., “When
we talk about things that matter to my spouse/partner, I am likely to . . .
feel energized by our conversation”), then a second set of 11 items based on the responses of the other person involved in the relationship (e.g.,
“When we talk about things that matter to me, my spouse/partner is likely to . . . pick up on my feelings.”). Item and total scores on the MPDQ
can range on a 6-point Likert scale from 1 (“never,” indicating a low
level of mutuality) to 6 (“all the time,” indicating a high level of mutuality). The wording of items alternates between the positively stated or
58
JOURNAL OF COLLEGE STUDENT PSYCHOTHERAPY
desirable response (i.e., “try to understand”) and the undesirable response
(i.e., get frustrated") in order to control for response set. Internal consistency was established with .92 for partner and .89 for friend MPDQ
forms, with reliability estimates ranging from .86 to .93. The authors also
reported construct and concurrent validity with other measures of social
support, relationship satisfaction, and cohesion.
The Silencing The Self Scale (Jack, 1991) is a 31-item self-report measure derived from a longitudinal study of depressed women receiving
outpatient psychotherapy. Interviews were qualitatively analyzed for
the purpose of developing 5-point Likert items, with high scores indicating a greater number of self-silencing beliefs and/or behaviors. Five
of the items are reverse scored to control for response set. Jack and Dill
(1992) reported test-retest reliability ranging from .88 to .93 in an undergraduate sample, while internal consistency for the STSS Total score
ranged from .86 to .94. Construct validity was established via significant correlations between the STSS Total score and the Beck Depression Inventory (BDI; Beck, Ward, Mendelson, Mock & Erbaugh, 1961)
in the undergraduate sample, as well as a sample of women who abused
drugs and alcohol during pregnancy, and a sample drawn from a battered women’s shelter.
In addition to the STSS Total score, the STSS identifies four subscales. The Externalized Self-Perception subscale assesses the extent to
which one’s self-appraisals are other-determined (␣ = .75 to .83). The
Divided Self subscale assesses the extent to which one’s inner selfpresentation and perceived authenticity is discrepant from how one
actually appears or behaves with others (␣ = .86 to .94). Care as SelfSacrifice refers to the belief that caring for others and maintaining secure relationships are achieved through self-sacrifice (␣ = .60 to .81).
Due to some indications of low internal consistency, Jack and Dill suggested caution for separate interpretation of this subscale. Lastly, the
Silencing the Self subscale measures the extent to which self-expression
is inhibited and withheld in order to avoid conflict or to protect the relationship (␣ = .74 to .83). To reiterate, in order to reduce potential confusion caused by similar labels, the overall STSS score will be referred to
as STSS Total and the subscale will be referred to as the Silencing the
Self subscale. Stevens and Galvin (1995) have confirmed the four factor
structure of the instrument.
The Eating Disorder Inventory–Second Edition (EDI-2; Garner, 1991)
is a widely used 91-item self-report questionnaire that measures symptom clusters and psychological characteristics that have differentiated
individuals with eating disorders from those who do not have eating dis-
Wechsler et al.
59
orders. Items are answered on a 6-point rating scale ranging from “always” to “never.” Higher scores indicate the respondent is endorsing a
greater degree of symptoms, attitudes, or beliefs in the pathological
direction, similar to responses of individuals with diagnosed eating disorders. Norms are provided for separate diagnostic groups, but the combined eating disorder norms are considered to be sufficient for most
purposes. Adequate test-retest reliability has been established over three
weeks (Wear & Pratz, 1987) to one-year (Crowther, Lilly, Crawford,
Shepard & Oliver, 1990). Extensive data are reported in the EDI-2 manual to support construct validity (Garner, 1991).
The EDI-2 includes the original 64 items from the EDI (Garner,
Olmstead & Polivy, 1983), which correspond to three symptom and five
attitude scales, along with 27 new items that correspond to three provisional scales. Of the three symptom scales, the Drive for Thinness scale
measures anorexic symptoms such as preoccupation with weight and
dieting, fear of weight gain and restricted eating. The Bulimia scale measures tendencies toward binge eating, while Body Dissatisfaction assesses dissatisfaction with body areas such as the stomach, hips, thighs
and buttocks. With respect to the EDI-2’s more general scales assessing
psychological characteristics or attitudes, the Ineffectiveness scale measures generalized perceptions of inadequacy, insecurity and lack of control over one’s life, while Perfectionism is correlated with unrealistic
and excessive self-imposed standards. Interpersonal Distrust is associated with a tendency to avoid openness and intimacy in relationships.
Interoceptive Awareness measures confusion in recognizing and labeling emotions and body sensations, and Maturity Fears assesses fears
and reluctance about assuming adult roles and responsibilities. All scales
demonstrated adequate to high reliability, with Cronbach’s alphas ranging from .79 to .92 in non-clinical college samples.
The provisional EDI-2 scale of Asceticism is thought to assess a tendency to pursue spiritual virtues of self-discipline, restraint, sacrifice
and control of physical urges. Impulse Regulation is another provisional
scale designed to measure tendencies toward impulsivity, recklessness
and destructiveness. Social Insecurity measures the perceptions and
beliefs that relationships are generally tense, disappointing and unrewarding. Internal consistency estimates (Cronbach’s alpha) for the provisional scales ranged from poor (.44 for Asceticism) to adequate (.80) for
the non-clinical college samples.
60
JOURNAL OF COLLEGE STUDENT PSYCHOTHERAPY
RESULTS
Preliminary Analyses
The mean scores for partner MPDQ, STSS Total, STSS subscales
and all eleven of the EDI-2 scales are provided in Table 1. Significant
negative correlations were found between age and all STSS scales as
well as two EDI-2 scales (Interoceptive Awareness, Maturity Fears).
Among these significant correlations, the only one that was possibly
strong enough for practical relevance (Cohen, 1988) was the negative
correlation between age and STSS Externalized Self-Perception, suggesting that younger women tend to score higher, while older women
tend to score lower on Externalized Self-Perception. Subsequent analyses
involving Externalized Self-Perception accounted for age by introducing it as a covariate.
