OnabotulinumtoxinA 100 U Significantly Improves All Idiopathic

E U R O P E A N U R O L O G Y 6 4 ( 2 0 1 3 ) 2 4 9 – 2 5 6 a v a i l a b l e a t w w w . s c i e n c e d i r e c t . c o m j o u r n a l h o m e p a g e : w w w . e u r o p e a n u r o l o g y . c o m
Platinum Priority – Incontinence
Editorial by Stephan Madersbacher on pp. 257–259 of this issue
OnabotulinumtoxinA 100 U Significantly Improves All Idiopathic
Overactive Bladder Symptoms and Quality of Life in Patients with
Overactive Bladder and Urinary Incontinence: A Randomised,
Double-Blind, Placebo-Controlled Trial
Christopher Chapple
Piotr Radziszewski
, Karl-Dietrich Sievert
, Christopher Nardo
Cornelia Haag-Molkenteller
, Scott MacDiarmid
, Catherine Thompson
, Vik Khullar
,
, Jihao Zhou
,
a
Royal Hallamshire Hospital, Sheffield, UK; b
University of Tuebingen, Tuebingen, Germany; c
Alliance Urology Specialists, Greensboro, NC, USA; d
Imperial
College, London, UK; e
Department of Urology, Medical University of Warsaw, Warsaw, Poland; f
Allergan, Inc., Irvine, CA, USA; g
Allergan Ltd., Marlow, UK
Article info
Article history:
Accepted April 1, 2013
Published online ahead of print on April 10, 2013
Keywords:
Botulinum toxin
OnabotulinumtoxinA
Overactive bladder
Urinary incontinence
Abstract
Background: Overactive bladder (OAB) syndrome with urinary incontinence (UI) is prevalent in the population and impairs health-related quality of life (HRQOL).
Objective: To assess the impact on efficacy, safety, and HRQOL of onabotulinumtoxinA
(BOTOX
1
, Allergan, Inc.) treatment in patients with OAB with UI.
Design, setting, and participants: This pivotal, multicentre, double-blind, randomised, placebocontrolled, phase 3 study enrolled patients with idiopathic OAB with 3 urgency UI episodes over 3 d and 8 micturitions per day who were inadequately managed by anticholinergics.
Intervention: OnabotulinumtoxinA at a 100 U dose ( n = 277) or placebo ( n = 271), administered as 20 intradetrusor injections of 0.5 ml.
Outcome measurements and statistical analysis: Co–primary end points were change from baseline in the number of UI episodes per day and proportion of patients reporting positive treatment response on the treatment benefit scale (TBS) at week 12. Additional end points included other OAB symptoms (episodes of urinary urgency incontinence, micturition, urgency, and nocturia) and HRQOL (Incontinence Quality of Life [I-QOL], King’s Health Questionnaire
[KHQ]). Safety assessments included adverse events (AEs), postvoid residual (PVR) urine volume, and initiation of clean intermittent catheterisation (CIC).
Results and limitations: OnabotulinumtoxinA significantly decreased UI episodes per day at week 12 ( 2.95 for onabotulinumtoxinA versus 1.03 for placebo; p < 0.001). Reductions from baseline in all other OAB symptoms were also significantly greater following onabotulinumtoxinA compared with placebo ( p 0.01). Patients perceived a significant improvement in their condition, as measured by patients with a positive treatment response on the TBS
(62.8% for onabotulinumtoxinA versus 26.8% for placebo; p < 0.001). Clinically meaningful improvements from baseline in all I-QOL and KHQ multi-item domains ( p < 0.001 versus placebo) indicated positive impact on HRQOL. AEs were mainly localised to the urinary tract.
Mean PVR was higher in the onabotulinumtoxinA group (46.9 ml versus 10.1 ml at week 2; p < 0.001); 6.9% of onabotulinumtoxinA patients versus 0.7% of placebo patients initiated CIC.
Conclusions: OnabotulinumtoxinA 100 U was well tolerated and demonstrated significant and clinically relevant improvements in all OAB symptoms, patient-reported benefit, and
HRQOL in patients inadequately managed by anticholinergics.
Trial registration: ClinicalTrials.gov: NCT00910520.
# 2013 European Association of Urology. Published by Elsevier B.V. All rights reserved.
* Corresponding author. Royal Hallamshire Hospital, Room H26, H-Floor, Glossop Road, Sheffield,
GB-S10 2JF, UK. Tel. +44 0 114 271 3048; Fax: +44 0 114 279 7841.
E-mail address: c.r.chapple@shef.ac.uk
(C. Chapple).
0302-2838/$ – see back matter # 2013 European Association of Urology. Published by Elsevier B.V. All rights reserved.
http://dx.doi.org/10.1016/j.eururo.2013.04.001
250 E U R O P E A N U R O L O G Y 6 4 ( 2 0 1 3 ) 2 4 9 – 2 5 6
1.
