Excess Alcohol Greatly Increases the Prevalence of Cirrhosis in
advertisement

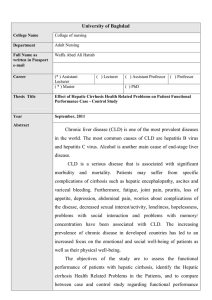
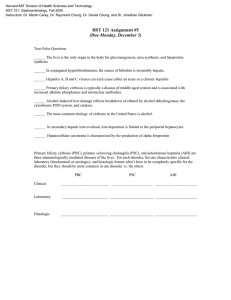
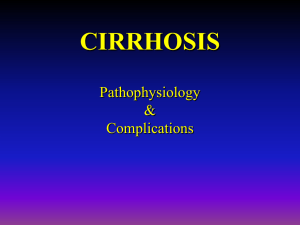
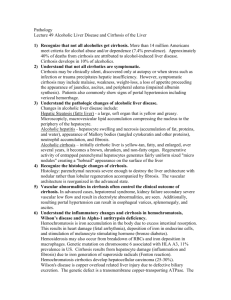
GASTROENTEROLOGY 2002;122:281–289 Excess Alcohol Greatly Increases the Prevalence of Cirrhosis in Hereditary Hemochromatosis LINDA M. FLETCHER,* JEANNETTE L. DIXON,‡ DAVID M. PURDIE,‡ LAWRIE W. POWELL,‡ and DARRELL H. G. CRAWFORD* *Department of Gastroenterology and Hepatology, Princess Alexandra Hospital, and ‡Population Health and Clinical Sciences Division, The Queensland Institute of Medical Research, Brisbane, Australia See editorial on page 563. Background & Aims: The progression of fibrosis to cirrhosis is the most significant prognostic factor in hereditary hemochromatosis. We aimed to determine the range of hepatic iron concentration associated with cirrhosis in the absence of alcohol and other pro-fibrogenic cofactors and to quantify the contribution of excess alcohol consumption to the development of cirrhosis. Methods: Liver biopsy data were evaluated on 224 C282Y homozygous hemochromatosis subjects. To determine the effect of alcohol alone on the development of fibrosis, subjects with viral hepatitis or nonalcoholic steatohepatitis were excluded. Subjects were divided into those who consumed less than 60 g alcohol per day and those who consumed 60 g per day or more. Results: Seven percent of subjects who consumed less than 60 g per day had severe fibrosis/cirrhosis compared with 61% of excess alcohol consumers. Conclusions: Hemochromatosis subjects who drink more than 60 g alcohol per day are approximately 9 times more likely to develop cirrhosis than those who drink less than this amount, and the range of hepatic iron concentration associated with cirrhosis in the absence of cofactors was 233– 675 mol/g dry weight. he excess iron that is characteristically deposited in a periportal distribution in hepatocytes in hereditary hemochromatosis (HHC) results in significant toxicity. A number of studies have suggested that the excess iron generates reactive oxygen species that exceed the normal antioxidant defenses and cause peroxidation of lipid membranes resulting in cell damage.1– 4 The subsequent cellular response in the liver as it attempts repair of this injury, is associated with the initiation of fibrogenic pathways.5,6 Progression from fibrosis to cirrhosis is critical in the clinical management of HHC because cirrhosis is associated with significant reduction in life expectancy as the 5-year survival in untreated cirrhotic patients is T 50%.7–9 There is also a greatly increased risk of development of primary hepatocellular carcinoma (HCC).10 Liver disease of various causes may have similar basic mechanisms underlying fibrogenesis to iron toxicity. Reactive oxygen species have been implicated in stellate cell activation in alcoholic liver disease, nonalcoholic steatohepatitis (NASH), and chronic viral hepatitis.11–15 Progressive fibrosis and cirrhosis develop in up to 20%–30% of subjects with these diseases if the offending insult is not attenuated. A combination of 2 or more toxic insults may potentiate more aggressive disease. For example, alcohol consumption has been shown to have a significant impact on both the histologic and clinical progression of chronic hepatitis C virus infection,16 –18 and iron overload complicated by viral hepatitis and/or alcohol may have accelerated the development of cirrhosis.19 –23 The extent to which iron alone contributes towards the development of fibrosis and therefore to the pathogenesis of the liver disease in HHC remains unclear. It has been previously suggested that the critical iron threshold at which fibrosis/cirrhosis occurs is 400 –500 mol/g dry weight, although patients in these studies may have had other concomitant liver disease.24,25 Although there is general agreement that the mean hepatic iron concentration (HIC) is higher in HHC patients with cirrhosis compared with those without cirrhosis, it seems unlikely that there exists a discrete threshold value for cirrhosis. Rather, it is more likely that there is range of the HIC above which the risk of cirrhosis is increased and below which the risk is low. In this study, we reevaluated the range of hepatic iron associated with cirrhosis in HHC in subjects without any profibrogenic stimuli other than iron. In addition, we aimed to quantify the additive Abbreviations used in this paper: HCC, hepatocellular carcinoma; HFE, hemochromatosis gene; HHC, hereditary hemochromatosis; HIC, hepatic iron concentration; HII, hepatic iron index; NASH, nonalcoholic steatohepatitis. © 2002 by the American Gastroenterological Association 0016-5085/02/$35.00 doi:10.1053/gast.2002.30992 282 FLETCHER ET AL. effect of excessive alcohol consumption to the development of severe fibrosis/cirrhosis in HHC. Materials and Methods Subjects The 224 subjects included in this study form part of a comprehensive and well characterized data base