High frequency alternating current ablation of an accessory pathway
advertisement

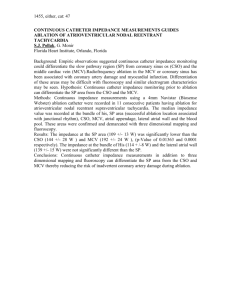
576 lACC Vol. 10. No.3 September 1987:576--82 High Frequency Alternating Current Ablation of an Accessory Pathway in Humans MARTIN BORGGREFE, MD, THOMAS BUDDE, MD, ANDREA PODCZECK, MD, GUNTER BREITHARDT, MD Dusseldorf, West Germany High frequency alternating current ablation of an accessory pathway was performed in a patient with incessant circus movement tachycardia using a right-sided, free walI accessory pathway. Antiarrhythmic drugs, antitachycardia pacing and transvenous catheter ablation using high energy direct current shocks could not control the supraventricular tachycardia. A 7F bipolar electrode catheter with an interelectrode distance of 1.2 em was positioned at the site of earliest retrograde activation during circus movement tachycardia. At this area, two alternating current high frequency impulses were delivered with an energy output of 50 W through the distal tip of the bipolar catheter, while the patient was awake. After the first shock supraventricular tachycardia ter- Catheter ablation or fulguration of structures involved in the genes is of tachycardias using high energy direct current through electrode catheters has become a therapeutic tool for selected patients. Since the initial reports of Scheinman et al. (I) and Gallagher et al . (2) , catheter ablation of the atrioventricular (AV) junction has been performed in a substanti al number of patients, resulting in good arrhythmia control in a high percentage of patient s (3). Catheter ablation of accessory pathways has also been attempted, but with less overall success (4-14). Catheter ablation of a left-sided accessory pathway by shocks delivered within the coronary sinus has resulted in perforation of the coronary sinus (5). Few attempts of ablation of a right free wall accessory pathwa y have been reported. However, the overall success From the Hospital of the University of DUsseldorf. Department of Ca rdiology. Pneumology and Angiology. DUsseldorf. West German y. Thi s study was supported by a grant fro m the Sonderforschun gsberei ch SFB 242 (Koronare Herzkrankhe it-Therapie und Proph ylaxe akuter Kompli kationen ) o f the Deutsche Forschun gsgemeinschaft. Bonn-Bad God esberg , West Germany. Addre ss for reprints: Martin Borggrefe , MD . Medi zinische Klinik und Poliklinik , Abte ilung fur Kardi ologie , Pneurnologie und Angiologie, Universitat DUsseldorf, Moorenstrasse 5 . D-4000 DUsseldorf. West German y. Manuscript received September 15. 1986; revised manuscript received Feb ruary 18 .1987. accepted March 12. 1987 . © 1987 by the American College of Cardiology Downloaded From: http://content.onlinejacc.org/ on 10/01/2016 minated and accessory pathway conduction was absent without altering anterograde conduction in the normal atrioventricular (AV) conduction system. No reports of pain or other complications were noted. In short-term folIow-up of 5 months, the patient had been free of arrhythmias without antiarrhythmic medication. Thus, high frequency alternating current ablation was performed for the first time in the treatment of an arrhythmia incorporating an accessory pathway in a human. This technique may be an attractive alternative to the available transcatheter ablation techniques and to antitachycardia surgery. o Am Call Cardiol 1987;10:576-82) rate seems to be low . In contrast to free wall accessory pathways, posteroseptal pathways may be eligible for this technique with a success rate of about 75 to 80% (II). One of the major problems of high energy direct current ablation techniques has been the transient nature of the antiarrhythmic effect due to recov ery of the arrhythmogenic tissue (3,5,11,14). Therefore, there is a need for ablation techniques that produce more persi stent tissue damage . In a recent experimental study (15 ), we evaluated the usefulness of alternating high frequen cy current ablation techniques; the results indicated that there was an energydose-related tissue response resulting in well delineated necrosis. The purpose of the present study is to present the first clinical application of high frequenc y alternating current for ablation of a right-sided acce ssory pathway in human s after previou sly unsucce ssful high energy direct current ablation . Case Report Previous history. A 40 year old man with Wolff-Parkinson- White syndrome presented with a history of incessant supraventricular tachycardia incorporating a right-sided accessory pathway. The arrhythmia had been present for 14 0735·I097/X7/$3 .50 JACC Vol. 10, No.3 September 1987:576-82 II III -rJ\,-- --v..rv- BORGGREFE ET AL. HIGH FREQUENCY ALTERNATING CURRENT ABLATION I? V3 r> ~ \1 aVR--....r- ~~ /' aVL ...flI.....r- I -----"- VI II --"-Jo.,r----- III --------v--- 577 --------r- V2 ~ 1 V3 ------ .