Name: Main reason for today`s visit:
advertisement

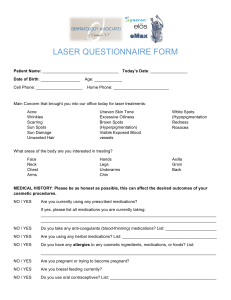
Name:__________________________ Main reason for today’s visit: __________________________________________________________________________________ __________________________________________________________________________________ Do you have any changes to your address or insurance information? Yes (list here)_____________________________________ No Check all that apply: I have the following prescriptions that need to be refilled:___________________________________________ I need a school or work excuse I need a referral to:_______________________________________ Have you had any lab work, x-rays, or other tests done recently? Yes, If so where & when? ___________________________________ No Have you been seen by a specialist recently, or started on any new medications, or had any changes in medications? Yes (explain)_____________________________________________ No Any changes to your family’s health (blood relatives?) Yes (explain)_____________________________________________ No Which pharmacy do you use? __________________________________ Is today’s visit work related? Yes No Other concerns I would like to discuss if there is time: Please note that due to time constraints we may need to address these issues at a future appointment.___________________________________