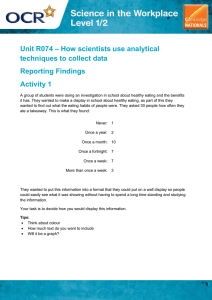
TABLE 1. Mutuality, Self-Silencing, and Disordered Eating: Means, Standard Deviations, and Correlations with Age
Scale
Mean
SD
r
3.45
2.29
.06
78.11
22.01
⫺.27**
Externalized self-perception
17.06
5.81
⫺.31***
Care as self-sacrifice
26.13
7.26
⫺.20*
Silencing the self
20.62
7.66
⫺.19*
Divided self
14.24
6.07
⫺.18*
Drive for thinness
5.94
5.69
⫺.03
Bulimia
1.56
2.92
⫺.02
11.11
8.30
⫺.00
Ineffectiveness
2.87
4.06
⫺.03
Perfectionism
7.77
4.21
⫺.13
Interpersonal distrust
2.88
3.39
⫺.09
Interoceptive awareness
3.82
4.55
⫺.18*
Maturity fears
3.71
3.92
⫺.17*
Asceticism
4.50
3.00
⫺.02
Impulse regulation
3.21
4.70
⫺.14
Social insecurity
3.37
3.40
⫺.04
MPDQ partner (N = 105)
STSS (N = 149)
EDI-2 (N = 149)
Body dissatisfaction
*p < .05,**p < .001,***p < .0001.
Wechsler et al.
61
To investigate potential differences among the mean test scores by
ethnic group, analysis of variance (ANOVA) tests were conducted. Dummy coding was used to form the ethnic groups and the smallest groups
(Native American and Other) were collapsed into one group (n = 5). The
overall F-test indicated significant differences among the groups on
STSS Total, F (4, 144) = 2.96, p = .02, as well as Externalized Self-Perception, F (4, 144) = 2.51, p = .04, and Divided Self scores, F (4, 144) =
4.19, p = .003. Post-hoc analyses utilizing the Least Significant Difference test indicated that Latinas scored significantly higher than Caucasians and Asian Americans on STSS Total, Externalized Self-Perception,
and Divided Self, while African American women scored significantly
higher than Caucasian and Asian-American women on Divided Self.
Subsequent analyses involving STSS Total, Externalized Self-Perception, and Divided Self accounted for these differences by using ethnic
group as a covariate.
Although the overall F-test indicated that relationship status was significantly associated with MPDQ partner mutuality, F (5, 143) = 16.92,
p < .001 and STSS Divided Self, F (5, 143) = 3.58, p = .004, no significant differences emerged in the post-hoc tests. STSS and MPDQ scales
were not related to relationship duration, academic class or sexual
orientation.
Primary Analyses
A Pearson r correlation coefficient was computed to determine the
degree of linear association between MPDQ partner scores and STSS
Total scores for only those participants reporting current dating or partner relationships (N = 105). As predicted, a significant negative correlation was found between partner mutuality and STSS Total (r = –.37, p =
.0001), with higher levels of partner mutuality associated with lower
levels of self-silencing.
With respect to the EDI-2 scales, partner mutuality was significantly
negatively correlated with Interpersonal Distrust (r = – .29, p < .001)
and Interoceptive Awareness (r = –.26, p = .004). However, the hypotheses that partner mutuality would be significantly negatively correlated
with Drive for Thinness (r = .24), Bulimia (r = –.007), and Body Dissatisfaction (r = –.058) were not supported.
Similarly, STSS Total was significantly positively correlated with
EDI-2 Interpersonal Distrust (r = .21, p = .006) and Interoceptive Awareness (r = .41, p = .01), but did not show expected correlations with EDI-2
Drive for Thinness (r = .18, p = .08), Bulimia (r = –.02, p = .41), and Body
62
JOURNAL OF COLLEGE STUDENT PSYCHOTHERAPY
Dissatisfaction (r = .13, p = .06). The four STSS subscales were expected to differ in their ability to predict disordered eating symptoms
and characteristics. Using age and ethnicity as covariates, a series of
multiple regression analyses was performed with the four STSS subscales as predictor variables for five of the EDI-2 scales (see Table 2).
As expected, STSS Externalized Self-Perception emerged as a significant positive predictor of Drive for Thinness, explaining 14% of the
variance, whereas STSS Care as Self-Sacrifice and African American
ethnicity were significant negative predictors of Drive for Thinness
[Adjusted R2 = .17, F (3, 141) = 10.47, p < .001]. STSS Externalized
Self-Perception was also a significant positive predictor of Bulimia, accounting for 9% of the variability, and the STSS Silencing the Self
subscale contributed an additional 2% but contrary to predictions was
negatively related to Bulimia, [Adjusted R2 = .11, F (2, 142) = 10.21,
p < .0001]. Of the four STSS scales, only Externalized Self-Perception
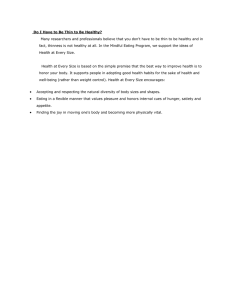
TABLE 2 . Regression Analyses: STSS Predictors of Dysfunctional Eating Patterns
Predictors
B
SE
Beta
t
Adj R2
Drive For Thinness
.472a
.088
.386
Care as self-sacrifice
⫺.132b
.077
⫺.210
⫺1.727*
.15
African American
⫺.169c
.999
⫺.129
⫺1.691*
.17
.21a
.04
.31
4.48***
.09
⫺.08b
.04
⫺.21
Ext self-perception
5.373***
.14
Bulimia
Ext self-perception
Silencing the self
⫺2.17*
.11
Body Dissatisfaction
.63a
.12
.394
5.16***
.14
3.19b
1.26
.193
2.53**
.17
Divided self
.14a
.05
.230
2.51**
.11
Silencing the self
.10b
.04
.198
2.17*
.11
Ext self-perception
.377a
.073
.430
5.19***
.29
Divided self
.320b
.063
.402
5.07***
.36
Care as self-sacrifice
.201c
.056
.262
3.61***
.38
⫺.197d
.058
⫺.302
⫺3.36***
.43
Ext self-perception
Caucasian
Interpersonal Distrust
Interoceptive Awareness
Silencing the self
*p < .05.**p < .01.***p < .001.