( - ---y-- aVR~ ~ aVL - - . - - / ' - Vs --..IV-- Figure 1. Left panel, 12 lead electrocardiogram (ECG) before ablation showing sinus rhythm with pre-excitation; delta waves are positive in leads I, II, aVL and V2 to V6 and negative in lead III, suggesting a right-sided accessory pathway. Right panel, ECG showing permanent normalization of the QRS complex after high frequency ablation. aVF ~v--- after ablation V6 --J '"--' before ablation days. The diagnosis of Wolff-Parkinson-White syndrome had been made 4 months before referral to our hospital when the patient reported short episodes of palpitation. At that time, the 12 lead electrocardiogram (ECG) revealed normal sinus rhythm with pre-excitation. Delta wave polarity suggested the presence of a right-sided accessory pathway (Fig. I). On admission to our hospital, the patient presented with supraventricular reentrant tachycardia with a cycle length of 445 ms and narrow QRS complexes (Fig. 2). A retrograde P wave was visible. Administration of verapamil, ajmaline, sotalol, propafenone, f1ecainide and digitalis proved ineffective in permanently terminating the tachycardia. A drug trial using amiodarone was refused by the patient because of possible side effects. Physical examination and echocardiographic evaluation revealed no cardiovascular abnormality. The supraventricular tachycardia was hemodynamically well tolerated when the patient was supine. Electrophysiologic study. The study was performed 16 hours after the last dose of propafenone. A 6F quadripolar catheter (USCI) was advanced to the coronary sinus using the left cephalic vein. Three additional catheters were inserted through the right femoral vein: a 6F quadripolar catheter (USCI) to the high right atrium, one bipolar catheter to the His bundle area and another bipolar catheter to the right ventricular apex. Additionally, a 6F quadripolar mapping catheter (Josephson catheter, USC)) was inserted by way of the left femoral vein for atrial mapping. The study confirmed the diagnosis of a circus movement tachycardia Downloaded From: http://content.onlinejacc.org/ on 10/01/2016 using a right free wall accessory pathway. Atrial or ventricular pacing resulted in only transient termination of the supraventricular tachycardia; after a single sinus beat, the tachycardia immediately resumed. At the time of electrophysiologic study, no anterograde conduction through the Figure 2. Electrocardiogram during supraventricular tachycardia with narrow QRS complexes with a cycle length of 455 ms and visible retrograde P waves. TOOO I~ V3 -4, r r V / J ' ~ ~VV\ r aVL ~ 578 BORGGREFE ET AL. HIGH FREQUENCY ALTERNATING CURRENTABLATION accessory pathway could be demonstrated. The anterograde effective refractory period of the AV node during incremental atrial pacing was 400 ms. The effective refractory period of the accessory pathway in retrograde direction was 215 ms. Detailed right atrial mapping was performed during circus movement tachycardia and during pacing from the right ventricular apex. The earliest retrograde activation occurred at the right atrial free wall. At this site, AV bypass tract deflections were recorded. Because the supraventricular tachycardia persisted despite antiarrhythmic treatment and antitachycardia pacing, the patient was offered the option of either surgical or catheter ablation of the accessory pathway. He chose the latter and gave his informed consent. High energy direct current ablation procedure. The ablation procedure was performed the next day. Surgical standby was available. A quadripolar 6F catheter was inserted through the left femoral vein for stimulation of the right ventricular apex as well as for recording ventricular activity. Additionally, one quadripolar catheter (USC}, Josephson) was inserted and atrial mapping was repeated. After endotrachial intubation and anesthesia, an initial 100 J discharge was delivered through the tip electrode (the anode) directed to a back paddle (the cathode) using a standard defibrillator (Hellige) at the site of earliest retrograde atrial activation at the right atrial free wall. At this site, bypass tract deflections were also recorded. This first shock resulted in only transient termination of the supraventricular tachycardia. Four additional shocks were also ineffective. However. after the sixth shock, permanent termination of the supraventricular tachycardia was observed. Thereafter, two additional shocks (100 J each) were delivered to the same location. Complete retrograde block was noted but anterograde conduction over the AV node remained intact. An angiogram of the right coronary artery revealed no structural abnormality before and after application of the shocks to the right-sided AV