Nitric oxide synthase in retina and optic nerve head of

Brain Research Bulletin 70 (2006) 406–413
Nitric oxide synthase in retina and optic nerve head of rat with increased intraocular pressure and effect of timolol
Lourdes Vidal
, Florent´ına D´ıaz
Jos´e Garc´ıa Campos
, Alicia Villena
, Mercedes Moreno
, Ignacio P´erez de Vargas
,
a
Department of Histology and Histopathology, School of Medicine, University of Malaga, Boulevard Louis Pasteur 32, 29071 Malaga, Spain b
Department of Ophthalmology, Snchool of Medicine, University of Malaga, Malaga, Spain
Received 3 May 2006; received in revised form 23 June 2006; accepted 14 July 2006
Available online 7 August 2006
Abstract
We investigated the expression of nitric oxide synthase (NOS) isoforms -1, -2 and -3 in the retina and optic nerve head (ONH) in an experimental rat model of elevated intraocular pressure (IOP) before and after treatment with timolol, to assess whether its neuroprotective action is associated with the activity of these enzymes. Episcleral vein cauterization in unilateral eyes of Wistar rats was performed to produce elevated IOP. Histological sections of retina and ONH from animals with normal IOP, with elevated IOP, and elevated IOP treated with timolol, were studied by immunohistochemistry with antibodies to NOS-1, NOS-2, and NOS-3. In the control rats, NOS-1 was localized to photoreceptor inner segments, amacrine cells and bipolar cells in the retina, and in astrocytes, pericytes and vascular nitrergic terminals in the ONH. NOS-3 immunostaining localized to the endothelial cells. The rats with elevated IOP showed increased expression of NOS-1 in the plexiform layers of the retina and reactive astrocytes in the ONH.
These cells also showed NOS-2 positivity. The rats treated with timolol showed reduced expression of NOS-1 in the retina and ONH. NOS-2 was only detected in a few groups of astrocytes in the ONH. NOS-3 was unchanged in both elevated IOP and timolol-treated groups. These results show that excessive levels of NO synthesized by the NOS-1 and -2 isoforms, considered neurotoxic, might contribute to the progressive lesions of retinal ganglion cell axons. Their reduction after treatment suggests a possible neuroprotective effect of timolol in neurons exposed to excessive amounts of NO.
© 2006 Elsevier Inc. All rights reserved.
Keywords: Immunohistochemistry; Intraocular pressure; Nitric oxide synthase; Optic nerve head; Retina; Timolol
1. Introduction
Glaucoma is a slowly progressive optic neuropathy that causes loss of retinal ganglion cells (RGC), changes in the optic nerve head (ONH) and a characteristic visual field defect. Elevated intraocular pressure (IOP) is considered to be the main risk factor for the development of the changes characteristic of glaucomatous optic neuropathy in the retina and in the ONH.
The mechanisms that lead to the neurodegenerative lesions are unclear
[4,36,37] . The most accepted possibilities are mechan-
ical compression of the axons of the RGC at the level of the cribrous lamina
[49] and alterations in vascular perfusion caus-
ing ischemia in the ONH
∗
Corresponding author. Tel.: +34 952131595; fax: +34 952131592.
E-mail address: lvidal@uma.es
(L. Vidal).
0361-9230/$ – see front matter © 2006 Elsevier Inc. All rights reserved.
doi: 10.1016/j.brainresbull.2006.07.009
Several changes might have a neurodegenerative effect in glaucoma, including molecular changes in the components of the extracellular matrix of the cribriform plates
tosis of the RGC due to lack of neurotrophic factors
excitotoxicity from an increased glutamate concentration
Likewise, astrocytes, the main cell type in the ONH
been suggested as possible initiating agents of the lesions associated with glaucomatous optic neuropathy
vital for maintenance of the normal physiology of the RGC.
They are activated in response to mechanical and ischemic factors
[13,58] and in the initial stages of their activation they may
have a direct toxic effect on the axons of the RGC, producing elevated levels of nitric oxide (NO)
Nitric oxide acts as a regulator of different physiological processes in numerous tissues. In the eye it is involved in the regulation of IOP. A small amount of NO production is beneficial to the retina as it can up-regulate the blood circulation and
L. Vidal et al. / Brain Research Bulletin 70 (2006) 406–413 thus facilitate the flow of metabolites
conditions, however, such as human neurodegenerative diseases, and in animal models of neurodegeneration, NO can have a neurodestructive or a neuroprotective action, or both
Nitric oxide is produced by the enzyme nitric oxide synthase
(NOS), for which three isoforms have been identified: neuronal
NOS (nNOS or NOS-1), endothelial NOS (eNOS or NOS-3) and inducible NOS (iNOS or NOS-2). The first two isoforms are constitutive and are normally expressed. They produce low levels of NO, which is thought to have homeostatic and regulatory functions. NOS-2 is not expressed under normal conditions, and it is primarily involved in inflammatory processes
Several different studies in the retina of humans, rats and other mammals have shown immunoreactivity for NOS-1 in diverse types of amacrine cells
[4,6,20,40] , as well as in horizontal and
interplexiform cells
[48,61] , ganglion cells [48] and bipolar cells
[21,28,48] . Positivity has also been seen in the inner segments
of the photoreceptors
The constitutive isoforms of NOS are present under normal conditions in the ONH of humans
have shown variation in the expression of the three isoforms in primary open angle glaucoma in humans
mental rat model
In order to examine further the cell mechanisms that contribute to glaucomatous optic neuropathy we used an experimental rat model of elevated IOP, based on the cauterization of three episcleral veins, similar to that developed by Shareef et al.