Introduction
Overactive bladder syndrome (OAB) is defined as urinary urgency, with or without urgency urinary incontinence
(UUI), and is usually accompanied by urinary frequency and nocturia
[1,2] . The prevalence of OAB is approximately
12–19% in both men and women
nence (UI) affects approximately one-third of patients with
OAB
and is inevitably associated with substantial negative effects on patients’ health-related quality of life
(HRQOL)
[4,7–9] . Patients with OAB report among the
lowest health utility scores compared to those with other chronic diseases such as asthma, cancer, diabetes, heart disease, and migraine headaches
. Consequently, this results in decreased work productivity, social embarrassment, and avoidance and limiting behaviours in OAB patients with UI
Oral anticholinergics are the mainstay of first-line pharmacologic treatment of OAB
; however, many patients discontinue their use due to inadequate efficacy and/or intolerable side effects
[15,16] . Options for patients
who fail anticholinergics may include sacral or tibial nerve neuromodulation or more invasive surgery such as a clam cystoplasty, but onabotulinumtoxinA treatment may be an alternate treatment option. A phase 2, placebo-controlled, dose-ranging study demonstrated that onabotulinumtoxinA significantly improved UUI episodes
parameters
in patients with UI and
OAB. This study demonstrated that the optimal benefit–risk profile was achieved with a dose of 100 U, so this dose was further evaluated in this study and a corresponding co-pivotal
[20] , phase 3, randomised, double-blind, place-
bo-controlled study of patients with OAB and UI who were inadequately managed by prior anticholinergic therapy.
2.
Patients and methods
2.1.
Study participants
This large, phase 3, international, pivotal, randomised, double-blind, placebo-controlled study was conducted from October 2009 to August
2011 in Europe and the United States. Eligible patients had idiopathic
OAB with UI and experienced 3 UUI episodes in a 3-d bladder diary, an average of 8 micturitions per day, and a postvoid residual (PVR) urine volume 100 ml. Patients had been inadequately managed by anticholinergic therapy (insufficient efficacy or intolerable side effects), and their use was not permitted throughout the study. Patients had to be willing to initiate clean intermittent catheterisation (CIC) posttreatment, if necessary. Exclusion criteria included previous botulinum toxin treatment for any urologic condition; symptoms of OAB for any known neurologic reason; a predominance of stress incontinence; and any pelvic or urologic abnormalities, bladder surgery, or disease that may affect bladder function.
2.2.
Study design
This study was conducted in compliance with Good Clinical
Practice guidelines. Patients were randomised 1 to 1 to placebo or onabotulinumtoxinA 100 U (BOTOX 1 , Allergan, Inc.), which was administered via cystoscopy as 20 intradetrusor injections of 0.5 ml, evenly spaced but avoiding the trigone. Units of biologic activity of onabotulinumtoxinA cannot be compared to or converted into units of any other botulinum toxin product, and onabotulinumtoxinA is not interchangeable with other botulinum toxin preparations. Randomisation was stratified within centre and by the number of UUI episodes during the 3-d screening period ( 9 or > 9 episodes). Treatment was blinded by use of a numbering system and preparation of study medication by an independent person. Patients could receive instillation of local anaesthesia to the bladder and/or sedation during treatment administration. Patients participated in the study for 24 wk and could have a retreatment with onabotulinumtoxinA 100 U from 12 wk onwards for both dose groups if requested by the patients and if they had 2 UI episodes as recorded in a 3-d diary.
2.3.
Efficacy and safety evaluations
The co–primary efficacy end points were change from baseline in the number of UI episodes and the proportion of patients with a positive treatment response on the treatment benefit scale (TBS) at wk 12. For the
TBS, patients rated their condition as greatly improved, improved, not changed, or worsened (with greatly improved or improved considered a positive treatment response)
[21] . A 3-d paper bladder diary was used to
assess OAB symptoms, and HRQOL was assessed using the Incontinence
Quality of Life (I-QOL) instrument
and the King’s Health
Questionnaire (KHQ)
[23] . The I-QOL is scored as three domain scores
(Avoidance and Limiting Behaviour, Psychosocial Impact, and Social
Embarrassment) and a total summary score, with higher scores indicating better HRQOL
. The KHQ consists of seven multi-item domains (Role Limitations, Social Limitations, Physical Limitations,
Personal Relationships, Emotions, Sleep/Energy, and Severity/Coping
Measures) and two single-item domains (General Health Perception and
Incontinence Impact); lower scores reflect better HRQOL
.
Safety measurements included adverse events (AEs) and PVR urine.
The study protocol specified that CIC was to be initiated if the PVR was
200 and < 350 ml if there were associated symptoms that were deemed to require CIC, or if PVR was 350 ml, regardless of symptoms. Urinary retention was defined as a PVR 200 ml that required CIC, and urinary tract infection (UTI) was defined as both a positive urine culture
(bacteriuria count of > 10
5 colony forming units/ml) and leukocyturia
( > 5 per high power field).
2.4.