of hemochromatosis subjects and their families. Subjects were included in this study if they had been genotyped for mutations in the hemochromatosis gene (HFE), had undergone liver biopsy with measurement of HIC, and had available serum biochemical data measured at the time of biopsy. No subject had commenced venesection therapy or was a regular blood donor. All subjects were homozygous for the C282Y mutation in HFE. Subjects aged less than 20 years were excluded because the likelihood of significant fibrosis being present in subjects less than 20 years of age was small.26 Clinical and Laboratory Data All subjects were interrogated and the data recorded predominantly by 1 physician (L.W.P.) and no more than 3 different physicians. Alcohol consumption was assessed by detailed questioning of patients (and in some cases relatives) and reflected both current and past (⬎10 years) drinking habits in grams of ethanol equivalent per day. Serum concentration of alanine aminotransferase, aspartate aminotransferase, gamma glutamyltransferase, and biochemical indices of iron proteins (serum ferritin, transferrin saturation) were measured by standard biochemical analyses. Liver blood tests were classed as abnormal if either one or more of alanine aminotransferase, aspartate aminotransferase, and gamma glutamyltransferase were elevated above the laboratory reference range. Viral serology (anti– hepatitis C virus and hepatitis B surface antigen) was determined when liver blood tests were abnormal. In those subjects in which laboratory testing was not available, clinical evaluation did not suggest chronic viral hepatitis in any patient. HIC HIC was measured by atomic absorption spectrophotometry on fresh biopsy specimens as previously described.24 We included iron-loaded rat liver as an internal control. The hepatic iron index (HII) was calculated as previously described (HII ⫽ HIC/age).24 Histologic Grading of Fibrosis and Steatosis Liver biopsies were stained with hematoxylin and eosin, van Gieson’s and Masson’s trichrome for collagen, and Perls’ Prussian blue for iron. Histologic assessment of iron grade on a scale of 0 to 4 (according to the method of Scheuer) after Perls’ staining was performed.27 The level of fibrosis was recorded as 0, no fibrosis; 1, mild fibrosis with enlarged fibrotic portal tracts; 2, moderate peri-portal or portal-portal septa but intact architecture; 3, severe fibrosis with architectural distor- GASTROENTEROLOGY Vol. 122, No. 2 tion but no cirrhosis; and 4, cirrhosis with annular fibrosis with architectural distortion. Steatosis was recorded as mild, moderate, or severe. Patient Groups To determine the impact of alcohol alone on the development of fibrosis in subjects with iron overload, subjects who had concomitant liver disease whose pathogenesis is associated with fibrosis (viral hepatitis or NASH) were excluded from statistical analysis. Patients were divided into those who consumed less than 60 g alcohol per day and those who drank equal to or more than 60 g alcohol per day. Statistical Analysis The variables age, serum ferritin, transferrin saturation, HIC, and HII were all assessed for normality, and appropriate transformations were performed to normalize the measures for statistical analysis. Age was approximately normally distributed and thus required no transformation; HIC and HII were approximately normally distributed after natural log transformations; square root transformations of serum ferritin and transferrin saturation were applied to normalize the distribution of these variables. Mean ⫾ standard deviation (of the untransformed variables) was used to summarize these variables. Student t tests and analysis of variance were conducted on the transformed variables to test for differences in means between groups. Linear regression (on normalized measures) was used to compare means between groups while adjusting for potential confounding by age and/or sex. Pearson’s correlation coefficient was used to measure the degree of association between 2 approximately normally distributed measures; however, to assess the correlation between HIC and degree of fibrosis (graded 0 to 4), a Spearman’s non-parametric coefficient was used. To compare proportions between groups, Pearson’s chisquared tests were used; however, when comparisons of proportions were done on small subgroups (e.g., among cirrhotic patients), a Fisher exact test was used instead. For comparative purposes, subjects with mild and moderate fibrosis were grouped together and subjects with severe fibrosis and cirrhosis were also combined. The statistical package SPSS version 10.1 (SPSS Inc., North Sydney, Australia) was used to conduct all analyses. Results Figure 1 shows the distribution of the study population in relation to alcohol consumption and liver blood tests. Of the 224 subjects, 18 patients were excluded because of coexistent viral hepatitis (6) or NASH (12). One hundred seventy (82.5%) of the 206 remaining subjects had an alcohol consumption of less than 60 g per day, whereas 