[52] . We have previously shown that chronic IOP elevation
causes a 33% loss of cells in the ganglion layer of the retina
Submitting these rats to topical treatment with timolol, a nonselective beta-blocker, significantly reduced the IOP, as well as resulting in a lower cell loss in the ganglion cell layer, as compared with untreated animals, although partial blockade of the axoplasmic transport persisted in the ONH
In this study we attempted to determine whether the neuroprotective action of timolol is associated with NOS activity.
Accordingly, we examined the expression of the different isoforms of NOS in the retina and the ONH of rats submitted to experimental elevation of the IOP for 3 months and after topical treatment with timolol under the same experimental conditions.
2.4. Immunohistochemical procedure
407 of 8% chloral hydrate (0.1 ml per 30 g body weight). Right eye limbus-draining veins were exposed by incising the conjunctiva and three of the four veins were cauterized using a small vessel cauterizer (Ophthalmic Cautery-Cautere, Moria,
Antony, France)
[16,32,52] . After ocular surgery, the eyes were treated topically
with an antibiotic (Tobrex
®
, Alcon Cus´ı S.A., Barcelona, Spain) during recovery.
The rats were immediately divided into two groups, an untreated group and a group treated with timolol (Timoftol
®
, MSD de Espa˜na, S.A.), and were caged individually. In the treated group, after verifying that the IOP remained elevated for 2 weeks, treatment was started by instilling in the operated eye two drops per day (every 12 h) of timolol for 10 weeks, thus completing the period of 3 months after the surgical procedure. All ocular tissues, including the cornea, lens and sclera, appeared normal throughout the experiment.
2.3. Measurement of intraocular pressure
The IOP of both eyes was measured using a calibrated Tono-Pen XL tonometer (Mentor Ophthalmics Inc., Norwell, MA, USA) before and immediately after cauterization and every 2 weeks for 3 months, as well as immediately before perfusion. After instillation of a drop of topical anesthetic (proparacaine hydrochloride; Alcon Inc., Mississauga ON, Canada) and with the eye under good illumination, the Tono-Pen was oriented perpendicular to the cornea and, using a swift and steady stroke, the tip was brought into contact with the cornea
[35] . Each IOP registered was the average of three consecutive measurements
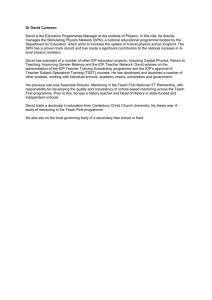
made at the same time of day (10 a.m. to noon). The average IOP in the control eyes was 14.85
±
0.65 mmHg. Immediately after the surgical procedure, the mean IOP in the experimental eyes increased to 33.5
±
1.06 mmHg. The IOP remained significantly elevated for the entire duration of the experiment. Before starting treatment in the treated group, the IOP was 34.91
±
1.12 mmHg; after starting treatment the IOP fell to normal, with a mean value at the end of the treatment phase of 14.05
±
Under deep anesthesia, as described above, we performed perfusion through the heart in control, experimental and timolol-treated animals with 0.1 M phosphate buffer (pH 7.4) and 4% paraformaldehyde in 0.1 M phosphate buffer (pH
7.4). After perfusion, the eyeballs were removed and postfixed in the same fixative for 4 h, transferred into ethanol 70
◦
C and processed following the protocol for embedding in paraffin. Longitudinal sections 6
m thick were prepared.
The sections were mounted onto pre-treated glass slides. They were deparaffined in xylene and rehydrated with distilled water through the conventional ethanol scale, preincubated in citrate buffer (pH 6.0) in a pressure cooker and treated with 0.06% H
2
O
2 for 15 min. The sections were then incubated overnight with primary NOS-1 (Santa Cruz Biotechnology, CA, USA; dilution 1:300),
NOS-2 (BD Transduction Laboratories, CA, USA; dilution 1:25), NOS-3 (Santa
Cruz Biotechnology, CA, USA; dilution 1:500) and GFAP (Glial fibrillary acidic protein) (DAKO, Denmark; dilution 1:1000) antibodies. The slides were rinsed
2. Material and methods
2.1. Subjects
We used 38 adult, male Wistar rats (Charles River Laboratories, Barcelona,
Spain), weighing 250–300 g at the start of the experiment. The rats were divided into three groups: control ( n = 14), experimental ( n = 14) and experimental treated with timolol ( n = 10). They were housed in individual home cages in an air-conditioned room (21
±
1
◦
C with 66
±
3% humidity) with a 12 h light–dark diurnal cycle. They had free access to food (dry pellets) and tap water. To minimize animal suffering and the number of animals used, the experiments were carried out in accordance with the guidelines of the European Union Council (86/609/EU) for the use of laboratory animals, and were approved by the
Scientific Committee of Malaga University.
2.2. Surgical procedure
All ocular surgical procedures were unilateral, with the contralateral eye remaining untouched. Rats were deeply anesthetized by intraperitoneal injection
Fig. 1. Comparison of the intraocular pressure between control eyes, experimental eyes and eyes treated with timolol. Measurements were made each 2 weeks. Data are the mean
±
S.E.M. of the results in each group.