Wechsler et al.
63
emerged as a positive predictor of Body Dissatisfaction, as did Caucasian ethnicity [Adjusted R2 = .17, F (2, 142) = 15.42, p < .0001]. The
STSS Divided Self and Silencing the Self subscales were positive predictors and together accounted for 11% of the variability in EDI-2 Interpersonal Distrust [Adjusted R2 = .11, F (2, 142) = 11.50, p < .0001]. A
full 38% of the variability in EDI-2 Interoceptive Awareness was explained by three positive STSS predictors of Externalized Self-Perception, Divided Self and Care as Self-Sacrifice [Adj R2 = .38, F (3, 141) =
30.85, p < .0001]. In contrast to other STSS subscales, the Silencing the
Self subscale emerged as a significant negative predictor of Interoceptive
Awareness, accounting for an additional 5% of the variance [Adjusted
R2 = .43, F (4, 140) = 27.65, p < .0001].
A canonical correlation analysis was utilized to test the hypothesis
that discernible patterns would emerge among the mutuality, self-silencing
and disordered eating variables. The canonical correlation analysis yields
a Pearson correlation, rc that determines the strength of linear relationship between a cluster of dependent variable (covariates) scores and a
cluster of independent (canonical) variable scores. In this study, there
were eleven dependent variables, including scores on the eight original
EDI-2 scales and on the three EDI-2 provisional scales, while the cluster
of six independent variable scores included the MPDQ Partner score, STSS Total score and the four STSS subscale scores. Based on preliminary
findings, age and four of the ethnic groups were included as covariates.
When examined together, the correlations between dependent and
canonical variables (also known as structure coefficients), along with
the correlations between covariates and canonical variables, revealed
patterns of association between combinations of mutuality and self-silencing with disordered eating. Using Cohen’s (1988) conventionally
accepted minimum criteria, factor loadings and correlations between
covariates and canonical variables of .40 and higher were interpreted as
significant. It was predicted that a pattern of low mutuality combined
with high self-silencing (both Total and subscale scores) would be correlated with higher scores on all of the EDI-2 scales. Results of the canonical correlations analysis yielded mixed findings in support of this
hypothesis (see Table 3). As predicted, lower MPDQ scores and higher
STSS total scores were indeed correlated with higher scores on Ineffectiveness, Interpersonal Distrust, Interoceptive Awareness, Maturity Fears,
Impulse Regulation and Social Insecurity. Contrary to predictions, however, a combination of low MPDQ scores and high STSS total scores
was not significantly correlated with Drive for Thinness, Bulimia, Body
Dissatisfaction, Perfectionism or Asceticism.
64
⫺.17
⫺.54
⫺.36
⫺.15
⫺.30
.15
⫺.10
⫺.39
.22
.54
.03
⫺.05
⫺.12
.08
.61
.09
.33
.14
⫺.23
⫺.37
s
u
⫺.25
.13
.14
.14
.71*
.13
.49*
.68*
.51*
.12
.41*
.63*
.96*
.83
scl
.09
.10
.10
.51
.09
.36
.49
.37
.09
.30
.46
⫺.17
⫺.27
.07
.24
⫺.10
.67
scl
⫺.48
s2
.05
s1cl
.44
u1
u2
s1
s2
s1cl
.13
⫺.77
.32
.30
⫺.23
⫺.03
.04
⫺.33
.16
⫺.25
⫺.10
.41
⫺.32
⫺.10
⫺.25
⫺.62
⫺.23
⫺.81*
⫺.10
⫺.63
.02
⫺.07
⫺.13
.06
⫺.10
⫺.07
⫺.34
⫺.39*
⫺.14
⫺.30
.58
⫺.52
⫺.75*
.38
⫺.58
⫺.07
.05
.54*
⫺.09
⫺.42
.16
.30
⫺.21
⫺.24
⫺.16
.24
.47
⫺.49*
.34
⫺.38
⫺.14
⫺.38
⫺.62*
⫺.14
⫺.48
.20
⫺.06
.23
⫺.10
.18
.43
.68
.20
⫺.30
.16
.30
.96
⫺.07
.33
⫺.05
.22
.86
⫺.21
.09
⫺.16
.35
.56
.24
.11
.18
Redundancies given other set: 1 = 10.57%, 2 = 12.44
1. Rc = .77, F (80, 394) = 2.50, p < .0001
2. Rc = .63, F (60, 322) = 1.70
⫺.42
s1
.57*
v2
⫺.24
Self-Silencing Subscales
⫺.92*
⫺.29
⫺.72
.59
⫺.39
.30
⫺.35
.11
⫺.79
⫺.60*
⫺.32
⫺.46
.33
⫺.84
⫺.74*
.42*
⫺.56
Redundancies given other set: 1 = 26.49%, 2 = 3.62%
⫺.72
⫺.20
v1
.20
Note. v, u = standardized canonical weights. s = correlations of variables with factors. . scl = cross-loadings
* r = .40 and higher.