36 (17.5%) subjects drank equal to or more than 60 g alcohol per day. One hundred seventeen (68.8%) of those subjects who drank less than 60 g February 2002 IRON, ALCOHOL, AND CIRRHOSIS IN HEMOCHROMATOSIS Figure 1. Distribution of study population of hereditary hemochromatosis subjects in relation to alcohol consumption and liver blood tests. alcohol per day had normal liver blood tests. Of these, 88 had no fibrosis, 27 had mild or moderate fibrosis, and only 2 had cirrhosis. Fifty-three (31.1%) of the low alcohol consumers had abnormal liver blood tests. Twenty-three patients had no fibrosis, 20 had fibrosis, and 10 were cirrhotic. In contrast, the majority of subjects who drank 60 g per day or more had abnormal liver blood tests (28 of 36; 77.8%), and 21 of these 28 (75%) patients were cirrhotic, whereas one subject with normal liver blood tests was cirrhotic. The laboratory characteristics of patients in relation to alcohol consumption are detailed in Table 1. Male sub- 283 jects predominated over female subjects in both groups (M:F 104:66, 34:2, respectively), but there was a significantly higher proportion of males among those who drank 60 g or more of alcohol per day (94%) than in those who drank less than 60 g per day (61%; P ⬍ 0.001). The mean and median age were similar in both groups; however, serum ferritin concentration and transferrin saturation were significantly higher among high alcohol consumers, which remained after adjustment for sex differences between the groups (P ⬍ 0.001). Mean HIC and HII were similar between the 2 groups. HIC did not correlate with age in either of the 2 groups of patients (alcohol ⬍60 g/day, r ⫽ 0.235; alcohol ⬎60 g/day, r ⫽ 0.227). The overall distribution of subjects in relation to histologic iron grade was significantly different in low alcohol consumers when compared with heavy alcohol consumers, indicating that the majority of heavy alcohol consumers were more likely to have higher iron grades (P ⬍ 0.033; Table 1). Relationship Between HIC, Alcohol, and Fibrosis HIC was positively correlated with degree of fibrosis (graded 0 to 4) in those subjects who drank less than 60 g per day (r ⫽ 0.379; P ⬍ 0.001) and in those subjects who consumed excess alcohol (Spearman’s r ⫽ 0.367; P ⫽ 0.027). The relationship between the HIC and degree of fibrosis is shown in Figure 2. The HIC (mean ⫾ SD) in those subjects with an alcohol consump- Table 1. Characteristics of C282Y Homozygous HHC Patients Grouped Into Those Who Consume Less Than 60 g Alcohol per Day and Those Who Consume Equal to or More Than 60 g Alcohol Per Day Total population n ⫽ 206 Alcohol ⬍ 60 g/day (n ⫽ 170) male:female 104:66 Alcohol ⱖ 60 g/day (n ⫽ 36) male:female 34:2 Variable Mean ⫾ SD Median Age ( yr) Serum ferritin (g/L) % Transferrin saturation HIC (mol/g dry weight) HII Elevated ALT and/or AST, GGT Fe grade (n) 1 2 3 4 42.3 ⫾ 14.6 41 946 ⫾ 836 678 77 ⫾ 18 81 27–100 89 ⫾ 12 182 ⫾ 120 4.5 ⫾ 3.0 148 3.7 23–675 0.5–18.8 31.2% N/A N/A 4 (2%) 23 (13%) 79 (47%) 64 (38%) Range 20–74 33–4500 Mean ⫾ SD Median 43 ⫾ 10 42 Range Sex-adjusted P value 0.652 0.402 405–4400 ⬍0.001 ⬍0.001 93 48–100 ⬍0.001 ⬍0.001 239 ⫾ 175 5.6 ⫾ 4.2 167 4.9 22–847 0.6 ⫾ 20.1 0.109 0.163 0.338 0.569 77.8% N/A N/A 2083 ⫾ 1159 1936 1 (3%) 3 (8%) 9 (25%) 23 (64%) 26–66 Crude P value ⬍0.001 0.033a ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, ␥-glutamyltransferase; N/A, nonapplicable. aSignificance of overall distribution of subjects in relation to iron grade in subjects who consume less than 60 g per day compared with those who consume equal to or more than 60 g per day. 284 FLETCHER ET AL. Figure 2. Relationship between HIC (mean ⫾ SD) and fibrosis in those subjects who consume less than 60 g alcohol per day (䊐) compared with those who drink greater than or equal to 60 g per day (1). Numbers in parentheses represent numbers of subjects in each group. *P value between groups with no fibrosis vs. severe/cirrhosis; mild/mod fibrosis vs. severe/cirrhosis in subjects with alcohol consumption ⬍60 g/day (䊐). **P value comparing patients with severe fibrosis/cirrhosis who consume ⬍60 g/day and those with severe fibrosis/cirrhosis who consume ⱖ60 g/day. tion of less than 60 g per day was 151 ⫾ 96 mol/g dry weight (n ⫽ 111), no fibrosis; 197 ⫾ 109 mol/g dry weight (n ⫽ 47), mild/moderate fibrosis; and 406 ⫾ 125 mol/g dry weight (n ⫽ 12), severe fibrosis/cirrhosis (normal range 5– 40 mol/g dry weight). The mean HIC of those subjects who consumed 60 g alcohol per day or more and who had cirrhosis (271 ⫾ 186 mol/g dry weight, n ⫽ 22) was significantly higher than those with no fibrosis (141 ⫾ 98 mol/g dry weight, n ⫽ 6), or mild/moderate fibrosis (228 ⫾ 179 mol/g dry weight, n ⫽ 8) (P ⬍ 0.001). There was no significant difference between the mean HIC in subjects with no fibrosis (P ⫽ 0.854) or subjects with mild/moderate fibrosis (P ⫽ GASTROENTEROLOGY Vol. 122, No. 2 0.913) who consumed less than 60 g alcohol per day compared with those who drank more than this amount. However, the mean HIC at