Document 16053189
advertisement

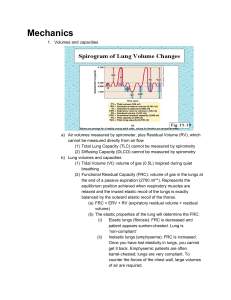
Lung is a mechanical organ • Built similar to pyramids (apex at top, base at bottom, with segments) • Packaging problem (55% on R, 45% on L) • Major properties are – Dry – Inflated Segmental Anatomy: redundancy • Purpose of segments – Prevent spread of infection – Prevent complete obstruction from an inflated foreign body • Lobes have more than one segment (20 total) – Upper – Middle – Lower Air is distributed in proportion to segmental volume • Maintain volume similar to a submarine • Ventilation is matched to volume: regional ventilation = regional volume Move during sleep; give lungs negative pressure to prevent atelectasis: airlessness Carina: branch point in the lungs • Bronchiole tree is not symmetrical • Food must pass from front to back and air from back to front – Can be problem in the old and the young – Glottis defends the airway Larnyx: rigid, cartilagenous box • Narrowest part of the system • “V” is front: vocal cords • Vocal cords move in synchrony with diaphragm Trachea: ~ vacuum hose • Posterior is muscle, anterior is cart. Rings • Muscle allows ability to cough • Posterior utilized to expel objects: blow gun or spit wad effect COPD: chronic obstructive pulmonary disease • Exhalation is restricted RLD: restrictive lung disease • Inhalation is restricted Air moves across a pressure gradient Muscles of inspiration (Active) • Diaphragm • External intercostals (bucket handles) • Inspiration is active Muscles of expiration (intercostals are stabilization) (usually passive): • Rectus abdominus • Obliques • Lats Diaphram originates in the chest wall and inserts on the central tendon: • Three muscles, right, left costal, and cural components • Criss-cross in the back to allow for the esphogus, vena cava, etc. Flow is swirly, not turbulent, difficult to characterize the flow in the upper airways to simplify, assume Ohms law: • Resistance (R) = change pressure/flow • Or flow = change in pressure/R Velocity (U = flow/area) • Need low pressure for inspiration: 5 cm/H2O • Inhale pressure has capacity for 120 cm/H2O • Maximal inspiratory pressure (MIP) usually occurs at FRC (functional residual capacity), low lung volumes, usually about -80 – -100 cm/H2O • MEP: occurs at high lung volumes, recoil of diaphragm (100-110 cm/H2O) • Due to length tension relationship Disease states: greater pressure for adequate flow (obstructive airway disease) Delta Vt/Delta pressure = compliance • High compliance: emphysema • Increase pressure – Increase chest wall diameter – Compress abdominal space Total Lung Capacity (TLC) determined by: • • • • Wt, gender, age, ht Compliance Surfactant Insp/expir. muscle strength Conducting airways have cartilage, lower do not: interdependent Alveoli are connected via smooth muscle and connective tissue: one opens, all open to prevent atelectasis Mucosal clearance: similar to flypaper, lubricates and protects: • Hydrates • Provides protective surface • Collect debris Goblet cells: secrete sticky, tenacious mucous Submucosal glands are less sticky, make islands Debris is moved up on islands to carinas via cillia “beating” • Clean from periphery to the central • Mucocilliary escalator Cystic Fibrosis: does not regulate sol (soluable) phase • Cillia are too deep, below the surface, cannot beat effectively, bacteria can overgrow Peripheral airways have laminar flow, allows for diffusion Alveoli have pores for gas diffusion, collateral airflow Two types of ventilation: • Pulmonary: air is brought into lungs and exchanged with air in lungs (Ve) • Alveolar: exchange of gases between alveoli and capillaries