Rc = .72, F (32, 168) = 2.78, p < .0001
Drive for thinness
Bulimia
Body dissatisfactory
Ineffectiveness
Perfectionism
Interpers. distrust
Intero. awareness
Maturity fears
Asceticism
Impulse regulation
Social insecurity
Age
Caucasian
African American
Latina
Asian
Redundancies given other set = 8.01%
Covariate
MPDQ partner
STSS total
Ext. self-percept
Care-self-sacrifice
Silencing the self
Divided self
Redundancies given other set = 35.32%
Self-Silencing Total
v
s
⫺.31
⫺.66*
TABLE 3. Canonical Correlation of Partner Mutuality and Self-Silencing with Disordered Eating
.15
.21
⫺.09
⫺.06
⫺.19
.21
.06
.07
⫺.06
⫺.22
.10
⫺.06
⫺.06
.04
⫺.09
.24
s2cl
.01
.16
⫺.13
.23
s2cl
.02
Wechsler et al.
65
Interestingly, when separately examining the STSS subscales, the
findings of the canonical correlations analysis were similarly supportive of RCT, but from an inverse direction (see Table 3). Specifically,
high partner mutuality, in combination with low scores on STSS Externalized Self-Perception, Divided Self and Silencing the Self subscales
were correlated with low scores on EDI-2 Ineffectiveness, Interpersonal
Distrust, Interoceptive Awareness, Maturity Fears, Impulse Regulation
and Social Insecurity. Again contrary to the proposed hypotheses, Drive
for Thinness, Bulimia, Body Dissatisfaction, Perfectionism and Asceticism were not correlated with either combination of partner mutuality
and self-silencing.
DISCUSSION
The present study extends previous research by examining partner
mutuality and self-silencing in a healthy college population and exploring the associations of these two feminist constructs to dysfunctional
eating attitudes and behaviors measured by the EDI-2. Many of the current findings supported hypotheses based on relational-cultural theory
(RCT), revealing associations of partner relational mutuality and selfsilencing behaviors with psychological characteristics and/or symptoms
related to eating dysfunction.
Significant ethnic differences emerged in the present study with respect to certain aspects of self-silencing and disordered eating. African
American participants endorsed less preoccupation with weight and dieting behaviors (low Drive for Thinness), whereas Caucasian participants reported higher levels of Body Dissatisfaction. Current findings
are consistent with the suggestion that African American women are less
likely to adopt dominant cultural values regarding appearance (Powell &
Kahn, 1995) and support a general trend in the literature that has indicated ethno-cultural differences in body image (Wilfley, Schreiber, Pike
& Striegel-Moore, 1996), ideal body definitions (Powell & Kahn, 1995)
and vulnerability to the effect of mainstream media images on body image (Schooler, Ward, Merriwether & Caruthers, 2004). Given these and
other findings, college counselors should consider and assess potential
ethnic and cultural differences in self-silencing and disordered eating
attitudes and behaviors among their clients.
Results confirm theoretical expectations that high levels of relational
mutuality are associated with low levels of self-silencing and lend
weight to conjectures that some behaviors and attitudes associated with
66
JOURNAL OF COLLEGE STUDENT PSYCHOTHERAPY
disordered eating are inversely associated with partner mutuality and/or
positively associated with self-silencing behavior. RCT assumes that a
generalized sense of competence and power is promoted and even enhanced by experiencing and learning how to facilitate and maintain mutuality in relationships. In contrast, a sense of personal effectiveness is
diminished, inhibited, or discouraged in non-mutual relationships. Current findings support this notion, indicating that women who experience
low mutuality in their partner relationships, and who have internalized
stereotyped gender schemas regarding their worth and how they should
behave in relationships (high STSS scores), were more likely to feel ineffective and immature (high EDI-2 Ineffectiveness and Maturity Fears
scores). Accordingly, a greater sense of competency and maturity was
linked with a higher level of mutuality in partner relationships and decreased use of self-silencing strategies. Due to the correlational nature
of these findings, however, it cannot be determined whether maturity
fears develop and lead to involvement in relationships characterized by
low mutuality and high self-silencing, or whether involvement in nonmutual relationships and the internalization of gender stereotypical
relationship schemas result in greater fears about assuming adult roles
and responsibilities, as well as doubts about one’s effectiveness.
Also as predicted by RCT and Self-Silencing theories, results indicated that participants who typically inhibit authentic expression of self
in order to maintain partner relationships (high self-silencing) and also
rated their partner relationships as low in mutuality, were more likely to
experience a generalized sense of Interpersonal Distrust. It is possible
that individuals who are more distrusting initially are more likely to engage in non-mutual partner relationships. Alternatively, low mutuality
and high self-silencing may be precursors to problems with Interpersonal
Distrust. Prospective longitudinal studies are recommended to further
clarify the directionality of influence.
Interoceptive Awareness distinguished itself from other EDI-2 scales
in being most consistently linked with mutuality and self-silencing behaviors across the various analyses. As suggested by RCT, attunement
with internal emotional and bodily experiences is strongly interwoven
with the quality of these women’s significant relationships and the extent
to which authentic communication takes place within those relationships.
Self-silencing strategies are similar to the “strategies of disconnection”
described by RCT (Miller & Stiver, 1997) in reflecting a phenomena in
which authentic parts of self are inhibited within non-mutual relationships as a way to preserve connection, yet paradoxically result in greater
disconnection. Present findings suggest that when women experience
Wechsler et al.
67
confusion regarding their internal emotions and bodily/sensory states,
they may also rely on others’ opinions in determining their self-worth,
consequently sacrificing their own needs and inhibiting the authentic
self. Current results suggest it may be important to explore the culturally imposed value for women to sacrifice their own needs for the sake
of others (Gilligan, 1993) in relation to client eating behaviors in order
to foster a healthy balance between appropriate self-care and compassionate concern for others. In addition, therapeutic interventions working against the diet mentality to teach clients “attuned eating” (Bloom
et al., 1994) or “intuitive eating” (Tribole & Resch, 2003) may be important in counteracting poor interoceptive awareness. These interventions teach clients to recognize and trust their internal physical and
emotional signals for hunger and satiety, distinguish hunger/satiety from
emotional responses and to outwardly express their hunger by bringing
behavior into alignment with these signals (i.e., to stop eating when comfortably full and to eat in response to early hunger signals).