Statistical analyses
The intention-to-treat (ITT) population (all randomised patients regardless of receipt of treatment) was used for efficacy analyses, and the safety population (all patients who received treatment, analysed by actual treatment received) was used for safety analyses. Planned enrolment was 534 patients, including a 15% attrition rate. The study design provided 82% power to detect a between-group difference in change from baseline of 2.3 UI episodes per day, assuming a common standard deviation of 8.5 episodes, and 99% power to detect a betweengroup difference of 22% for TBS. OnabotulinumtoxinA and placebo treatment groups were compared for each posttreatment visit using analysis of covariance (ANCOVA) for change from baseline in UI episodes, with treatment as a factor and number of UI episodes at baseline and site as covariates. The Cochran-Mantel-Haenszel test was used to compare the proportion of TBS responders at wk 12 between the treatment groups, with baseline UUI ( 9 versus > 9 in the 3-d bladder diary) as a stratification factor. Missing values were imputed by last observation carried forward for the co–primary end points. Other OAB symptoms,
I-QOL, and KHQ were analysed using an ANCOVA model similar to that for the UI episodes.
Placebo-controlled comparisons focused on the first 12 wk, as thereafter, patients could be eligible to receive retreatment with onabotulinumtoxinA 100 U.
E U R O P E A N U R O L O G Y 6 4 ( 2 0 1 3 ) 2 4 9 – 2 5 6
Randomised n
= 548
32 Discontinued n
3 Adverse events
= 271
0 Lack of efficacy
7 Lost to follow-up
15 Personal reasons
5 Protocol violation
2 Other
Placebo OnabotulinumtoxinA 100 U n
= 277
27 Discontinued
6 Adverse events
1 Lack of efficacy
6 Lost to follow-up
10 Personal reasons
3 Protocol violation
1 Other
Completed Treatment Cycle 1 n
= 239
Completed Treatment Cycle 1 n
= 250
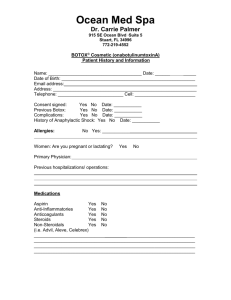
Fig. 1 – Patient disposition for the intention-to-treat population.
251
3.
Results
3.1.
Demographic and disease characteristics
The ITT population consisted of 548 randomised patients, of whom 489 patients (89.2%) completed the 24-wk study and
59 patients (10.8%) discontinued early (
); 223 (82.3%) and 163 (58.8%) patients who initially received placebo and onabotulinumtoxinA, respectively, received retreatment.
Only nine patients (1.6%) discontinued due to AEs. Baseline characteristics were balanced between the treatment
groups ( Table 1 ), with a slightly higher weight in the
placebo group. Patients had OAB for a mean duration of 5.5
yr and had taken an average of 2.4 anticholinergic medications prior to study entry; the primary reason for the inadequate management of the patients’ OAB was inadequate efficacy. Patients experienced a mean of 5.6 UI episodes per day at baseline.
3.2.
Overactive bladder symptoms
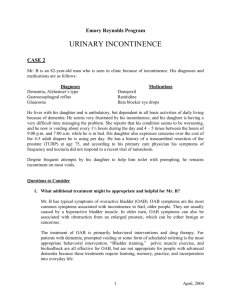
OnabotulinumtoxinA significantly decreased the co–primary end point of UI episodes per day; at wk 12, the mean decreases from baseline were 2.95 and 1.03 in the onabotulinumtoxinA and placebo groups, respectively
( p < 0.001). Significant reductions from baseline compared with placebo in all other OAB symptoms were also observed at wk 12 following treatment with onabotulinumtoxinA 100
U ( p < 0.001 for all except nocturia, which was p < 0.01)
(
). Significant differences from placebo occurred from the first evaluation visit at wk 2 posttreatment.
The significant reductions from baseline in onabotulinumtoxinA treatment compared with placebo corresponded to a large separation between the treatment groups in all OAB symptoms in the percentage decreases from baseline. For example, at wk 12, the percentage decreases from baseline
Table 1 – Baseline demographics and disease characteristics of the intention-to-treat population
Characteristic Placebo, n = 271
OnabotA 100 U, n = 277
Age, yr
Age group, no. (%)
65 yr
75 yr
Female, no. (%)
Weight, kg
Height, cm
Duration of OAB, yr
Prior anticholinergic use
Duration, yr
Anticholinergics, no.
Daily UI episodes, no.
Daily UUI episodes, no.
Daily micturition episodes, no.
Daily urgency episodes, no.
Daily nocturia episodes, no.
PVR urine volume, ml
I-QOL score
Total summary
Avoidance and Limiting Behaviour
Psychosocial Impact
Social Embarrassment
KHQ multi-item domain score
Role Limitations
Social Limitations
Physical Limitations
Personal Relationships
Emotions
Sleep/Energy
Severity/Coping Measures
KHQ single-item domain score
General Health Perception
Incontinence Impact
59.2
66.5
14.1
108 (39.9)
35 (12.9)
229 (84.5)
80.9
165.7
5.7
2.1
19.7
8.7
6.7
2.5
1.5
5.7
3.9
5.2
11.8
8.8
2.1
13.8
32.1
31.4
38.2
22.4
66.4
45.4
69.5
17.2
16.4
22.4
19.9
26.8
30.8
27.1
38.8
36.5
60.8
28.4
64.9
2.9
3.7
3.6
4.5
1.5
20.6
26.6
23.1
59.5
124 (44.8)
42 (15.2)
244 (88.1)
77.7
164.5
5.2
2.2
5.1
12.0
9.1
2.2
17.2
31.7
30.6
37.9
23.0
69.6
49.1
70.5
66.4
15.5
17.0
8.8
6.3
2.7
2.3
1.5
5.5
3.8
3.7
4.0
4.6
1.5
23.1
17.0
15.9
22.7
19.5
26.8
31.5
27.2
40.7
36.0
62.4
29.9
64.8
27.9
23.2
41.3
26.2
85.6
21.9
39.8
24.9
85.6
23.6
I-QOL = Incontinence Quality of Life; KHQ = King’s Health Questionnaire;
OAB = overactive bladder; OnabotA = onabotulinumtoxinA; PVR = postvoid residual; UI = urinary incontinence; UUI = urinary urgency incontinence.