408 L. Vidal et al. / Brain Research Bulletin 70 (2006) 406–413
Fig. 2. Immunohistochemistry for NOS in the rat retina: (A) control group. NOS-1 positivity in the photoreceptor inner segments (asterisk), in some bipolar cells
(white arrow), amacrine cells, and displaced amacrine cells (arrows); (B) elevated IOP group. NOS-1 staining is more intense in the plexiform layers. (C, D) timolol-treated group; (C) staining for NOS-1 is very weak in all the retinal layers; it is conserved in isolated amacrine cells (arrow) and in nitrergic nerve terminals of the vessel walls (white arrow); (D) no positive NOS-2 cells were detected. PRL: photoreceptor layer; ONL: outer nuclear layer; OPL: outer plexiform layer; INL: inner nuclear layer; IPL: inner plexiform layer; GCL: ganglion cell layer; NFL: nerve fibre layer. Scale bars: (A–D) 10
m.
in phosphate buffer and incubated with biotinylated anti-mouse IgG for NOS-
2 (Vector Lab Inc., Burlingame, CA, USA) and goat anti-rabbit (Dako A/S,
Denmark) for NOS-1, NOS-3 and GFAP for 1 h (dilution 1:600) and treated with the avidin–biotin peroxidase complex (Vectastain-Abc Kit, Vector Lab Inc.,
Burlingame, CA, USA) for 60 min and 3,3 -diaminobenzidine tetrahydrochloride (Sigma chemical, St. Louis, MO, USA) as the peroxidase substrate for
5 min. Finally, the sections were counterstained with hematoxylin, dehydrated, mounted with Entellan and examined with a Leitz microscope.
As a control, one section from each animal was processed with the same protocol but with the omission of the primary antibodies (NOS-1, NOS-2, NOS-3 and GFAP).
3. Results
3.1. Retina
Immunohistochemical study of the rat retina from the control group demonstrated NOS-1 positivity in the inner segments
of the photoreceptors ( Fig. 2 A, asterisk) and in numerous soma
cells in the inner nuclear layer, which may correspond to bipolar
cells and horizontal cells situated in the outermost part ( Fig. 2 A,
white arrow) and especially to amacrine cells in the innermost part (
Fig. 2 A, arrow). The immunoreactivity was weakest in the
ganglion cell layer (GCL) and in the plexiform layers. Occasionally visible in the inner plexiform layer were isolated positive
NOS-1 cells that could correspond to displaced amacrine cells
( Fig. 2 A, arrow). The retina also showed positivity for the NOS-
3 isoform in the endothelium of the capillary vessels.
The rats with chronic elevated IOP showed immunoreactivity for NOS-1 in the same places as in the control group, although the staining was more intense in the nerve fibers of the plexiform
layers, especially the inner layer ( Fig. 2 B). NOS-3 positivity in
the vascular endothelium showed no differences with respect to the controls. No positive NOS-2 cells were visible in the retina after 3 months with elevated IOP.
In the group treated with timolol, staining for NOS-1 was very weak in all the retinal layers, although it was conserved intensely and well-defined in the cytoplasm of isolated amacrine cells in
the internal part of the inner nuclear layer ( Fig. 2 C, arrow).
Intense NOS-1 positivity was also retained in the vessel walls
(
No positive NOS-2 cells were detected in the treated rats
(
Fig. 2 D) and immunoreactivity for NOS-3 was conserved in
the endothelium of the retinal vessels.
3.2. Optic nerve head
The rat ONH shows several important anatomic similarities to the human ONH. We used the regional classification reported by Morrison
[37] which distinguishes three regions in the ONH.
The neck region is located at the level of the sclera; in this region there are glial columns in linear arrays of single cells that run parallel to the nerve bundles. The transition region is an expanding zone below the neck region; glial cells have an orientation
L. Vidal et al. / Brain Research Bulletin 70 (2006) 406–413 409
Fig. 3. Immunohistochemistry for NOS-1 in the rat ONH from the control group: (A) NOS-1 positive astrocytes (arrow) and pericytes (arrowhead); (B) punctate staining for NOS-1 in the arterial walls, associated with nitrergic nerve terminals. Scale bars: 10
m.
perpendicular to the nerve bundles. Scattered patches of connective tissue are seen throughout this zone that may represent a rudimentary lamina cribrosa, which are spread over a greater relative distance than in the human ONH
rior region, the axons become myelinated and glial cells form the glial columns and the glia limitans, as in the human.
In the control group, immunostaining for NOS-1 was visible in the perinuclear cytoplasm of a few astrocyte-like cells, either isolated or in small groups, situated in the three regions of the
ONH, especially in the neck region (
showed positivity for NOS-1 in fiber-like structures arranged in a parallel fashion, which at some points showed continuity with the stained soma cells; they probably corresponded to prolon-
arrowhead). The artery walls showed a punctate-like pattern that
was suggestive of nitrergic nerve terminals ( Fig. 3 B).
In the group with chronic elevated IOP, we saw NOS-1 expression in the neck and posterior regions, whereas the tran-
sition region showed weak positivity ( Fig. 4 A). The pattern of
distribution of NOS-1 was similar to the pattern of GFAP positive cells (
Fig. 4 B) suggesting that positivity for NOS-1 was located
in astrocytes. A greater number of stained cells, especially cell processes, were visible as compared with those of the control group (
Fig. 4 C). These stained cells were situated between the
nerve fascicles, always in locations associated with glia, and they probably corresponded to reactive astrocytes. NOS-1 was also visible in the vessel walls (
Some NOS-2 positive cells, presumably astrocytes, were visible in the ONH after 3 months of chronic moderately elevated
IOP. These cells were few and isolated, mainly in the posterior
and transition zones ( Fig. 4 D, arrows). Positivity was also visi-
ble in fiber-like structures forming fascicles parallel to the nerve bundles and with a subpial location, probably corresponding to astrocyte processes and their end-feet, formers of the glia limitans separating the nervous components from the pial elements.