Contrary to predictions, however, Interoceptive Awareness was negatively related to the Silencing the Self subscale, which is thought to reflect a sophisticated, conscious strategy employed when a woman expects
or has learned that her true emotions and opinions are likely to be perceived as threatening by her partner (Jack, 1999). Upon closer examination of our own hypotheses, we realized that the ability to be attuned to
one’s inner experiences, while choosing to withhold them seems conceptually distinct from the lack of awareness and internal disconnection
that is reflected by high scores on the EDI-2 Interoceptive Awareness
scale. Moreover, the confusion about one’s internal sensory and emotional experiences, represented by high Interoceptive Awareness, implies limited self-awareness and self-knowledge, which would then
make it unlikely that an individual would know and be able to suppress
her authentic feelings and behaviors. Furthermore, the choice to withhold conflict-related expression from a partner, who is perceived to be
easily threatened by one’s authentic feelings, would seem to imply a lack
of trust, which is congruent with the finding that the Silencing the Self
subscale was positively associated with Interpersonal Distrust.
Although low partner mutuality was also associated with distrust in interpersonal relationships and a lack of internal attunement, counter to predictions, it was not directly associated with the EDI-2 symptom-focused
scales Drive for Thinness, Bulimia or Body Dissatisfaction in the present study. This pattern of findings is somewhat puzzling and suggests
that partner mutuality may be related to attitudinal or personality correlates of eating dysfunction, but not to the manifest symptoms of eating
68
JOURNAL OF COLLEGE STUDENT PSYCHOTHERAPY
disorder diagnoses. It is possible that partner mutuality serves a protective function, and when present tends to decrease the likelihood of
disordered eating symptoms; however, low mutuality in partner relationships may not, in and of itself, correspond with specific disordered eating symptoms unless other factors are also present. Another possible
explanation is the scoring method of the MPDQ, which allows low and
high scores to be interpreted more clearly than moderate scores, may
have affected the results. RCT proposes that women’s psychological
health is strongly influenced by their level of participation and giving in
relationships, and by their level of receiving in relationships. However,
it cannot be precisely known from the current results the extent to which
MPDQ scores reflect perceptions of being the less mutual partner in an
intimate relationship or perceptions of the other person as being the less
mutual partner.
In contrast to the lack of direct associations between mutuality and the
three symptom scales, the Silencing the Self subscale was negatively
associated with Bulimia, whereas Externalized Self-Perception was positively associated with Bulimia, Drive for Thinness and Body Dissatisfaction. In a recent study, the STSS Externalized Self-Perception and
Silencing the Self subscales were both linked to restrained eating, while
Externalized Self-Perception alone was correlated with binge eating
(Smolak & Munstertieger, 2002). Current results support those findings
suggesting that Externalized Self-Perception may be reliably associated
with binge-eating or bulimic symptoms. In addition, although the Silencing the Self subscale did not correspond with Drive for Thinness in
the multiple regression analyses, low Silencing the Self subscale scores,
in combination with low scores on Externalized Self-Perception, were
associated with low scores on Drive for Thinness in the canonical correlation analyses. Taken together with Smolak and Munstertieger’s findings, these results suggest that the strategy of self-silencing may be
more characteristic of women who restrain eating than those who binge
eat. From a clinical standpoint, restrained or anorexic eating patterns may
parallel a restriction of affect or withholding of self-expression in personal relationships. Correspondingly, bulimic eating patterns that vacillate
between the extremes of restraint, binge eating and purging, may reflect a
tendency to fluctuate between radical self-control and impulsive selfexpression.
Interestingly, in canonical correlations, both relational mutuality and
STSS were more strongly related to the attitudinal/trait aspects of the
EDI-2 rather than the symptom scales. This pattern may simply reflect
the nature of the current college sample, which is less likely to show
Wechsler et al.
69
high levels of clinical symptomatology than psychiatric samples. However, it may also be true that these feminist constructs are related more
generally to psychological characteristics represented by the EDI-2 attitude scales, which accompany not only eating disorders but also other
forms of psychological distress as well. For example, a sense of ineffectiveness is common to depression, anxiety and avoidant personality disorder. Alternatively, based on previous research demonstrating links
between eating disorders and defensive strategies formed in early attachment relationships (e.g, Cole-Detke & Kobak, 1996; see Ward,
Ramsay & Treasure, 2000, for comprehensive review), it is conceivable
that long-standing attachments with parents rather than current partner
attachments have more direct influence on the development of eating
disorder symptoms. While low mutuality and self-silencing in adult
partner relationships may be disappointing and/or unhealthy, and consequently related to maladaptive attitudes that often accompany eating
disorders, they may contribute only indirectly to primary eating disorder
symptoms via their relationships with other developmental influences,
such as a history of poor parent-child attachment. Research examining
these constructs in clinical samples and in conjunction with measures of
early parent-child relationships is needed to clarify the meaning of current findings.
Results also support RCT and other feminist relational theories,
which assert that restrained eating or anorexic symptoms reflect the
most rigid adherence to external beauty standards. Based on the current
pattern of associations, it appears that the relentless pursuit of thinness is
less likely to emerge for college women who rely more on self-defined
values and behaviors in relationships, as opposed to gender-stereotypical
standards. Accordingly, greater allegiance to traditional gender-role beliefs and behaviors in relationships may coincide with an extreme focus
on appearance, thinness and restrained eating. Furthermore, self-silencing alone may not necessarily be associated with believing one must be
thin, unless it is coupled with a pervasive tendency to evaluate the self
from an external perspective. In other words, when low, Externalized
Self-Perception may have a buffering influence with respect to Drive
for Thinness, but an exacerbating influence when scores are high. Although further research is needed to replicate these findings, clinicians
may find it useful to inquire about both self-silencing and outer-directed
self-perceptions, with an awareness that the presence of both these tendencies together may be a red flag for increased client vulnerability to
disordered eating. Assessment and early intervention with these particu-
70
JOURNAL OF COLLEGE STUDENT PSYCHOTHERAPY
lar cognitive schemas in therapy might serve a preventive function with
respect to disordered eating.