Values are mean plus or minus standard deviation, unless indicated otherwise.
252 E U R O P E A N U R O L O G Y 6 4 ( 2 0 1 3 ) 2 4 9 – 2 5 6
Table 2 – Mean change and percentage change from baseline in daily urinary incontinence, micturition, urgency, and nocturia episodes in the intention-to-treat population
Mean change from baseline, episodes per day (95% CI) Mean change from baseline, %
OnabotA 100 U, n = 277 Placebo, n = 271 OnabotA 100 U, n = 277 Placebo, n = 271
UI episodes
Week 2
Week 6
Week 12
1.34
( 1.66 to 1.01)
1.37
( 1.73 to 1.02)
1.03
( 1.39 to 0.67)
( 3.27 to 2.43)
( 3.60 to 2.75)
( 3.37 to 2.53)
25.7
25.5
16.8
UUI episodes
Week 2
Week 6
Week 12
1.27
( 1.58 to 0.96)
1.22
( 1.56 to 0.88)
0.82
( 1.16 to 0.48)
( 3.21 to 2.36)
( 3.50 to 2.66)
( 3.23 to 2.38)
26.5
25.0
13.9
Micturition episodes
Week 2
Week 6
Week 12
0.77
( 1.07 to 0.47)
0.97
( 1.29 to 0.66)
0.83
( 1.14 to 0.53)
1.48
y
( 1.91 to 1.06)
( 2.79 to 2.01)
( 2.97 to 2.16)
6.1
7.3
6.0
Urgency episodes
Week 2
Week 6
Week 12
1.36
( 1.76 to 0.96)
1.35
( 1.80 to 0.90)
1.24
( 1.70 to 0.78)
( 3.49 to 2.40)
( 4.42 to 3.41)
( 4.19 to 3.15)
14.5
11.9
8.4
Nocturia episodes
Week 2
Week 6
Week 12
0.16
( 0.29 to 0.03)
(
0.27
( 0.41 to 0.13)
0.25
0.38 to 0.12)
0.36
z
( 0.49 to 0.23)
0.54
y
( 0.67 to 0.41)
0.54
y
( 0.70 to 0.38)
1.8
5.2
8.8
*
CI = confidence interval; onabotA = onabotulinumtoxinA; UI = urinary incontinence; UUI = urgency urinary incontinence.
p < 0.001.
y p < 0.01.
z p < 0.05.
52.0
58.2
53.1
53.6
61.5
53.2
9.8
17.8
19.7
31.5
45.3
41.1
16.6
26.4
25.1
for onabotulinumtoxinA and placebo groups, respectively, were 53.1% and 16.8% for UI episodes per day, 19.7% and
6.0% for micturition episodes, and 25.1% and 8.8% for nocturia episodes (
3.3.
Treatment benefit
The patients’ perception of change in their condition using the TBS, the co–primary variable, demonstrated a large and significant difference between the onabotulinumtoxinA and placebo groups in the proportion of patients with a positive response at wk 12 (62.8% versus 26.8%; p < 0.001) (
Between-group differences were observed beginning from the first posttreatment evaluation at wk 2 ( p < 0.001 at each comparison).
3.4.
Health-related quality of life
Patients experienced poor HRQOL at baseline as reflected by the low I-QOL total summary scores and high KHQ domain
). Compared with placebo, there were significant improvements in the I-QOL total summary score and all three domain scores in the onabotulinumtoxinA group ( p < 0.001) (
A). The improvement from baseline following onabotulinumtoxinA treatment far exceeded the predefined minimal important difference (MID) of a 10point increase
[22] ; for example, the mean increase in I-QOL
total summary score at wk 12 was 23.1 compared with 6.3
in the onabotulinumtoxinA and placebo groups, respectively. Likewise, improvements from baseline in all seven multiitem domains of the KHQ were far greater in the onabotulinumtoxinA group than the MID of a 5-point decrease
and were significantly greater than placebo
( p <
B). For example, the decrease from baseline at wk 12 in the Role Limitations domain was 26.5
and 5.0 in the onabotulinumtoxinA and placebo groups, respectively. This was also the case for the KHQ single-item domain of Incontinence Impact, whereas the MID was not reached for the non–disease-specific single-item domain of
General Health Perception.