No NOS-2 positive cells were present in control eyes with normal IOP.
The timolol-treated animals showed a reduction in the expression of NOS-1 in all parts of the ONH, whereas positivity was seen in the nerve endings of the vessel walls (
After treatment with timolol, immunoreactivity for NOS-2 was detected in the cytoplasm of a few isolated cells in the pos-
terior and transition zones ( Fig. 4 F and G), weaker than in the
groups with untreated elevated IOP.
In the control group, the NOS-3 isoform was detected in the cytoplasm of the endothelial cells in the large arteries and veins of the ONH, and in the capillary vessels in the three areas of
the ONH ( Fig. 5 A). No positivity was seen in the remaining
structures of the vessel walls. No differences were detected in
NOS-3 expression in the ONH from rats with chronic elevated
IOP (
Fig. 5 B) or in the group treated with timolol ( Fig. 5 C) as
compared with the controls.
4. Discussion
We analyzed the expression of the NOS -1, -2 and -3 isoforms in the retina and the ONH of rats submitted to chronic elevated IOP before and after treatment with timolol, a nonselective beta-blocker and one of the most important drugs used in clinical practice to lower elevated IOP in glaucoma patients
[24,46,60,65] . For this purpose, we used an experimental model
of glaucoma, which followed the protocol of Shareef et al.
with cauterization of three episcleral veins to reduce the flow of aqueous humor from the anterior chamber and produce a constant, prolonged increase in the IOP. We have previously verified the efficacy of this model, in which the IOP remains consistently elevated by 1.25-fold in cauterized eyes for up to 3 months after the surgical procedure, as compared with a control group
The results in the retina of the control group showed immunoreactivity of the NOS-1 isoform in the inner segments of the photoreceptors, in bipolar and amacrine neurons of the inner nuclear layer and weaker staining in the ganglion cell layer and in both plexiform layers, sites that have been previously reported by others
[6,14,40,53] . In the inner segments of photorecep-
tors NOS-1 could be closely associated with the membranes of mitochondria
[14,29] . NO synthesized at this level may be
able to increase cGMP levels
[30,31] . Others have found NOS-1
mainly in amacrine cells and in displaced amacrine cells
which are thought to be the major source of NO in the mammalian retina. NO released by amacrine cells could modulate
RGC activity by activating GMP-gated cation channels
410 L. Vidal et al. / Brain Research Bulletin 70 (2006) 406–413
Fig. 4. Immunohistochemistry in the rat ONH from the elevated IOP group: (A) low-power magnification of ONH demonstrating expression of NOS-1 in the neck
(NR) and posterior (PR) regions. The transition region (TR) shows weak positivity; (B) inmunohistochemistry for GFAP. The pattern of distribution of NOS-1 is similar to the pattern of GFAP; (C) immunoreactivity for NOS-1 in reactive astrocytes in the neck region, and in the vascular wall (arrow); (D) NOS-2 positive cells
(arrows) and processes, presumably reactive astrocytes, in the transition and posterior regions of ONH, (E–G) immunohistochemistry for NOS in the rat ONH from the timolol-treated group; (E) decrease in NOS-1 expression in the neck region. Immunoreactivity is conserved in the nitrergic nerve terminals of the vessel walls
(arrow); (F) low-power magnification of ONH demonstrating a few isolated NOS-2 positive cells, presumably reactive astrocytes; (G) high-power magnification of region in the inset demonstrating NOS-2 expression in the cellular cytoplasm. Scale bars: (A, B) 50
m; (C–E, G) 10
m; (F) 20
m.
could also influence both amacrine cells and RGC, modulating the activity of GABA
A and NMDA receptors
In the ONH, we found positivity in the soma and in the prolongations of a few astrocytes. A similar distribution was reported by Shareef et al.
[53] in the rat and by Neufeld et al.
human ONH. The release of NO by these cells is likely to have a physiological function, acting as a mediator between astrocytes or between astrocytes and axons
Immunohistochemical study of the vascular structures of the
ONH showed punctiform staining in the walls of the large arteries of the anterior zone, near the vitreous body, similar to that shown by the choroid arteries, in which NO produces vasodilatation
[61] . These points could correspond to parasympathetic
nitrergic terminals, in which the NO has a vasodilator function regulating blood flow
[53] . In the capillaries of the ONH, NOS-
1 was detected in the pericytes, whereas the endothelium was positive for NOS-3. The NO produced by NOS-1 probably contributes with NOS-3 to the vasodilatation and autoregulation of the blood flow in the capillary network
In the group with elevated IOP, NOS-1 was expressed in the same sites as in the control group, although the staining was more intense in the plexiform layers of the retina. In these layers,
NO may be involved in synaptic transmission, modifying the electrical coupling in horizontal cells and decreasing dopamine release
[29] . Consequently, increased synthesis of NOS-1 may
produce changes in the synaptic activity of the retina.
We also saw increased expression of NOS-1 in the neck and posterior regions, compatible with the presence of reactive astro-
L. Vidal et al. / Brain Research Bulletin 70 (2006) 406–413
Fig. 5. Immunohistochemistry for NOS-3 in the rat ONH: (A) control group.