The positive correlation between Externalized Self-Perception and
Body Dissatisfaction underscores the importance of exploring in either
individual or couple therapy the extent to which female clients perceive
their intimate partners as subscribing to the dominant masculine-defined
beauty standards that are portrayed in media images and the larger culture.
Psycho-educational, CBT and feminist interventions also might be appropriate for addressing the role of Externalized Self-Perception in disordered eating symptoms. Feminist therapy methods such as consciousnessraising have been utilized in individual therapy (Boskind-White & White,
2000; Pipher, 1995) and can be applied in workshops and/or therapy
groups that tackle topics such as body acceptance and the media’s influence on negative body image, and also teach participants to become
critical and judicious media consumers. Specific group interventions
might include identifying emotions that commercials are designed to
elicit from viewers and the use of homework assignments instructing
clients to talk back to the television by disagreeing with messages or images or to switch channels or turn off material that is offensive and damaging (Pipher, 1995). Feminist theory also encourages social activism
(Marecek, 2002), which can take the form of boycotting companies and
products, writing letters of protest to companies that use demeaning or
stereotyped images and writing letters of support to companies that promote healthy messages regarding females and female bodies in their advertisements.
In a related vein, cognitive-behavioral therapies (CBT) that incorporate a body-image awareness component have been found to be effective
in the treatment of obesity (Ramirez & Rosen, 2001) and body-dysmorphic
disorder (Rosen, Reiter & Orosan, 1995). Cognitive-behavioral Internetbased interventions have likewise shown success in reducing potential
risk factors for disturbed eating, using a combination of psychoeducation
about eating disorders, challenges to cultural and media factors contributing to body image, and CBT interventions for improving body satisfaction (Winzelberg, Eppstein, Eldredge, Wilfley, Dasmahapatra, Dev
& Taylor, 2000; Zabinski, Wilfley, Calfas, Winzelberg & Taylor, 2004).
CONCLUSION
Current findings indicate that feminist relational theories of women’s
psychological development continue to find support and relevance, not
Wechsler et al.
71
just clinically, but empirically. Results of the current study indicated
that the lack of mutuality in partner relationships is related to attitudinal
features associated with eating dysfunction and provided evidence linking the use of self-silencing strategies to psychological symptoms of
distress in the form of disordered eating patterns. However, several limitations should be considered. First, the data from this study are correlational in nature and therefore interpretations are limited regarding
the directionality of associations among mutuality, self-silencing and
disordered eating symptoms and traits. Subsequent studies utilizing a
prospective longitudinal design are needed to address causality. Also,
the use of self-report data may result in either under-reporting or overreporting of disordered eating symptoms and traits. In particular, since
intimate partners did not participate in the study, the self-reported ratings of partner mutuality and self-silencing behavior may be limited in
their accuracy. In addition, although the EDI-2 is one of the most widely
used assessments of eating dysfunction with good psychometric properties, future research may want to employ an interview-based measure,
such as the Eating Disorders Examination (Cooper & Fairburn, 1987),
which may be less susceptible to some of the limitations of self-report
pen-and-paper instruments. Finally, generalizability of these findings
may be limited. Because this study used a sub-clinical collegiate sample, the findings may be most relevant for counselors working at university counseling centers rather than other clinical settings.
The findings that mutuality and self-silencing were associated with a
number of the EDI-2 scales in the present study provides support for the
role of interpersonal and internalized gender-role schemas in the development of dysfunctional eating patterns. In particular, it appears that
Externalized Self-Perception is an especially salient dimension of the
self-silencing process with respect to disordered eating. When concerned about potential eating problems in clients, clinicians may wish to
pay particular attention to the degree to which clients exhibit a tendency
to judge themselves by external standards rather than their own internal
standards. However, it appears that the patterns of association between
mutuality and/or self-silencing and disordered eating are complex and
warrant ongoing investigation. Interpersonal factors likely constitute
just some of the influences among the many to be explored. The development of eating problems stems from multidimensional pathways
(O’Kearney, 1996; Suldo & Sandberg, 2000), including biogenetic predisposing factors, past and current family system functioning, symbolic
reenactment of childhood trauma (Gay, 1996; Schneer, 2002), susceptibility to media images (Irving & Berel, 2002; Schooler, Ward, Merri-
72
JOURNAL OF COLLEGE STUDENT PSYCHOTHERAPY
wether & Carruthers, 2004) and self-objectification (Calogero, 2004;
Fredrickson & Roberts, 1997), among others. Researchers and clinicians
must keep in mind this broad context of development in order to more
fully study and understand eating disorders and subsequently develop
comprehensive treatment plans to address multiple levels of influence in
the lives of their clients.
REFERENCES
Beck, A.T., Ward, C., Mendelson, M., Mock, J., & Erbaugh, J. (1961). An inventory
for measuring depression. Archives of General Psychiatry, 4, 892-898.
Bloom, C., Gitter, A., Gutwill, S., Kogel, L., & Zaphiropoulos, L. (Eds.). (1994). Eating problems: A feminist psychoanalytic treatment model. New York: Basic Books.
Boskind-White, M., & White, W.C. (2000). Bulimia/anorexia: The binge/purge cycle
and self-starvation. New York: W.W. Norton & Co.
Bruner, L.A. (1997). The relationship of college women’s self-silencing and safer sex
behaviors. (Doctoral dissertation, University of Pittsburgh, 1997). Dissertation
Abstracts International, 58, (6-B), 3366.
Calogero, R.M. (2004). A test of objectification theory: The effect of the male gaze
onappearance concerns in college women. Psychology of Women Quarterly, 28,
16-21.
Carr, J.G., Gilroy, F.D., & Sherman, M.F. (1996). Silencing the self and depression
among women: The moderating role of race. Psychology of Women Quarterly, 20,
375-392.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.).