groove. However, after 8 hours supraventricular tachycardia with a cycle length of 440 ms resumed. Under the assumption that catheter ablation may have altered the properties of the accessory pathway, antiarrhythmic treatment with propafenone was started again and proved ineffective. Therefore, the patient was offered two alternatives: I) the possibility of high frequency alternating current ablation of the accessory pathway as a new approach or 2) a surgical procedure. High frequency catheter ablation. High frequency catheter ablation was performed 3 days later without the use of anesthesia. Because trans venous catheter ablation technique using high energy direct current had been unsuccessful, this experimental mode of treatment was chosen. Surgical standby was available. Blood pressure was monitored with a 6F pigtail catheter inserted into the right femoral artery. A 6F quadripolar catheter was inserted through the left femoral vein for stimulation of and recording from the right ventricular apex. A 7F bipolar catheter (Lumelec, CorDownloaded From: http://content.onlinejacc.org/ on 10/01/2016 lACC Vol. 10. No.3 September 1987:576-82 dis) with an interelectrode distance of 1.2 cm was inserted into the right femoral vein and used for right atrial mapping and ablation. This catheter possesses a central lumen with a diameter of I mrrr', which allows for continuous rinse with saline solution during the ablation procedure to prevent both blood coagulation and overheating at the catheter tip. Continuous rinsing of the catheter lumen was performed during application of high frequency current using a O. 19% saline solution at 50 mllmin. High frequency alternating current was administered through the distal electrode using a back paddle as neutral electrode. A specially designed energy source for high frequency coagulation (HAT 100; Dr. Osypka GmbH, Grenzach-Wyhlen, West Germany) was used. With this unit, energy can be varied in 10 steps from 2.5 W (step I) up to 50 W (step 10). Alternating current frequency varies between 500 and 1,000 kHz. The unit was designed to switch off automatically as soon as the impedance of the tissue increases during the coagulation procedure. During the ablation procedure, the earliest site of retrograde atrial activation during circus movement tachycardia was found at the identical site as during the first ablation procedure. Again, electrograms with three distinct deflections were recorded (Fig. 3). The first broad electrogram is probably due to local ventricular activation (V), the second deflection most likely represents accessory pathway depolarization (K) and the third deflection represents atrial activity (A). The following points are suggested to support the idea that the deflections named K may represent electrical activity from the accessory pathway: I) These three simultaneous deflections were only recorded at the earliest site of retrograde activation during reciprocating tachycardia, indicating a close proximity to the accessory pathway; 2) all recordings were made at low gain; 3) during ventricular pacing with varying cycle lengths the VK and KA intervals were nearly identical, thus excluding that K represents far field ventricular activity (if K was far field ventricular activity, the K deflections should have become more fragmented and delayed with shorter cycle lengths and closer premature ventricuiar stimuli); 4) after successful ablation of the accessory pathway the deflection K could no longer be recorded during sinus rhythm or ventricular pacing, even when pacing at the same cycle length as before ablation the catheter remained at the same recording site; and 5) during incremental atrial pacing only A and V electrograms were recorded as the impulse traveled only through the normal AV node conduction system. In contrast tothefirst electrophysiologic study, the effective refractory period of the accessory pathway in retrograde direction had increased from 215 to 370 ms as a result of the previous transcatheter ablation. During incremental ventricular pacing, block between the accessory pathway potential and the atrium was observed (Fig. 4). Although the exact site of retrograde block cannot be determined, this finding supports the con- BORGGREFE ET AL. HIGH FREQUENCY ALTERNATING CURRENT ABLATION lACC Vol. 10, No.3 September 1987:576-82 579 500 --------"--...._------------------[ [[ --.. . . . -.- - - - - - - - - - ..... ....- - - - - - - - - - ...... ' --"" -"\ '--- V RA - _. c-: ~' ----- 1\• , (unipolar) . --J 460 RVA - _~ - - ..-.0-_-,\ I K A ~~-- V _ K A /'. ~---...._.I\./'·...,.:\A..- r...- .-'..