E U R O P E A N U R O L O G Y 6 4 ( 2 0 1 3 ) 2 4 9 – 2 5 6 253
A
–2.5
–3
–3.5
–4
–0.5
–1
–1.5
–2
0
0
B
100
80
60
40
20
2
–1.34
–2.85
36.8
*
*
64.2
Time posttreatment, wk
4 6 8
–1.37
–3.18
30.9
*
*
69.3
10
26.8
12
–1.03
–2.95
*
Placebo
OnabotA 100 U
0
2 6
Time posttreatment, wk
12
Fig. 2 – Change from baseline in (A) daily average frequency of urinary incontinence (UI) episodes and (B) proportion of patients with a positive response (greatly improved or improved) on the treatment benefit scale in the intention-to-treat population.
OnabotA = onabotulinumtoxinA.
* p < 0.001.
3.5.
Safety and tolerability
In both the first 12 wk posttreatment and across the entire treatment cycle, the most common AEs in the
Table 4 – Mean change from baseline in postvoid residual urine volume and proportion of patients initiating clean intermittent catheterisation, both overall and by postvoid residual urine volume
Placebo, n = 270
OnabotA 100 U, n = 274
Proportion of patients with maximum change from baseline in PVR to different thresholds, no. (%)
100 ml
> 100 and
200 and < 350 ml
350 ml
< 200 ml
254 (94.1)
13 (4.8)
2 (0.7)
1 (0.4)
Proportion of patients initiating CIC
207 (75.8)
42 (15.4)
16 (5.9)
8 (2.9)
19 (6.9) Overall, no. (%) 2 (0.7)
By maximum attained PVR urine volume, n/N (%)
100 ml
> 100 and < 200 ml
1/244 (0.4)
0/22 (0)
200 and
350 ml
< 350 ml 0/3 (0)
1/1 (100)
1/192 (0.5)
1/53 (1.8)
7/17 (41.1)
10/11 (90.9)
CIC = clean intermittent catheterisation; OnabotA = onabotulinumtoxinA;
PVR = postvoid residual.
Placebo
OnabotA 100 U
*
62.8
onabotulinumtoxinA group, which were more prevalent compared with the placebo group, were urologic events, with the majority occurring within the first 12 wk after
). Uncomplicated UTI was the most frequently reported AE. The one case of complicated UTI was pyelonephritis that occurred approximately 4 mo after treatment with onabotulinumtoxinA.
The majority of patients (75.8%) did not have an increase from baseline in PVR > 100 ml following treatment with
onabotulinumtoxinA 100 U ( Table 4
), and only 8.8% of patients in the onabotulinumtoxinA group had a change from baseline in PVR 200 ml at any point during the treatment cycle. The proportion of patients who initiated
CIC following onabotulinumtoxinA treatment was 6.9%. CIC was started in nearly all patients within the first 12 wk following treatment; only two patients in the placebo group
(0.7%) initiated CIC. All patients with a PVR 350 ml initiated CIC, apart from 1 patient (10 of 11 patients), whereas in patients who had a PVR volume 200 and
< 350 ml, only 41.1% initiated CIC (7 of 17 patients).
Discontinuations due to AEs were infrequent; 1.5% and
0.7% of patients in the onabotulinumtoxinA and placebo groups withdrew for this reason during the treatment cycle
Table 3 – Safety parameters in the first 12 weeks and any time during the treatment cycle in the safety population
Adverse event First 12 wk Entire treatment cycle
Placebo, n = 270 OnabotA 100 U, n = 274 Placebo, n = 270 OnabotA 100 U, n = 274
AEs with incidence 3%, no. (%)
UTI
Dysuria
Bacteriuria
Urinary retention
Haematuria
Leukocyturia
Residual urine volume
Discontinuations, no. (%)
Due to AEs
14 (5.2)
10 (3.7)
6 (2.2)
1 (0.4)
1 (0.4)
2 (0.7)
1 (0.4)
15 (5.6)
2 (0.7)
56 (20.4)
16 (5.8)
10 (3.6)
16 (5.8)
10 (3.6)
7 (2.6)
8 (2.9)
9 (3.3)
2 (0.7)
AE = adverse event; OnabotA = onabotulinumtoxinA; UTI = urinary tract infection.
26 (9.6)
11 (4.1)
9 (3.3)
1 (0.4)
2 (0.7)
2 (0.7)
2 (0.7)
23 (8.5)
2 (0.7)
66 (24.1)
16 (5.8)
17 (6.2)
16 (5.8)
10 (3.6)
10 (3.6)
9 (3.3)
18 (6.6)
4 (1.5)
254 E U R O P E A N U R O L O G Y 6 4 ( 2 0 1 3 ) 2 4 9 – 2 5 6
A
35
30
25
20
15
10
5
0
Avoidance and
Limiting
Behaviour
Psychosocial
Impact
Social
Embarrassment
Total summary score
B
0
–5
–10
–15
–20
–25
–30
–35
Fig. 3 – Change from baseline in (A) Incontinence Quality of Life total and domain scores and (B) King’s Health Questionnaire single- and multi-item domain scores at week 12 in the intention-to-treat population. Dashed lines indicate the respective minimal important differences.
OnabotA = onabotulinumtoxinA.