Hillsdale, NJ: Erlbaum.
Cowan, G., Bommersbach, M., & Curtis, S.R. (1995). Codependency, loss of self, and
power. Psychology of Women Quarterly, 19, 221-236.
Cole-Detke, H., & Kobak, R. (1996). Attachment processes in eating disorder and depression. Journal of Consulting and Clinical Psychology, 64, 282-290.
Cooper, Z., & Fairburn, C. (1987). The Eating Disorder Examination: A semi-structured interview for the assessment of specific psychopathology of eating disorders.
International Journal of Eating Disorders, 6, 1-8.
Cramer, K.M., Gallant, M.D., & Langlois, M.W. (2005). Self-silencing and depression
in women and men: Comparative structural equation models. Personality and Individual Differences, 39, 581-592.
Fossum, J.L. (1996). A correlational study of feminist/womanist identity development
and depression in women. (Doctoral dissertation, University of Southern California, 1996). Dissertation Abstracts International, 58, (1-B), 415.
Fredrickson, B.L., & Roberts, T.A. (1997). Objectification theory: Toward an understanding of women’s lived experiences and mental health risks. Psychology of
Women Quarterly, 21, 173-206.
Garner, D.M. (1991). The Eating Disorder Inventory - Second edition manual. Odessa,
FL: Psychological Assessment Resources.
Wechsler et al.
73
Garner, D.M., & Garfinkel, P.E. (1979). The Eating Attitudes Test: An index of the
symptoms of anorexia nervosa. Psychological Medicine, 9, 273-279.
Garner, D.M., Olmsted, M.P., & Polivy, J. (1983). Development and validation of a
multidimensional Eating Disorder Inventory for anorexia nervosa and bulimia.
International Journal of Eating Disorders, 2, 15-34.
Geller, J., Cockell, S.J., & Goldner, E.M. (2000). Inhibited expression of negative
emotions and interpersonal orientation in anorexia nervosa. International Journal
of Eating Disorders, 28, 8-19.
Genero, N.P., Miller, J.B., Surrey, J., & Baldwin, L.M. (1992). Measuring perceived
mutuality in close relationships: Validation of the Mutual Psychological Development Questionnaire. Journal of Family Psychology, 6, 36-48.
Gilligan, C. (1993). In a different voice: Psychological theory and women’s development. Cambridge, MA: Harvard University Press.
Hirsch, T.G. (1999). Relational identity, psychological differentiation, perceived social support, and eating attitudes in college women. (Doctoral dissertation, Temple
University). Dissertation Abstracts International, 59 (10-B), 5577.
Irving, L.M., & Berel, S.R. (2001). Comparison of media-literacy programs to strengthen
college women’s resistance to media images. Psychology of Women Quarterly, 25,
103-111.
Jack, D.C. (1999). Silencing the self: Inner dialogues and outer realities. In T. Joiner &
J.C.Coyne (Eds.), The interactional nature of depression: Advances in interpersonal
approaches (pp. 221-246). Washington, DC: American Psychological Association.
Jack, D.C. (1991). Silencing the self: Women and depression. Cambridge, MA: Harvard University Press.
Jack, D.C., & Dill, D. (1992). The Silencing the Self Scale: Schemas of intimacy associated with depression in women. Psychology of Women Quarterly, 16, 97-106.
Jackson, T., Weiss, K. E., Lunquist, J. J. & Soderlind, A. (2005). Sociotropy and perceptions of interpersonal relationships as predictors of eating disturbances among
college women Two prospective studies. Journal of Genetic Psychology, 166,
346-359.
Johnston, A. (1996). Eating in the light of the moon: How women can transform their
relationships with food through myths, metaphors and storytelling. Carlsbad, CA:
Gurze.
Jordan, J.V. (1991). The meaning of mutuality. In J.V. Jordan, A.G. Kaplan, J.B.
Miller, I.P. Stiver & J.L. Surrey (Eds.), Women’s growth in connection: Writings
from the Stone Center (pp. 81-96). New York: Guilford Press.
Jordan, J.V. (1997). A relational perspective for understanding women’s development.
In J.V. Jordan (Ed.), Women’s growth in diversity: More writings from the Stone
Center (pp. 9-24). New York: The Guilford Press.
Kaschak, E. (1992). Engendered lives: A new psychology of women’s experience. New
York: Basic Books.
Kayser, K., Sormanti, M., & Strainchamps, E. (1999). Women coping with cancer: The
influence of relationship factors on psychosocial adjustment. Psychology of Women
Quarterly, 23, 725-739.
74
JOURNAL OF COLLEGE STUDENT PSYCHOTHERAPY
Lippes, T.E. (1999). Mutuality in marriage: The self-esteem connection. A self-in-relation analysis. (Doctoral dissertation, Chicago School of Professional Psychology).
Dissertation Abstracts International, 59 (9-B), 5095.
Marecek, J. (2002). Unfinished business: Postmodern feminism in personality psychology. In M. Ballou & L.S. Brown (Eds.), Rethinking mental health and disorder:
Feminist perspectives (pp. 3-28). New York: Guilford.
McCann, M.E. (1995). The silence that speaks through the belly’s roar: A study of eating disorders, depression, and self-silencing. (Doctoral dissertation, Harvard University, 1995). Dissertation Abstracts International, 55, (7-A), 1879.
Miller, J.B. (1986). Toward a new psychology of women (2nd ed.). Boston: Beacon
Press.
Miller, J.B. (1988). Connections, disconnections and violations (Work in Progress, No.
33). Wellesley, MA: Stone Center, Wellesley College.
Miller, J.B., & Stiver, I.P. (1997). The healing connection: How women form relationships in therapy and in life. Boston: Beacon Press.
Mintz, L., & Betz, N. (1988). Prevalence and correlates of eating disordered behaviors
among undergraduate women. Journal of Counseling Psychology, 35, 463-471.