Immunoreactivity localized in the endothelial cells; (B) experimental group.
In large vessels near the vitreous surface the vascular endothelia are positive for NOS-3; (C) treated with timolol group. Large vessels and capillaries with endothelial cells positive for NOS-3. Scale bars: 10
m.
cytes. This finding may be because this enzyme is subject to regulation and its level of expression changes in response to different physiological and pathological stimuli
the distribution and characteristics of these cells, with hypertrophy, hyperplasia and increased expression of GFAP, have been seen in patients with primary open angle glaucoma
These patients have increased expression of NOS-1 in astrocytes, which by producing excess NO are probably responsible for the glaucomatous changes in the ONH
however, using this same experimental model of elevated IOP in rats, have failed to detect changes in the expression of NOS-1
411
[53] . We did not detect the NOS-2 isoform in any type of reti-
nal cell or in the ONH in the control animals. Although this enzyme is induced in disease states, we did not detect it in the retina after 3 months of elevated IOP, probably because the glial reaction, typical during the first 3 post-operative weeks, is not maintained at 3 months
[59] . An ultrastructural study undertaken
by us (unpublished results) also failed to show during this period either microglial cells or reactive astrocytes, which are the cells that predominantly express NOS-2
In the ONH we saw an irregular pattern of positivity for
NOS-2 in small groups of cells, which we interpreted as reactive astrocytes, and in the glia limitans, which is in agreement with the characteristic zonal involvement of the optic nerve in glaucoma. According to Shareef et al.
in the ONH 4 days after elevation of the IOP and remains for at least 3 months. Our results are similar to those seen in the
ONH of human glaucomatous eyes, which have been shown to have groups of NOS-2 positive reactive astrocytes, responsible for the production of massive amounts of NO with a powerful neurodestructive effect on neighboring cells
Our results concerning the NOS-1 and NOS-2 isoforms in the retina and in the ONH of rats submitted to prolonged periods of elevated IOP suggest that excessive levels of NO, considered neurotoxic, could be the cause of the progressive lesions in the axons of the RGC. NO generated from NOS-3, however, is protective
[25] . Low levels exert a vasodilatory function
regulating blood flow. In the retina and the ONH of both control animals and animals with elevated IOP, we saw that this enzyme was mainly located in the endothelial cells of the arteries, veins and capillaries, chiefly in the neck region of the ONH and in the choriovascular layer. These results coincide with those of Neufeld et al.
[39] in healthy persons and in glaucomatous
patients. The same author, nevertheless, found positive astrocytes in the prelaminar region and the cribrous lamina of the
ONH.
Finally, we studied the effect of timolol, a non-selective betaadrenoceptor antagonist, submitting a group of animals with elevated IOP to topical treatment with this drug for 10 weeks.
Timolol and betaxolol (selective beta1-adrenoceptor antagonist) are the most important drugs used clinically in patients with glaucoma
[24,56,65] . For 10 years clinical trials have shown that
timolol prevents progression of visual field loss, optic-disc cupping and decreased retinal thickness
IOP by reducing the production of aqueous humor
also seen this pressure-lowering effect in the experimental model of elevated IOP
Timolol has a neuroprotective action on the RGC and other neurons of the retina
[3,60] . In a previous study, we reported
a lower cell loss in the ganglion cell layer in rats submitted to topical treatment with timolol as compared with untreated animals. Timolol treatment in our study resulted in an attenuation of the detrimental effects in neurons in the GCL (17% better compared to the untreated elevated IOP group), although the mean number of neurons did not reach the same density as in normal eyes (21.74% loss compared with normal eyes)
It is unclear whether the action is direct or indirect, as a consequence of the reduction in IOP. Applied topically, timolol
412 reaches the retina-choroid at a concentration within the effective pharmacological range and it is effective against retinal neuron damage both in vitro and in vivo have been clearly shown in astrocytes expressed by M¨uller cells in culture
of calcium and sodium towards the interior of the neurons by blocking the ion channels
[3,5,19,23,34,47,60] or by modulat-
ing the intracellular concentration of calcium via the glutamate receptors
[63] . It has recently been suggested that beta-blockers
might exert their neuroprotective effect in the retina via induction of the expression of endogenous brain-derived neurotrophic factor (BDNF), a strong neuroprotector of the RGC
The rats treated with timolol showed decreased expression of NOS-1 in the retina, as compared with the other two groups, with only a few isolated amacrine cells showing positivity. The expression of this enzyme was also reduced in all areas of the
ONH and NOS-2 was only noted in the cytoplasm of a few isolated cells. These results suggest that timolol may lower the expression of these enzymes and the synthesis of NO, acting as a neuroprotector in neurons exposed to an excessive amount of extracellular NO. Whether this effect is due to direct action on beta-adrenergic receptors of the astrocytes
their ability to attenuate neuronal calcium and sodium influx by blocking the ion channels
Finally, it is important to note that the persistence of NOS-
1 staining after treatment with timolol in nerve terminals and smooth muscle cells of artery walls, together with NOS-3 staining in the vascular endothelia, indicates that the vasodilator function and regulation of blood flow exerted by NO in the
ONH could be conserved after treatment, contributing to the neuroprotective effect of timolol.