which cirrhosis developed was lower in the alcoholic group compared with those subjects who consumed less than 60 g/day (P ⫽ 0.003). After adjusting for age and sex, this difference between drinking groups remained significant (P ⫽ 0.045), indicating that those subjects who had disease complicated by alcohol consumption developed cirrhosis at significantly lower HICs than those whose disease was not complicated by alcohol. The distribution of HIC in relation to the degree of fibrosis in both groups is shown in Figure 3. In the subjects who drank less than 60 g alcohol per day, cirrhosis was present in 12 (7%) subjects. Cirrhosis was, however, present in 22 of 36 (61.1%) of those subjects who consumed 60 g per day or more (Figure 3), indicating that cirrhosis was 8.7 (95% confidence interval ⫽ 4.7–15.8) times more frequent in HHC subjects who consumed alcohol in excess compared with those who did not. No subject who consumed less than 60 g alcohol per day and who had an HIC less than 233 developed cirrhosis; however, 50% of subjects who drank more than 60 g per day and had an HIC less than 233 had cirrhosis. When subjects who consumed less than 60 g alcohol per day were considered in relation to liver blood tests (Figure 4), only 2 subjects (1.7%) with normal liver blood tests had cirrhosis. These 2 subjects with normal liver blood tests were elderly men (aged 63 years and 67 years) who had markedly elevated serum ferritin (2231 and 3100 g/L, respectively). In subjects with abnormal liver blood tests, 18.9% (10 of 53) of subjects who consumed less than 60 g per day had cirrhosis compared with 75% (21 of 28) of subjects who consumed 60 g or more per Figure 3. Relationship between HIC and fibrosis in (A ) all subjects who consume less than 60 g alcohol/day (n ⫽ 170) and (B) those subjects who drink equal to or more than 60 g per day (n ⫽ 36). Numbers in parentheses represent numbers of subjects in each group. Horizontal bars represent mean HIC. February 2002 IRON, ALCOHOL, AND CIRRHOSIS IN HEMOCHROMATOSIS 285 Figure 4. Relationship between HIC and fibrosis in (A ) subjects who drink less than 60 g per day and who have normal liver blood tests (LBT) (n ⫽ 117) and (B) those who have abnormal LBT (n ⫽ 53). Numbers in parentheses represent numbers of subjects in each group. Horizontal bars represent mean HIC. day (P ⬍ 0.001; Figure 1). In addition, 75% (88 of 117) of subjects with elevated hepatic iron and normal liver blood tests who did not consume excess alcohol, had no fibrosis on liver biopsy. When age was taken into consideration via the calculation of the HII (Figure 5), the mean HII of cirrhotic subjects who consumed less than 60 g alcohol per day was higher (8.1 ⫾ 4.0) than those subjects who drank more than 60 g per day (6.0 ⫾ 4.2), and after adjusting for age and sex, this difference approached significance (P ⫽ 0.09). This further indicated that subjects who consume excess alcohol are likely to develop cirrhosis at lower HIC than those who do not. Irrespective of whether subjects consumed excess alcohol or not, 98 of the 206 subjects in the study had serum ferritin levels less than 1000 g/L and normal liver blood tests. None of these subjects had severe fibrosis/cirrhosis present on liver biopsy. One hundred eleven subjects (65.3%) who drank less than 60 g alcohol per day irrespective of liver blood tests did not have any hepatic fibrosis despite elevated HIC (mean 151 mol/g dry weight) compared with only 17% in those who drank 60 g or more per day. Characteristics of Cirrhotic Subjects The clinical characteristics of HHC subjects with cirrhosis are shown in Table 2. Twelve subjects (7.1%) in the low alcohol consuming group developed cirrhosis, compared with 61.1% percent in the group who drank more than 60 g per day (P ⬍ 0.001). Male subjects predominated in both groups. The mean age, HIC, and HII were lower in subjects who consumed alcohol in excess (P ⬍ 0.05); however, the mean serum ferritin was similar in both groups. Sixty-one percent of the heavy alcohol consumers had cirrhosis, and 77.8% had abnormal liver blood tests. Twenty-two of the 35 (62.3%) Figure 5. Relationship between HII and fibrosis in (A ) all subjects who consume less than 60 g alcohol per day (n ⫽ 170) and (B) those subjects who drink more than 60 g per day (n ⫽ 36). Numbers in parentheses represent numbers of subjects in each group. Horizontal bars represent mean HII. 286 FLETCHER ET AL. GASTROENTEROLOGY Vol. 122, No. 2 Table 2. Clinical Characteristics of HHC Subjects With Severe Fibrosis/Cirrhosis N (% of group) Male:female Age ( yr ) Serum ferritin (g/L) HIC (mol/g dry wt) (range) HII Elevated ALT and/or AST/GGT Alcohol ⬍ 60 g/da Alcohol ⱖ 60 g/da P value Adjusted P valueb 12 (7.1%) 11:1 53.7 ⫾ 11.9 2916 ⫾ 939 406 ⫾ 125 (233–675) 8.1 ⫾ 3.9 10/13 (76.9%) 22 (61.1%) 22:0 46.5 ⫾ 10.5 2667 ⫾ 1017 271 ⫾ 186 (22–847) 6.0 ⫾ 4.2 28/36 (77.8%) ⬍0.001 0.353 0.048 0.439 0.003 0.042 0.279 0.494 0.045 0.049 0.343 ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, ␥-glutamyltransferase. shown