O’Kearney, R. (1996). Attachment disruption in anorexia nervosa and bulimia nervosa:
A review of theory and empirical research. International Journal of Eating Disorders, 20, 115-127.
Paxton, S.J., & Plythian, K. (1999). Body image, self-esteem, and health status in middle and late adulthood. Australian Psychologist, 34, 116-121.
Pipher, M. (1995). Hunger pains: The modern woman’s tragic quest for thinness. New
York: Ballantine.
Piran, N. & Cormier, H. C. (2005). The social construction of women and disordered
eating patterns. Journal of Counseling Psychology, 52, 549-558.
Pohle, M.S. (1996). Battered women: Self-Definition. (Doctoral dissertation, The
Fielding Institute). Dissertation Abstracts International, 57 (2-B), 1480.
Polivy, J., & Herman, C.P. (1995). Dieting and its relation to eating disorders. In K.D.
Brownell & C.G. Fairburn (Eds.), Eating disorders and obesity: A comprehensive
handbook (pp. 83-86). New York: Guilford Press.
Powell, A.D., & Kahn, A.S. (1995). Racial differences in women’s desires to be thin.
International Journal of Eating Disorders, 17, 191-195.
Ramirez, E. M. & Rosen, J. C. (2001). A comparison of weight control and weight control plus body image therapy for obese men and women. Journal of Consulting and
Clinical Psychology. 69, 440-446.
Rodin, J., Silberstein, L.R., & Striegel-Moore, R.H. (1985). Women and weight: A
normative discontent. In T.B. Sonderegger (Ed.), Nebraska symposium on motivation: Vol. 32, Psychology and gender (pp. 267-307). Lincoln: University of Nebraska
Press.
Rosen, J.C., Reiter, J., & Orosan, P.(1995). Cognitive-behavioral body image therapy
for body dysmorphic disorder. Journal of Consulting and Clinical Psychology, 63,
263-269.
Schooler, D., Ward, L.M., Merriwether, A., & Caruthers, A. (2004). Who’s that girl:
Television’s role in the body image development of young White and Black
women. Psychology of Women Quarterly, 28, 38-47.
Wechsler et al.
75
Smolak, L., & Murnen, S.K. (2001). Gender and eating problems. In R.H. StriegelMoore & L. Smolak (Eds.), Eating disorders: Innovative directions in research and
practice. Washington, DC: American Psychological Association.
Sperberg, E.D., & Stabb, S.D. (1998). Depression in women as related to anger and
mutuality in relationships. Psychology of Women Quarterly, 22, 223-238.
Spitzer, B.L., Henderson, K.A., & Zivian, M.T. (1999). Gender differences in population versus media body sizes: A comparison over four decades. Sex Roles, 40,
545-565.
Stevens, H.B., & Galvin, S.L. (1995). Structural findings regarding the Silencing the
Self Scale. Psychological Reports, 77, 11-17.
Stice, E., Nemeroff, C., & Shaw, H.E. (1996). Test of the dual pathway model of
bulimia nervosa: Evidence for dietary restraint and affect regulation mechanisms.
Journal of Social and Clinical Psychology, 15, 340-363.
Strober, M., & Katz, J. (1988). Depression in the eating disorders: A review and analysis of descriptive, family and biological factors. In D.M. Garner and P.E. Garfinkel
(Eds.), Diagnostic issues in anorexia and bulimia nervosa (pp. 80-111). New York:
Brunner/Mazel.
Suldo, S.M., & Sandberg, D.A. (2000). Relationship between attachment styles and
eating disorder symptomatology among college women. Journal of College Student Psychotherapy, 15, 59-73.
Surrey, J.L. (1991). Eating patterns as a reflection of women’s development. In J.V.
Jordan, A.G. Kaplan, J.B. Miller, I.P. Stiver and J.L. Surrey (Eds.), Women’s
growth in connection: Writings from the Stone Center (pp. 237-249). New York:
The Guilford Press.
Thompson, J.M. (1995). Silencing the self: Depressive symptomatology and close relationships. Psychology of Women Quarterly, 19, 337-353.
Tiggemann, M., & Lynch, J.E. (2001). Body image across the life span in adult women:
The role of self-objectification. Developmental Psychology, 37, 243-253.
Tribole, E., & Resch, E. (2003). Intuitive eating: A revolutionary program that works.
New York: St. Martin’s Griffin.
Ward, A., Ramsay, R., & Treasure, J. (2000). Attachment research in eating disorders.
British Journal of Medical Psychology, 73, 35-51.
Webster, J., & Tiggemann, M. (2003). The relationship between women’s body satisfaction and self-image across the life span: The role of cognitive control. Journal of
Genetic Psychology, 164, 241-252.
Wechsler, L.S. (1999). Acculturation, self-silencing and depression in Asian American
college women. Unpublished manuscript, Texas Woman’s University.
Wilfley, D.E., Schreiber, G.B., Pike, K.M., & Striegel-Moore, R.H. (1996). Eating disturbance and body image: A comparison of a community sample of adult Black and
White women. International Journal of Eating Disorders, 20, 377-387.
Winzelberg, A.J., Eppstein, D., Eldredge, K. L., Wilfley, D., Dasmahapatra, R., Dev, P.
& Taylor, C.B. (2000). Effectiveness of an Internet-based program for reducing
risk factors for eating disorders. Journal of Consulting and Clinical Psychology, 68,
346-350.
76
JOURNAL OF COLLEGE STUDENT PSYCHOTHERAPY
Woods, S.J. (1999). Normative beliefs regarding the maintenance of intimate relationships among abused and nonabused women. Journal of Interpersonal Violence, 14,
479- 491.
Zabinski, M.F., Wilfley, D.E., Calfas, K.J., Winzelberg, A.J. & Taylor, C.B. (2004).
An interactive psychoeducational intervention for women at risk of developing an
eating disorder. Journal of Consulting and Clinical Psychology, 72, 914-919.
RECEIVED: 01/06/06
REVISED/ACCEPTED: 03/10/06