* p < 0.001.
y p < 0.05.
(
Table 3 ). One patient treated with onabotulinumtoxinA
died during the study due to acute myocardial infarction, which was not considered to be related to the study treatment.
4.
Discussion
This study is one of the largest randomised, placebocontrolled studies performed to date in patients with OAB and UI who were not adequately managed with anticholinergic therapy. The results demonstrate that treatment with onabotulinumtoxinA 100 U provides both statistically significant and, more importantly, clinically relevant improvements in all OAB symptoms. This finding was clearly substantiated by the results of the TBS, which confirmed that patients perceived a significant overall improvement in their condition. These results are consistent with those from another large placebo-controlled clinical trial of onabotulinumtoxinA in OAB patients with UI
[20] , which showed a mean decrease from baseline in UI
episodes per day of 2.65 at wk 12 following treatment with onabotulinumtoxinA 100 U, in line with the mean decrease of 2.95 observed in the present study. TBS improvements following onabotulinumtoxinA treatment were also similar in the two studies, with 60.8% of patients reporting a positive treatment response at wk 12 in the previous trial compared with 62.8% in this study. Yet another large randomised clinical trial
demonstrated reductions in UUI episodes with onabotulinumtoxinA treatment that were also similar to those in this study, with a reduction of approximately 3 UUI episodes per day at month 3 compared with 2.80 in this study. Finally, the results of this trial are consistent with those of other smaller trials and case series in which onabotulinumtoxinA treatment improved OAB symptoms
.
The clinically meaningful improvement in OAB symptoms following onabotulinumtoxinA treatment resulted in positive effects on patients’ HRQOL, as reflected by the fact that the change from baseline in all I-QOL and diseasespecific KHQ domains far exceeded the respective published
E U R O P E A N U R O L O G Y 6 4 ( 2 0 1 3 ) 2 4 9 – 2 5 6 255
MIDs. These domains reflect the impact of OAB with associated UI on a number of social aspects, which contribute greatly to the HRQOL of patients. The improvements in HRQOL are consistent with previous observations in a phase 2 dose-ranging study of onabotulinumtoxinA
[19] . Together, these data indicate that the improvements in
OAB symptoms following onabotulinumtoxinA treatment translate into relevant effects on patients’ lives.
The significant clinical efficacy of onabotulinumtoxinA may be explained by its proposed dual mechanism of action in targeting both the afferent and efferent neuronal pathways of bladder control. OnabotulinumtoxinA blocks the release of acetylcholine and other neurotransmitters and may decrease the expression of sensory receptors
.
Overall, treatment with onabotulinumtoxinA was well tolerated. Most AEs were localised to the urinary tract, in contrast to the systemic effects observed with anticholinergic treatments. Although more patients treated with onabotulinumtoxinA experienced PVR urine volumes
> 100 ml compared with patients treated with placebo, only 6.9% of patients had an elevation that required the initiation of CIC. This percentage is on the lower end of that reported in the published literature
to higher doses previously being used or differing guidance provided in other studies regarding when CIC should be started. For example, in this study, when PVR was 200 ml but < 350 ml, CIC was to be initiated only if the patient experienced associated symptoms that were considered to warrant CIC, whereas in other studies, the initiation of CIC was mandated at that PVR volume.
One limitation of this study is that comparisons with placebo were not appropriate after wk 12, since patients could request and receive retreatment beyond that point. To address the long-term efficacy, an ongoing study is currently assessing the efficacy of repeated treatments of onabotulinumtoxinA. Another limitation is that the definition of UTI was based purely on central laboratory findings, using a low threshold of leukocytes
, and was not dependent on patients’ symptoms, which may be different in clinical practice.
5.
Conclusions
In this large phase 3 clinical study, onabotulinumtoxinA 100
U treatment was associated with significant and clinically relevant reductions in all OAB symptoms compared with placebo in patients experiencing OAB with UI who were inadequately managed with anticholinergic therapy. This finding was reflected in the patients’ perception of improvement in their condition and a clear positive impact on their
HRQOL. OnabotulinumtoxinA 100 U, which is a lower dose than previously evaluated in other placebo-controlled studies, was well tolerated, with a lower incidence of PVR elevation requiring CIC than previously observed. Results from this study indicate that onabotulinumtoxinA 100 U is an effective treatment option for patients with OAB and
UI who have not been adequately managed by prior anticholinergic therapy.
Author contributions: Christopher Chapple had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Study concept and design: Nardo, Thompson, Haag-Molkenteller.
Acquisition of data: Chapple, Sievert, MacDiarmid, Khullar, Radziszewski.
Analysis and interpretation of data: Chapple, Sievert, MacDiarmid, Khullar,
Radziszewski, Nardo, Thompson, Zhou, Haag-Molkenteller.
Drafting of the manuscript: Chapple, Sievert, MacDiarmid, Khullar,
Radziszewski, Nardo, Thompson, Zhou, Haag-Molkenteller.
Critical revision of the manuscript for important intellectual content:
Chapple, Sievert, MacDiarmid, Khullar, Radziszewski, Nardo, Thompson,
Zhou, Haag-Molkenteller.
