Document 16053163
advertisement

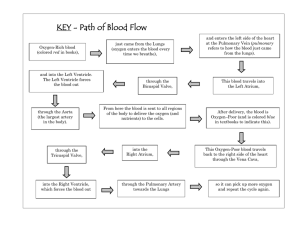
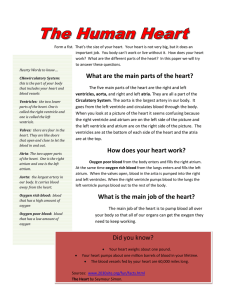
Cardiovascular Structure and Function Function of CV system: Transport of O2 to tissues and remove waste (delivery and garbage) Transport nutrients to tissues Regulate body temperature Right and left sides have separate functions: R side Atria receives blood from systemic circulation (superior and inferior vena cavas) Ventricle pumps blood to lungs for oxygenation via pulmonary artery L side Receive blood (oxygenated) from lungs Pump blood into the aorta (thick-walled and muscular in nature) to systemic circulation 4 chambered muscular organ 2 pumps, pulmonary and systemic circulation Heart muscle is called myocardium Striated, with actin and myosin filaments, similar to skeletal muscle Difference, cells are single nucleated, interconnected in a form similar to a lattice Connected by intercalated disks that allows chemical and electrical coupling between cells Thick septum (interventricular septum) that separates R and L sides Cardiac Chambers Atria are thin walled, sac-like chambers, low pressure function is to receive and store blood while ventricles are contracting, act as primer pumps reservoir is more important than pump for blood propulsion Ventricles are a continuum of muscle fibers contract from apex to base R ventricle is thicker than R atria L ventricle is 3X thicker than the R ventricular walls L ventricle can develop 4-5X more pressure than the R ventricle Number of valves in heart Thin flaps of endothelium covered fibrous tissue Movement of the valve leaflets are essentially passive Orientation of valves is responsible for the unidirectional flow of blood through the heart Atrioventricular valves prevent backflow of blood from the ventricles into the atria – also called tricuspid valve (three flaps or cusps) and mitral (bicuspid two flaps or cusps) valve Between right ventricle and pulmonary artery is a semilunar valve (three cusps) also called pulmonic valve Between left ventricle and aorta are semilunar valve (prevents backflow of blood from aorta into the heart) Blood flow through the heart 1. blood flows into right atrium from superior and inferior vena cava 2. blood travels from R atrium into R ventricle 3. blood flows through pulmonary artery into the lungs (for oxygenation) 4. blood returns from the lungs through the pulmonary veins, and is deposited into L atrium 5. from L atrium, blood flows into L ventricle 6. blood leaves L ventricle via aorta, enters general systemic circulation Flow of electricity through the heart Heart has intrinsic rhythmicity 1. originates in SA (sino-atrial) node, superior, lateral aspect of R atrium 2. travels through both atria to AV node (atrioventricular), this causes depolarization of atria 3. from AV node, pause for 0.01 sec, flows through AV bundle (aka bundle of His), through R and L bundle branches (RBB, LBB) – this pause allows time for atrial contraction, pumping the last 20-25% of blood into ventricles 4. from RBB and LBB, signal travels to the purkinje fibers in ventricles, which passes the current of depolarization to the ventricle muscle ventricles have a powerful contraction, and provide the major impetus to move blood throughout the CV system Action Potentials in cardiac muscle resting membrane potential of normal cardiac muscle is -85 to -95 millivolts specialized conductive fibers, purkinje, have a resting membrane potential of -90 to -100 mV action potential (AP) has a magnitude of ~105 mV this rise is ~ +20 mV greater than needed, called the overshoot potential after depolarization, remains depolarized for 0.2 sec in atrial muscle and 0.3 sec in ventricular muscle, which gives it the plateau plateau is followed by abrupt repolarization this plateau causes a contraction to last 315 times longer than a skeletal muscle twitch Differenced in cardiac and skeletal muscle membranes: Action potential is caused by the opening of two types of channels: a) fast sodium channels allow the sodium ions to enter the cell and b) slow calcium channel are slower to open and remain open longer (can be several tenths of a second; sodium can also pass through these channels) The permeability of cardiac muscle membrane to potassium decreases about 5X This decreases the outflux of K during plateau, preventing early recovery When Na and Ca channels close, influx stops, permeability for K increases rapidly Rapid influx of K, membrane potential returns to resting