- - -- -- Figure 3. Recording during incessant supraventricular tachycardia. From top to bottom, electrocardiographic leads I, II and VI , and intracardiac leads from the right ventricular apex (RVA) and right atrial (RA) free wall. At the site of earliest right atrial retrograde activation, simultaneous recordings of ventricular (V), accessory pathway (K)and atrial (A)activity were obtained during circus movement tachycardia with a cycle length of 460 ms. cept that the distal junction of the accessory pathway may be the most vulnerable to block. At this site. high frequency alternating current ablation was performed. An energy of 50 W was applied for 10 seconds during circus movement tachycardia (Fig. 5). After 10 seconds, the device automatically switched off because "-- - -- - , ·· ../ .. _. ' '- 'vv"'-"" - ' of increasing tissue impedance due to the coagulation process. During the application of high frequency current, the patient was awake and did not report any pain. Tachycardia terminated at the time when the device automatically switched off. The PR interval during sinus rhythm was 230 ms without evidence of pre-excitation (Fig. I) . Five minutes after ablation, ventricular stimulation revealed complete retrograde block. Despite this apparent success, a second high frequency alternating impulse was applied using the same energy at the identical site. This time the device switched off automatically after 15 seconds. At the immediate electrophysiologic control study. the anterograde effective refractory period of the AV node was 1000 \ - - - - _\...._----------'------[ 370 [[ -- '--\,--~.~ ~V\.rr--'r'~ ---..........,~ RA (bipolar) Downloaded From: http://content.onlinejacc.org/ on 10/01/2016 ~ Figure 4. Recordings during incremental right ventricular pacing at a cycle length of 370 rns, which produced 2:I retrograde block in the accessory pathway . After the first stimulated beat, activity from the accessory pathway (K)andthe atrium (A)were recorded, whereas afterthesecond stimulated beat, block occurs between the Kent potential and the atrial signal . RA = right atrium. 580 lACC Vol. 10, No.3 September 1987:576-82 BORGGREFE ET AL. HIGH FREQUENCY ALTERNATING CURRENT ABLATION TOOO \ I 1 - \ . , . - '''''''''-- ' L 460 Jstart -<v----- v-''j' - HF ablation - 10 seconds Figure S. Recordings of leads I, II and VI during the high frequency ablation procedure. During incessant supraventricular reentrant tachycardia (SVT) with a cycle length of 460 ms high frequency (HF) alternating current ablation was started (arrow). After 10seconds,the deviceautomatically switched off and normal sinus rhythm (NSR) with a cycle length of 850 ms resumed. See text for further explanations. incessanf SVT \ \ I efc stop HF ablation 1 , NSR 390 ms as determined during incremental atrial pacing. There was no evidence of pre-excitation. Ventricular pacing revealed complete retrograde block. Coronary angiography of the right coronary artery was performed before and after high frequency ablation, without evidence of any deleterious side effect. The patient was effectively heparinized and monitored for 6 days without any evidence of pre-excitation or any reappearing arrhythmias. A lung perfusion scan performed 24 hours after the ablation procedure was normal. Serial echocardiographic evaluation revealed no intracardiac thrombus formation. The maximal serum creatine kinase level was 60 Uzliter, and the creatine kinase, MB fraction levels were also normal. A control electrophysiologic study carried out 10 days after the ablation procedure revealed absence of accessory pathway conduction. The refractory period of the AV node during incremental atrial pacing was 460 ms. During a treadmill exercise test, the patient was exercised up to 150 W without evidence of arrhythmias or pre-excitation. During a follow-up period of 5 months, during which time the patient has taken no cardioactive medication, his clinical course has been uneventful without arrhythmias or any ECG evidence of pre-excitation. Discussion Previous experience with catheter ablation techniques in the WoltT·Parkinson-White syndrome. After the initial reports by Morady and Scheinman (4) and Gallagher et al. (2), several groups (5-14) have reported that transvenous Downloaded From: http://content.onlinejacc.org/ on 10/01/2016 catheter ablation of accessory pathway can be used in selected patients with refractory arrhythmias. However, the number of patients studied so far is small and the success rate is difficult to determine. Fisher et al. (5) were the first to attempt catheter ablation of left free wall accessory pathways through the coronary sinus. However, this approach seldom resulted in permanent interruption of accessory pathway conduction. Ward and Camm (9) studied three such patients, only two of whom were free of pre-excitation during follow-up. Morady et al. (12) studied eight patients with a posteroseptal pathway, in whom trans venous high energy direct current catheter