as mean ⫾ SD where applicable. bAdjusted for age and sex. aData cirrhotic subjects consumed alcohol in excess, confirming that alcohol is a significant co-factor in the pathogenesis of fibrosis in HHC. Eighty percent of the cirrhotic subjects had serum ferritin levels in excess of 2000 g/L. The prevalence of abnormal liver blood tests, steatosis, fibrosis, and HCC in those subjects who consumed less than 60 g alcohol per day compared with those who drink more than this amount is shown in Figure 6. With the exception of the percentage of subjects with fibrosis, which was not significantly different between the 2 groups, significantly more subjects who consumed alcohol in excess had abnormal liver blood tests, steatosis, cirrhosis, and HCC. Only 17% of heavy drinkers showed no fibrosis present on liver biopsy, compared with 65% of subjects who consumed less than 60 g alcohol per day (P ⬍ 0.001). There was a lack of histologic features of alcoholic liver disease in those subjects who consumed alcohol in excess, and only 25% had steatosis. Discussion We have investigated the prevalence of cirrhosis in 2 groups of subjects with C282Y-associated HHC Figure 6. The prevalence of abnormal liver blood tests, steatosis, fibrosis, cirrhosis, and HCC in relation to alcohol consumption in hereditary hemochromatosis (䊐, alcohol consumption ⬍60 g per day; 1, alcohol consumption ⱖ60 g per day). Numbers refer to number of subjects in each group. AbnLBT, abnormal liver blood tests; HCC, hepatocellular carcinoma. distinguished on the basis of exposure to excess alcohol. Our study showed that cirrhosis was relatively uncommon (7%) in subjects who consumed less than 60 g alcohol per day and present in only 1.7% of subjects in this group who had normal liver blood tests, despite elevated hepatic iron. In contrast, 61% of HHC individuals who had a history of exposure to alcohol in excess of 60 g per day had cirrhosis. This indicates that HHC subjects who consume alcohol in excess are almost 9 times more likely to develop cirrhosis than those who drink less than 60 g alcohol per day. The lowest HIC associated with cirrhosis in the low alcohol group was 233 mol/g, whereas 11 of 22 cirrhotic subjects in the high alcohol group had an HIC below this value. Thus, although severe fibrosis/cirrhosis is uncommon in HHC patients with low alcohol intake, excess alcohol consumption can significantly influence the development of cirrhosis even at modestly elevated HIC. None of the subjects in this study with normal liver blood tests and serum ferritin levels below 1000 g/L had cirrhosis, thus our study confirms the recommendation of Guyader et al.28 that liver biopsy was not recommended in such patients. However, we have highlighted the importance of also noting the alcohol history. Population screening studies for C282Y-associated HHC are being conducted in many centers throughout the world. Given this development, it is probable that practicing clinicians will see many more subjects who are otherwise well (i.e., normal liver blood tests and no risks for intercurrent liver disease), but who will have biochemical evidence of increased body iron stores. This study provides some insights into the most appropriate clinical management of such patients. Cirrhosis in C282Y homozygous patients has important clinical and prognostic significance, but in general those patients with normal liver blood tests and an alcohol consumption of less than 60 g per day can be reassured that the risk of underlying cirrhosis is small (⬍2% in this population). The 2 subjects who consumed less than 60 g alcohol per day who February 2002 had liver cirrhosis but normal liver blood tests, were elderly males (67 and 63 years of age) who had high hepatic iron stores (HIC 516 and 380; HII 7.7 and 6.0) and serum ferritin concentrations greater than 2000 g/L. This suggests the threshold for liver biopsy in such patients could be a serum ferritin of 2000 g/L. However, some caution should be exercised because of the small number of cirrhotic subjects in the group in which excess iron was the only toxic insult and studies of larger groups of patients are required to define more precisely their risk of cirrhosis and the appropriate threshold for liver biopsy. Our data also indicate that duration of exposure of the liver to high iron stores (and patient age) may be important in determining the risk of developing cirrhosis, particularly if liver blood tests are not elevated. Although duration of exposure to toxic insult from excessive hepatic iron was probably a significant determining factor of development of fibrosis in 2 subjects, fibrosis was absent in 4 other subjects aged greater than 60 years, with normal liver blood tests and elevated HIC (302, 322, 408, and 429 mol/g dry weight). It is possible that these subjects and indeed other subjects with elevated HIC but no fibrosis (65% subjects had no fibrosis), may have as yet undetermined factors that offer some protective effect against the development of fibrosis. In contrast, of