The mechanism of action of beta-blockers on the cells of the retina is not well known. Some evidence exists concerning the presence of beta-adrenergic receptors in the RGC
action seems to be related with their ability to reduce the flow
Acknowledgements
This study was supported by a grant from Plan Nacional de
Investigaci´on Cient´ıfica, Desarrollo e Innovaci´on Tecnol´ogica
(I + D + I) and Instituto de Salud Carlos III (FIS PI021295). The authors are grateful to Dr. Carmen Alba and Ms. Carmen R´ıos for their excellent technical assistance. The authors also thank
Ian Johnstone for editorial assistance.
References
L. Vidal et al. / Brain Research Bulletin 70 (2006) 406–413
[1] I. Ahmad, T. Leinders-Zufall, J.D. Koesis, G.M. Shepherd, F. Zufall, C.J.
Barnstable, Retinal ganglion cells express a cGMP-gated cation conductance activatable by nitric oxide donors, Neuron 12 (1994) 155–165.
[2] D.R. Anderson, Ultrastructure of human and monkey lamina cribrosa and optic nerve head, Arch. Ophthalmol. 82 (1969) 800–814.
[3] K. Arai, J.P.M. Wood, N.N. Osborne,

-Adrenergic receptor agonists and antagonists counteract LPS-induced neuronal death in retinal cultures by different mechanisms, Brain Res. 985 (2003) 176–186.
[4] E.W. Cheon, C.H. Park, S.S. Kang, G.J. Cho, J.M. Yoo, J.K. Song, W.S.
Choi, Nitric oxide synthase expression in the transient ischemic rat retina: neuroprotection of betaxolol, Neurosci. Lett. 330 (2002) 265–269.
[5] G. Chidlow, J. Melena, N.N. Osborne, Betaxolol, a

1 onist, reduces Na
+
-adrenoceptor antaginflux into cortical synaptosomes by direct interaction with Na
+ channels: comparison with other beta-adrenoceptor antagonists,
Br. J. Pharmacol. 130 (2000) 759–766.
[6] M.-H. Chun, S.-J. Oh, I.-B. Kim, K.-Y. Kim, Light and electron microscopical analysis of nitric oxide synthase-like immunoreactive neurons in the rat retina, Vis. Neurosci. 16 (1999) 379–389.
[7] G.M. Dawidek, M.I. Robinson, Beta adrenergic receptors in human anterior optic nerve: an autoradiographic study, Eye 7 (1993) 122–126.
[8] T.M. Dawson, D.S. Bredt, M. Fotuhi, P.M. Hwang, S.H. Snyder,
Nitric oxide synthase and neuronal NADPH diaphorase are identical in brain and peripheral tissues, Proc. Natl. Acad. Sci. U.S.A. 88 (1991)
7797–7801.
[9] V.L. Dawson, T.M. Dawson, D.A. Bartley, G.R. Uhl, S.H. Snyder, Mechanisms of nitric oxide-mediated neurotoxicity in primary brain cultures, J.
Neurosci. 13 (1993) 2651–2661.
[10] T.M. Dawson, V.L. Dawson, S.H. Snyder, Molecular mechanisms of nitric oxide actions in the brain, Ann. NY Acad. Sci. 738 (1994) 76–85.
[11] F. D´ıaz, A. Villena, M. Moreno, L. Vidal, C. Parrado, J. Garc´ıa-Campos, I.
P´erez de Vargas, Effects of a non selective

-blocker on adult rat anterograde axonal transport and retinal ganglion layer after increased intraocular pressure, Histol. Histopathol. 20 (2005) 1077–1084.
[12] E.B. Dreyer, D. Zurakowski, R.A. Schumer, S.M. Podos, S.A. Lipton, Elevated glutamate levels in the vitreous body of humans and monkeys with glaucoma, Arch. Ophthalmol. 114 (1996) 299–305.
[13] M. Eddleston, L. Mucke, Molecular profile of reactive astrocytes: implications for their role in neurologic disease, Neuroscience 54 (1993) 15–36.
[14] W.D. Eldred, T.A. Blute, Imaging of nitric oxide in the retina, Vision Res.
45 (2005) 3469–3486.
[15] W.H. Frishman, M.S. Fuksbrumer, M. Tannenbaum, Topical ophthalmic

adrenergic blockade for the treatment of glaucoma and ocular hypertension,
J. Clin. Pharmacol. 34 (1994) 795–803.
[16] E. Garcia-Valenzuela, S. Shareef, J. Walsh, S.C. Sharma, Programmed cell death of retinal ganglion cells during experimental glaucoma, Exp. Eye
Res. 61 (1995) 33–44.
[17] H. Ghazi, N.N. Osborne, Agonist-induced glycogenolysis in rabbit retinal slices and cultures, Br. J. Pharmacol. 96 (1989) 895–905.
[18] W. Goto, T. Ota, N. Morikawa, Y. Otori, H. Hara, K. Kawazu, N. Miyawaki,
Y. Tamo, Protective effect of timolol against the neuronal damage induced by glutamate and ischemia in the rat retina, Brain Res. 958 (2002)
10–19.
[19] R.L. Gross, S.H. Hensley, F. Gao, S.M. Wu, Retinal ganglion cell dysfunction induced by hypoxia and glutamate: potential neuroprotective effects of beta-blockers, Surv. Ophthalmol. 43 (Suppl. 1) (1999) S162–S170.
[20] J.S. Gwon, W.K. Ju, S.J. Park, I.B. Kim, M.Y. Lee, S.J. Oh, M.H. Chun,
The regulatory expression of neuronal nitric oxide synthase in the ischemic rat retina, Neuroreport 12 (2001) 3385–3389.