ablation was performed, with an overall success rate of 75%. Similar results have been reported by Kunze and Kuck (7). Thus, transvenous catheter ablation for accessory pathways may be effective in some patients; however, the overall success rate seems to be only about 60 to 80%. Reasons for failures are difficult to interpret. One possible explanation may be problems in correctly identifying the site of the accessory pathway. Furthermore, the local injury produced by high energy transvenous catheter shocks may be insufficient to produce block. Therefore, the new technique applied in the present case may be a promising alternative. Catheter electroshocks may result in thermal electrocoagulation of tissue, concussive shock waves or membrane damage due to the intense electric field. The histologic changes produced by the shocks are lesions I to 2 em in diameter (16,17). However, these injuries may be only transient in nature because of a recovery process of the tissue possibly due to local recovery from edema or to only minor histologic JACC Vol. 10. No.3 September 1987:57&-82 lesions. Because of these limitations of catheter ablation techniques, there is a need for alternative techniques to produce delineated and more controlled focal tissue necrosis. High frequency ablation. Recently, high frequency alternating current coagulation has been introduced as an alternative to conventional ablation techniques in the experimental animal (15,18,19). Previous extensive animal experiments in our laboratory (15) demonstrated that high frequency catheter ablation may be a promising technique for ablation of myocardial structures resulting in local necrosis. Our results as well as those of previous studies (18) showed a relation between applied energy and tissue response. Coagulation zones or tissue necrosis could be induced in a size-correlated relation to the applied energy. Furthermore, deleterious effects of thermal injury induced by ablation procedures such as thrombus formation at the tip of the electrode catheter may be prevented by continuously rinsing the catheter at the tip using a specialelectrode catheter (Lumelec , Cordis). The energy source used (HAT 100, Dr. Osypka GmbH, Grenzach-Wyhlen) is designed to automatically terminate the energy delivery as soon as the impedance of the ablated tissue increases. In our patient, a right-sided free wall accessory pathway could be ablated by the delivery of transvenous high energy alternating current impulses. The procedure was effective and safe and the patient did not require general anesthesia. High energy direct current shock had been ineffective in this patient; however, it might already have damaged the accessory pathway before the attempt at high frequency alternating current ablation . This new catheterablation technique, performed in a human for the first time, appears to be an attractive alternative to conventional ablation procedures. High frequency ablation techniques obviate the need for general anesthesia and may be associated with less expense, less discomfort and a shorter convalescence period than are associated with high energy transvenous ablation techniques. Role of intracardiac electrocatheter recordings of an atrioventricular bypass tract. Since the initial reports (20,21) on intracardiac electrocatheter recordings of accessory pathways, several studies (22,23) have demonstrated that potentials originating from accessory bypass tracts may be recorded using electrode catheters in humans. Although many methodologic problems exist to validate the accessory pathwayelectrogram, recording of the signal may be helpful in defining the site of application of transvenous catheter shocks. In our present case the ablation procedure was also guided by endocardial recordings of the accessory pathway. Interestingly, during ventricular pacing retrograde blockoccurred at the accessory pathway-atrial junction, suggesting that the proximal junction of the pathway is the most vulnerableto block. Application of transvenous alternating current shock to this site resulted in a permanent abolition of Downloaded From: http://content.onlinejacc.org/ on 10/01/2016 BORGGREFE ET AL. HIGH FREQUENCY ALTERNATING CURRENT ABLATION 581 accessory pathway conduction. This finding in our patient is consistent with the concept of "impedance mismatch," elegantly demonstrated in a series of experiments carried out by de la Fuente et al. (24). Clinical implications. Our results suggest that high frequency catheter ablation of an accessory pathway may be an alternative to "conventional" catheter ablation procedures and to surgical intervention; however, further studies are needed to ascertain the efficacy and safety of this procedure. Whether other myocardial structures such as ventricular myocardium in patients suffering from ventricular tachycardia or a left-sided accessory pathway are also suitable for this technique has to be further demonstrated. References I. Scheinman MM. Morady F, Hess OS. Gonzales R. Catheter-induced ablation of the atrioventricular junction to control refractory supraventricular arrhythmias . JAMA 1982;248:851-5 . 