the 22 subjects with cirrhosis who consumed 60 g alcohol per day or more, only one was older than 60 years, one subject was 60 years old at the time of diagnosis, whereas 20 others were aged 54 years or less. The mean age of cirrhotic patients who consumed excess alcohol was 46.5 ⫾ 10.5 years compared with 53.7 ⫾ 11.9 years in those cirrhotic patients who consumed less than 60 g of alcohol per day (Table 2, P ⫽ 0.048), indicating that cirrhosis develops at a significantly earlier age in HHC subjects who consume alcohol in excess of 60 g per day. We found a substantial overlap between HICs in cirrhotic alcoholic patients and cirrhotic patients with low alcohol intake. As suggested, individual susceptibility to fibrogenic stimuli—possibly related to age, gender, and other unidentified host factors—may all contribute to this overlap. The mean HIC was not decreased in the high alcohol group with mild/moderate fibrosis compared with the low alcohol group. This may be a result of the relatively small number of high alcohol users in the mild to moderate fibrosis group, and further studies with larger numbers of patients with milder degrees of fibrosis are necessary. Oxidative stress has been implicated as playing an important role in initiating the complex series of events involving interplay between parenchymal cells and non- IRON, ALCOHOL, AND CIRRHOSIS IN HEMOCHROMATOSIS 287 parenchymal cells that eventually results in hepatic stellate cell activation in subjects with iron overload.29,30 Many groups have found evidence of enhanced oxidative stress in liver tissue of iron-loaded subjects, and Houglum et al.2 showed that markers of oxidative stress decreased after venesection treatment in serum and liver samples from HHC patients. Many subjects in our study in which iron was the only toxin had no evidence of fibrosis, despite HIC within the range associated with cirrhosis. Clearly, elevated HIC does cause oxidative stress, but high concentrations of hepatic iron alone may be insufficient to overwhelm the antioxidant protective systems and/or stimulate hepatic fibrogenesis in many patients. Reactive oxygen species have been associated with stellate cell activation in other forms of hepatocellular disease such as hepatitis C. Hepatitis C patients who also drink alcohol to excess have more aggressive disease, and it is likely that the level of inflammation in these diseases may be important in this context.16,17 The progression of fibrosis to cirrhosis in different hepatocellular diseases may therefore be multifactorial. It has been suggested that an inflammatory response in association with increased tumor necrosis factor ␣ is an important component in the activation of stellate cells and subsequent fibrogenesis.31 The absence of a significant inflammatory infiltrate in HHC where iron is the only insult may also explain, in part, the reduced frequency of cirrhosis in uncomplicated HHC. Our observations are supported by findings in animal models of hemochromatosis whereby, despite intensive iron loading, significant fibrosis is not usually shown in iron-loaded rodents.32,33 A number of other reports have also implicated excessive alcohol consumption in more severe disease expression in iron overload disease,20 –22,25,34 and the severity of disease is attenuated by venesection therapy.9,35 The present study differs from earlier studies by including only C282Y homozygous individuals and excluding complicating factors contributing to fibrogenesis, apart from excess alcohol consumption, in the analysis. This more clearly identified the contribution of iron alone and the additive effect of alcohol to the development of fibrogenesis. In an experimental model of alcoholic liver disease, the addition of small amounts of iron to the diet of rats fed a high fat alcoholic diet resulted in significant fibrosis compared with those fed the high fat alcohol diet alone, where only mild fibrosis was reported.36 These small amounts of iron markedly exacerbated the oxidative stress and thus contributed to the pathogenesis of the liver disease. Just how much alcohol ingestion is required in hemochromatosis to initiate significant fibrosis is difficult to determine. We have chosen 60 g per day 288 FLETCHER ET AL. as a cutoff in the present study, and re-analysis of results using 40 g per day did not significantly alter our results. Bassett et al.24 suggested that the critical iron concentration at which fibrosis/cirrhosis occurred in homozygous hemochromatosis subjects approximated 400 mol/g dry weight. This was based on the fact that all 6 HLA-linked homozygous hemochromatosis subjects with an HIC of ⬎400 mol/g dry weight had cirrhosis. In our study, 11 subjects in the group who consumed less than 60 g/day had HICs above this level; however, only 4 of these subjects had cirrhosis. In the report by Bassett et al., a further 3 subjects with HIC below 400 mol/g dry weight had cirrhosis, and this was attributed to high alcohol consumption, indicating that alcohol indeed may lower the threshold