[21] S. Haverkamp, W.D. Eldred, Localization of nNOS in photoreceptor, bipolar and horizontal cells in turtle and rat retinas, Neuroreport 13 (1998)
2231–2235.
[22] M.R. Hernandez, J.D.O. Pena, The optic nerve head in glaucomatous optic neuropathy, Arch. Ophthalmol. 115 (1997) 389–395.
[23] K. Hirooka, M.E. Kelly, W.H. Baldridge, S. Barnes, Suppressive actions of betaxolol on ionic currents in retinal ganglion cells may explain its neuroprotective effects, Exp. Eye Res. 70 (2000) 611–621.
[24] P.F. Hoyng, L.M. van Beek, Pharmacological therapy for glaucoma: a review, Drugs 59 (2000) 411–434.
[25] C. Iadecola, Bright and dark sides of nitric oxide in ischemic brain injury,
Trends Neurosci. 20 (1997) 132–139.
[26] E.C. Johnson, J.C. Morrison, S. Farrell, L. Deppmeier, C.G. Moore, M.R.
McGinty, The effect of chronically elevated intraocular pressure on the rat optic nerve head extracellular matrix, Exp. Eye Res. 62 (1996) 663–674.
[27] L.A. Kerrigan, D.J. Zack, H.A. Quigley, S.D. Smith, M.E. Pease, TUNELpositive ganglion cells in human primary open-angle glaucoma, Arch.
Ophthalmol. 115 (1997) 1031–1035.
[28] I.-B. Kim, E.J. Lee, K.Y. Kim, W.-K. Ju, S.J. Oh, C.-K. Joo, M.H. Chum,
Immunocytochemical localization of nitric oxide synthase in the mammalian retina, Neurosci. Lett. 267 (1999) 193–196.
L. Vidal et al. / Brain Research Bulletin 70 (2006) 406–413
[29] I.-B. Kim, S.-J. Oh, M.-H. Chun, Neuronal nitric oxide synthase immunoreactive neurons in the mammalian retina, Microsc. Res. Tech. 50 (2000)
112–123.
[30] K.W. Koch, H.G. Lambreecht, M. Haberecht, D. Redburn, H.H. Schmidt,
Functional coupling of Ca
2+
/calmodulin-dependent nitric oxide synthase and a soluble guanylyl cyclase in vertebrate photoreceptor cells, EMBO J.
13 (1994) 3312–3320.
[31] D.E. Kurenny, L.L. Moroz, R.W. Turner, K. Sharkey, S. Barnes, Modulation of ion channels in rod photoreceptors by nitric oxide, Neuron 13 (1994)
315–324.
[32] S. Laquis, P. Chaudhary, S.C. Sharma, The patterns of retinal ganglion cell in hypertensive eyes, Brain Res. 784 (1998) 100–104.
[33] B. Liu, A.H. Neufeld, Expression of nitric oxide synthase-2 (NOS-2) in reactive astrocytes of the human glaucomatous optic nerve head, Glia 30
(2000) 178–186.
[34] J. Melena, D. Stanton, N.N. Osborne, Comparative effects of antiglaucoma drugs on voltage-dependent calcium channels, Graefes Arch. Clin. Exp.
Ophthalmol. 239 (2001) 522–530.
[35] C.G. Moore, S.T. Milne, J.C. Morrison, Noninvasive measurement of rat intraocular pressure with the Tono-Pen, Invest. Ophthalmol. Vis. Sci. 34
(1993) 363–369.
[36] J.E. Morgan, Optic nerve head structure in glaucoma: astrocytes as mediators of axonal damage, Eye 14 (2000) 437–444.
[37] J.C. Morrison, E.C. Johnson, W. Cepurna, L. Jia, Understanding mechanisms of pressure-induced optic nerve damage, Prog. Retin. Eye Res. 24
(2005) 217–240.
[38] A.H. Neufeld, M.R. Hernandez, M. Gonz´alez, Nitric oxide synthase in the human glaucomatous optic nerve head, Arch. Ophthalmol. 115 (1997)
497–503.
[39] A.H. Neufeld, A. Sawada, B. Becker, Inhibition of nitric-oxide synthase
2 by aminoguanidine provides neuroprotection of retinal ganglion cells in a rat model of chronic glaucoma, Proc. Natl. Acad. Sci. U.S.A. 96 (1999)
9944–9948.
[40] A.H. Neufeld, S. Shareef, J. Pena, Cellular localization of neuronal nitric oxide synthase (NOS-1) in the human and rat retina, J. Comp. Neurol. 416
(2000) 269–275.
[41] A.H. Neufeld, S. Das, S. Vora, E. Gachie, S. Kawai, P.T. Manning, J.R.
Connor, A prodrug of a selective inhibitor of inducible nitric oxide synthase is a neuroprotective in the rat model of glaucoma, J. Glaucoma 11 (2002)
221–225.
[42] A.H. Neufeld, Pharmacologic neuroprotection with an inhibitor of nitric oxide synthase for the treatment of glaucoma, Brain Res.Bull. 62 (2004)
455–459.
[43] C. O’Brien, Z. Butt, C. Ludlam, P. Dektova, Activation of the coagulation cascade in untreated primary open angle glaucoma, Ophthalmology 104
(1996) 725–730.
[44] H. Oku, H. Yamaguchi, T. Sugiyama, S. Kojima, M. Ota, I. Azuma,
Retinal toxicity of nitric oxide released by administration of a nitric oxide donor in the albino rabbit, Prog. Retin. Eye Res. 38 (1997) 2540–
2544.