Statistical analysis: Zhou.
Obtaining funding: Haag-Molkenteller.
Administrative, technical, or material support: Nardo.
Supervision: Nardo, Thompson, Haag-Molkenteller.
Other (specify): None.
Financial disclosures: Christopher Chapple certifies that all conflicts of interest, including specific financial interests and relationships and affiliations relevant to the subject matter or materials discussed in the manuscript (eg, employment/affiliation, grants or funding, consultancies, honoraria, stock ownership or options, expert testimony, royalties, or patents filed, received, or pending), are the following: Christopher
Chapple: consultant for AMS and Lilly; consultant and researcher for
ONO; consultant, researcher, and speaker for Allergan, Astellas, Pfizer, and Recordati; speaker for Ranbaxy. Karl-Dietrich Sievert: consultant, speaker honorarium, research grants, and trial participation for
Medtronic and Neotract; consultant, research grant, and trial participation for Allergan, Inc.; consultant, speaker honorarium, and travel grants for Astellas and AMS; fellowship, speaker honorarium, research grants, and travel grants from Karl Storz; fellowship from AMS; consultant for
Jansen. Scott MacDiarmid: speaker bureau and consultant for Allergan,
Inc., Astellas, Uroplasty, and Pfizer; consultant for Ferring. Vik Khullar: consultant/advisor, investigator, meeting participant/lecturer, and scientific study/trial for Allergan, Inc., Astellas, and Pfizer. Piotr
Radziszewski: consultant, lecturer, and clinical trials for Allergan, Inc., and Astellas; consultant for Glaxo, Recordati, Coloplast, and Teva; lecturer for Glaxo, Lilly, and Pfizer. Christopher Nardo, Catherine
Thompson, Jihao Zhou, and Cornelia Haag-Molkenteller are all employees of Allergan, Inc., and have stock options in the company.
Funding/Support and role of the sponsor: Allergan, Inc. helped design and conduct the study; collect, manage, analyse, and interpret the data; and prepare, review, and approve the manuscript.
Acknowledgement statement: The authors acknowledge Jennifer L. Giel,
PhD, of Evidence Scientific Solutions (Philadelphia, PA, USA) for assistance with writing and developing the manuscript.
Appendix. – Participating EMBARK Investigator Sites
Belgium: D. DeRidder, K. Everaert, V. Keppenne, B.
Kimpe, T. Quackels, S. Schapmans, P. Vossaert, J-J. Wyndaele.
Czech Republic: J. Heracek, V. Janda, J. Mecl, P.
Navratil, J. Schraml, M. Sincl, V. Student, J. Vseticka.
Germany: S. Carl, E. Hessdoerfer, A. Kaufmann, R. Kirschner-Hermanns, H. Loertzer, U. Peschers.
Poland: L. Grochala, Z. Jablonska, R. Kmieciak, T. Rechberger.
Russia: S. Al-
Shukri, O. Apolikhin, S. Darenkov, A. Gorelov, S. Gorelov, D.
Pushkar, O. Teodorovich, G. Uchvatkin.
United Kingdom:
M. Drake, P. Granitsiotis, M. Lucas, M. Parsons, M. Speakman.
United States: J.L. Bailen, D. Finn, D. Glazier, E.
256 E U R O P E A N U R O L O G Y 6 4 ( 2 0 1 3 ) 2 4 9 – 2 5 6
Goldfischer, L. Green, R.H. Greengold, G. Karlin, C. King, A.
Kohan, K. McCammon, R.D. Moore, M.I. Murdock, D.
Oselinsky, M. Platt, H. Samowitz, J.D. Small, C.A. Smith, J.
Sobol, C.P. Steidle, S. Varady.
References
[1] Abrams P, Artibani W, Cardozo L, Dmochowski R, van Kerrebroeck P,
Sand P. Reviewing the ICS 2002 terminology report: the ongoing debate. Neurourol Urodyn 2009;28:287.
[2] Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology of lower urinary tract function: report from the Standardisation
Sub-committee of the International Continence Society. Neurourol
Urodyn 2002;21:167–78.
[3] Onukwugha E, Zuckerman IH, McNally D, Coyne KS, Vats V, Mullins
CD. The total economic burden of overactive bladder in the United
States: a disease-specific approach. Am J Manag Care 2009;15:
S90–7.
[4] Stewart WF, Van Rooyen JB, Cundiff GW, et al. Prevalence and burden of overactive bladder in the United States. World J Urol
2003;20:327–36.
[5] Irwin DE, Milsom I, Hunskaar S, et al. Population-based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: results of the EPIC study. Eur Urol
2006;50:1306–15, discussion 1314–5.
[6] Milsom I, Abrams P, Cardozo L, Roberts RG, Thuroff J, Wein AJ. How widespread are the symptoms of an overactive bladder and how are they managed? A population-based prevalence study. BJU Int
2001;87:760–6.
[7] O’Conor RM, Johannesson M, Hass SL, Kobelt-Nguyen G. Urge incontinence: quality of life and patients’ valuation of symptom reduction. Pharmacoeconomics 1998;14:531–9.