2. Gallagher JJ. Svenson RH. Kasell J. et al. Catheter technique for closed-chest ablation of the atrioventricular conduction system. A therapeutic alternative for the treatment of refractory supraventricular tachycardia . N Engl J Med 1982;306: 194-200. 3. Scheinman MM. Evans-Bell T. and the Executive Committee of the Percutaneous Cardiac Mappingand Ablation Registry. Catheter ablation of the atrioventricular junction: a reportof the percutaneous mapping and ablation registry . Circulation 1984;70:1024-9. 4. Morady F. Scheinman MM. Transvenous catheter ablation of a posteroseptal accessory pathway in a patient with the Wolff-ParkinsonWhite syndrome. N Engl J Med 1984;310:705-7. 5. Fisher 10. Brodman R. Kim SG, et al. Attempted nonsurgical electrical ablation of accessory pathways via the coronary sinus in the Wolff-Parkinson-White syndrome. J AmColICardiol 1984;4:684-94 . 6. Jackman WM, Friday KJ, Scherlag BJ. Direct endocardial recording from an accessory atrioventricular pathway: localization of the site of block, effectof antiarrhythmic drugs, and attemptof nonsurgical ablation. Circulation 1983;68:906-16. 7. Kunze KP. Kuck K-H. Transvenous ablation of accessory pathways in patients with incessant atrioventricular tachycardia (abstr). Circulation 1984;70 (suppl II): 11-412. 8. Nathan AW. Davies OW. Creamer JE. Butrons GS. Camm AJ. Successful catheter ablationof abnormal atrioventricular pathwaysin man (abstr). Circulation 1984;70 (supplll): 11-99. 9. Ward DE, Camm AJ. Treatment of tachycardias associated with the Wolff-Parkinson-White syndrome by transvenous electrical ablation of accessory pathways . Br Heart J 1985;53:64-8. 10. BardyGH, PooleJF, ColtortiF, et al. Catheterablationof a concealed accessory pathway. Am J Cardiol 1984;54:1316-68. II. Weber H. Schmitz L. Catheter technique for closed chest ablation of an accessory pathway. N Engl J Med 1983;308:653. 12. Morady F. Scheinman MM, Winston SA. et al. Efficacy and safety of transcatheter ablation of posteroseptal accessory pathways. Circulation 1985;72:170-7. 13. Critelli G, GallagherJ1. Monda V. Coltroni F, ScherilloM, Rossi L. Anatomic and electrophysiologic substrate of the permanent form of junctional reciprocating tachycardia. J Am Coli CardioI1984;4:60I-IO. 14. Borggrcfe M, Breithardt G. Ectopic atrial tachycardia after transvenous catheterablationof a posteroseptal accessory pathway. J Am Coli Cardiol 1986;8:441-5. IS. BuddeTh, JacobB, Langwasser J, Borggrefe M, Frenzel H, Breithardt 582 BORGGREFE ET AL. HIGH FREQUENCY ALTERNATING CURRENT ABLATION JACC Vol. 10, No.3 September 1987:576-82 G. Hochfrequenz-Katheterablation: eine Methode zur Erzeugung dosisabhangiger Koagulationszonen. Z Kardiol 1987;76:204-210. catheter electrode of accessory pathway depolarization. J Am Coli Cardiol 1983;I:468-70. 16. Lerman BB, Weiss JL, Bulkley BH, Becker LC, Weisfeld MC. Myocardial injury and induction of arrhythmias by direct shock delivered via endocardial catheter in dogs. Circulation 1984;69:1006-12. 21. Jackman W, Beck B, Aliot E, Friday K, Lazzara R. Basis for concealed accessory AV pathways (abstr). Circulation 1984;70 (supplll): 11-1348. 17. Winston SA, Morady F, Davis JC, DiCarlo LA, Wexman MD, Scheinman MM. Catheter ablation of ventricular tachycardia abstr. Circulation 1984;70 (supplll):11-412. 22. Winters SL, Gomes A. Intracardiac electrode catheter recordings of atrioventricular bypass tracts in Wolff-Parkinson-White syndrome: techniques, electrophysiologic characteristics and demonstration of concealed and decremental propagation. J Am Coli Cardiol 1986;7: 1392-403. 18. Huang SK, Jordan N. Graham A, et al. Closed-chest catheter desiccation of atrioventricular junction using radiofrequency energy-a new method of catheter ablation (abstr). Circulation 1985;72 (suppl III): 1II-389. 19. Hoyt RH, Huang SK, Jordan N, Marcus F. Factors influencing transcatheter radiofrequency ablation of the myocardium (abstr). Circulation 1985;72 (suppl III): III-473. 20. Prystowsky EM, Brown KF, Zipes DP. Intracardiac recording by Downloaded From: http://content.onlinejacc.org/ on 10/01/2016 23. O'Callaghan WG, Colavita PG, Kay N, Ellenbogen KA, Gilbert MR, German LD. Characterization of retrograde conduction by direct endocardial recording from an accessory atrioventricular pathway. J Am Coli Cardiol 1986;7:167-71. 24. de la Fuente D, Sasyniuk D, Moe GK. Conduction through a narrow isthmus in isolated canine atrial tissue. Circulation 1971;44:803-9.