for development of fibrosis. Adams37 revisited the question of a specific hepatic iron threshold for cirrhosis in HHC after the cloning of the HFE. One hundred C282Y homozygotes were evaluated, and he concluded that an HIC in excess of 283 mol/g was associated with cirrhosis. However, the low sensitivity of this threshold suggested that other cofactors contribute to the development of cirrhosis in HHC. Loreal et al.25 (in a study before the cloning of HFE that included patients with concomitant disease) also could not demonstrate a threshold of HIC above which fibrosis occurred.25 Thus, there is general agreement that although the mean HIC is higher in HHC patients with cirrhosis compared with those without cirrhosis, it is unlikely that there exists a discrete threshold value of hepatic iron for cirrhosis. Rather, it is likely that there is a range of the HIC above which the risk of cirrhosis is increased and below which the risk of cirrhosis is low. In the present study, the lowest HIC associated with cirrhosis in the nonalcoholic patients was 233 mol/g. This value is remarkably similar to the 283 mol/g that Adams proposed as an important cut point—albeit with limited sensitivity. It is likely that factors such as age, gender, and individual susceptibility to cirrhosis may all contribute to the pathogenesis of cirrhosis in this disease. Of interest, we did not find a strong correlation between HIC and age in either of our 2 groups, and this is consistent with findings of others38 – 40 who could not find a correlation between HIC and age. These results differ from those of Bassett et al.,24 who found that HIC correlated with age in the predominantly male population, and Loreal et al.,25 who reported an HIC correlation with age in males less than 40 years old. We conclude that a daily alcohol intake of greater than 60 g per day increases the risk of cirrhosis in HHC by approximately ninefold. These subjects are more likely to progress to cirrhosis at an earlier age than those who do GASTROENTEROLOGY Vol. 122, No. 2 not drink excess alcohol. The range of HIC associated with cirrhosis in the absence of alcohol and other profibrogenic factors was 233– 675 mol/g dry weight. Nevertheless, venesection therapy is recommended in all cases of elevated body iron stores irrespective of alcohol consumption to minimize the risk of disease progression. In addition, all HHC patients should be encouraged to severely curtail alcohol consumption. References 1. Britton RS. Metal-induced hepatotoxicity. Semin Liver Dis 1996; 16:3–12. 2. Houglum K, Ramm GA, Crawford DHG, Witztum JL, Powell LW, Chojkier M. Excess iron induces hepatic oxidative stress and transforming growth factor beta in genetic haemochromatosis. Hepatology 1997;26:605– 610. 3. Paradis V, Kollinger M, Fabre M, Holstege A, Poynard T, Bedossa P. In situ detection of lipid peroxidation by-products in chronic liver diseases. Hepatology 1997;26:135–142. 4. Niemela O, Parkkila S, Britton RS, Brunt E, Janney C, Bacon B. Hepatic lipid peroxidation in hereditary hemochromatosis and alcoholic liver injury. J Lab Clin Med 1999;133:451– 460. 5. Pietrangelo A. Metals, oxidative stress, and hepatic fibrogenesis. Semin Liver Dis 1996;16:26 –30. 6. Li D, Friedman SL. Liver fibrogenesis and the role of hepatic stellate cells: new insights and prospects for therapy. J Gastroenterol Hepatol 1999;14:618 – 633. 7. Adams PC, Speechley M, Kertesz AE. Long-term survival analysis in hereditary hemochromatosis. Gastroenterology 1991; 101:368 –372. 8. Fargion S, Mandelli C, Piperno A, Cesana B, Fracanzani AL, Fraquelli M, Bianchi PA, Fiorelli G, Conte D. Survival and prognostic factors in 212 Italian patients with genetic hemochromatosis. Hepatology 1992;15:655– 659. 9. Niederau C, Fischer R, Sonnenberg A, Stremmel W, Trampisch HJ, Strohmeyer G. Survival and causes of death in cirrhotic and in noncirrhotic patients with primary hemochromatosis. N Engl J Med 1985;313:1256 –1262. 10. Niederau C, Fischer R, Purschel A, Stremmel W, Haussinger D, Strohmeyer G. Long-term survival in patients with hereditary hemochromatosis. Gastroenterology 1996;110:1107–1119. 11. Poli G. Pathogenesis of liver fibrosis: role of oxidative stress. Mol Aspects Med 2000;21:49 –98. 12. Lieber CS. Alcoholic liver disease: new insights in pathogenesis lead to new treatments. J Hepatol 2000;32:113–128. 13. Leclercq IA, Farrell GC, Field J, Bell DR, Gonzalez FJ, Robertson GR. CYP2E1 and CYP4A as microsomal catalysts of lipid peroxides in murine nonalcoholic steatohepatitis. J Clin Invest 2000; 105:1067–1075. 14. Paradis V, Mathurin P, Kollinger M, Imbert-Bismut F, Charlotte F, Piton A, Opolon P, Holstege A, Poynard T, Bedossa P. In situ detection of lipid peroxidation in chronic hepatitis C: correlation with pathological features. J Clin Pathol 1997;50:401– 406. 15. Washington K, Wright K, Shyr Y, Hunter EB, Olson S, Raiford DS. Hepatic stellate cell activation in nonalcoholic steatohepatitis and fatty liver. Hum Pathol 2000;31:822– 828. 