[8] Chiaffarino F, Parazzini F, Lavezzari M, Giambanco V. Impact of urinary incontinence and overactive bladder on quality of life. Eur
Urol 2003;43:535–8.
[9] Coyne KS, Sexton CC, Irwin DE, Kopp ZS, Kelleher CJ, Milsom I. The impact of overactive bladder, incontinence and other lower urinary tract symptoms on quality of life, work productivity, sexuality and emotional well-being in men and women: results from the EPIC study. BJU Int 2008;101:1388–95.
[10] Mittmann N, Trakas K, Risebrough N, Liu BA. Utility scores for chronic conditions in a community-dwelling population. Pharmacoeconomics 1999;15:369–76.
[11] Sexton CC, Coyne KS, Vats V, Kopp ZS, Irwin DE, Wagner TH. Impact of overactive bladder on work productivity in the United States: results from EpiLUTS. Am J Manag Care 2009;15(Suppl 4):S98–107.
[12] Bartoli S, Aguzzi G, Tarricone R. Impact on quality of life of urinary incontinence and overactive bladder: a systematic literature review. Urology 2010;75:491–500.
[13] Chapple CR, Khullar V, Gabriel Z, Muston D, Bitoun CE, Weinstein D.
The effects of antimuscarinic treatments in overactive bladder: an update of a systematic review and meta-analysis. Eur Urol
2008;54:543–62.
[14] Allahdin S, Oo N. An overview of treatment of overactive bladder syndrome in women. J Obstet Gynaecol 2012;32:217–21.
[15] Sexton CC, Notte SM, Maroulis C, et al. Persistence and adherence in the treatment of overactive bladder syndrome with anticholinergic therapy: a systematic review of the literature. Int J Clin Pract
2011;65:567–85.
[16] Brostrom S, Hallas J. Persistence of antimuscarinic drug use. Eur J
Clin Pharmacol 2009;65:309–14.
[17] Dmochowski R, Chapple C, Nitti VW, et al. Efficacy and safety of onabotulinumtoxinA for idiopathic overactive bladder: a doubleblind, placebo controlled, randomized, dose ranging trial. J Urol
2010;184:2416–22.
[18] Rovner E, Kennelly M, Schulte-Baukloh H, Zhou J, Haag-Molkenteller C, Dasgupta P. Urodynamic results and clinical outcomes with intradetrusor injections of onabotulinumtoxinA in a randomized, placebo-controlled dose-finding study in idiopathic overactive bladder. Neurourol Urodyn 2011;30:556–62.
[19] Fowler CJ, Auerbach S, Ginsberg D, et al. OnabotulinumtoxinA improves health-related quality of life in patients with urinary incontinence due to idiopathic overactive bladder: a 36-week, double-blind, placebo-controlled, randomized, dose-ranging trial.
Eur Urol 2012;62:148–57.
[20] Nitti VW, Dmochowski R, Herschorn S, et al. OnabotulinumtoxinA for the treatment of patients with overactive bladder and urinary incontinence: results of a phase 3, randomized, placebo-controlled trial. J Urol 2013;189:2186–93.
[21] Colman S, Chapple C, Nitti V, Haag-Molkenteller C, Hastedt C,
Massow U. Validation of treatment benefit scale for assessing subjective outcomes in treatment of overactive bladder. Urology
2008;72:803–7.
[22] Patrick DL, Martin ML, Bushnell DM, Marquis P, Andrejasich CM,
Buesching DP. Cultural adaptation of a quality-of-life measure for urinary incontinence. Eur Urol 1999;36:427–35.
[23] Kelleher CJ, Cardozo LD, Khullar V, Salvatore S. A new questionnaire to assess the quality of life of urinary incontinent women. Br J
Obstet Gynaecol 1997;104:1374–9.
[24] Kelleher CJ, Pleil AM, Reese PR, Burgess SM, Brodish PH. How much is enough and who says so? BJOG 2004;111:605–12.
[25] Visco AG, Brubaker L, Richter HE, et al. Anticholinergic therapy vs.
onabotulinumtoxinA for urgency urinary incontinence. N Engl J
Med 2012;367:1803–13.
[26] Anger JT, Weinberg A, Suttorp MJ, Litwin MS, Shekelle PG. Outcomes of intravesical botulinum toxin for idiopathic overactive bladder symptoms: a systematic review of the literature. J Urol
2010;183:2258–64.
[27] Mangera A, Andersson KE, Apostolidis A, et al. Contemporary management of lower urinary tract disease with botulinum toxin
A: a systematic review of Botox (onabotulinumtoxinA) and Dysport
(abobotulinumtoxinA). Eur Urol 2011;60:784–95.
[28] Apostolidis A, Dasgupta P, Fowler CJ. Proposed mechanism for the efficacy of injected botulinum toxin in the treatment of human detrusor overactivity. Eur Urol 2006;49:644–50.
[29] Yokoyama T, Chancellor MB, Oguma K, et al. Botulinum toxin type A for the treatment of lower urinary tract disorders. Int J Urol
2012;19:202–15.
[30] Stamm WE. Measurement of pyuria and its relation to bacteriuria.
Am J Med 1983;75:53–8.