[45] T. Okuno, H. Oku, T. Sugiyama, Y. Yang, T. Ikeda, Evidence that nitric oxide is involved in autoregulation in optic nerve head of rabbits, Invest.
Ophthalmol. Vis. Sci. 43 (2002) 784–789.
[46] N.N. Osborne, L. DeSantis, J.H. Bae, M. Ugarte, J.P. Wood, M.S. Nash, G.
Chidlow, Topically applied betaxolol attenuates NMDA-induced toxicity to ganglion cells and the effects of ischemia to the retina, Exp. Eye Res. 69
(1999) 331–342.
413
[47] N.N. Osborne, J.P.M. Wood, G. Chidlow, R. Casson, L. DeSantis, K.-G.
Schmidt, Effectiveness of levobetaxolol and timolol at blunting retinal ischemia is related to their calcium and sodium blocking activities: relevance to glaucoma, Brain Res. Bull. 62 (2004) 525–528.
[48] M.T.R. Perez, B. Larsson, P. Alm, K.-E. Andersson, B. Ehinger, Localization of neuronal nitric oxide synthase-immunoreactivity in rat and rabbit retinas, Exp Brain Res. 104 (1995) 207–217.
[49] H.A. Quigley, E.M. Addicks, Chronic experimental glaucoma in primates.
II. Effect of extended intraocular pressure on optic nerve head and axonal transport, Invest. Ophthalmol. Vis. Sci. 19 (1980) 137–152.
[50] B. Schwartz, T. Takamoto, P. Lavin, Increase of retinal vessel width in ocular hypertensives with timolol therapy, Acad. Ophthalmol. Scand. Suppl.
215 (1995) 41–53.
[51] M. Seki, T. Tanaka, H. Matsuda, T. Togano, K. Hasimoto, J. Ueda, T.
Fukuchi, H. Abe, Topically administered timolol and dorzolamide reduce intraocular pressure and protect retinal ganglion cells in a rat experimental glaucoma model, Br. J. Ophtalmol. 89 (2005) 504–507.
[52] S.R. Shareef, E. Garcia-Valenzuela, A. Salieron, J. Walsh, S.C. Sharma,
Chronic ocular hypertension following episcleral venous occlusion in rats
(letter), Exp. Eye Res. 61 (1995) 379–382.
[53] S. Shareef, A. Sawada, A.H. Neufeld, Isoforms of nitric oxide synthase in the optic nerves of rat eyes with chronic moderately elevated intraocular pressure, Invest. Ophthalmol. Vis. Sci. 40 (1999) 2884–2891.
[54] N.A. Sharif, S.X. Xu, J.Y. Crider, M. McLaughlin, T.L. Davis, Levobetaxolol (Betaxon) and other beta-adrenergic antagonists: preclinical pharmacology. IOP-lowering activity and sites of action in human eyes, J. Ocul.
Pharmacol. Ther. 17 (2001) 305–317.
[55] T. Sugiyama, H. Oku, S. Ikari, T. Ikeda, Effect of nitric oxide synthase inhibitor on optic nerve head circulation in conscious rabbits, Invest. Ophthalmol. Vis. Sci. 41 (2000) 1149–1152.
[56] M.F. Sugrue, New approaches to antiglaucoma therapy, J. Med. Chem. 40
(1997) 2793–2809.
[57] A.Y. Tan, T.L. Le Vatte, M.L. Archibald, F. Tremblay, M.E. Kelly, B.C.
Chauhan, Timolol concentrations in rat ocular tissues and plasma after topical and intraperitoneal dosing, J. Glaucoma 11 (2002) 134–142.
[58] H.J. Varela, M.R. Hernandez, Astrocyte responses in human optic nerve head with primary open-angle glaucoma, J. Glaucoma 6 (1997) 303–313.
[59] X. Wang, S.S.-W. Tay, Y.-K. Ng, An electron microscopic study of neural degeneration and glial cell reaction in the retina of glaucomatous rats,
Histol. Histopathol. 17 (2002) 1043–1052.
[60] J.P.M. Wood, K.-G. Schmidt, J. Melena, G. Chidlow, H. Allmeier, N.N.
Osborne, The

-adrenoceptor antagonists metipranolol and timolol are retinal neuroprotectans: comparison with betaxolol, Exp. Eye Res. 76 (2003)
505–516.
[61] R. Yamamoto, D.S. Bredt, S.H. Snyder, R.A. Stone, The localization of nitric oxide synthase in the rat eye and related cranial ganglia, Neuroscience
54 (1993) 189–200.
[62] H.Y. Yun, V.L. Dawson, T.M. Dawson, Neurobiology of nitric oxide, Crit.
Rev. Neurobiol. 10 (1996) 291–316.
[63] J. Zhang, S.M. Wu, R.L. Gross, Effects of

-adrenergic blockers on glutamate-induced calcium signals in adult mouse retinal ganglion cells,
Brain Res. 959 (2003) 111–119.
[64] Y. Zheng, A. Horii, P.F. Smith, C.L. Darlington, Differences in NOS protein expression and activity in the rat vestibular nucleus following unilateral laberynthectomy, Mol. Brain Res. 88 (2001) 166–170.
[65] T.J. Zimmerman, Topical ophthalmic beta-blockers: a comparative review,
J. Ocular Pharmacol. 9 (1993) 373–384.