16. Schiff ER. Hepatitis C and alcohol. Hepatology 1997;26:39S– 42S. 17. Ostapowicz G, Watson KJ, Locarnini SA, Desmond PV. Role of alcohol in the progression of liver disease caused by hepatitis C virus infection. Hepatology 1998;27:1730 –1735. 18. Wiley TE, McCarthy M, Breidi L, Layden TJ. Impact of alcohol on the histological and clinical progression of hepatitis C infection. Hepatology 1998;28:805– 809. February 2002 19. Piperno A, Fargion S, D’Alba R, Roffi L, Fracanzani AL, Vecchi L, Failla M, Fiorelli G. Liver damage in Italian patients with hereditary hemochromatosis is highly influenced by hepatitis B and C virus infection. J Hepatol 1992;16:364 –368. 20. Irving MG, Halliday JW, Powell LW. Association between alcoholism and increased hepatic iron stores. Alcohol Clin Exp Res 1988;12:7–13. 21. Fletcher LM, Halliday JW, Powell LW. Interrelationships of alcohol and iron in liver disease with particular reference to the iron binding proteins, ferritin and transferrin. J Gastroenterol Hepatol 1999;14:202–214. 22. Adams PC, Agnew S. Alcoholism in hereditary hemochromatosis revisited: prevalence and clinical consequences among homozygous siblings. Hepatology 1996;23:724 –727. 23. Ganne-Carrie N, Christidis C, Chastang C, Ziol M, Chapel F, Imbert-Bismut F, Trinchet JC, Guettier C, Beaugrand M. Liver iron is predictive of death in alcoholic cirrhosis: a multivariate study of 229 consecutive patients with alcoholic and/or hepatitis C virus cirrhosis: a prospective follow up study. Gut 2000;46:277–282. 24. Bassett ML, Halliday JW, Powell LW. Value of hepatic iron measurements in early hemochromatosis and determination of the critical iron level associated with fibrosis. Hepatology 1986;6: 24 –29. 25. Loreal O, Deugnier Y, Moirand R, Lauvin L, Guyader D, Jouanolle H, Turlin B, Lescoat G, Brissot P. Liver fibrosis in genetic hemochromatosis. Respective roles of iron and non-iron-related factors in 127 homozygous patients. J Hepatol 1992;16:122–127. 26. Bacon BR. Diagnosis and management of hemochromatosis. Gastroenterology 1997;113:995–999. 27. Scheuer PJ, Williams R, Muir AR. Hepatic pathology in relatives of patients with haemochromatosis. J Pathol Bacteriol 1962;84: 53– 64. 28. Guyader D, Jacquelinet C, Moirand R, Turlin B, Mendler MH, Chaperon J, David V, Brissot P, Adams P, Deugnier Y. Noninvasive prediction of fibrosis in C282Y homozygous hemochromatosis. Gastroenterology 1998;115:929 –936. 29. Friedman SL. Molecular regulation of hepatic fibrosis, an integrated cellular response to tissue injury. J Biol Chem 2000;275: 2247–2250. 30. Lee KS, Buck M, Houglum K, Chojkier M. Activation of hepatic stellate cells by TGF alpha and collagen type I is mediated by oxidative stress through c-myb expression. J Clin Invest 1995; 96:2461–2468. IRON, ALCOHOL, AND CIRRHOSIS IN HEMOCHROMATOSIS 289 31. Tilg H, Diehl AM. Cytokines in alcoholic and nonalcoholic steatohepatitis. N Engl J Med 2000;343:1467–1476. 32. Park CH, Bacon BR, Brittenham GM, Tavill AS. Pathology of dietary carbonyl iron overload in rats. Lab Invest 1987;57:555– 563. 33. Roberts FD, Charalambous P, Fletcher L, Powell LW, Halliday JW. Effect of chronic iron overload on procollagen gene expression. Hepatology 1993;18:590 –595. 34. LeSage GD, Baldus WP, Fairbanks VF, Baggenstoss AH, McCall JT, Moore SB, Taswell HF, Gordon H. Hemochromatosis: genetic or alcohol-induced? Gastroenterology 1983;84:1471–1477. 35. Ramm GA, Crawford DHG, Powell LW, Walker NJ, Fletcher LM, Halliday JW. Hepatic stellate cell activation in genetic hemochromatosis: lobular distribution, effect of increasing hepatic iron and response to phlebotomy. J Hepatol 1997;26:584 –592. 36. Tsukamoto H, Horne W, Kamimura S, Niemela O, Parkkila S, Yla-Herttuala S, Brittenham GM. Experimental liver cirrhosis induced by alcohol and iron. J Clin Invest 1995;96:620 – 630. 37. Adams PC. Is there a threshold of hepatic iron concentration that leads to cirrhosis in C282Y hemochromatosis? Am J Gastroenterol 2001;96:567–569. 38. Adams PC, Deugnier Y, Moirand R, Brissot P. The relationship between iron overload, clinical symptoms, and age in 410 patients with genetic hemochromatosis. Hepatology 1997;25:162– 166. 39. Kowdley KV, Trainer TD, Saltzman JR, Pedrosa M, Krawitt EL, Knox TA, Susskind K, Pratt D, Bonkovsky HL, Grace ND, Kaplan MM. Utility of hepatic iron index in American patients with hereditary hemochromatosis: a multicenter study. Gastroenterology 1997;113:1270 –1277. 40. Olynyk JK, Luxon BA, Britton RS, Bacon BR. Hepatic iron concentration in hereditary hemochromatosis does not saturate or accurately predict phlebotomy requirements. Am J Gastroenterol 1998;93:346 –350. Received December 28, 2000. Accepted October 8, 2001. Address requests for reprints to: Linda M. Fletcher, Ph.D., Department of Gastroenterology and Hepatology, Princess Alexandra Hospital, Ipswich Road, Woolloongabba, Brisbane, Queensland 4102, Australia. e-mail: Lin_Fletcher@health.qld.gov.au; fax: 61-7-3240 5111. This project was supported, in part, by the National Health and Medical Research Council of Australia.